Measuring the Impacts of Water Safety Plans in the Asia-Pacific Region

 ,
,
Abstract
1. Introduction
2. Materials and Methods
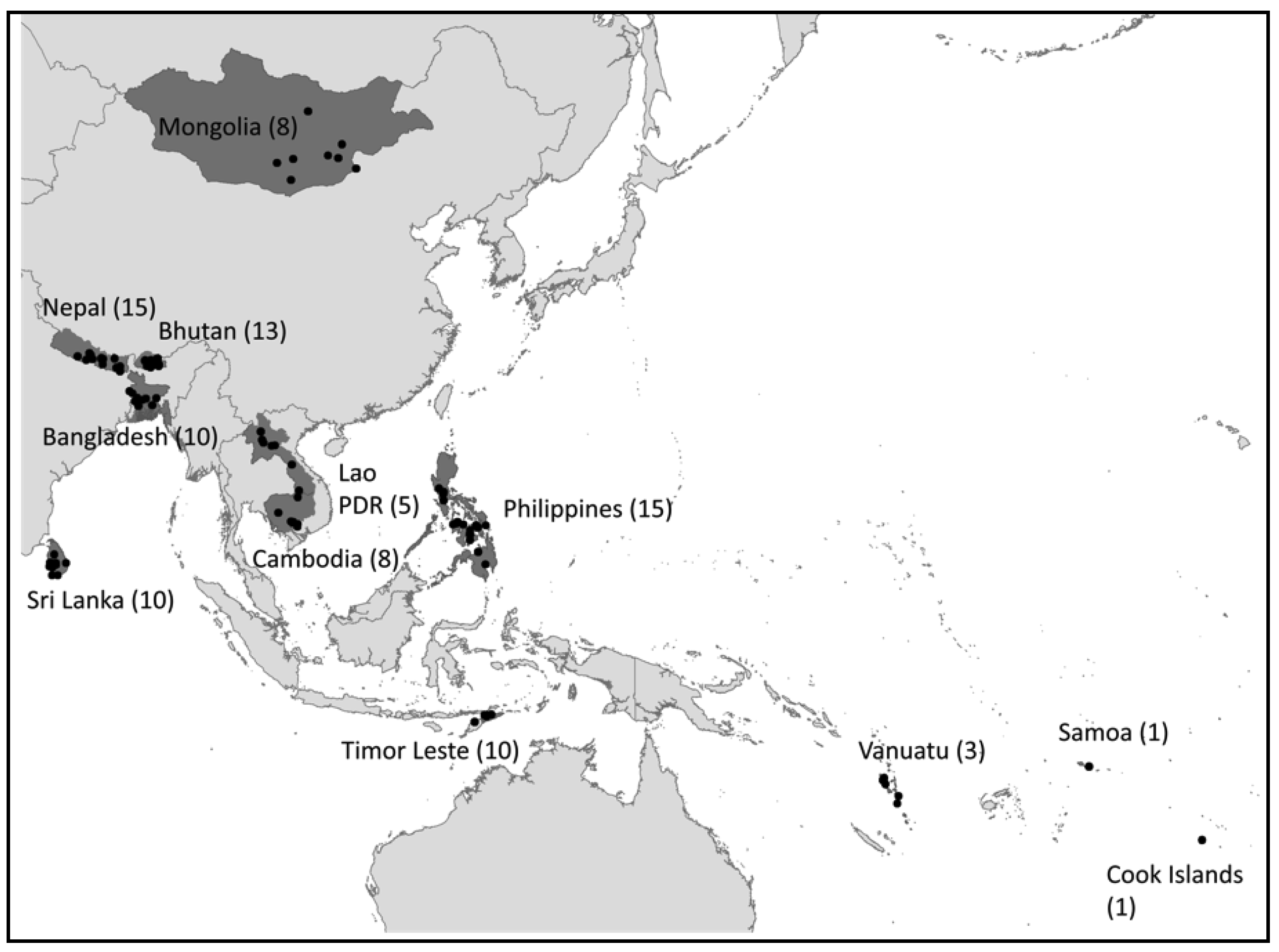
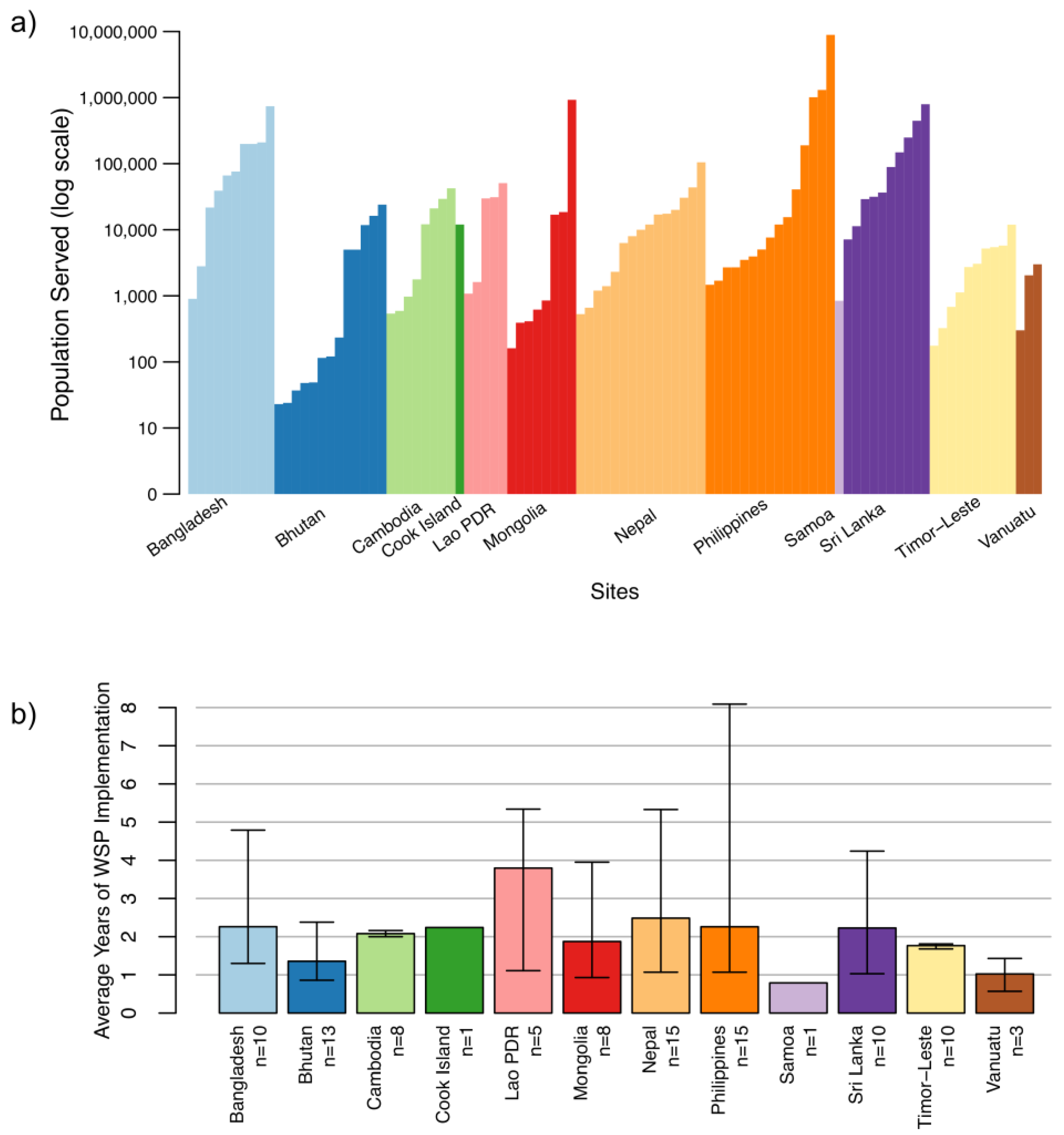
2.1. Study Sites
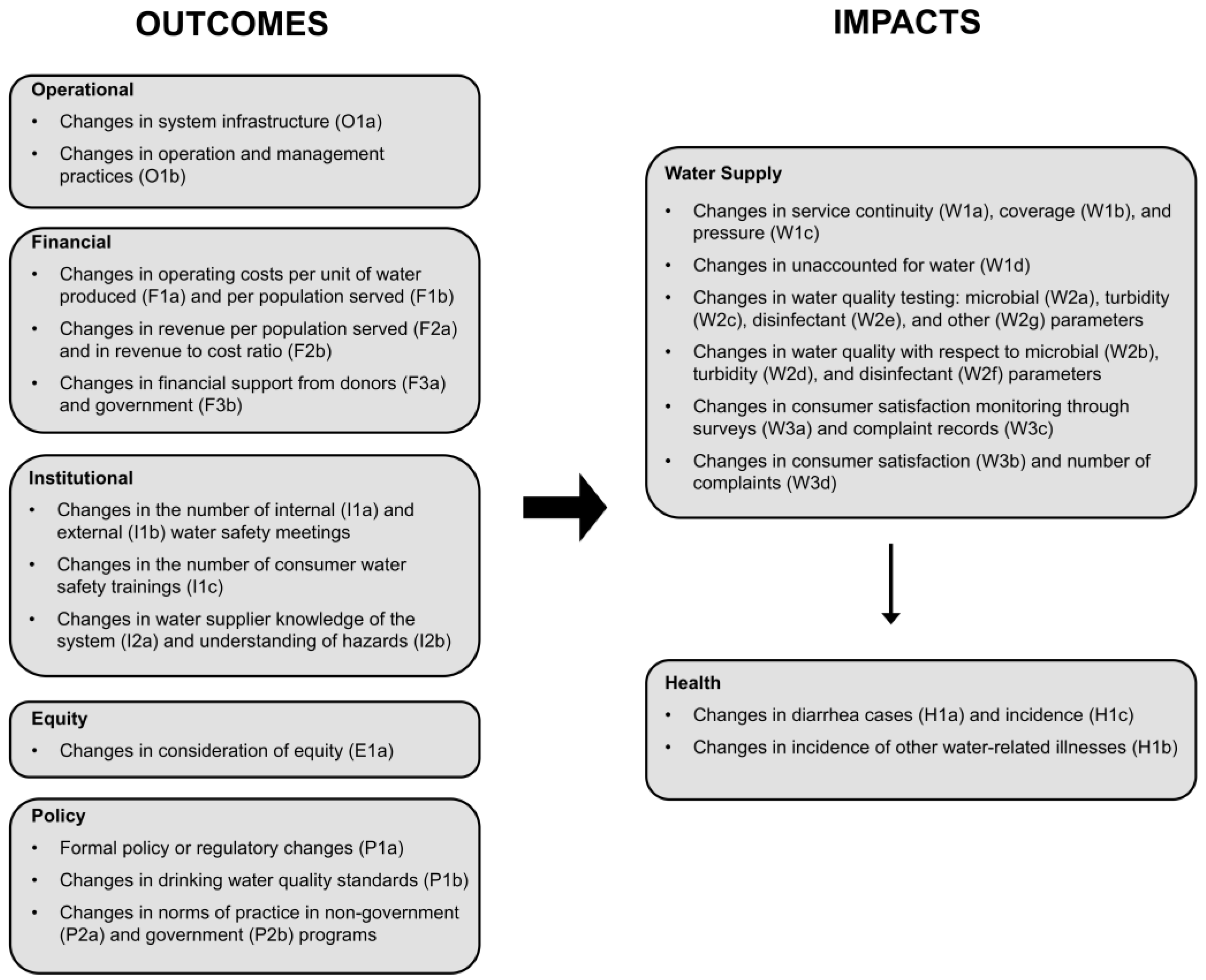
2.2. Evaluation Framework
2.3. Study Design and Data Collection
2.4. Data Processing and Analysis
2.5. Ethics Statement
3. Results
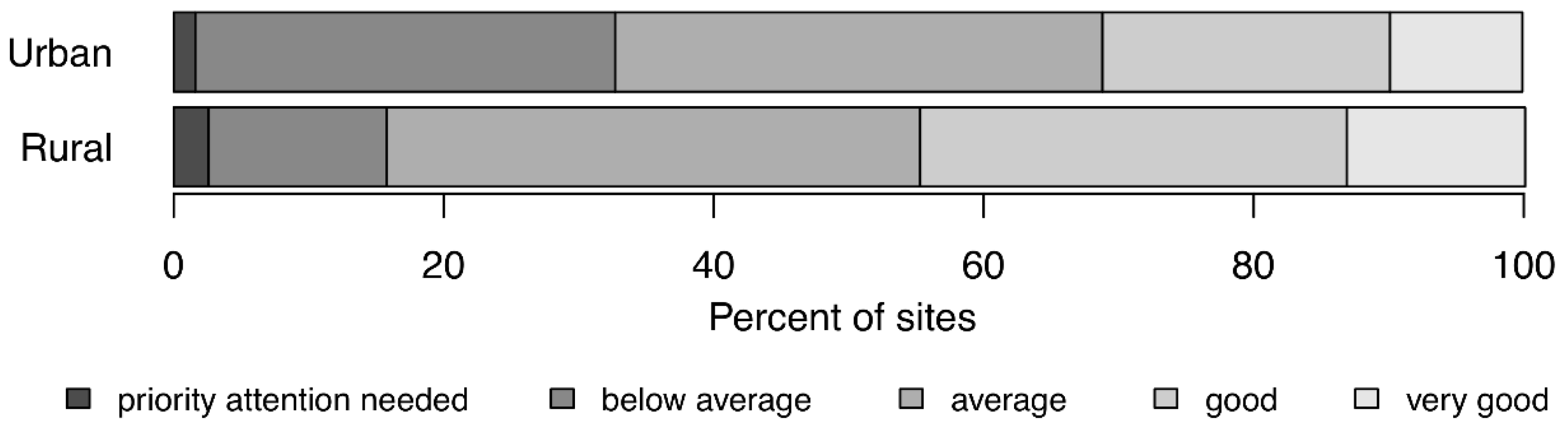
3.1. WSP Audit Scores
3.2. Evaluation Process: Analysis of the Indicators
3.3. Outcomes and Impacts of WSPs in the Asia-Pacific Region
4. Discussion
4.1. How to Improve the WSP Impact Evaluation Process
- Retain without changes. Indicators are important and reliable data were easily collected.
- Retain but modify to standardize answers and avoid calculation mistakes. Indicators are important but were associated with data quality and/or availability challenges that can be easily overcome.
- Retention requires further consideration. Indicators were associated with significant data quality and/or availability challenges that may be difficult to overcome (except at higher-capacity sites). If retained, modifications will be needed.
- Do not retain. Indicators are not core to the WSP process, are redundant and/or are not sufficiently important to warrant addressing data quality and/or availability challenges experienced.
4.2. Achievements of WSPs in the Asia-Pacific Region
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prüss-Ustün, A.; Bartram, J.; Clasen, T.; Colford, J.M.; Cumming, O.; Curtis, V.; Bonjour, S.; Dangour, A.D.; De France, J.; Fewtrell, L.; et al. Burden of Disease from Inadequate Water, Sanitation and Hygiene in Low- and Middle-Income Settings: A Retrospective Analysis of Data from 145 Countries. Trop. Med. Int. Health 2014, 19, 894–905. [Google Scholar] [CrossRef] [PubMed]
- Bain, R.; Cronk, R.; Wright, J.; Yang, H.; Slaymaker, T.; Bartram, J. Fecal Contamination of Drinking-Water in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS Med. 2014, 11, e1001644. [Google Scholar] [CrossRef] [PubMed]
- Peletz, R.; Kumpel, E.; Bonham, M.; Rahman, Z.; Khush, R. To What Extent Is Drinking Water Tested in Sub-Saharan Africa? A Comparative Analysis of Regulated Water Quality Monitoring. Int. J. Environ. Res. Public Health 2016, 13, 275. [Google Scholar] [CrossRef] [PubMed]
- Kumpel, E.; Peletz, R.; Mateyo, B.; Khush, R. Assessing Drinking Water Quality and Water Safety Management in Sub-Saharan Africa Using Regulated Monitoring Data. Environ. Sci. Technol. 2016, 50, 10869–10876. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Guidelines for Drinking Water Quality, 3rd ed.; World Health Organization: Geneva, Switzerland, 2004; Available online: http://www.who.int/water_sanitation_health/publications/gdwq3/en/ (accessed on 28 May 2018).
- Bartram, J.; Corrales, L.; Davison, A.; Deere, D.; Drury, D.; Gordon, B.; Howard, G.; Rinehold, A.; Stevens, M. Water Safety Plan Manual: Step-by-Step Risk Management for Drinking-Water Suppliers; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organisation (WHO). Water Safety Planning for Small Community Water Supplies: Step-by-Step Risk Management Guidance for Drinking-Water Supplies in Small Communities; World Health Organisation: Geneva, Switzerland, 2012; Available online: http://www.who.int/water_sanitation_health/publications/small-comm-water_supplies/en/ (accessed on 28 May 2018).
- World Health Organization (WHO). Guidelines for Drinking-Water Quality, 5th ed.; World Health Organisation: Geneva, Switzerland, 2011; Available online: http://www.who.int/water_sanitation_health/publications/2011/dwq_guidelines/en/ (accessed on 28 May 2018).
- World Health Organization (WHO)/International Water Association (IWA). Global Status Report on Water Safety Plans: A Review of Proactive Risk Assessment and Risk Management Practices to Ensure the Safety of Drinking-Water; World Health Organisation: Geneva, Switzerland, 2017; Available online: http://www.who.int/water_sanitation_health/publications/global-status-report-on-water-safety-plans/en/ (accessed on 28 May 2018).
- Byleveld, P.; Leask, S.; Jarvis, L.; Wall, K.; Henderson, W.; Tickell, J. Safe Drinking Water in Regional NSW, Australia. Public Health Res. Pract. 2016, 26, 2621615. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, B.; Gelting, R.; del Carmen Portillo, M.; Williams, T.; Torres, R. Awareness, Adoption and Implementation of the Water Safety Plan Methodology: Insights from Five Latin American and Caribbean Experiences. J. Water Sanit. Hyg. Dev. 2013, 3, 541–548. [Google Scholar] [CrossRef]
- Kot, M.; Castleden, H.; Gagnon, G.A. The Human Dimension of Water Safety Plans: A Critical Review of Literature and Information Gaps. Environ. Rev. 2014, 23, 24–29. [Google Scholar] [CrossRef]
- Mahmud, S.G.; Shamsuddin, S.A.J.; Feroze Ahmed, M.; Davison, A.; Deere, D.; Howard, G. Development and Implementation of Water Safety Plans for Small Water Supplies in Bangladesh: Benefits and Lessons Learned. J. Water Health 2007, 5, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Ncube, M.; Pawandiwa, M.N. Water Safety Planning and Implementation: Lessons from South Africa. J. Water Sanit. Hyg. Dev. 2013, 3, 557–563. [Google Scholar] [CrossRef]
- Omar, Y.Y.; Parker, A.; Smith, J.A.; Pollard, S.J.T. Risk Management for Drinking Water Safety in Low and Middle Income Countries–Cultural Influences on Water Safety Plan (WSP) Implementation in Urban Water Utilities. Sci. Total Environ. 2017, 576, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Tibatemwa, S.; Godfrey, S.; Niwagaba, C.; Kizito, F. Implementing Water-Safety Plans in Urban Piped-Water Supplies in Uganda. Waterlines 2005, 23, 8–10. [Google Scholar] [CrossRef]
- String, G.; Lantagne, D. A Systematic Review of Outcomes and Lessons Learned from General, Rural, and Country-Specific Water Safety Plan Implementations. Water Sci. Technol. Water Supply 2016, 16, 1580–1594. [Google Scholar] [CrossRef]
- Gunnarsdottir, M.J.; Gardarsson, S.M.; Elliott, M.; Sigmundsdottir, G.; Bartram, J. Benefits of Water Safety Plans: Microbiology, Compliance, and Public Health. Environ. Sci. Technol. 2012, 46, 7782–7789. [Google Scholar] [CrossRef] [PubMed]
- Setty, K.E.; Kayser, G.L.; Bowling, M.; Enault, J.; Loret, J.-F.; Serra, C.P.; Alonso, J.M.; Mateu, A.P.; Bartram, J. Water Quality, Compliance, and Health Outcomes among Utilities Implementing Water Safety Plans in France and Spain. Int. J. Hyg. Environ. Health 2017, 220, 513–530. [Google Scholar] [CrossRef] [PubMed]
- Gelting, R.J.; Delea, K.; Medlin, E. A Conceptual Framework to Evaluate the Outcomes and Impacts of Water Safety Plans. J. Water Sanit. Hyg. Dev. 2012, 2, 103–111. [Google Scholar] [CrossRef]
- Lockhart, G.; Oswald, W.E.; Hubbard, B.; Medlin, E.; Gelting, R.J. Development of Indicators for Measuring Outcomes of Water Safety Plans. J. Water Sanit. Hyg. Dev. 2014, 4, 171–181. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). Auditing Water Safety Plans. 2016. Available online: http://www.who.int/water_sanitation_health/publications/auditing-water-safety-plans/en/ (accessed on 28 May 2018).
- QSR International Pty Ltd. NVivo Qualitative Data Analysis Software; QSR International Pty Ltd.: Burlington, MA, USA, 2014. [Google Scholar]
- Schmidt, W.-P.; Arnold, B.F.; Boisson, S.; Genser, B.; Luby, S.P.; Barreto, M.L.; Clasen, T.; Cairncross, S. Epidemiological Methods in Diarrhoea Studies—An Update. Int. J. Epidemiol. 2011, 40, 1678–1692. [Google Scholar] [CrossRef] [PubMed]
- Benjamin-Chung, J.; Sultana, S.; Halder, A.K.; Ahsan, M.A.; Arnold, B.F.; Hubbard, A.E.; Unicomb, L.; Luby, S.P.; Colford, J.M. Scaling Up a Water, Sanitation, and Hygiene Program in Rural Bangladesh: The Role of Program Implementation. Am. J. Public Health 2017, 107, 694–701. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Total Sites | Type of System | Context | Age | ||||
|---|---|---|---|---|---|---|---|---|
| Piped Systems | Point Sources | Urban | Rural | <2 years | >2 years | |||
| Utility/LGU a | Community-Managed b | |||||||
| Bangladesh | 10 | 8 | 2 | 0 | 8 | 2 | 7 | 3 |
| Bhutan | 13 | 6 | 7 b | 0 | 7 | 6 | 10 | 3 |
| Cambodia | 8 | 4 | 0 | 4 c | 4 | 4 | 0 | 8 |
| Cook Islands | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 |
| Lao PDR | 5 | 3 | 0 | 2 c | 3 | 2 | 1 | 4 |
| Mongolia | 8 | 7 | 0 | 1 c | 3 | 5 | 5 | 3 |
| Nepal | 15 | 1 | 14 | 0 | 11 | 4 | 9 | 6 |
| Philippines | 15 | 12 | 0 | 3 d | 8 | 7 | 11 | 4 |
| Samoa | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 |
| Sri Lanka | 10 | 10 | 0 | 0 | 10 | 0 | 4 | 6 |
| Timor-Leste | 10 | 6 | 4 | 0 | 6 | 4 | 10 | 0 |
| Vanuatu | 3 | 0 | 3 | 0 | 0 | 3 | 3 | 0 |
| Total | 99 | 58 | 31 | 10 | 60 | 39 | 61 | 38 |
| Code | Indicator | Data Format | Availability (% of Sites) 5 | Data Quality | Category 6 | Comments on Suggested Revisions |
|---|---|---|---|---|---|---|
| O | Operational Outcomes | |||||
| O1a | Infrastructure change as a result of WSP 1 | Y/N, description | 95 | Good | A | Retain |
| O1b | Level of operations and management practices | Score of 8–40 (score of 1–5 each) | 93 | Good | ||
| (1) Operational monitoring plan | A | Retain | ||||
| (2) Compliance monitoring plan | A | Retain | ||||
| (3) Consumer satisfaction monitoring | D | Exclude because redundant with W3b | ||||
| (4) Standard operating procedures | A | Retain | ||||
| (5) Emergency response plan | A | Retain | ||||
| (6) Operator or caretaker training programs | A | Retain | ||||
| (7) Consumer education programs | D | Exclude because redundant with I1c | ||||
| (8) Equipment maintenance/calibration schedules | C | Reconsider including as addressing such maintenance schedules is not emphasized in the WSP process | ||||
| F | Financial Outcomes | |||||
| F1a | Operating costs per unit water 2 | $/m3 | 72 | Poor | D | Exclude to simplify; revenue to cost ratio will suffice |
| F1b | Operating costs per population 2 | $/pop | 71 | Poor | D | Exclude to simplify; revenue to cost ratio will suffice |
| F2a | Revenue per population 2 | $/pop | 71 | Poor | D | Exclude to simplify; revenue to cost ratio will suffice |
| F2b | Revenue to cost ratio 2 | % | 66 | Poor | B | Retain but provide a step-by-step calculation guide to avoid mistakes and standardize the definitions of operating costs and revenue |
| F3a | Financial support as a direct result of WSP 1 | Y/N, description | 89 | Good | A | Retain |
| F3b | Funds from government for water supply | $/description | 59 | Poor | B | Retain but combine with indicator F3a and provide more guidance to clarify indicator and to improve reliability of data |
| I | Institutional Outcomes | |||||
| I1a | Internal water safety meetings 2 | Number | 92 | Good | A | Retain |
| I1b | External water safety meetings 2 | Number | 92 | Good | A | Retain |
| I1c | Consumer water safety trainings 2 | Number | 85 | Good | A | Retain |
| I2a | Understanding of system 3 | Score of 5–25 | 19 | Poor | C | Reconsider including due to lack of meaningful measurements (unless a more effective and systematic measurement approach can be designed) |
| I2b | Understanding of hazards 3 | Number | 19 | Poor | C | |
| E | Equity Outcomes | |||||
| E1a | Equity 4 | Score of 6–30 (score of 1–5 each) | 88 | Poor | C | Reconsider including due to widespread misinterpretation until explicit consideration of equity through the WSP process is widely promoted |
| (1) Participation | ||||||
| (2) Groups identified and documented | ||||||
| (3) Hazards/issues prioritized | ||||||
| (4) Improvements benefit equitably | ||||||
| (5) Monitoring data disaggregated | ||||||
| (6) Emergency response and communication programs reflect needs | ||||||
| W | Water Supply Impact | |||||
| W1a | Continuity | Hours/week | 93 | Good | B | Retain but consider refining guidance to avoid rough estimates of continuity |
| W1b | Service coverage | % | 76 | Good | C | Reconsider including as expanding service coverage is often not a core priority or key outcome of WSPs |
| W1c | Pressure | atm/bar/m | 22 | Poor | C | Reconsider including due to data quality concerns (variable measurement methods and tendency to provide rough estimates) |
| W1d | Unaccounted-for Water (UFW) | % | 30 | Good | B | Retain but revise guidance to better distinguish between UFW and non-revenue water (NRW) |
| W2a | Microbial tests 2 | Number | 89 | Good | A | Retain |
| W2b | Microbial compliance 2 | % | 60 | Good | A | Retain |
| W2c | Turbidity tests 2 | Number | 87 | Good | A | Retain |
| W2d | Turbidity compliance 2 | % | 37 | Good | A | Retain |
| W2e | Disinfectant residual tests 2 | Number | 74 | Good | A | Retain |
| W2f | Disinfectant compliance 2 | % | 21 | Good | A | Retain |
| W2g | Other water quality parameter compliance 2 | %, description | 0 | Poor | B | Retain but standardize list of parameters and formatting |
| W3a | Consumer satisfaction surveys conducted | Y/N | 92 | Good | A | Retain |
| W3b | Consumers satisfied 2 | % | 10 | Good | B | Retain but consider recommending a household survey where suppliers do not have standardized data |
| W3c | Consumer complaint records kept | Y/N | 92 | Good | A | Retain |
| W3d | Number of consumer complaints 2 | % | 22 | Poor | B | Retain but standardize reporting |
| H | Health Impact | |||||
| H1a | Cases of diarrhea 2 | Number | 43 | Poor | B | Retain but revise guidance to highlight/address common discrepancies between health center and WSP coverage areas |
| H1b | Other water-related illnesses 2 | Number | 31 | Poor | B | Retain but revise guidance to highlight/address common discrepancies between health center and WSP coverage areas and combine with indicator H1a |
| H1c | Diarrheal incidence 2 | % | 5 | Poor | B | Retain but change to primary household data collection rather than review of existing household data available |
| P | Policy Outcomes | |||||
| P1a | Proactive water quality risk management approaches are/were included in formal water sector policies or regulations at time of follow-up assessment | Y/N, description | 92 | Poor | B | Retain but provide a standardized definition of risk management |
| P1b | Activity to develop or revise national drinking water quality standards has been undertaken | Y/N, description | 92 | Poor | D | Exclude because difficult to obtain information in a standardized and meaningful way and link to WSP implementation |
| P2a | Proactive water quality risk management approaches have been adopted by other water-sector stakeholders (e.g., NGOs, UNICEF) | Y/N, description | 83 | Poor | D | Exclude because difficult to obtain information in a standardized and meaningful way |
| P2b | Proactive water quality risk management approaches are promoted in national or sub-national programs | Y/N, description | 83 | Poor | C | Reconsider including this indicator reflects drivers of WSPs as opposed to outcomes |
| Code | Indicator | n | Unit | % of Sites | Median Values | p-Values | ||
|---|---|---|---|---|---|---|---|---|
| Base-Line | Follow-Up | Base-Line | Follow-Up | |||||
| Operational Outcomes | ||||||||
| O1a | Infrastructure changes due to WSP | 95 | yes/no | - | 86 | - | - | - |
| O1b | Level of operations and management practices | 93 | % | - | - | 9 | 44 | <0.01 |
| Financial Outcomes | ||||||||
| F3a | Financial support due to WSP | 89 | yes/no | - | 42 | - | - | - |
| Institutional Outcomes | ||||||||
| I1a | Internal meetings | 92 | number | 16 | 60 | 0 | 2 | <0.01 |
| I1b | External water safety meetings | 92 | number | 25 | 48 | 0 | 0 | <0.01 |
| I1c | Consumer water safety trainings | 85 | number | 16 | 53 | 0 | 1 | <0.01 |
| Water Supply Impact | ||||||||
| W1a | Continuity | 93 | h/week | 34 a | 37 a | 97 | 104 | 0.59 |
| W1b | Service coverage | 76 | % | - | - | 85 | 81 | 0.75 |
| W1d | Unaccounted-for water (UFW) | 30 | % | - | - | 25 | 20 | 0.01 |
| W2a | Microbial tests | 89 | number | 73 | 85 | 3 | 12 | <0.01 |
| W2b | Microbial compliance | 60 | % | - | - | 99 | 98 | 0.24 |
| W2c | Turbidity tests | 87 | number | 45 | 70 | 0 | 4 | <0.01 |
| W2d | Turbidity compliance | 37 | % | - | - | 100 | 100 | 0.5 |
| W2e | Disinfectant residual tests | 74 | number | 39 | 57 | 0 | 10 | <0.01 |
| W3a | Consumer satisfaction surveys | 92 | % | 13 | 33 | - | - | <0.01 |
| W3c | Consumer complaint records | 92 | % | 41 | 61 | - | - | <0.01 |
| Indicators | Observed WSP Outcomes and Impacts | % of Sites Showing Improvements 1 (and Number of Countries) |
|---|---|---|
| O1a | Infrastructure improvements | 86% (10 countries) |
| O1b | Improvement in operation and management | 95% (12 countries) |
| F3a | Leveraging of donor funds | 39% (9 countries) |
| I1a, b, c | Increased stakeholder communication and collaboration | 66% (10 countries) |
| W1d | Reduction in unaccounted-for water (UFW) | 21% (7 countries) |
| W2a, c, e | Increased water quality testing | 65% (11 countries) |
| W3a, c | Increased monitoring of consumer satisfaction | 33% (11 countries) |
| Uncontrolled Study Designs | Controlled Study Designs | |||
| Context: Site- or Country-Level Monitoring and Evaluation | Context: Research and Rigorous Impact Assessments | |||
| Before-after Comparison | Interrupted Time Series | Matched Controls | Randomized Controlled Trial | |
| Control group | No control group; for each site, relevant indicators are compared before and after WSP implementation | No control group; for each site, historical time series of relevant indicators are investigated to detect potential changes in slope coinciding with WSP implementation | Before WSP implementation, sites are manually assigned to a “control” or “intervention” group by matching a number of selected parameters between the two groups (e.g., system size, age, revenue, geographic setting) | Before WSP implementation, sites are randomly assigned to a “control” or “intervention” group. The randomization ensures that all possible confounding factors are equally distributed amongst the two groups. |
| WSP implementation | To all sites | To all sites | Only to “intervention” group | Only to “intervention” group |
| Data needed | Baseline and follow-up data | Historical data (pre- and post-WSP) on all relevant indicators (i.e., time series, not just baseline and follow-up data) | Inventory of all eligible study sites with data on parameters for matching Baseline and follow-up data | Inventory of all eligible study sites, ideally with data on some key parameters to confirm comparability between intervention and control groups Baseline and follow-up data |
| Advantages | Simplest study design (does not require a control group and only two data points per indicator: before and after) Results can be valuable for national advocacy and to encourage better monitoring/data collection practices Two rounds of data collection | Does not require a control group Provides more confidence than a simple before-after comparison that the changes observed may be associated with WSP implementation | A rigorous study design to examine associations between WSP implementation and outcomes/impacts, as long as all key parameters potentially affecting a water system’s performance (i.e., confounding factors) are used for matching Two rounds of data collection | The only study design able to establish causality, i.e., the differences between the control and intervention groups can be attributed to WSP implementation because confounding factors are equally distributed amongst the two groups Two rounds of data collection |
| Challenges and limitation | Causality cannot be established from a simple before-after comparison, i.e., the changes observed cannot be attributed to WSP implementation | Limitations in establishing causality (i.e., the change in slope observed cannot be rigorously attributed to WSP implementation) Multiple (>2) rounds of data collection Difficult to obtain time series of all relevant indicators, especially in low-capacity sites that do not keep rigorous records. Where available data are limited, data collection could be limited to those indicators that are most likely to show changes (as identified by prior rigorous impact assessments conducted at other sites) | Difficult to obtain data on matching parameters, especially for small water systems Risk that confounding factors may be unevenly distributed between the two groups (especially if an insufficient number of parameters are selected for matching), limiting ability to establish causality | Randomizing WSP implementation may cause ethical concerns or political frictions. To mitigate these, WSPs could be implemented in the control group at the end of data collection (i.e., staggered implementation). |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumpel, E.; Delaire, C.; Peletz, R.; Kisiangani, J.; Rinehold, A.; De France, J.; Sutherland, D.; Khush, R. Measuring the Impacts of Water Safety Plans in the Asia-Pacific Region. Int. J. Environ. Res. Public Health 2018, 15, 1223. https://doi.org/10.3390/ijerph15061223
Kumpel E, Delaire C, Peletz R, Kisiangani J, Rinehold A, De France J, Sutherland D, Khush R. Measuring the Impacts of Water Safety Plans in the Asia-Pacific Region. International Journal of Environmental Research and Public Health. 2018; 15(6):1223. https://doi.org/10.3390/ijerph15061223
Chicago/Turabian StyleKumpel, Emily, Caroline Delaire, Rachel Peletz, Joyce Kisiangani, Angella Rinehold, Jennifer De France, David Sutherland, and Ranjiv Khush. 2018. "Measuring the Impacts of Water Safety Plans in the Asia-Pacific Region" International Journal of Environmental Research and Public Health 15, no. 6: 1223. https://doi.org/10.3390/ijerph15061223
APA StyleKumpel, E., Delaire, C., Peletz, R., Kisiangani, J., Rinehold, A., De France, J., Sutherland, D., & Khush, R. (2018). Measuring the Impacts of Water Safety Plans in the Asia-Pacific Region. International Journal of Environmental Research and Public Health, 15(6), 1223. https://doi.org/10.3390/ijerph15061223