Analysis of Socioeconomic Status in the Patients with Rheumatoid Arthritis




Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Annual Denominator Data
2.3. Selection of RA Case
2.4. Statistical Analyses
3. Results
3.1. Increasing Prevalence of RA in Taiwan from 2001 to 2011
3.2. Different Prevalence of RA in Different Age, and Higher Prevalence in the Group of 70–79 Years Old Especially
3.3. Higher Prevalence of RA in the People with Women, Older Age, Living in Rural Area or Low-Income Earner (Monthly Income Less Than 1000 USD)
3.4. Lower Socioeconomic Status, Women, and Living Closed Rural Area Increased the Risk of RA
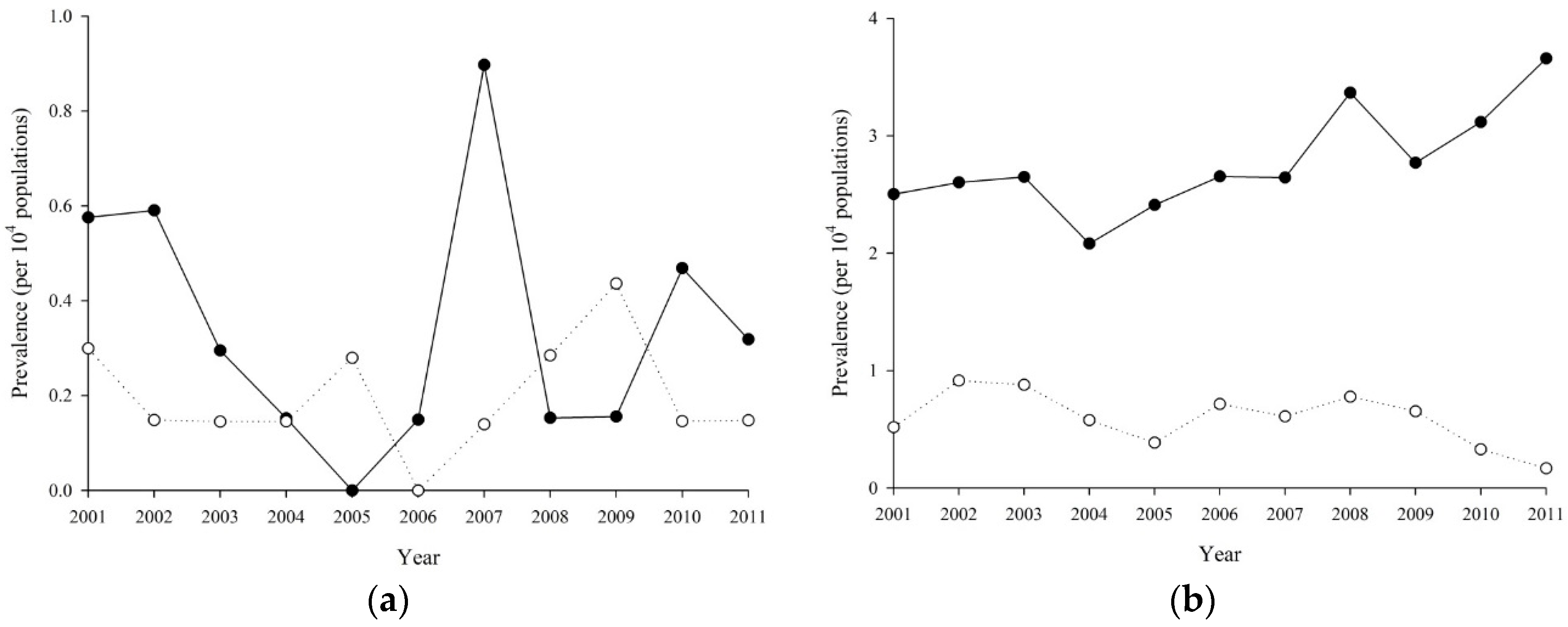
3.5. The Incidence of RA was Increasing with Age Except Women or Men
3.6. Elder and Women were the Risk for Developing RA
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Minichiello, E.; Semerano, L.; Boissier, M.C. Time trends in the incidence, prevalence, and severity of rheumatoid arthritis: A systematic literature review. Jt. Bone Spine 2016, 83, 625–630. [Google Scholar] [CrossRef] [PubMed]
- McDougall, C.; Hurd, K.; Barnabe, C. Systematic review of rheumatic disease epidemiology in the indigenous populations of Canada, the United States, Australia, and New Zealand. Semin. Arthritis Rheum. 2017, 46, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Guillemin, F.; Saraux, A.; Guggenbuhl, P.; Roux, C.H.; Fardellone, P.; Le Bihan, E.; Cantagrel, A.; Chary-Valckenaere, I.; Euller-Ziegler, L.; Flipo, R.M.; et al. Prevalence of rheumatoid arthritis in France: 2001. Ann. Rheum. Dis. 2005, 64, 1427–1430. [Google Scholar] [CrossRef] [PubMed]
- Symmons, D.P. Environmental factors and the outcome of rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 2003, 17, 717–727. [Google Scholar] [CrossRef]
- Cooper, G.S. Occupational exposures and risk of rheumatoid arthritis: Continued advances and opportunities for research. J. Rheumatol. 2008, 35, 950–952. [Google Scholar] [PubMed]
- Jin, Z.; Xiang, C.; Cai, Q.; Wei, X.; He, J. Alcohol consumption as a preventive factor for developing rheumatoid arthritis: A dose-response meta-analysis of prospective studies. Ann. Rheum. Dis. 2014, 73, 1962–1967. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, D.; Alfredsson, L.; Bottai, M.; Askling, J.; Wolk, A. Long term alcohol intake and risk of rheumatoid arthritis in women: A population based cohort study. BMJ 2012, 345, e4230. [Google Scholar] [CrossRef] [PubMed]
- Stolt, P.; Kallberg, H.; Lundberg, I.; Sjögren, B.; Klareskog, L.; Alfredsson, L. Silica exposure is associated with increased risk of developing rheumatoid arthritis: Results from the Swedish EIRA study. Ann. Rheum. Dis. 2005, 64, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Schmickler, J.; Rupprecht, A.; Patschan, S.; Patschan, D.; Müller, G.A.; Haak, R.; Mausberg, R.F.; Schmalz, G.; Kottmann, T.; Ziebolz, D. Cross-sectional Evaluation of Periodontal Status, Microbiological and Rheumatoid Parameters in a large Cohort of Patients With Rheumatoid Arthritis. J. Periodontol. 2017, 88, 368–379. [Google Scholar] [CrossRef]
- Scher, J.U.; Ubeda, C.; Artacho, A.; Attur, M.; Isaac, S.; Reddy, S.M.; Marmon, S.; Neimann, A.; Brusca, S.; Patel, T.; et al. Decreased bacterial diversity characterizes the altered gut microbiota in patients with psoriatic arthritis, resembling dysbiosis in inflammatory bowel disease. Arthritis Rheumatol. 2015, 67, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Marotte, H.; Farge, P.; Gaudin, P.; Alexandre, C.; Mougin, B.; Miossec, P. The association between periodontal disease and joint destruction in rheumatoid arthritis extends the link between the HLA-DR shared epitope and severity of bone destruction. Ann. Rheum. Dis. 2006, 65, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Kau, A.L.; Ahern, P.P.; Griffin, N.W.; Goodman, A.L.; Gordon, J.I. Human nutrition, the gut microbiome and the immune system. Nature 2011, 474, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Sandberg, M.E.; Saevarsdottir, S.; Klareskog, L.; Alfredsson, L.; Bengtsson, C. Higher education is associated with a better rheumatoid arthritis outcome concerning for pain and function but not disease activity: Results from the EIRA cohort and Swedish rheumatology register. Arthritis Res. Ther. 2015, 17, 317. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.J.; Chao, Y.L.; Chen, C.Y.; Chang, C.M.; Wu, E.C.; Wu, C.S.; Yeh, H.H.; Chen, C.H.; Tsai, H.J. Prevalence of autoimmune diseases in in-patients with schizophrenia: Nationwide population-based study. Br. J. Psychiatry 2012, 200, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.H.; Wang, P.H.; Wang, S.J.; Sun, W.Z.; Oyang, Y.J.; Fuh, J.L. Women with endometriosis are more likely to suffer from migraines: A population-based study. PLoS ONE 2012, 7, e33941. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-Y.; Hung, Y.T.; Chuang, Y.; Chen, Y.; Weng, W.; Liu, J.; Liang, K. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar]
- Hsu, C.C.; Lee, C.H.; Wahlqvist, M.L.; Huang, H.L.; Chang, H.Y.; Chen, L.; Shih, S.F.; Shin, S.J.; Tsai, W.C.; Chen, T.; et al. Poverty increases type 2 diabetes incidence and inequality of care despite universal health coverage. Diabetes Care 2012, 35, 2286–2292. [Google Scholar] [CrossRef] [PubMed]
- Abhishek, A.; Doherty, M.; Kuo, C.F.; Mallen, C.D.; Zhang, W.; Grainge, M.J. Rheumatoid arthritis is getting less frequent-results of a nationwide population-based cohort study. Rheumatology 2017, 56, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.L.; Wolfe, F.; Huizinga, T.W. Rheumatoid arthritis. Lancet 2010, 376, 1094–1108. [Google Scholar] [CrossRef]
- Ghawi, H.; Crowson, C.S.; Rand-Weaver, J.; Krusemark, E.; Gabriel, S.E.; Juhn, Y.J. A novel measure of socioeconomic status using individual housing data to assess the association of SES with rheumatoid arthritis and its mortality: A population-based case-control study. BMJ Open 2015, 5, e006469. [Google Scholar] [CrossRef] [PubMed]
- Baldassari, A.R.; Cleveland, R.J.; Luong, M.L.; Jonas, B.L.; Conn, D.L.; Moreland, L.W.; Bridges, S.L.; Callahan, L.F. Socioeconomic factors and self-reported health outcomes in African Americans with rheumatoid arthritis from the Southeastern United States: The contribution of childhood socioeconomic status. BMC Musculoskelet. Disord. 2016, 17, 10. [Google Scholar] [CrossRef] [PubMed]
- Verstappen, S.M. The impact of socio-economic status in rheumatoid arthritis: What do(n’t) we know? Rheumatology 2016, 56, 1051–1052. [Google Scholar] [CrossRef] [PubMed]
- Criswell, L.A.; Saag, K.G.; Mikuls, T.R.; Cerhan, J.R.; Merlino, L.A.; Lum, R.F.; Pfeiffer, K.A.; Woehl, B.; Seldin, M.F. Smoking interacts with genetic risk factors in the development of rheumatoid arthritis among older Caucasian women. Ann. Rheum. Dis. 2006, 65, 1163–1167. [Google Scholar] [CrossRef] [PubMed]
- Van Wesemael, T.J.; Ajeganova, S.; Humphreys, J.; Terao, C.; Muhammad, A.; Symmons, D.P.; MacGregor, A.J.; Hafström, I.; Trouw, L.A.; van der Helm-van, A.H.; et al. Smoking is associated with the concurrent presence of multiple autoantibodies in rheumatoid arthritis rather than with anti-citrullinated protein antibodies per se: A multicenter cohort study. Arthritis Res. Ther. 2016, 18, 285. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Hiraki, L.T.; Sparks, J.A.; Malspeis, S.; Chen, C.Y.; Awosogba, J.A.; Arkema, E.V.; Costenbader, K.H.; Karlson, E.W. Being overweight or obese and risk of developing rheumatoid arthritis among women: A prospective cohort study. Ann. Rheum. Dis. 2014, 73, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.K.; Kim, D.; Won, S.; Lee, J.; Choi, C.B.; Choe, J.Y.; Hong, S.J.; Jun, J.B.; Kim, T.H.; Koh, E.; et al. Factors associated with time to diagnosis from symptom onset in patients with early rheumatoid arthritis. Korean J. Intern. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Barnabe, C.; Xiong, J.; Pope, J.E.; Boire, G.; Hitchon, C.; Haraoui, B.; Thorne, J.C.; Tin, D.; Keystone, E.C.; Bykerk, V.P.; et al. Factors associated with time to diagnosis in early rheumatoid arthritis. Rheumatol. Int. 2014, 34, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Demmelmaier, I.; Bjork, A.; Dufour, A.B.; Nordgren, B.; Opava, C.H. Trajectories of Fear-Avoidance Beliefs on Physical Activity Over Two Years in People with Rheumatoid Arthritis. Arthritis Care Res. 2018, 70, 695–702. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | All | Female | Male | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Population | Case | Prevalence (95% CI) | Population | Case | Prevalence (95% CI) | Population | Case | Prevalence (95% CI) | |
| 2001 | 778,103 | 516 | 6.63 (6.08–7.23) | 392,460 | 414 | 10.55 (9.58–11.62) | 385,643 | 102 | 2.64 (2.18–3.21) |
| 2002 | 789,642 | 565 | 7.16 (6.59–7.77) | 397,925 | 453 | 11.38 (10.38–12.48) | 391,717 | 112 | 2.86 (2.38–3.44) |
| 2003 | 814,451 | 627 | 7.70 (7.12–8.33) | 417,117 | 496 | 11.89 (10.89–12.99) | 397,334 | 131 | 3.30 (2.78–3.91) |
| 2004 | 821,388 | 686 | 8.35 (7.75–9.00) | 419,710 | 540 | 12.87 (11.83–14.00) | 401,678 | 146 | 3.63 (3.09–4.27) |
| 2005 | 864,560 | 777 | 8.99 (8.38–9.64) | 439,144 | 626 | 14.26 (13.18–15.42) | 425,416 | 151 | 3.55 (3.03–4.16) |
| 2006 | 860,999 | 847 | 9.84 (9.20–10.52) | 439,640 | 669 | 15.22 (14.11–16.41) | 421,359 | 178 | 4.22 (3.65–4.89) |
| 2007 | 859,730 | 950 | 11.05 (10.37–11.78) | 440,212 | 761 | 17.29 (16.10–18.56) | 419,518 | 189 | 4.51 (3.91–5.20) |
| 2008 | 859,891 | 996 | 11.58 (10.89–12.33) | 440,202 | 789 | 17.92 (16.72–19.22) | 419,689 | 207 | 4.93 (4.30–5.65) |
| 2009 | 851,996 | 1052 | 12.35 (11.62–13.12) | 435,757 | 835 | 19.16 (17.91–20.51) | 416,239 | 217 | 5.21 (4.56–5.96) |
| 2010 | 861,288 | 1157 | 13.43 (12.68–14.23) | 440,785 | 930 | 21.10 (19.79–22.50) | 420,503 | 227 | 5.40 (4.74–6.15) |
| 2011 | 862,136 | 1208 | 14.01 (13.24–14.82) | 441,393 | 982 | 22.25 (20.90–23.68) | 420,743 | 226 | 5.37 (4.71–6.12) |
| All | Female | Male | ||||
|---|---|---|---|---|---|---|
| RR (95% CI) | p Value | RR (95% CI) | p Value | RR (95% CI) | p Value | |
| Year (per 1 year) | 1.06 (1.05–1.07) | <0.0001 | 1.06 (1.05–1.07) | <0.0001 | 1.06 (1.05–1.08) | <0.0001 |
| Sex (ref: Male) | ||||||
| Female | 3.77 (3.58–3.96) | <0.0001 | - | - | ||
| Age(ref: 10–19 years old) | ||||||
| 20–29 | 6.34 (4.56–8.83) | <0.0001 | 8.08 (5.35–12.19) | <0.0001 | 3.28 (1.83–5.89) | <0.0001 |
| 30–39 | 16.61 (12.08–22.83) | <0.0001 | 21.37 (14.33–31.86) | <0.0001 | 8.24 (4.81–14.10) | <0.0001 |
| 40–49 | 39.22 (28.67–53.68) | <0.0001 | 50.42 (33.95–74.88) | <0.0001 | 19.57 (11.63–32.93) | <0.0001 |
| 50–59 | 73.71 (53.93–100.77) | <0.0001 | 91.8 (61.87–136.20) | <0.0001 | 43.29 (25.87–72.44) | <0.0001 |
| 60–69 | 110.97 (81.18–151.7) | <0.0001 | 133.47 (89.95–198.09) | <0.0001 | 74.90 (44.81–125.16) | <0.0001 |
| 70–79 | 105.67 (77.19–144.65) | <0.0001 | 123.24 (82.91–183.19) | <0.0001 | 77.08 (46.03–129.08) | <0.0001 |
| Residential urbanization (ref: Urban) | ||||||
| Sub-urban | 1.05 (1.00–1.09) | 0.0518 | 1.01 (0.96–1.06) | 0.7885 | 1.24 (1.13–1.37) | <0.0001 |
| Rural | 1.00 (0.93–1.07) | 0.9227 | 0.92 (0.85–1.00) | 0.0562 | 1.31 (1.14–1.50) | 0.0002 |
| Income (ref: <30,000) | ||||||
| 30,000–60,000 | 0.88 (0.83–0.94) | 0.0001 | 0.94 (0.88–1.01) | 0.1041 | 0.72 (0.63–0.83) | <0.0001 |
| ≥60,000 | 0.79 (0.70–0.89) | 0.0001 | 0.99 (0.85–1.14) | 0.8695 | 0.54 (0.43–0.68) | <0.0001 |
| All | Female | Male | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Py * | New Case | Incidence Rate * (95% CI) | Py * | New Case | Incidence Rate * (95% CI) | Py * | New Case | Incidence Rate * (95% CI) | |
| Year | |||||||||
| 2003 | 813,767 | 144 | 1.77 (1.50–2.08) | 416,574 | 103 | 2.47 (2.04–3.00) | 397,193 | 41 | 1.03 (0.76–1.4) |
| 2004 | 820,579 | 139 | 1.69 (1.43–2.00) | 419,077 | 100 | 2.39 (1.96–2.90) | 401,502 | 39 | 0.97 (0.71–1.33) |
| 2005 | 863,607 | 170 | 1.97 (1.69–2.29) | 438,407 | 134 | 3.06 (2.58–3.62) | 425,200 | 36 | 0.85 (0.61–1.17) |
| 2006 | 859,912 | 174 | 2.02 (1.74–2.35) | 438,793 | 128 | 2.92 (2.45–3.47) | 421,119 | 46 | 1.09 (0.82–1.46) |
| 2007 | 858,510 | 173 | 2.02 (1.74–2.34) | 439,262 | 134 | 3.05 (2.58–3.61) | 419,248 | 39 | 0.93 (0.68–1.27) |
| 2008 | 858,550 | 158 | 1.84 (1.57–2.15) | 439,152 | 109 | 2.48 (2.06–2.99) | 419,398 | 49 | 1.17 (0.88–1.55) |
| 2009 | 850,566 | 138 | 1.62 (1.37–1.92) | 434,646 | 100 | 2.30 (1.89–2.80) | 415,920 | 38 | 0.91 (0.66–1.26) |
| 2010 | 859,762 | 168 | 1.95 (1.68–2.27) | 439,594 | 138 | 3.14 (2.66–3.71) | 420,168 | 30 | 0.71 (0.50–1.02) |
| 2011 | 860,498 | 159 | 1.85 (1.58–2.16) | 440,107 | 125 | 2.84 (2.38–3.38) | 420,391 | 34 | 0.81 (0.58–1.13) |
| Age | |||||||||
| 16–19 | 1,218,345 | 17 | 0.14 (0.09–0.22) | 590,245 | 11 | 0.19 (0.10–0.34) | 628,100 | 6 | 0.10 (0.04–0.21) |
| 20–29 | 1,331,445 | 58 | 0.44 (0.34–0.56) | 735,024 | 48 | 0.65 (0.49–0.87) | 596,421 | 10 | 0.17 (0.09–0.31) |
| 30–39 | 1,469,061 | 145 | 0.99 (0.84–1.16) | 747,384 | 119 | 1.59 (1.33–1.91) | 721,677 | 26 | 0.36 (0.25–0.53) |
| 40–49 | 1,441,546 | 290 | 2.01 (1.79–2.26) | 720,385 | 232 | 3.22 (2.83–3.66) | 721,161 | 58 | 0.80 (0.62–1.04) |
| 50–59 | 1,127,002 | 376 | 3.34 (3.02–3.69) | 569,415 | 278 | 4.88 (4.34–5.49) | 557,587 | 98 | 1.76 (1.44–2.14) |
| 60–69 | 622,731 | 298 | 4.79 (4.27–5.36) | 323,433 | 213 | 6.59 (5.76–7.53) | 299,298 | 85 | 2.84 (2.30–3.51) |
| 70–79 | 435,621 | 239 | 5.49 (4.83–6.23) | 219,726 | 170 | 7.74 (6.66–8.99) | 215,895 | 69 | 3.20 (2.52–4.05) |
| Urbanization | |||||||||
| Urban | 4,745,237 | 843 | 1.78 (1.66–1.90) | 2,480,107 | 640 | 2.58 (2.39–2.79) | 2,265,130 | 203 | 0.90 (0.78–1.03) |
| Sub-urban | 2,267,357 | 436 | 1.92 (1.75–2.11) | 1,113,034 | 317 | 2.85 (2.55–3.18) | 1,154,323 | 119 | 1.03 (0.86–1.23) |
| Rural | 633,157 | 144 | 2.27 (1.93–2.68) | 312,471 | 114 | 3.65 (3.04–4.38) | 320,686 | 30 | 0.94 (0.65–1.34) |
| Income | |||||||||
| <30,000 | 6,067,440 | 1185 | 1.95 (1.84–2.07) | 3,253,211 | 902 | 2.77 (2.6–2.96) | 281,4229 | 283 | 1.01 (0.9–1.13) |
| 30,000–60,000 | 1,246,777 | 193 | 1.55 (1.34–1.78) | 559,822 | 142 | 2.54 (2.15–2.99) | 686,955 | 51 | 0.74 (0.56–0.98) |
| ≥60,000 | 331,534 | 45 | 1.36 (1.01–1.82) | 92,579 | 27 | 2.92 (2.00–4.25) | 238,955 | 18 | 0.75 (0.47–1.2) |
| All | Female | Male | ||||
|---|---|---|---|---|---|---|
| RR (95% CI) | p Value | RR (95% CI) | p Value | RR (95% CI) | p Value | |
| Year (per 1 year) | 0.99 (0.97–1.01) | 0.1752 | 0.99 (0.97–1.02) | 0.613 | 0.96 (0.92–1) | 0.0607 |
| Sex (ref: Male) | ||||||
| Female | 2.9 (2.57–3.27) | <0.0001 | - | - | - | - |
| Age(ref: 16–19 years old) | ||||||
| 20–29 | 2.98 (1.73–5.11) | <0.0001 | 3.55 (1.84–6.84) | 0.0002 | 1.8 (0.65–4.96) | 0.2552 |
| 30–39 | 7.19 (4.34–11.9) | <0.0001 | 8.73 (4.7–16.22) | <0.0001 | 4.16 (1.7–10.17) | 0.0017 |
| 40–49 | 14.79 (9.05–24.15) | <0.0001 | 17.63 (9.62–32.33) | <0.0001 | 9.36 (4.02–21.8) | <0.0001 |
| 50–59 | 24.43 (15.01–39.77) | <0.0001 | 26.76 (14.63–48.95) | <0.0001 | 20.61 (9–47.21) | <0.0001 |
| 60–69 | 33.61 (20.61–54.8) | <0.0001 | 35.41 (19.31–64.92) | <0.0001 | 31.44 (13.73–72) | <0.0001 |
| 70–79 | 38.55 (23.57–63.07) | <0.0001 | 41.06 (22.31–75.58) | <0.0001 | 34.18 (14.83–78.74) | <0.0001 |
| Residential urbanization (ref: Urban) | ||||||
| Sub-urban | 1.07 (0.96–1.21) | 0.2293 | 1.08 (0.94–1.23) | 0.2867 | 1.08 (0.86–1.35) | 0.5114 |
| Rural | 1.04 (0.87–1.24) | 0.6728 | 1.15 (0.94–1.41) | 0.1682 | 0.76 (0.52–1.12) | 0.1698 |
| Income (ref: ≥30,000) | ||||||
| 30,000–60,000 | 0.90 (0.77–1.06) | 0.2004 | 0.95 (0.79–1.14) | 0.5974 | 0.79 (0.58–1.08) | 0.1453 |
| ≥60,000 | 0.79 (0.59–1.08) | 0.1362 | 0.94 (0.64–1.38) | 0.7465 | 0.64 (0.39–1.04) | 0.0711 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, D.-H.; Huang, J.-Y.; Chiou, J.-Y.; Wei, J.C.-C. Analysis of Socioeconomic Status in the Patients with Rheumatoid Arthritis. Int. J. Environ. Res. Public Health 2018, 15, 1194. https://doi.org/10.3390/ijerph15061194
Yang D-H, Huang J-Y, Chiou J-Y, Wei JC-C. Analysis of Socioeconomic Status in the Patients with Rheumatoid Arthritis. International Journal of Environmental Research and Public Health. 2018; 15(6):1194. https://doi.org/10.3390/ijerph15061194
Chicago/Turabian StyleYang, Deng-Ho, Jing-Yang Huang, Jeng-Yuan Chiou, and James Cheng-Chung Wei. 2018. "Analysis of Socioeconomic Status in the Patients with Rheumatoid Arthritis" International Journal of Environmental Research and Public Health 15, no. 6: 1194. https://doi.org/10.3390/ijerph15061194
APA StyleYang, D.-H., Huang, J.-Y., Chiou, J.-Y., & Wei, J. C.-C. (2018). Analysis of Socioeconomic Status in the Patients with Rheumatoid Arthritis. International Journal of Environmental Research and Public Health, 15(6), 1194. https://doi.org/10.3390/ijerph15061194