Effect of Intermittent Energy Restriction on Flow Mediated Dilatation, a Measure of Endothelial Function: A Short Report




Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Methods
2.3. Dietary Intervention
2.4. Weight and Height
2.5. Flow Mediated Dilatation
2.6. FMD Analysis
2.7. Blood Pressure
2.8. Laboratory Analysis
2.9. Ethics
2.10. Statistical Analysis
3. Results
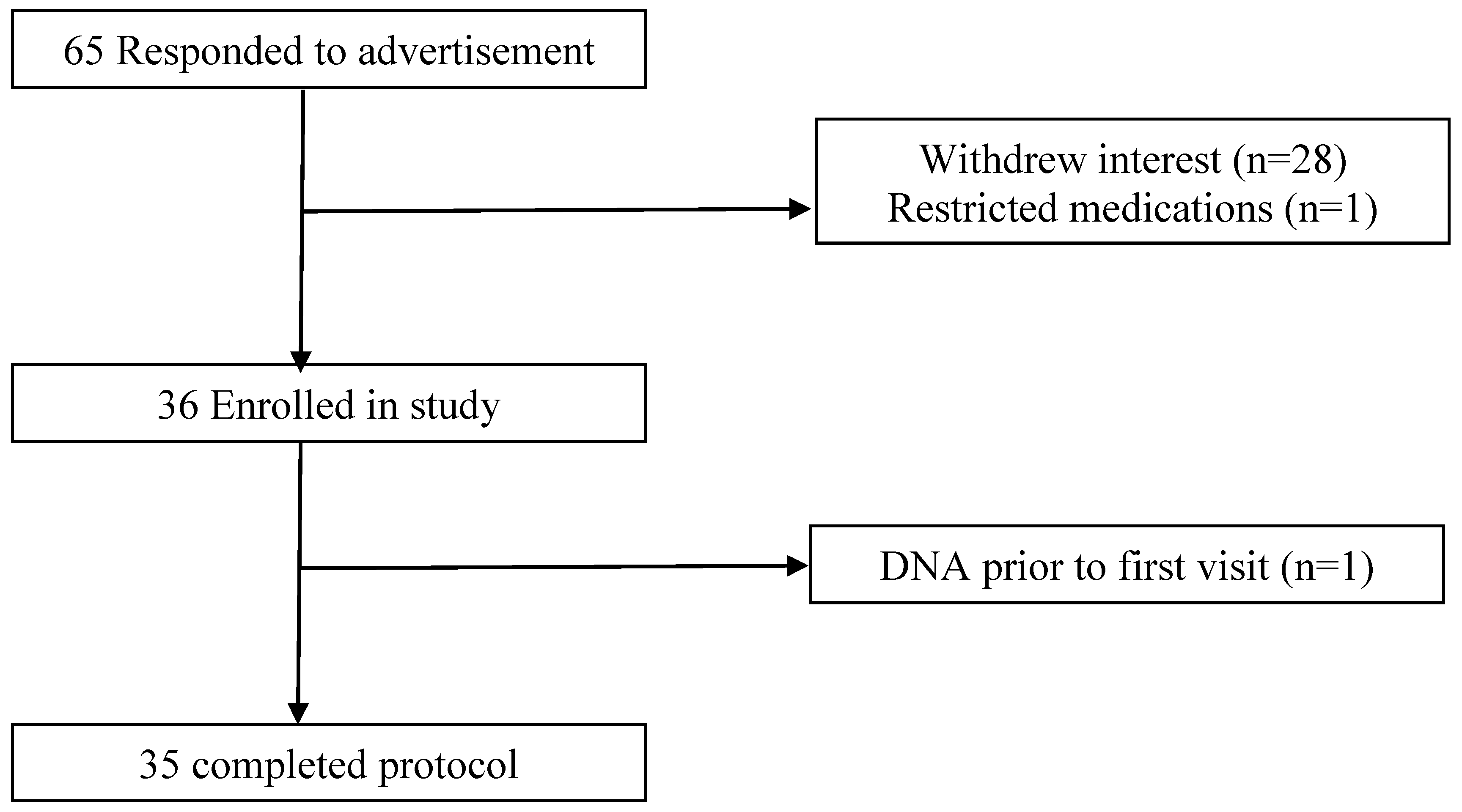
3.1. Subjects
3.2. Weight Loss
3.3. Brachial Artery Endothelial Function and Blood Pressure
3.4. Biochemical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hubert, H.B.; Feinleib, M.; McNamara, P.M.; Castelli, W.P. Obesity as an independent risk factor for cardiovascular disease: A 26-year follow-up of participants in the Framingham Heart Study. Circulation 1983, 67, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.F.; D’Agostino, D.P.; Sullivan, L.; Parise, H.; Kannel, W.B. Overweight and obesity as determinants of cardiovascular risk. The Framingham experience. Arch. Intern. Med. 2002, 162, 1867–1872. [Google Scholar] [CrossRef] [PubMed]
- Schachinger, V.; Britten, M.B.; Zeiher, A.M. Prognostic impact of coronary vasodilation dysfunction on adverse long-term outcome of coronary heart disease. Circulation 2000, 101, 1899–1906. [Google Scholar] [CrossRef] [PubMed]
- Van Gaal, L.F.; Mertens, I.L.; De Block, C.E. Mechanisms linking obesity with cardiovascular disease. Nature 2006, 444, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Joris, P.J.; Zeegers, M.P.; Mensink, R.P. Weight loss improves fasting flow-mediated vasodilation in adults: A meta-analysis of intervention studies. Atherosclerosis 2015, 239, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Karbowska, J.; Kochan, Z. Intermittent fasting up-regulates Fsp27/Cidec gene expression in white adipose tissue. Nutrition 2012, 28, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Kyrou, I.; Kumar, S. Weight management in overweight and obese patients with type 2 diabetes mellitus. Br. J. Diabetes Vasc. Dis. 2010, 10, 274–283. [Google Scholar] [CrossRef]
- Headland, M.; Clifton, P.M.; Carter, S.; Keogh, J.B. Weight loss outcomes: A systematic review and meta-analysis of intermittent energy restriction trials lasting a minimum of 6 months. Nutrients 2016, 8, 354. [Google Scholar] [CrossRef] [PubMed]
- Seimon, R.V.; Roekenes, J.A.; Zibellini, J.; Zhu, B.; Gibson, A.A.; Hills, A.P.; Wood, R.E.; King, N.A.; Byrne, N.M.; Sainsbury, A. Do intermittent diets provide physiological benefits over continuous diets for weight loss? A systematic review of clinical trials. Mol. Cell. Endocrinol. 2015, 418, 153–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoni, R.; Johnston, K.L.; Collins, A.L.; Robertson, M.D. The effects of intermittent energy restriction on indices of cardiometabolic health. Res. Endocrinol. 2014, 2014, 1–24. [Google Scholar] [CrossRef]
- Antoni, R.; Johnston, K.L.; Collins, A.L.; Robertson, M.D. Investigation into the acute effects of total and partial energy restriction on postprandial metabolism among overweight/obese participants. Br. J. Nutr. 2016, 115, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chen, J.A.; Bergmann, S.R. Prediction of future cardiovascular outcomes by flow-mediated vasodilation of brachial artery: A meta-analysis. Int. J. Cardiovasc. Imaging 2010, 26, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Bull, C.; Robinson, J.; Deanfield, J.E. Endothelium-dependent dilation in the systemic arteries of asymptomatic subjects relates to coronary risk factors and their interaction. J. Am. Coll. Cardiol. 1994, 24, 1468–1474. [Google Scholar] [CrossRef]
- Raitakari, O.T.; Celermajer, D.S. Flow-mediated dilatation. Br. J. Clin. Pharmacol. 2000, 50, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Ras, R.T.; Streppel, M.T.; Draijer, R.; Zock, P.L. Flow mediated dilation and cardiovascular risk prediction: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 168, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Brinkworth, G.D.; Keogh, J.B.; Noakes, M.; Buckley, J.D.; Clifton, P.M. Long-term effects of weight loss with a very low carbohydrate and low fat diet on vascular function in overweight and obese patients. J. Intern. Med. 2010, 267, 452–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, S.E.; Mulla, U.Z.; Chowiencyzk, P.J.; Sanders, T.A. Increased potassium intake from fruit and vegetables or supplements does not lower blood pressure or improve vascular function in UK men and women with early hypertension: A randomised controlled trial. Br. J. Nutr. 2010, 104, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; Klempel, M.; Kroeger, C.M.; Trepanowski, J.F.; Phillips, S.A.; Norkeviciute, E.; Varady, K.A. Alternate day fasting with or without exercise: Effects on endothelial function and adipokines in obese humans. e-SPEN J. 2013, 8, e205–e209. [Google Scholar] [CrossRef]
- Williams, I.L.; Wheatcroft, S.B.; Sha, A.M.; Kearney, M.T. Obesity, atherosclesosis and the vascular endothelium: Mechanisms of reduced nitric oxide bioavailability in obese humans. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Title, L.M.; Cummings, A.A.; Giddens, K.; Nassar, B.A. Oral glucose loading acutely attenuates endothelium-dependent vasodilation in healthy adults without diabetes: An effect prevented by vitamins C and E. J. Am. Coll. Cardiol. 2000, 36, 2185–2191. [Google Scholar] [CrossRef]
- Williams, S.B.; Goldfine, A.B.; Timimi, F.K.; Ting, H.H.; Roddy, M.A.; Simonson, D.C.; Creager, M.A. Acute hyperglycemia attenuates endothelium-dependent vasodilation in humans in vivo. Circulation 1998, 97, 1695–1701. [Google Scholar] [CrossRef] [PubMed]
- Beckman, J.A.; Goldfine, A.B.; Gordon, M.B.; Creager, M.A. Ascorbate restores endothelium-dependent vasodilation impaired by acute hyperglycemia in humans. Circulation 2001, 103, 1618–1623. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Hishikawa, K.; Katusic, Z.S.; Luscher, T.F. High glucose increases nitric oxide synthase expression and superoxide anion generation in human aortic endothelial cells. Circulation 1997, 96, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Christ, M.; Bauersachs, J.; Liebetrau, C.; Heck, M.; Gunther, A.; Wehling, M. Glucose increases endothelial-dependent superoxide formation in coronary arteries by NAD(P)H oxidase activation: Attenuation by the 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor atorvastatin. Diabetes 2002, 52, 2648–2652. [Google Scholar] [CrossRef]
- Bucala, R.; Tracey, K.J.; Cerami, A. Advanced glycosylation products quench nitric oxide and mediate defective endothelium-dependent vasodilatation in experimental diabetes. J. Clin. Investig. 1991, 87, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, S.V.; Morrishow, A.M.; Dharia, N.; Gross, S.S.; Goligorsky, M.S. Glucose scavenging of nitric oxide. Am. J. Physiol. Renal Physiol. 2001, 280, F480–F486. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.J.; Miyake, Y.; Grahame, C.; Di Tullio, M.R.; Sciacca, R.R.; Boden-Albala, B.; Sacco, R.L.; Homma, S. Relation of plasma glucose and endothelial function in a population of multiethnic sample of subjects without diabetes mellitus. Am. J. Cardiol. 2005, 96, 1273–1277. [Google Scholar] [CrossRef] [PubMed]
- Raitakari, M.; Ilvonen, T.; Ahotupa, M.; Lehtimaki, T.; Harmoinen, A.; Suominen, P.; Elo, J.; Hartiala, J.; Raitakari, O.T. Weight reduction with very-low-caloric diet and endothelial function in overweight adults: Role of plasma glucose. Arterioscler. Throm. Vasc. Biol. 2004, 24, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Clifton, P.M.; Keogh, J.B.; Foster, P.R.; Noakes, M. Effect of weight loss on inflammatory and endothelial markers and FMD using two low-fat diets. Int. J. Obes. 2005, 29, 1445–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergholm, R.; Tiikkainen, M.; Vehkavaara, S.; Tamminen, M.; Teramo, K.; Rissanen, A.; Yki-Jarvinen, H. Lowering of LDL cholesterol rather than moderate weight loss improves endothelium-dependent vasodilatation in obese women with previous gestational diabetes. Diabetes Care 2003, 26, 1667–1672. [Google Scholar] [CrossRef] [PubMed]
- Brook, A.D. Obesity, weight loss, and vascular function. Endocrine 2006, 29, 21–25. [Google Scholar] [CrossRef]
- Keogh, J.B.; Grieger, J.A.; Noakes, M.; Clifton, P.M. Flow-mediated dilatation is impaired by a high-saturated fat diet but not by a high-carbohydrate diet. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1274–1279. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, K.M.; Clifton, P.M.; Keogh, J.B. Endothelial function is impaired after a high-salt meal in healthy subjects. Am. J. Clin. Nutr. 2011, 93, 500–555. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, K.L.; Racine, M.L.; Geolfos, C.J.; Gates, P.E.; Chonchol, M.; McQueen, M.B.; Seals, D.R. Dietary sodium restriction reverses vascular endothelial dysfunction in middle-aged/older adults with moderately elevated systolic blood pressure. J. Am. Coll. Cardiol. 2013, 61, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, K.M.; Clifton, P.M.; Keogh, J.B. A reduction of 3 g/day from a usual 9 g/day salt diet improves endothelial function and decreases endothelin-1 in a randomised cross_over study in normotensive overweight and obese subjects. Atherosclerosis 2014, 233, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Blanch, N.; Clifton, P.M.; Petersen, K.S.; Willoughby, S.R.; Keogh, J.B. Effect of high potassium diet on endothelial function. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Blanch, N.; Clifton, P.M.; Keogh, J.B. Postprandial effects of potassium supplementation on vascular function and blood pressure: A randomised cross-over study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Blanch, N.; Clifton, P.M.; Peterson, K.S.; Keogh, J.B. Effect of sodium and potassium supplementation on vascular and endothelial function: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 101, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Dharmashankar, K.; Widlansky, M.E. Vascular endothelial function and hypertension: Insights and directions. Curr. Hypertens. Rep. 2010, 12, 448–455. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age, y | 46.5 ± 17.5 |
| Height, m | 1.7 ± 0.1 |
| Weight, kg | 72.1 ± 16.7 |
| BMI, kg/m2 | 26.0 ± 5.5 |
| SBP, mm Hg | 118 ± 16 |
| DBP, mm Hg | 75 ± 11 |
| Baseline diameter, mm | 4.1 ± 1.0 |
| Brachial artery diameter change, mm | 0.3 ± 0.1 |
| FMD, % | 8.2 ± 2.4 |
| Glucose, mmol/L | 5.2 ± 0.8 |
| Nutrient | Male | Female |
|---|---|---|
| Energy (cal) | 442 ± 104 | 369 ± 71 |
| Protein (g) | 34 ± 6 | 29 ± 6 |
| Total fat (g) | 12 ± 6 | 12 ± 5 |
| Saturated Fat (g) | 4 ± 3 | 4 ± 2 |
| Carbohydrate (g) | 43 ± 13 | 31 ± 9 |
| Sugars (g) | 28 ± 5 | 24 ± 7 |
| Fibre (g) | 14 ± 6 | 11 ± 4 |
| Sodium (mg) | 387 ± 222 | 392 ± 245 |
| Potassium (mg) | 1452 ± 261 | 1258 ± 220 |
| Iron (mg) | 4 ± 1 | 3 ± 1 |
| Zinc (mg) | 3 ± 1 | 3 ± 1 |
| Magnesium (mg) | 127 ± 37 | 99 ± 21 |
| Calcium (mg) | 355 ± 106 | 272 ± 74 |
| 2 ER Days | 2 HB Days | p-Value 2 | |
|---|---|---|---|
| Baseline diameter, mm | 4.0 ± 0.9 | 4.0 ± 0.8 | 0.7 |
| Absolute change in artery diameter, mm | 0.3 ± 0.02 | 0.3 ± 0.02 | 0.5 |
| FMD, % | 8.6 ± 0.4 | 8.3 ± 0.5 | 0.7 |
| SBP, mm Hg | 115 ± 12 | 118 ± 15 | 0.2 |
| DBP, mm Hg | 74 ± 9 | 73 ± 11 | 0.8 |
| Glucose, mmol/L * | 5.0 ± 0.7 | 5.1 ± 0.6 | 0.2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Headland, M.L.; Clifton, P.M.; Keogh, J.B. Effect of Intermittent Energy Restriction on Flow Mediated Dilatation, a Measure of Endothelial Function: A Short Report. Int. J. Environ. Res. Public Health 2018, 15, 1166. https://doi.org/10.3390/ijerph15061166
Headland ML, Clifton PM, Keogh JB. Effect of Intermittent Energy Restriction on Flow Mediated Dilatation, a Measure of Endothelial Function: A Short Report. International Journal of Environmental Research and Public Health. 2018; 15(6):1166. https://doi.org/10.3390/ijerph15061166
Chicago/Turabian StyleHeadland, Michelle L., Peter M. Clifton, and Jennifer B. Keogh. 2018. "Effect of Intermittent Energy Restriction on Flow Mediated Dilatation, a Measure of Endothelial Function: A Short Report" International Journal of Environmental Research and Public Health 15, no. 6: 1166. https://doi.org/10.3390/ijerph15061166