Do Physical Activity Friendly Neighborhoods Affect Community Members Equally? A Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Physical Activity and Sedentary Behavior
2.3. Personal Characteristics–Socio-Demographic Characteristics and Health-Related Quality of Life
2.4. Environmental Characteristics
2.5. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
3.2. Physical Activity Levels
3.3. Neighborhood Environment Walkability Scale
3.4. Associations between SB, LPA, MVPA and Personal and Environmental Characteristics
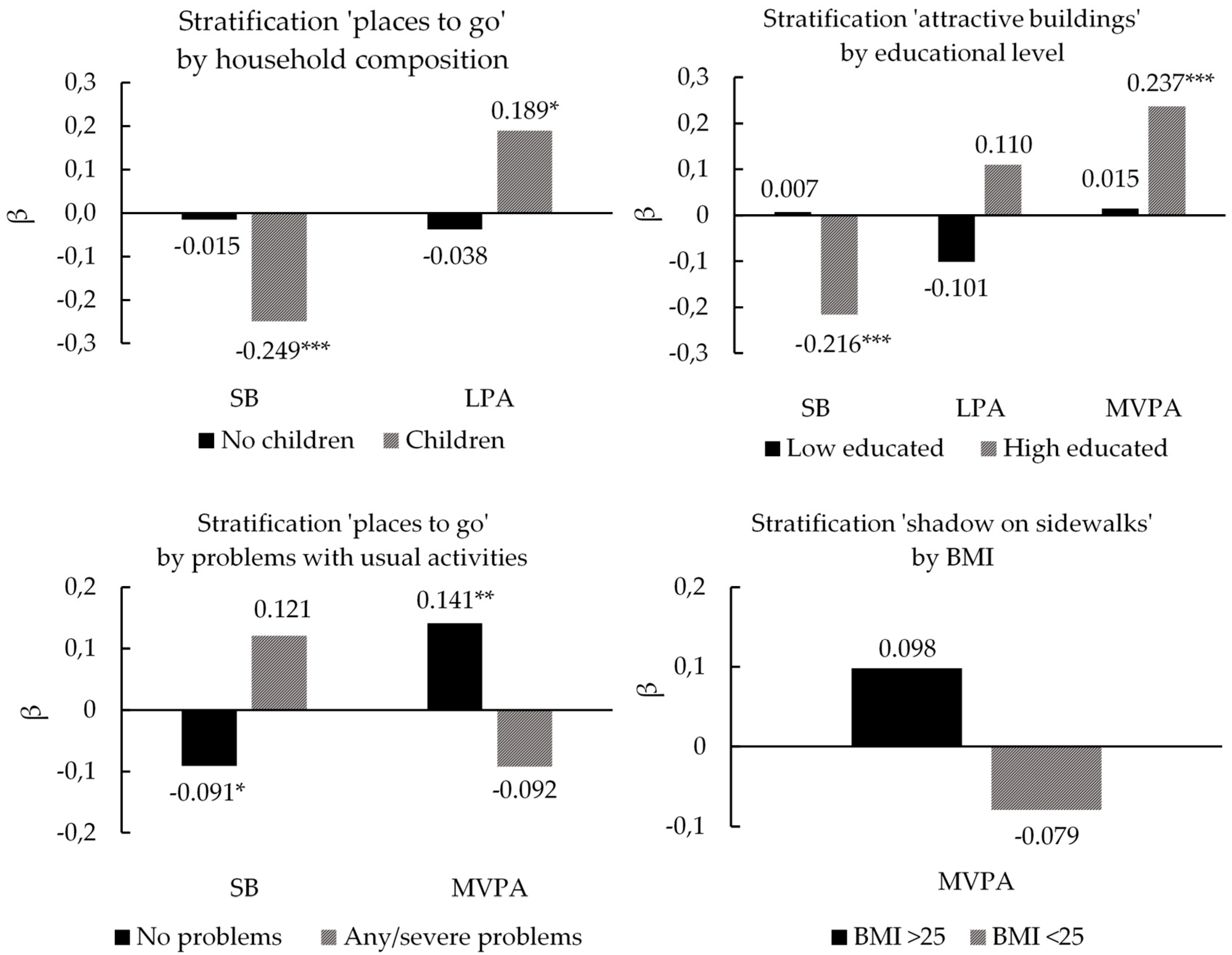
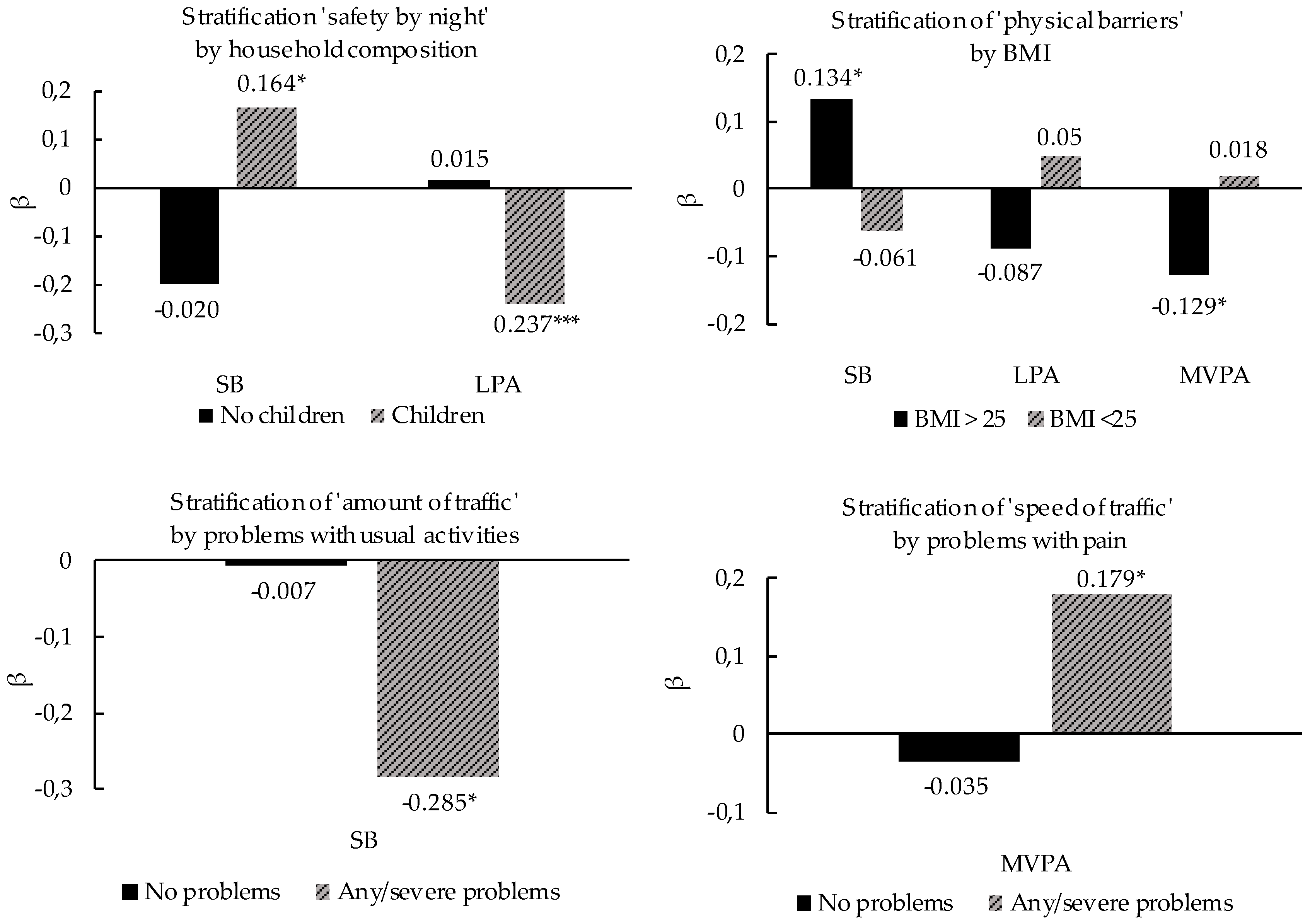
3.5. Interactions between Personal and Environmental Characteristics
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Haeberer, M.; Noguer, I.; Mujica, O.J. Educational inequalities in mortality and survival of women and men in the Americas, 1990–2010. Rev. Panam. Salud Publica 2015, 38, 89–95. [Google Scholar] [PubMed]
- Reques, L.; Giráldez-García, C.; Miqueleiz, E.; Belza, M.J.; Regidor, E. Educational differences in mortality and the relative importance of different causes of death: A 7-year follow-up study of Spanish adults. J. Epidemiol. Community Health 2014, 68, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Van der Noordt, M.; IJzelenberg, H.; Droomers, M.; Proper, K.I. Health effects of employment: A systematic review of prospective studies. Int. J. Occup. Environ. Med. 2014, 10, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R.; Mohammed, S.A. Discrimination and racial disparities in health: Evidence and needed research. J. Behav. Med. 2009, 32, 20–47. [Google Scholar] [CrossRef] [PubMed]
- Stringhini, S.; Sabia, S.; Shipley, M.; Brunner, E.; Nabi, H.; Kivimaki, M.; Singh-Manoux, A. Association of socioeconomic position with health behaviors and mortality. JAMA 2010, 303, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Bauman, A.; Brown, W. Too much sitting: A novel and important predictor of chronic disease risk? Br. J. Sports Med. 2009, 43, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Devaux, M.; Sassi, F. Social inequalities in obesity and overweight in 11 OECD countries. Eur. J. Public Health 2013, 23, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Mackenbach, J.D.; Lakerveld, J.; van Lenthe, F.J.; Bardos, H.; Glonti, K.; Compernolle, S.; De Bourdeaudhuij, I.; Oppert, J.M.; Roda, C.; Rutter, H.; et al. Exploring why residents of socioeconomically deprived neighbourhoods have less favourable perceptions of their neighbourhood environment than residents of wealthy neighbourhoods. Obes. Rev. 2016, 17 (Suppl. 1), 42–52. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; Mytton, O.; White, M.; Monsivais, P. Why are some population interventions for diet and obesity more equitable and effective than others? The role of individual agency. PLoS Med. 2016, 13, e1001990. [Google Scholar] [CrossRef]
- Capewell, S.; Graham, H. Will cardiovascular disease prevention widen health inequalities? PLoS Med. 2010, 7, e1000320. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Dill, J.; Mohr, C. The objective versus the perceived environment: What matters for bicycling? Transportation 2014, 41, 1135–1152. [Google Scholar] [CrossRef]
- Cerin, E.; Cain, K.L.; Conway, T.L.; Van Dyck, D.; Hinckson, E.; Schipperijn, J.; De Bourdeaudhuij, I.; Owen, N.; Davey, R.C.; Hino, A.A.F. Neighborhood environments and objectively measured physical activity in 11 countries. Med. Sci. Sports Exerc. 2014, 46, 2253. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Conway, T.L.; Dillon, L.I.; Frank, L.D.; Adams, M.A.; Cain, K.L.; Saelens, B.E. Environmental and demographic correlates of bicycling. J. Prev. Med. 2013, 57, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, D.; Cerin, E.; Conway, T.L.; De Bourdeaudhuij, I.; Owen, N.; Kerr, J.; Cardon, G.; Frank, L.D.; Saelens, B.E.; Sallis, J.F. Associations between perceived neighborhood environmental attributes and adults’ sedentary behavior: Findings from the U.S.A., Australia and Belgium. Soc. Sci. Med. 2012, 74, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Foster, S.; Giles-Corti, B. The built environment, neighborhood crime and constrained physical activity: An exploration of inconsistent findings. J. Prev. Med. 2008, 47, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Hosking, J.; Woodward, A.; Witten, K.; MacMillan, A.; Field, A.; Baas, P.; Mackie, H. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 158. [Google Scholar] [CrossRef] [PubMed]
- Mariela, A.A. To Walk or Not to Walk? The Hierarchy of Walking Needs. Environ. Behav. 2005, 37, 808–836. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357. [Google Scholar] [CrossRef] [PubMed]
- Wolff-Hughes, D.L.; Troiano, R.P.; Boyer, W.R.; Fitzhugh, E.C.; McClain, J.J. Use of population-referenced total activity counts percentiles to assess and classify physical activity of population groups. J. Prev. Med. 2016, 87, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. Med. Sci. Sports Exerc. 2011, 14, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Farías, N.; Brown, W.J.; Peeters, G.M.E.E. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. Med. Sci. Sports Exerc. 2014, 17, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef] [PubMed]
- EuroQol, G. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199. [Google Scholar] [CrossRef]
- Neighborhood Environment Walkability Scale-Abbreviated (NEWS-A): Sample Survey. Available online: http://sallis.ucsd.edu/Documents/Measures_documents/NEWS_A.pdf (accessed on 16 May 2018).
- Cerin, E.; Conway, T.L.; Saelens, B.E.; Frank, L.D.; Sallis, J.F. Cross-validation of the factorial structure of the Neighborhood Environment Walkability Scale (NEWS) and its abbreviated form (NEWS-A). Int. J. Behav. Nutr. Phys. Act. 2009, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Friederichs, S.A.; Kremers, S.P.; Lechner, L.; de Vries, N.K. Neighborhood walkability and walking behavior: The moderating role of action orientation. J. Phys. Act. Health 2013, 10, 515–522. [Google Scholar] [CrossRef] [PubMed]
- De Bourdeaudhuij, I.; Sallis, J.F.; Saelens, B.E. Environmental correlates of physical activity in a sample of Belgian adults. Am. J. Health Promot. 2003, 18, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Bize, R.; Johnson, J.A.; Plotnikoff, R.C. Physical activity level and health-related quality of life in the general adult population: A systematic review. J. Prev. Med. 2007, 45, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Anokye, N.K.; Trueman, P.; Green, C.; Pavey, T.G.; Taylor, R.S. Physical activity and health related quality of life. BMC Public Health 2012, 12, 624. [Google Scholar] [CrossRef] [PubMed]
- Christian, H.; Giles-Corti, B.; Knuiman, M.; Timperio, A.; Foster, S. The influence of the built environment, social environment and health behaviors on body mass index. Results from RESIDE. Prev. Med. 2011, 53, 57–60. [Google Scholar] [CrossRef] [PubMed]
- O’Donoghue, G.; Perchoux, C.; Mensah, K.; Lakerveld, J.; van der Ploeg, H.; Bernaards, C.; Chastin, S.F.; Simon, C.; O’Gorman, D.; Nazare, J.A. A systematic review of correlates of sedentary behaviour in adults aged 18–65 years: A socio-ecological approach. BMC Public Health 2016, 16, 163. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Heneweer, H.; Vanhees, L.; Picavet, H.S.J. Physical activity and low back pain: A U-shaped relation? Pain 2009, 143, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Nyunt, M.S.Z.; Shuvo, F.K.; Eng, J.Y.; Yap, K.B.; Scherer, S.; Hee, L.M.; Chan, S.P.; Ng, T.P. Objective and subjective measures of neighborhood environment (NE): Relationships with transportation physical activity among older persons. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 108. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Humpel, N.; Leslie, E.; Bauman, A.; Sallis, J.F. Understanding environmental influences on walking: Review and research agenda. Am. J. Prev. Med. 2004, 27, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Compernolle, S.; De Cocker, K.; Roda, C.; Oppert, J.M.; Mackenbach, J.D.; Lakerveld, J.; Glonti, K.; Bardos, H.; Rutter, H.; Cardon, G.; et al. Physical Environmental Correlates of Domain-Specific Sedentary Behaviours across Five European Regions (the SPOTLIGHT Project). PLoS ONE 2016, 11, e0164812. [Google Scholar] [CrossRef] [PubMed]
- Mason, P.; Kearns, A.; Livingston, M. “Safe Going”: The influence of crime rates and perceived crime and safety on walking in deprived neighbourhoods. Soc. Sci. Med. 2013, 91, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Carlson, J.A.; Bracy, N.L.; Sallis, J.F.; Millstein, R.A.; Saelens, B.E.; Kerr, J.; Conway, T.L.; Frank, L.D.; Cain, K.L.; King, A.C. Sociodemographic Moderators of Relations of Neighborhood Safety to Physical Activity. Med. Sci. Sports Exerc. 2014, 46, 1554–1563. [Google Scholar] [CrossRef] [PubMed]
- Mertens, L.; Compernolle, S.; Deforche, B.; Mackenbach, J.D.; Lakerveld, J.; Brug, J.; Roda, C.; Feuillet, T.; Oppert, J.-M.; Glonti, K.; et al. Built environmental correlates of cycling for transport across Europe. Health Place 2017, 44, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.; Ettema, D.; Pierik, F.; Dijst, M. Sports Facilities, Shopping centers or homes: What locations are important for adults’ physical activity? A cross-sectional study. Int. J. Environ. Res. Public Health 2016, 13, 287. [Google Scholar] [CrossRef] [PubMed]
- Luzak, A.; Heier, M.; Thorand, B.; Laxy, M.; Nowak, D.; Peters, A.; Schulz, H.; Group, K.-S. Physical activity levels, duration pattern and adherence to WHO recommendations in German adults. PLoS ONE 2017, 12, e0172503. [Google Scholar] [CrossRef] [PubMed]
- Pfister, T.; Matthews, C.E.; Wang, Q.; Kopciuk, K.A.; Courneya, K.; Friedenreich, C. Comparison of two accelerometers for measuring physical activity and sedentary behaviour. BMJ Open Sport Exerc. Med. 2017, 3, e000227. [Google Scholar] [CrossRef] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Nyström, C.D.; Mora-Gonzalez, J.; Löf, M.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Stone-Romero, E.F.; Liakhovitski, D. Strategies for detecting moderator variables: A review of conceptual and empirical issues. Res. Pers. Hum. Resour. Manag. 2002, 21, 333–372. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Socio-Demographic Characteristics (n = 622) | %/Mean (±SD) |
| Gender (% Males) | 46% |
| Age (years) | 57.3 (15.6) |
| Educational level (% Higher educated) * | 54% |
| Work status (% Employed) | 48% |
| Ethnicity (% Western) | 98% |
| Household composition | |
| without children | 76% |
| with children | 24% |
| Body Mass Index (kg/m2) | 24.9 (4.2) |
| Health-related quality of life (n = 622) | |
| Mobility | |
| no problems | 88% |
| moderate problems | 12% |
| extreme problems | 0% |
| Self-care | |
| no problems | 99% |
| moderate problems | 1% |
| extreme problems | <1% |
| Usual activities | |
| no problems | 90% |
| moderate problems | 10% |
| extreme problems | <1% |
| Pain/discomfort | |
| no problems | 69% |
| moderate problems | 30% |
| extreme problems | 1% |
| Anxiety/depression | |
| no problems | 90% |
| moderate problems | 9% |
| extreme problems | 1% |
| Physical Activity Levels (n = 622) | % (±SD) | Mean minutes/Day (±SD) |
|---|---|---|
| Wear time | 868.5 (196.0) | |
| Vector magnitude | ||
| % Sedentary behavior | 65.4 (7.8) | 567.5 (98.1) |
| % Light physical activity | 26.1 (6.2) | 227.5 (64.0) |
| % Moderate-to-vigorous physical activity | 8.4 (3.7) | 73.4 (34.0) |
| Vertical axis | ||
| % Sedentary behavior | 74.7 (6.2) | 647.7 (99.7) |
| % Light physical activity | 19.9 (5.3) | 173.4 (53.5) |
| % Moderate-to-vigorous physical activity | 5.5 (4.9) | 47.4 (25.7) |
| Scale | Variable | Mean * (±SD) |
|---|---|---|
| PA facilitating characteristics | ||
| Access to facilities | Stores within easy walking distance | 3.5 (0.7) |
| Many places within walking distance | 3.2 (0.7) | |
| Easy to walk to transit stop (bus, train) | 3.4 (0.7) | |
| Infrastructure and safety for walking | Cars dividing sidewalk and traffic | 2.9 (0.6) |
| Grass/dirt dividing sidewalk and traffic | 2.0 (0.7) | |
| Street lights | 3.1 (0.5) | |
| Walkers and bikers easily seen | 3.0 (0.5) | |
| Crosswalks and pedestrian signals | 2.6 (0.8) | |
| Aesthetics | Trees | 3.1 (0.8) |
| Many interesting things to look at | 2.5 (0.7) | |
| Many attractive natural sights | 2.6 (0.8) | |
| Attractive buildings/homes | 2.5 (0.8) | |
| PA hindering characteristics | ||
| Traffic hazards | Amount of traffic | 2.0 (0.7) |
| Speed of traffic | 2.0 (0.7) | |
| Drivers exceed posted limits | 2.7 (0.8) | |
| Crime | High crime rate | 2.9 (0.6) |
| Crime rate makes it unsafe during the day | 3.3 (0.6) | |
| Crime rate makes it unsafe at night | 3.0 (0.7) | |
| Lack of parking | Parking is difficult | 2.1 (0.8) |
| Hilliness | Hilliness | 3.4 (0.6) |
| Physical barriers | Physical barriers | 3.4 (0.7) |
| Variables | SB | LPA | MVPA | |||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |
| β | β | β | β | β | β | |
| Personal characteristics | ||||||
| Gender-female (REF = male) | −0.156 *** | −0.154 *** | 0.199 *** | 0.199 *** | ||
| Age | 0.158 *** | 0.158 *** | −0.132 ** | −0.141 ** | ||
| Body Mass Index | 0.182 *** | 0.177 *** | −0.179 *** | −0.179 *** | −0.127 ** | −0.115 ** |
| Educational level-low (REF = high) | −0.182 *** | −0.195 *** | 0.139 *** | 0.139 *** | 0.122 ** | 0.120 ** |
| Household composition-with child (ren) (REF = no children) | −0.139 *** | −0.130 ** | 0.184 *** | 0.184 *** | ||
| Self-care-any problems (REF = no problems) | 0.150 *** | 0.150 *** | −0.113 ** | −0.113 ** | −0.104 ** | −0.099 * |
| Usual activities-any problems (REF = no problems) | −0.158 ** | −0.160 *** | ||||
| Pain-any problems (REF = no problems) | 0.100 * | 0.102 * | ||||
| Explained variance (R2) | 0.143 | 0.150 | 0.078 | |||
| Environmental characteristics | ||||||
| Places to go within walking distance (higher score, more places to go) | 0.106 ** | |||||
| Attractive buildings (higher score, more attractive buildings) | −0.086 ** | 0.118 ** | ||||
| Crime (higher score, less crime) | −0.092 * | |||||
| Explained variance (R2) | 0.150 | 0.150 | 0.113 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stappers, N.E.H.; Van Kann, D.H.H.; De Vries, N.K.; Kremers, S.P.J. Do Physical Activity Friendly Neighborhoods Affect Community Members Equally? A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1062. https://doi.org/10.3390/ijerph15061062
Stappers NEH, Van Kann DHH, De Vries NK, Kremers SPJ. Do Physical Activity Friendly Neighborhoods Affect Community Members Equally? A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2018; 15(6):1062. https://doi.org/10.3390/ijerph15061062
Chicago/Turabian StyleStappers, Nicole E. H., Dave H. H. Van Kann, Nanne K. De Vries, and Stef P. J. Kremers. 2018. "Do Physical Activity Friendly Neighborhoods Affect Community Members Equally? A Cross-Sectional Study" International Journal of Environmental Research and Public Health 15, no. 6: 1062. https://doi.org/10.3390/ijerph15061062
APA StyleStappers, N. E. H., Van Kann, D. H. H., De Vries, N. K., & Kremers, S. P. J. (2018). Do Physical Activity Friendly Neighborhoods Affect Community Members Equally? A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 15(6), 1062. https://doi.org/10.3390/ijerph15061062