Evidencing Protective and Risk Factors for Harmful Alcohol Drinking in Adolescence: A Prospective Analysis of Sport-Participation and Scholastic-Achievement in Older Adolescents from Croatia


 ,
,
Abstract
1. Introduction
2. Materials and Methods
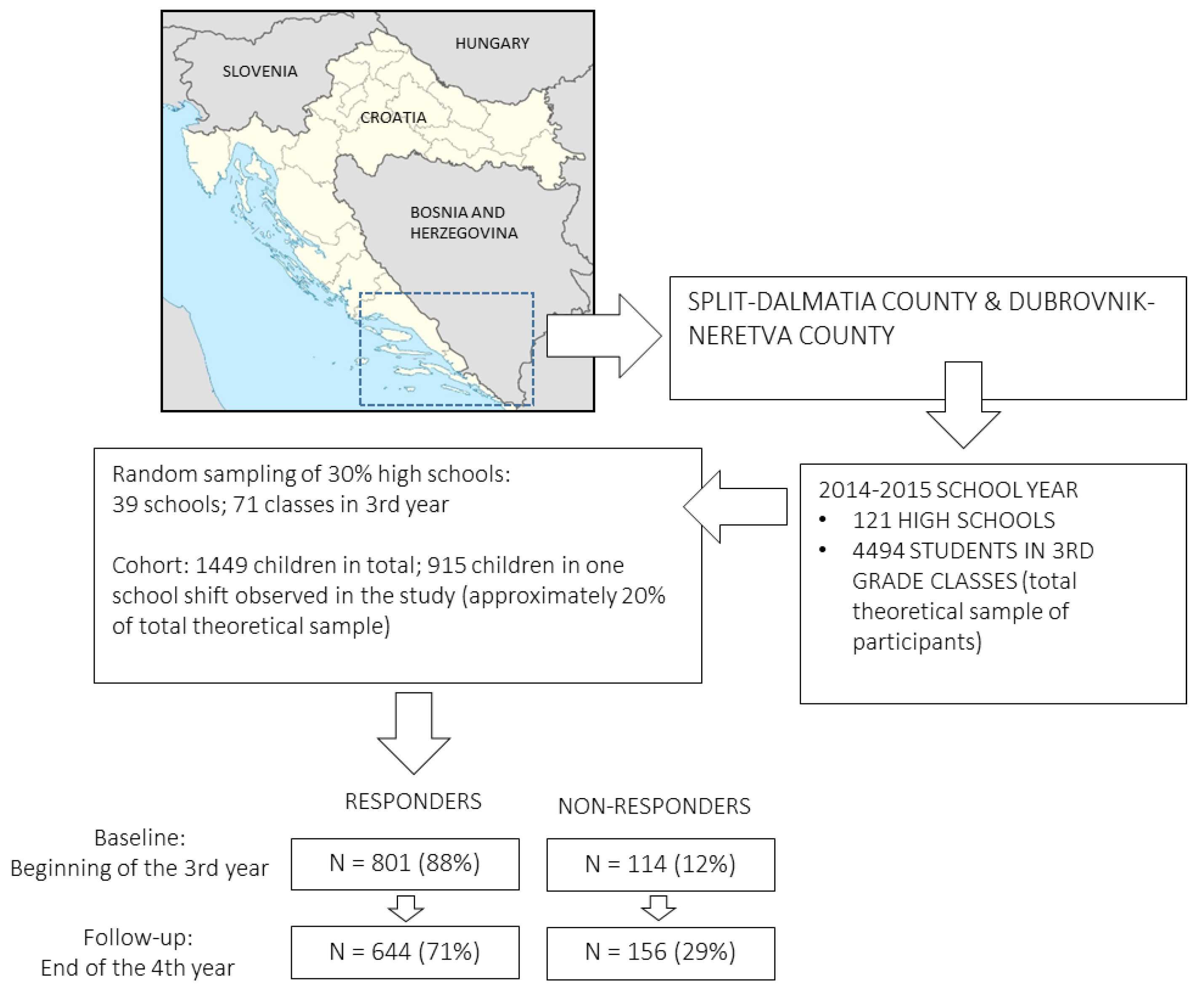
2.1. Participants and Testing
2.2. Variables
2.3. Statistics
3. Results
4. Discussion
4.1. Prevalence of Harmful Drinking
4.2. Sport Factors and Harmful Drinking
4.3. Scholastic Variables and Harmful Drinking
4.4. Study Limitations and Strengths
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Pulido, J.; Indave-Ruiz, B.I.; Colell-Ortega, E.; Ruiz-Garcia, M.; Bartroli, M.; Barrio, G. Population-based studies on alcohol-related harm in spain. Rev. Espanola Salud Publica 2014, 88, 493–513. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.N.; Raetz, A.; Harte, M.; McMahon, L.E.; Grandsoult, V.; Garcia-Filion, P.; Notrica, D.M. Pediatric trauma patient alcohol screening: A 3 year review of screening at a level i pediatric trauma center using the crafft tool. J. Pediatr. Surg. 2014, 49, 330–332. [Google Scholar] [CrossRef] [PubMed]
- O‘Meara, C.; Witherspoon, R.; Hapangama, N.; Hyam, D.M. Alcohol and interpersonal violence may increase the severity of facial fracture. Br. J. Oral Maxillofac. Surg. 2012, 50, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Swahn, M.H.; Culbreth, R.E.; Staton, C.A.; Self-Brown, S.R.; Kasirye, R. Alcohol-related physical abuse of children in the slums of kampala, uganda. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, M.; Romano, E.; Dawson, C.; Huang, H.; Sneij, A.; Cyrus, E.; Rojas, P.; Cano, M.A.; Brook, J.; De La Rosa, M. Drinking and driving among recent latino immigrants: The impact of neighborhoods and social support. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Kanteres, F.; Lachenmeier, D.W. Unrecorded consumption, quality of alcohol and health consequences. Drug Alcohol Rev. 2010, 29, 426–436. [Google Scholar] [CrossRef] [PubMed]
- Konnopka, A.; Konig, H.H. The health and economic consequences of moderate alcohol consumption in germany 2002. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 2009, 12, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Seigers, D.K.; Carey, K.B. Screening and brief interventions for alcohol use in college health centers: A review. J. Am. Coll. Health J. ACH 2010, 59, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Clemens, S.L.; Grant, B.M.; Matthews, S.L. A review of the impacts of health and health behaviors on women‘s alcohol use. Am. J. Health Behav. 2009, 33, 400–415. [Google Scholar] [CrossRef] [PubMed]
- Spear, L.P. The adolescent brain and the college drinker: biological basis of propensity to use and misuse alcohol. J. Stud. Alcohol Drugs Suppl. 2002, 14, 71–81. [Google Scholar] [CrossRef]
- Squeglia, L.; Jacobus, J.; Tapert, S.F. The influence of substance use on adolescent brain development. Clin. EEG Neurosci. 2009, 40, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Ellickson, P.; Saner, H.; McGuigan, K.A. Profiles of violent youth: Substance use and other concurrent problems. Am. J. Public Health 1997, 87, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Mathijssen, J.; Janssen, M.; van Bon-Martens, M.; van de Goor, I. Adolescents and alcohol: An explorative audience segmentation analysis. BMC Public Health 2012, 12, 742. [Google Scholar] [CrossRef] [PubMed]
- Ellickson, P.L.; Tucker, J.S.; Klein, D.J. Ten-year prospective study of public health problems associated with early drinking. Pediatrics 2003, 111, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Legleye, S.; Janssen, E.; Spilka, S.; Le Nezet, O.; Chau, N.; Beck, F. Opposite social gradient for alcohol use and misuse among french adolescents. Int. J. Drug Policy 2013, 24, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Heradstveit, O.; Skogen, J.C.; Hetland, J.; Hysing, M. Alcohol and illicit drug use are important factors for school-related problems among adolescents. Front. Psychol. 2017, 8, 1023. [Google Scholar] [CrossRef] [PubMed]
- Leung, R.K.; Toumbourou, J.W.; Hemphill, S.A.; Catalano, R.F. Peer group patterns of alcohol-using behaviors among early adolescents in victoria, australia, and washington state, united states. J. Res. Adolesc. Off. J. Soc. Res. Adolesc. 2016, 26, 902–917. [Google Scholar] [CrossRef] [PubMed]
- Lipperman-Kreda, S.; Gruenewald, P.J.; Grube, J.W.; Bersamin, M. Adolescents, alcohol, and marijuana: Context characteristics and problems associated with simultaneous use. Drug Alcohol Depend. 2017, 179, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Chatterji, P. Does alcohol use during high school affect educational attainment? Evidence from the national education longitudinal study. Econ. Educ. Rev. 2006, 25, 482–497. [Google Scholar] [CrossRef]
- Gil, A.I.; Molina, J.A. Human development and alcohol abuse in adolescence. Appl. Econ. 2007, 39, 1315–1323. [Google Scholar] [CrossRef]
- Koch, S.F.; Ribar, D.C. A siblings analysis of the effects of alcohol consumption onset on educational attainment. Contemp. Econ. Policy 2001, 19, 162–174. [Google Scholar] [CrossRef]
- Sekulic, D.; Ostojic, M.; Ostojic, Z.; Hajdarevic, B.; Ostojic, L. Substance abuse prevalence and its relation to scholastic achievement and sport factors: An analysis among adolescents of the herzegovina-neretva canton in bosnia and herzegovina. BMC Public Health 2012, 12, 274. [Google Scholar] [CrossRef] [PubMed]
- Tahiraj, E.; Cubela, M.; Ostojic, L.; Rodek, J.; Zenic, N.; Sekulic, D.; Lesnik, B. Prevalence and factors associated with substance use and misuse among kosovar adolescents; cross sectional study of scholastic, familial-, and sports-related factors of influence. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Zenic, N.; Ostojic, L.; Sisic, N.; Pojskic, H.; Peric, M.; Uljevic, O.; Sekulic, D. Examination of the community-specific prevalence of and factors associated with substance use and misuse among rural and urban adolescents: A cross-sectional analysis in bosnia and herzegovina. BMJ Open 2015, 5, e009446. [Google Scholar] [CrossRef] [PubMed]
- Cerkez, I.; Culjak, Z.; Zenic, N.; Sekulic, D.; Kondric, M. Harmful alcohol drinking among adolescents: The influence of sport participation, religiosity, and parental factors. J. Child Adolesc. Subst. Abuse 2015, 24, 94–101. [Google Scholar] [CrossRef]
- Eitle, D.; Turner, R.J.; Eitle, T.M. The deterrence hypothesis reexamined: Sports participation and substance use among young adults. J. Drug Issues 2003, 33, 193–221. [Google Scholar] [CrossRef]
- Wichstrøm, T.; Wichstrøm, L. Does sports participation during adolescence prevent later alcohol, tobacco and cannabis use? Addiction 2009, 104, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Bedendo, A.; Opaleye, E.S.; Andrade, A.L.; Noto, A.R. Heavy episodic drinking and soccer practice among high school students in brazil: The contextual aspects of this relationship. BMC Public Health 2013, 13, 247. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, D.; Idrizovic, K.; Popovic, S.; Sisic, N.; Sekulic, D.; Ostojic, L.; Spasic, M.; Zenic, N. An examination of the ethnicity-specific prevalence of and factors associated with substance use and misuse: Cross-sectional analysis of croatian and bosniak adolescents in bosnia and herzegovina. Int. J. Environ. Res. Public Health 2016, 13, E968. [Google Scholar] [CrossRef] [PubMed]
- Vest, A.E.; Simpkins, S.D. When is sport participation risky or protective for alcohol use? The role of teammates, friendships, and popularity. New Direct. Child Adolesc. Dev. 2013, 2013, 37–55. [Google Scholar] [CrossRef] [PubMed]
- Sigfusdottir, I.D.; Kristjansson, A.L.; Thorlindsson, T.; Allegrante, J.P. Trends in prevalence of substance use among icelandic adolescents, 1995–2006. Subst. Abuse Treat. Preve. Policy 2008, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Modric, T.; Zenic, N.; Sekulic, D. Substance use and misuse among 17- to 18-year-old croatian adolescents: Correlation with scholastic variables and sport factors. Subst. Use Misuse 2011, 46, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Reinert, D.F.; Allen, J.P. The Alcohol Use Disorders Identification Test (Audit): A Review of Recent Research. Alcohol. Clin. Exp. Res. 2002, 26, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Kraus, L.; Guttormsson, U.; Leifman, H.; Hibell, B.; Arpa, S.; Molinaro, S.; Monshouwer, K.; Trapencieris, M.; Vicente, J.; Arnarsson, Á.M.; et al. ESPAD Report 2015. Results from the European School Survey Project on Alcohol and Other Drugs; European Monitoring Centre for Drugs and Addiction. 2016. Available online: http://www.espad.org/sites/espad.org/files/ESPAD_report_2015.pdf (accessed on 1 March 2018).
- Zenic, N.; Terzic, A.; Rodek, J.; Spasic, M.; Sekulic, D. Gender-specific analyses of the prevalence and factors associated with substance use and misuse among bosniak adolescents. Int. J. Environ. Res. Public Health 2015, 12, 6626–6640. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; De la Fuente, J.R.; Grant, M. Development of the alcohol use disorders identification test (audit): Who collaborative project on early detection of persons with harmful alcohol consumption-ii. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Killip, S.; Mahfoud, Z.; Pearce, K. What is an intracluster correlation coefficient? Crucial concepts for primary care researchers. Ann. Fam. Med. 2004, 2, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Kraus, L.; Nociar, A. Espad Report 2015: Results from the European School Survey Project on Alcohol and Other Drugs; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2016. [Google Scholar]
- Maletiæ, E.; Pejiæ, I.; Kontiæ, J.K.; Piljac, J.; Dangl, G.; Vokurka, A.; Lacombe, T.; Miroševiæ, N.; Meredith, C. Zinfandel, dobrieiae, and plavac mali: The genetic relationship among three cultivars of the dalmatian coast of croatia. Am. J. Enol. Viticult. 2004, 55, 174–180. [Google Scholar]
- Stueve, A.; O’donnell, L.N. Early alcohol initiation and subsequent sexual and alcohol risk behaviors among urban youths. Am. J. Public Health 2005, 95, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Litt, D.M.; Stock, M.L. Adolescent alcohol-related risk cognitions: The roles of social norms and social networking sites. Psychol. Addict. Behav. 2011, 25, 708. [Google Scholar] [CrossRef] [PubMed]
- Sajber, D.; Tahiraj, E.; Zenic, N.; Peric, M.; Sekulic, D. Alcohol drinking among kosovar adolescents: An examination of gender-specific sociodemographic, sport, and familial factors associated with harmful drinking. Subst. Use Misuse 2016, 51, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Bjelanovic, L.; Pehar, M.; Pelivan, K.; Zenic, N. Substance use and misuse and potential doping behaviour in rugby union players. Res. Sports Med. 2014, 22, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Coulton, S.; Alam, M.F.; Boniface, S.; Deluca, P.; Donoghue, K.; Gilvarry, E.; Kaner, E.; Lynch, E.; Maconochie, I.; McArdle, P.; et al. Opportunistic screening for alcohol use problems in adolescents attending emergency departments: An evaluation of screening tools. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Pawlowska-Kamieniak, A.; Mroczkowska-Juchkiewicz, A.; Kominek, K.; Krawiec, P.; Melges, B.; Pac-Kozuchowska, E. Alcohol intoxication among adolescents and children in urban and rural environments—A retrospective analysis. Ann. Agric. Environ. Med. AAEM 2018, 25, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lisha, N.E.; Sussman, S. Relationship of high school and college sports participation with alcohol, tobacco, and illicit drug use: A review. Addict. Behav. 2010, 35, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Vieno, A.; Altoe, G.; Kuntsche, E.; Elgar, F.J. Do public expenditures on health and families relate to alcohol abstaining in adolescents? Multilevel study of adolescents in 24 countries. Drug Alcohol Rev. 2018, 37 (Suppl. 1), S120–S128. [Google Scholar] [CrossRef] [PubMed]
- Zeigler, D.W.; Wang, C.C.; Yoast, R.A.; Dickinson, B.D.; McCaffree, M.A.; Robinowitz, C.B.; Sterling, M.L. The neurocognitive effects of alcohol on adolescents and college students. Prev. Med. 2005, 40, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Waszkiewicz, N.; Olanski, W.; Chojnowska, S.; Kolakowska, U.; Plewa, K.; Mielech, W.; Bagniuk-Plewa, A.; Wasilewska, A.; Szulc, A.; Szajda, S.D.; et al. Serum exoglycosidases in children and adolescents with harmful alcohol use. J. Addict. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Balsa, A.I.; Giuliano, L.M.; French, M.T. The effects of alcohol use on academic achievement in high school. Econ. Educ. Rev. 2011, 30, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Steward, R.J.; Devine Steward, A.; Blair, J.; Jo, H.; Hill, M.F. School attendance revisited: A study of urban african american students‘ grade point averages and coping strategies. Urban Educ. 2008, 43, 519–536. [Google Scholar] [CrossRef]
- Jessor, R.; Jessor, S.L. Problem behavior and psychosocial development: A longitudinal study of youth. J. Stud. Alcohol 1978, 39, 948–949. [Google Scholar]


{kind=link}
| Scholastic Variables | Baseline | Follow-Up | ||||
|---|---|---|---|---|---|---|
| Non-HD | HD | MW | Non-HD | HD | MW | |
| F (%) | F (%) | Z (p) | F (%) | F (%) | Z (p) | |
| Grade point average | ||||||
| Excellent | 84 (16.8) | 16 (11.11) | −3.26 (0.01) | 96 (20.87) | 30 (16.3) | −1.27 (0.2) |
| Very good | 256 (51.2) | 56 (38.89) | 222 (48.26) | 88 (47.83) | ||
| Average | 122 (24.4) | 68 (47.22) | 122 (26.52) | 64 (34.78) | ||
| Under average | 18 (3.6) | 4 (2.78) | 16 (3.48) | 2 (1.09) | ||
| Poor | 18 (3.6) | 0 (0) | 4 (0.87) | 0 (0) | ||
| Missing | 2 (100) | 0 (0) | 0 (0) | 0 (0) | ||
| Absences from school | ||||||
| Less than 10 hours | 154 (30.8) | 32 (22.22) | −2.72 (0.01) | 90 (19.57) | 22 (11.96) | −4.56 (0.01) |
| 10-20 hours | 210 (42) | 60 (41.67) | 174 (37.83) | 52 (28.26) | ||
| 21-40 hours | 122 (24.4) | 38 (26.39) | 160 (34.78) | 74 (40.22) | ||
| More than 40 hours | 14 (2.8) | 14 (9.72) | 36 (7.83) | 36 (19.57) | ||
| Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Unexcused absences | ||||||
| None | 318 (63.6) | 60 (41.67) | −3.65 (0.01) | 244 (53.04) | 64 (34.78) | −4.49 (0.01) |
| 1-5 hours | 100 (20) | 54 (37.5) | 106 (23.04) | 56 (30.43) | ||
| 6-10 hours | 36 (7.2) | 22 (15.28) | 50 (10.87) | 16 (8.7) | ||
| 11-20 hours | 24 (4.8) | 6 (4.17) | 26 (5.65) | 14 (7.61) | ||
| More than 20 hours | 22 (4.4) | 0 (0) | 34 (7.39) | 34 (18.48) | ||
| Missing | 0 (0) | 2 (1.39) | 0 (0) | 0 (0) | ||
| Behavioral grade | ||||||
| Exceptional | 430 (86) | 128 (88.89) | 0.97 (0.32) | 388 (84.35) | 136 (73.91) | −3.14 (0.01) |
| Average | 58 (11.6) | 16 (11.11) | 68 (14.78) | 42 (22.83) | ||
| Poor | 12 (2.4) | 0 (0) | 4 (0.87) | 6 (3.26) | ||
| Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Sport Factors | Baseline | Follow-Up | ||||
|---|---|---|---|---|---|---|
| Non-HD | HD | MW | Non-HD | HD | MW | |
| F (%) | F (%) | Z (p) | F (%) | F (%) | Z (p) | |
| Sport success/result | ||||||
| Never competed | 190 (38) | 34 (23.61) | 2.8 (0.06) | 162 (35.22) | 64 (34.78) | 0.08 (0.93) |
| Local rank | 210 (42) | 74 (51.39) | 204 (44.35) | 84 (45.65) | ||
| National rank | 84 (16.8) | 36 (25) | 74 (16.09) | 30 (16.3) | ||
| International rank | 14 (2.8) | 0 (0) | 20 (4.35) | 6 (3.26) | ||
| Missing | 2 (0.4) | 0 (0) | 0 (0) | 0 (0) | ||
| Socioeconomic status | ||||||
| Under average | 14 (2.8) | 4 (2.78) | 0.26 (0.79) | 8 (1.74) | 8 (4.35) | 2.25 (0.02) |
| Average | 424 (84.8) | 124 (86.11) | 390 (84.78) | 160 (86.96) | ||
| Above average | 60 (12) | 16 (11.11) | 62 (13.48) | 16 (8.7) | ||
| Missing | 2 (0.4) | 0 (0) | 0 (0) | 0 (0) | ||
| Experience in sport | ||||||
| Never been involved | 72 (14.4) | 12 (8.33) | −0.91 (0.36) | 96 (20.87) | 40 (21.74) | −0.91 (0.35) |
| <1 year | 36 (7.2) | 20 (13.89) | 26 (5.65) | 10 (5.43) | ||
| 2–5 years | 172 (34.4) | 42 (29.17) | 138 (30) | 42 (22.83) | ||
| >5 years | 220 (44) | 70 (48.61) | 200 (43.48) | 92 (50) | ||
| Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Chi Square (p) | Chi Square (p) | |||||
| Individual sport participation | ||||||
| Yes, participating | 104 (20.8) | 22 (15.28) | 4.23 (0.12) | 78 (16.96) | 16 (8.7) | 8.10 (0.02) |
| Quit | 218 (43.6) | 76 (52.78) | 230 (50) | 94 (51.09) | ||
| Never | 178 (35.6) | 46 (31.94) | 152 (33.04) | 74 (40.22) | ||
| Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Team sport participation | ||||||
| Yes, participating | 98 (19.6) | 48 (33.33) | 20.88 (0.01) | 82 (17.83) | 28 (15.22) | 9.18 (0.01) |
| Quit | 250 (50) | 76 (52.78) | 220 (47.83) | 84 (45.65) | ||
| Never | 152 (30.4) | 20 (13.89) | 158 (34.35) | 72 (39.13) | ||
| Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Covariates | Baseline | Follow-Up | ||||
|---|---|---|---|---|---|---|
| Non-HD | HD | MW | Non-HD | HD | MW | |
| F (%) | F (%) | Z (p) | F (%) | F (%) | Z (p) | |
| Socioeconomic status | ||||||
| Under average | 14 (2.8) | 4 (2.78) | 0.26 (0.79) | 8 (1.74) | 8 (4.35) | 2.25 (0.02) |
| Average | 424 (84.8) | 124 (86.11) | 390 (84.78) | 160 (86.96) | ||
| Above average | 60 (12) | 16 (11.11) | 62 (13.48) | 16 (8.7) | ||
| Missing | 2 (0.4) | 0 (0) | 0 (0) | 0 (0) | ||
| Conflict with parents | ||||||
| Almost never | 80 (16) | 22 (15.28) | −4.17 (0.01) | 110 (23.91) | 52 (28.26) | −0.55 (0.57) |
| Rarely | 230 (46) | 36 (25) | 202 (43.91) | 62 (33.7) | ||
| Occasionally | 164 (32.8) | 64 (44.44) | 132 (28.7) | 56 (30.43) | ||
| Frequently | 26 (5.2) | 22 (15.28) | 16 (3.48) | 14 (7.61) | ||
| Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Gender | ||||||
| Male | 250 (50) | 96 (66.66) | 12.49 (0.01) | 222 (48.26) | 124 (67.39) | 19.34 (0.01) |
| Female | 250 (50) | 48 (33.33) | 238 (51.74) | 60 (32.61) | ||
| Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Predictors | Baseline | Follow-Up | Initiation ¥ | |||
|---|---|---|---|---|---|---|
| Crude OR (95% CI) | Adjusted OR (95% CI) | Crude OR (95% CI) | Adjusted OR (95% CI) | Crude OR (95% CI) | Adjusted OR (95% CI) | |
| Grade point average cont | 2.76 (1.94–3.94) | 2.45 (1.70–3.53) | 2.92 (1.82–4.65) | 2.65 (1.61–4.37) | 3.05 (1.25–7.49) | 2.99 (0.94–9.50) |
| Absences cont | 1.98 (1.43–2.75) | 1.99 (1.40.2.80) | 1.45 (1.02–2.05) | 1.58 (1.09–2.26) | 1.36 (0.68–2.72) | 1.14 (0.65–3.22) |
| Unexcused absences cont | 2.16 (1.44–3.23) | 1.75 (1.17–2.60) | 1.63 (1.15–2.28) | 1.49 (1.06–2.11) | 1.35 (0.54–3.36) | 1.22 (0.44–3.37) |
| Behavioral grade cont | 3.00 (1.12–8.01) | 1.9 (0.7–5.2) | / | / | / | / |
| Individual sport | ||||||
| Yes, participating | 1.50 (0.71–2.96) | 1.39 (0.71–2.76) | 1.42 (0.45–3.66) | 1.06 (0.39–2.85) | / | / |
| Quit | 1.81 (1.07–3.09) | 1.57 (0.91–2.72) | 1.65 (0.85–3.19) | 1.47 (0.75–2.90) | 6.00 (1.73–20.81) | 13.13 (2.67–64.62) |
| Never | REF | REF | REF | REF | REF | REF |
| Team sport | ||||||
| Yes, participating | 2.55 (1.26–5.16) | 2.35 (1.12–4.94) | 0.95 (0.43–2.11) | 0.57 (0.34–1.37) | 2.27 (0.42–12.34) | 1.50 (0.21–10.61) |
| Quit | 1.96 (1.16–3.31) | 1.78 (1.04–3.06) | 1.97 (0.97–3.99) | 1.59 (0.77–3.27) | 1.09 (0.38–3.12) | 0.82 (0.23–2.93) |
| Never | REF | REF | REF | REF | REF | REF |
| Sport success/result cont | 1.38 (0.99–1.90) | 1.24 (0.89–1.74) | 1.32 (1.04–1.69) | 1.18 (0.91–1.53) | 3.67 (1.48–9.11) | 3.15 (1.19–8.34) |
| Experience in sport cont | 1.45 (1.18–1.80) | 1.38 (1.10–1.73) | 1.75 (1.13–2.73) | 1.49 (0.95–2.32) | 1.75 (1.12–2.73) | 2.10 (1.18–3.72) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devcic, S.; Sekulic, D.; Ban, D.; Kutlesa, Z.; Rodek, J.; Sajber, D. Evidencing Protective and Risk Factors for Harmful Alcohol Drinking in Adolescence: A Prospective Analysis of Sport-Participation and Scholastic-Achievement in Older Adolescents from Croatia. Int. J. Environ. Res. Public Health 2018, 15, 986. https://doi.org/10.3390/ijerph15050986
Devcic S, Sekulic D, Ban D, Kutlesa Z, Rodek J, Sajber D. Evidencing Protective and Risk Factors for Harmful Alcohol Drinking in Adolescence: A Prospective Analysis of Sport-Participation and Scholastic-Achievement in Older Adolescents from Croatia. International Journal of Environmental Research and Public Health. 2018; 15(5):986. https://doi.org/10.3390/ijerph15050986
Chicago/Turabian StyleDevcic, Sime, Damir Sekulic, Divo Ban, Zvonimir Kutlesa, Jelena Rodek, and Dorica Sajber. 2018. "Evidencing Protective and Risk Factors for Harmful Alcohol Drinking in Adolescence: A Prospective Analysis of Sport-Participation and Scholastic-Achievement in Older Adolescents from Croatia" International Journal of Environmental Research and Public Health 15, no. 5: 986. https://doi.org/10.3390/ijerph15050986
APA StyleDevcic, S., Sekulic, D., Ban, D., Kutlesa, Z., Rodek, J., & Sajber, D. (2018). Evidencing Protective and Risk Factors for Harmful Alcohol Drinking in Adolescence: A Prospective Analysis of Sport-Participation and Scholastic-Achievement in Older Adolescents from Croatia. International Journal of Environmental Research and Public Health, 15(5), 986. https://doi.org/10.3390/ijerph15050986