Immunization Offer Targeting Migrants: Policies and Practices in Italy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- i.
- legal framework/regulations supporting vaccination offer to asylum seekers, refugees, irregular migrants and unaccompanied minors;
- ii.
- target groups for vaccination, assessment of immunization status and vaccination offered to migrants (children, adolescents and adults);
- iii.
- place for vaccination delivery, availability of Standard Operating Procedures (SOPs) for migrants’ immunization;
- iv.
- recording and transmission of data on administered vaccines, and challenges.
3. Results
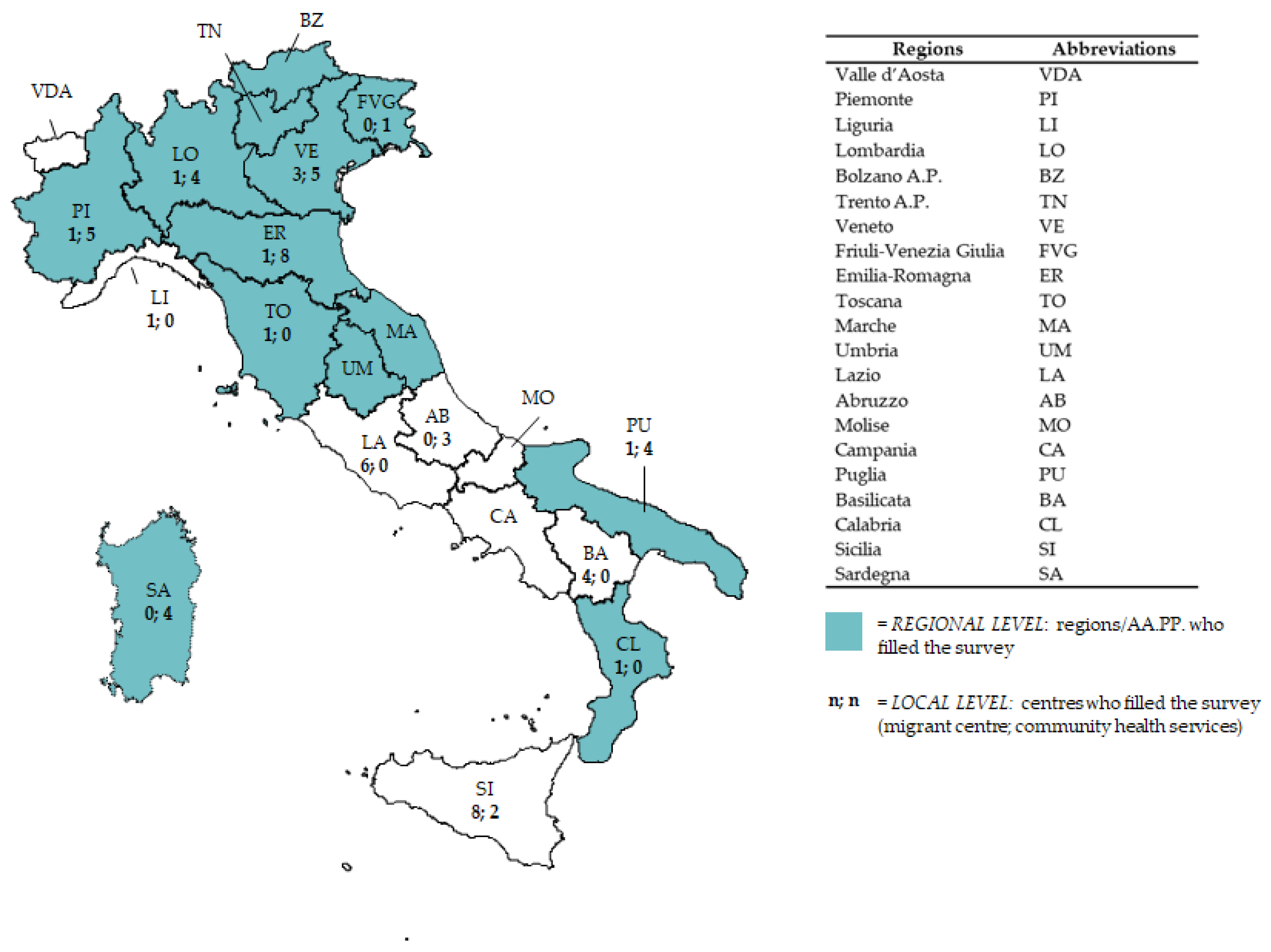
3.1. Profile of the Responders
3.2. Vaccination Offer at National and Regional Levels
3.2.1. Legal Framework Supporting Vaccination Offers Targeting Asylum Seekers, Refugees, Irregular Migrants and Unaccompanied Minors
3.2.2. Vaccination Offer to Migrant Children and Adolescents
3.2.3. Vaccination Offer to Migrant Adults
3.2.4. Vaccine Delivery
3.2.5. Recording of Information on Administered Vaccines and Practical Challenges
3.3. Vaccination Offer at Local Level
3.3.1. General Information on Responding Centres
3.3.2. Immunization Practices in Migrant Reception Centres
3.3.3. Immunization Practices in Community Health Services
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- FRONTEX. Migratory Routes Map. Available online: http://frontex.europa.eu/trends-and-routes/migratory-routes-map/ (accessed on 3 March 2017).
- Italian Ministry of the Interior. Cruscotto Statistico Giornaliero. Available online: http://www.libertaciviliimmigrazione.dlci.interno.gov.it/it/ documentazione/statistica/cruscotto-statistico-giornaliero (accessed on 10 July 2017).
- Italian Ministry of Interior. Schema di Capitolato di Appalto per la Gestione dei Centri di Accoglienza per Immigrati. Available online: http://www1.interno.gov.it/mininterno/export/sites/default/it/assets/files/28_2014/2014_06_20_capitolato_appalto_approvato_D.M._21-11-2008.pdf (accessed on 13 July 2017).
- Centro Studi e Ricerche IDOS. Dossier Statistico Immigrazione; IDOS, Ed.; IDOS: Rome, Italy, 2016; ISBN 9788864800462. [Google Scholar]
- SPRAR-Manuale Operativo. Available online: http://www.meltingpot.org/IMG/pdf/sprar_-_manuale_operativo_2015-2.pdf (accessed on 16 July 2017).
- Anci, Caritas Italiana, Cittalia, Fondazione Migrantes, Ministry of Interior-Sprar, with the Contribution of UNHCR: Rapporto Sulla Protezione Internazionale in Italia, 2016. Available online: http://www.anci.it/Contenuti/Allegati/Rapporto%20protezione%20internazionale%202016.pdf (accessed on 9 July 2017).
- WHO Regional Office for Europe. Migration and Health: Key Issues. Available online: http://www.euro.who.int/en/health-topics/health-determinants/migration-and-health/migranthealth-in-the-european-region/migration-and-health-key-issues (accessed on 15 July 2017).
- WHO Data on Immunization, Vaccines and Biologicals. Available online: http://www.who.int/immunization/monitoring_surveillance/data/en/ (accessed on 8 January 2018).
- Napoli, C.; Riccardo, F.; Declich, S.; Dente, M.G.; Pompa, M.G.; Rizzo, C.; Rota, M.C.; Bella, A.; National Working Group. An early warning system based on syndromic surveillance to detect potential health emergencies among migrants: Results of a two-year experience in Italy. Int. J. Environ. Res. Public Health 2014, 11, 8529–8541. [Google Scholar] [CrossRef] [PubMed]
- Castelli, F.; Sulis, G. Migration and infectious diseases. Clin. Microbiol. Infect. 2017, 23, 283–289. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Handbook on Using the ECDC Preparedness Checklist Tool to Strengthen Preparedness against Communicable Disease Outbreaks at Migrant Reception/Detention Centres. Available online: http://ecdc.europa.eu/en/publications/Publications/preparedness-checklist-migrant-centres-tool.pdf (accessed on 3 July 2017).
- WHO Regional Office per Europe. WHO-UNHCR-UNICEF Joint Technical Guidance: General Principles of Vaccination of Refugees, Asylum-Seekers and Migrants in the WHO European Region. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/vaccines-and-immunization/news/news/2015/11/who,-unicef-and-unhcr-call-for-equitable-access-to-vaccines-for-refugees-and-migrants/who-unhcr-unicef-joint-technical-guidance-general-principles-of-vaccination-of-refugees,-asylumseekers-and-migrants-in-the-who-european-region (accessed on 16 July 2017).
- ECDC Technical Document: Infectious Diseases of Specific Relevance to Newly-Arrived Migrants in the EU/EEA. Available online: https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/Infectious-diseases-of-specific-relevance-to-newly-arrived-migrants-in-EU-EEA.pdf (accessed on 16 July 2017).
- Italian National Law N. 40, 1998. Available online: http://www.camera.it/parlam/leggi/98040l.htm (accessed on 8 January 2018).
- European Observatory on Health Systems and Policies. The Health Systems and Policy Monitor. Available online: http://www.hspm.org/searchandcompare.aspx (accessed on 3 March 2017).
- Italian National Immunization Plan 2012–2014. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_1721_allegato.pdf (accessed on 19 November 2017).
- Constitutional Law N. 3, 18 Oct 2001. Modifiche al Titolo V Della Parte Seconda Della Costituzione. Available online: http://www.parlamento.it/parlam/leggi/01003lc.htm (accessed on 8 May 2018).
- Lo Scalzo, A.; Donatini, A.; Orzella, L.; Cicchetti, A.; Profi li, S.; Maresso, A. Italy: Health system review. Health Syst. Transit. 2009, 11, 1–216. Available online: http://www.euro.who.int/__data/assets/pdf_file/0006/87225/E93666.pdf (accessed on 3 March 2017).
- Riccardo, F.; Dente, M.G.; Kojouharova, M.; Fabiani, M.; Alfonsi, V.; Kurchatova, A.; Vladimirova, N.; Declich, S. Migrant’s access to immunization in Mediterranean Countries. Health Policy 2012, 105, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Giambi, C.; Del Manso, M.; Dente, M.G.; Napoli, C.; Montaño-Remacha, C.; Riccardo, F.; Declich, S. Immunization Strategies Targeting Newly Arrived Migrants in Non-EU Countries of the Mediterranean Basin and Black Sea. Int. J. Environ. Res. Public Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Germinario, C.; Gallone, M.S.; Tafuri, S. Migrant health: The Apulian model. Epidemiol. Prev. 2015, 39, 76–80. [Google Scholar] [PubMed]
- El-Hamad, I.; Pezzoli, M.C.; Chiari, E.; Scarcella, C.; Vassallo, F.; Puoti, M.; Ciccaglione, A.; Ciccozzi, M.; Scalzini, A.; Castelli, F. Point-of-Care Screening, Prevalence, and Risk Factors for Hepatitis B Infection Among 3728 Mainly Undocumented Migrants from Non-EU Countries in Northern Italy. J. Travel Med. 2015, 22, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Tornesello, M.; Cassese, R.; De Rosa, N.; Buonaguro, L.; Masucci, A.; Vallefuoco, G.; Palmieri, S.; Schiavone, V.; Piccoli, R.; Buonaguro, F.M. High Prevalence of Human Papillomavirus Infection in Eastern European and West African women immigrants in South Italy. APMIS 2011, 119, 701–709. [Google Scholar] [CrossRef] [PubMed]
- CARE. “Common Approach for Refugees and Other Migrants’ Health”. Communicable Diseases Monitoring. Available online: http://careformigrants.eu/communicable-diseases-monitoring/ (accessed on 17 July 2017).
- SurveyMonkey®. Available online: http://it.surveymonkey.com/home.aspx. (accessed on 2 February 2017).
- International Organization for Migration (IOM), Glossary of Termis. Available online: http://www.iom.int/key-migration-terms (accessed on 15 December 2017).
- Ministerial Circular, N. 8, 1993. Available online: http://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=0&codLeg=23605&parte=1%20&serie (accessed on 3 March 2017).
- Operative Procedure, 2011. Available online: http://www.salute.gov.it/imgs/C_17_newsAree_1478_listaFile_itemName_1_file.pdf (accessed on 3 March 2017).
- Ministerial Circular, 2014. Available online: http://www.seremi.it/sites/default/files/Ministero%20Salute%20-%20Aggiornamento%20delle%20raccomandazioni%20di%20immunoprofilassi%20virus%209%20maggio%202014.pdf (accessed on 3 March 2017).
- Ministerial Circular, 2017. Available online: http://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2017&codLeg=59725&parte=1%20&serie=null (accessed on 20 November 2017).
- National Plan for Elimination of Measles and Congenital Rubella 2010–2015. G.U. Serie Generale n.297 of 23/12/2003. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_1519_allegato.pdf (accessed on 29 January 2018).
- Italian Ministry of Health. Coperture Vaccinali Pediatriche, i Dati 2015 [Childhood Vaccination Coverage Data, 2015]. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?menu=notizie&p=dalministero&id=2718 (accessed on 17 July 2017).
- Mipatrini, D.; Stefanelli, P.; Severoni, S.; Rezza, G. Vaccinations in migrants and refugees: A challenge for European health systems. A systematic review of current scientific evidence. Pathog. Glob. Health 2017, 111, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.C.; Mytton, J. Estimating infectious disease in UK asylum seekers and refugees: A systematic review of prevalence studies. J. Public Health 2007, 29, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, A.; Evlampidou, I.; Irish, C.; Ingle, S.M.; Hickman, M. Hepatitis B infection prevalence by country of birth in migrant populations in a large UK city. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2015, 68, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Linee Guida Sulla Tutela Della Salute e L’assistenza Sociosanitaria Alle Popolazioni Migranti [Italian Guidelines for Migrants’ Health]. Available online: http://www.inmp.it/index.php/ita/Pubblicazioni/Libri/Rassegna-di-revisioni-sistematiche-linee-guida-e-documenti-di-indirizzo-sulla-salute-degli-immigrati-Scarica-il-documento (accessed on 20 July 2017).
- Italian Ministry of Interior. I Diritti Riconosciuti. Available online: http://www.integrazionemigranti.gov.it/Areetematiche/ProtezioneInternazionale/Pagine/I-diritti.aspx (accessed on 15 July 2017).
- D’Ancona, F.; Gianfredi, V.; Riccardo, F.; Iannazzo, S. Immunization strategies at national level in Italy and the roadmap for a future Italian National Registry. Ann. Ig. 2018, 30, 77–85. [Google Scholar] [PubMed]
- Piano Nazionale di Prevenzione Vaccinale (PNPV) 2017–2019 (National Immunization Plan). Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 10 July 2017).
- De Vito, E.; Parente, P.; de Waure, C.; Poscia, A.; Ricciardi, W. A Review of Evidence on Equitable Delivery, Access and Utilization of Immunization Services for Migrants and Refugees in the WHO European Region; Health Evidence Network Synthesis Report; WHO: Geneva, Switzerland, 2017; Volume 53. [Google Scholar]


{kind=link}
| Question | National Level | N of Regions * | % ** | Regions |
|---|---|---|---|---|
| Is there a regional regulation supporting immunization of migrants? | ||||
| None | - | 6/14 | 43 | LO, TN, TO, MA, CL, SA |
| Regional regulation specific for migrants ^ | - | 8/14 | 57 | PI (2012) 1, BZ (2016), VE (2014), FVG (2016), ER (2014), UM (2015), PU (2009) SI (2011) |
| CHILDREN/ADOLESCENTS | ||||
| Which are the target groups for vaccination? | ||||
| Immigration status | ||||
| All (asylum seekers, refugees, irregular migrants, unaccompanied minors) | X | 14/14 | 100 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, PU, CL, SI, SA |
| Age group (years) | ||||
| 0–15 | 6/14 | 43 | BZ, VE, UM, CL, SI, SA | |
| 0–18 | X | 8/14 | 57 | PI, LO, TN, FVG, ER, TO, MA, PU |
| Risk conditions | ||||
| None | X | 14/14 | 100 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, PU, CL, SI, SA |
| Is the immunization status verified through anamnesis or check of vaccination card? | ||||
| Yes | X | 14/14 | 100 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, PU, CL, SI, SA |
| Use of laboratory test if migrant has no immunization card? | ||||
| Yes | X (HBV, tetanus) | 9/13 | 69 | PI (tetanus, measles, HBV), LO (tetanus, diphtheria), BZ (tetanus, diphtheria, HBV), TN (tetanus), FVG (tetanus, HBV, varicella), ER (tetanus, measles, rubella, HBV), UM 2, PU (IPV, MMR, varicella, HBV), SI 2 |
| Which vaccinations are offered to susceptible migrants? | ||||
| All vaccinations included in the NIP | X | 13/14 | 93 | PI, LO, BZ, VE, FVG, ER, TO, MA, UM, PU, CL, SI, SA |
| IPV, tetanus, diphtheria, MMR | 1/14 | 7 | TN | |
| ADULTS | ||||
| Which are the target groups for vaccination? | ||||
| Immigration status | ||||
| All (asylum seekers, refugees, irregular migrants) | X | 14/14 | 100 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, PU, CL, SI, SA |
| Age group (years) | ||||
| No limits other than those in the NIP | X | 14/14 | 100 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, PU, CL, SI, SA |
| Risk conditions | ||||
| None | X 3 | 13/14 | 93 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, PU, CL, SI |
| from polio endemic countries/countries at risk of polio reintroduction | 1/14 | 7 | SA | |
| Is the immunization status verified through anamnesis or check of vaccination card in ADULTS? | ||||
| Yes | X (polio) | 14/14 | 100 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, PU, CL, SI, SA |
| Use of laboratory test if migrant has no immunization card? | ||||
| Yes | X (HBV, tetanus) | 4/14 | BZ (tetanus, HBV), TN (tetanus), ER (tetanus, HBV, measles, rubella), CL (all included in the NIP, according to risks) | |
| Informed consent before vaccinating (both for ADULTS and CHILDREN)? | ||||
| Yes, oral | n.a. 4 | 5/11 | 45 | PI, TN, VE, FVG, MA |
| Yes, written | 6/11 | 55 | LO, BZ, ER, TO, PU, CL | |
| Sites for vaccination delivery (both for ADULTS and CHILDREN)? | ||||
| Holding level | X | 6/14 | 43 | TN, VE, FVG, TO, PU, SI |
| Vaccination services | X | 13/14 | 93 | PI, LO, BZ, TN, VE, FVG, ER, TO, MA, UM, CL, SI, SA |
| Primary health care (GP/Paediatricians) | 3/14 | 21 | TO, PU 5, CL | |
| Vaccine | ITALY | REGIONS | LOCAL LEVEL | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PI | LO | BZ | TN | VE | FVG | ER | TO | MA | UM | PU | CL | SA | SI | Migrant Centres (3) a | Health Services (30) a | ||
| Polio | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | 14 | |
| Tetanus | X b | X | X | X | X | X | X | X | X | X | X | X | X | X | X b | 2 * | 28 |
| Diphtheria | X | X | X | X | X | X | X | X | X | X | X | X | 2 * | 27 | |||
| Pertussis | X | X | X | X | X | X | 2 * | 19 | |||||||||
| MMR | X | X | X | X | X | X | X | X | X | X | 2 * | 22 | |||||
| Varicella | X | X c | 2 * | 18 | |||||||||||||
| Hepatitis B | X | X | X * | X * | X * | X * | 2 * | 20 *,d | |||||||||
| Hepatitis A | X * | X * | X * | X * | X * | 2 * | 16 * | ||||||||||
| BCG e | |||||||||||||||||
| Influenza | X * | X * | X * | X * | X * | 3 * | 20 * | ||||||||||
| PCV | X | X * | X * | X * | X * | X * | 2 * | 16 * | |||||||||
| Meningococcus C/ACWY | X * | X * | X * | X * | X * | 2 * | 15 * | ||||||||||
| Challenges | ITALY | REGIONS | LOCAL LEVEL | |
|---|---|---|---|---|
| Migrant Centres (28) a | Health Services (36) a | |||
| Scarcity of resources | X | PI, LO, TN, ER, TO, PU, CL, SA | 6 | 17 |
| Need of specific training of health care workers on migrant health | X | LO, TO, MA, SA | 3 | 11 |
| Lack of operating procedures | X | PI, MA, CL | 4 | 8 |
| Scarce collaboration within health institutions | PI, LO, MA, TO | 7 | 5 | |
| Low compliance of migrants to vaccination | VE | 5 | 7 | |
| Lack of health staff | BZ | |||
| Logistic issues | 4 | 2 | ||
| Waiting time | 1 | |||
| Difficulties due to the short time of staying of migrants and the frequency of relocation | 1 | 1 | ||
| Language barriers | 3 | |||
| Total No. of Responding Centres | Migrant Centres (28) a | Health Services (36) a | ||
|---|---|---|---|---|
| Dealing with children/adolescents | 15 b | 35 | ||
| Dealing with adults | 25 | 32 | ||
| Performing Health assessment | 23 | 23 | ||
| Giving a personal health card to migrants | 23 | 22 | ||
| Available cultural mediators | 28 | 13 c | ||
| Length of stay of migrants in the centre d | <6 months | 6 | ||
| 6–12 months | 12 | |||
| >12 months | 10 | |||
| Maximum capacity of the centre d | <50 people | 9 | ||
| 51–150 | 11 | |||
| 151–300 | 1 | |||
| >300 | 7 | |||
| Presence of an outpatient clinics inside the centre d | 22 | |||
| Who provides health services? d | PHC services | 22 | ||
| NGOs | 7 | |||
| Staff of the centre | 5 | |||
| Migrant Reception Centres (5) * | Community Health Services (36) * | ||
|---|---|---|---|
| Is information on vaccine administration recorded? | |||
| Yes (specify where, more than one answer possible) | 5 | 35 1 | |
| Individual health record delivered to migrants | 4 | 18 | |
| Electronic archive dedicated to migrants | 2 | 9 | |
| Paper archives dedicated to migrants | 3 | 8 | |
| General population electronic immunization registries | 3 | 25 | |
| General population paper-based immunization registries | 2 | 4 | |
| Is information on vaccine administration made available to other institutions? | |||
| Yes (specify to whom, more than one answer possible) | 5 | 30 1 | |
| It follows the same flow of the information on immunization of general population | - | 18 | |
| To migrants’ holding centres | - | 15 | |
| To LHU vaccination services | 4 | 9 | |
| To GPs and paediatricians | - | 5 | |
| To holding centres where migrants are relocated | 4 | 6 | |
| To local health authorities | 1 | 3 | |
| To regional health authorities | - | 7 | |
| To international institutions | 1 (IOM) | - | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalla Zuanna, T.; Del Manso, M.; Giambi, C.; Riccardo, F.; Bella, A.; Caporali, M.G.; Dente, M.G.; Declich, S.; The Italian Survey CARE Working Group. Immunization Offer Targeting Migrants: Policies and Practices in Italy. Int. J. Environ. Res. Public Health 2018, 15, 968. https://doi.org/10.3390/ijerph15050968
Dalla Zuanna T, Del Manso M, Giambi C, Riccardo F, Bella A, Caporali MG, Dente MG, Declich S, The Italian Survey CARE Working Group. Immunization Offer Targeting Migrants: Policies and Practices in Italy. International Journal of Environmental Research and Public Health. 2018; 15(5):968. https://doi.org/10.3390/ijerph15050968
Chicago/Turabian StyleDalla Zuanna, Teresa, Martina Del Manso, Cristina Giambi, Flavia Riccardo, Antonino Bella, Maria Grazia Caporali, Maria Grazia Dente, Silvia Declich, and The Italian Survey CARE Working Group. 2018. "Immunization Offer Targeting Migrants: Policies and Practices in Italy" International Journal of Environmental Research and Public Health 15, no. 5: 968. https://doi.org/10.3390/ijerph15050968
APA StyleDalla Zuanna, T., Del Manso, M., Giambi, C., Riccardo, F., Bella, A., Caporali, M. G., Dente, M. G., Declich, S., & The Italian Survey CARE Working Group. (2018). Immunization Offer Targeting Migrants: Policies and Practices in Italy. International Journal of Environmental Research and Public Health, 15(5), 968. https://doi.org/10.3390/ijerph15050968