Smelting Remains a Public Health Risk Nearly a Century Later: A Case Study in Pueblo, Colorado, USA

Abstract
:1. Introduction
2. Materials and Methods
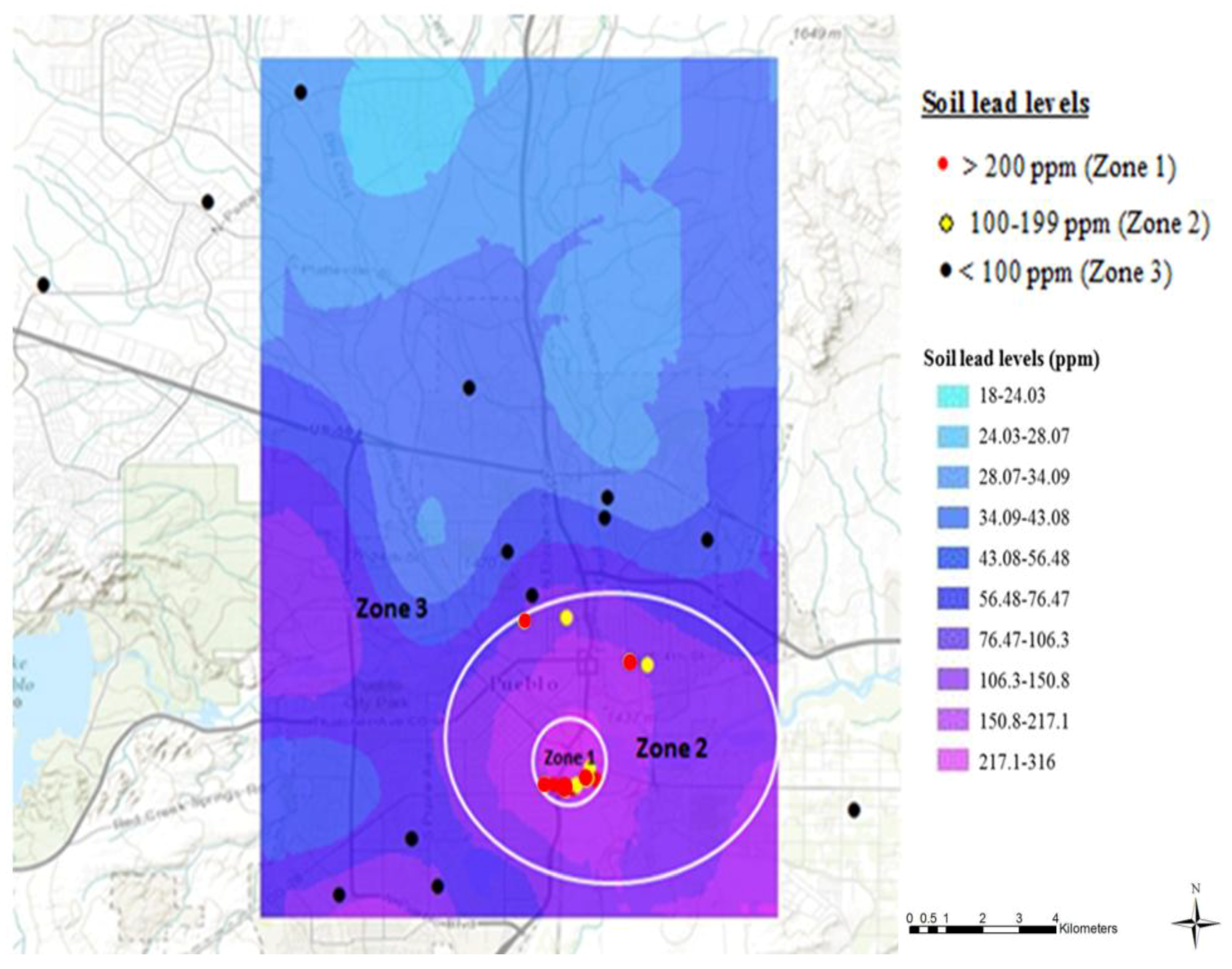
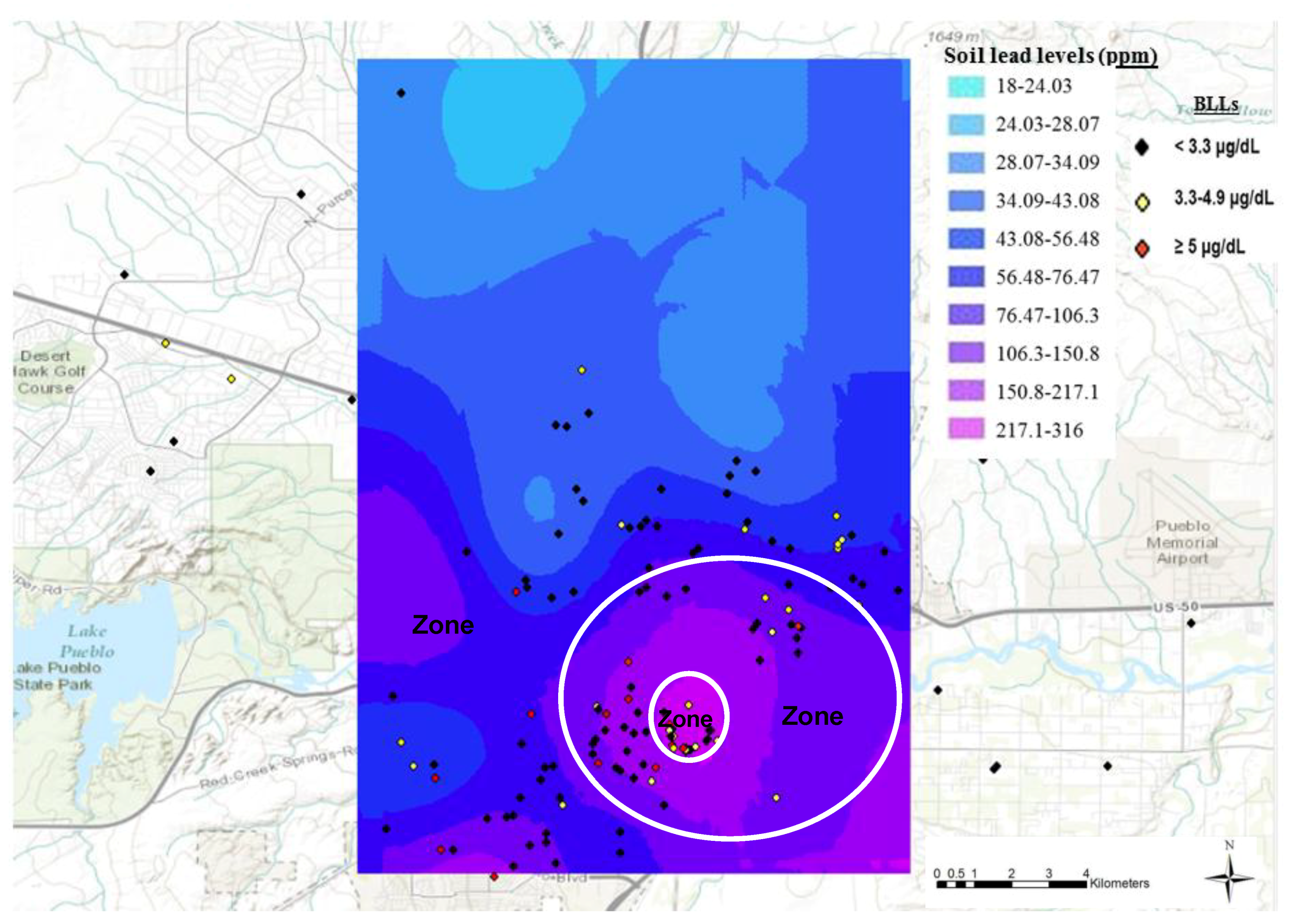
2.1. Classification of Zones
2.2. Participants
2.3. Blood Lead Testing
2.4. Soil Analysis
2.5. Genotyping for ALAD Polymorphism
2.6. Statistical Analyses
3. Results
3.1. Blood Lead Testing
3.2. Soil Analysis
3.3. Genotyping for ALAD Polymorphism
4. Discussion
4.1. Blood Lead Levels in Children of Pueblo, Colorado vs. the U.S. National Average
4.2. Association between Topsoil Lead Levels and Blood Lead Levels in Pueblo Children
4.3. ALAD Polymorphisms and Blood Lead Levels
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Buckingham, A.N. Analytical Results Report Santa Fe Avenue Bridge Culvert; COD #982572513; Colorado Department of Public Health and Environment (CDPHE): Pueblo, CO, USA, 1995; p. 20. Available online: https://www.epa.gov/sites/production/files/2014-10/documents/colorado-smelter-ref-14-santa-fe-ave-bridge-culvert-arr-6-10-1995.pdf (accessed on 1 May 2013).
- Fry, E. Smelters of Pueblo; Pueblo County Historical Society: Pueblo, CO, USA, 2000; p. 164. [Google Scholar]
- EVRAZ North America. About EVRAZ North America. 2018. Available online: evrazna.com (accessed on 20 April 2018).
- Diawara, M.M.; Litt, J.S.; Unis, D.; Alfonso, N.; Martinez, L.A.; Crock, J.G.; Smith, D.B.; Carsella, J. Arsenic, cadmium, lead, and mercury in surface soils, Pueblo, Colorado: Implications for population health risk. Environ. Geochem. Health 2006, 28, 297–315. [Google Scholar] [CrossRef] [PubMed]
- GeoLytics Inc. United States Census CD 2000 Long form SF3; GeoLytics Inc.: East Brunswick, NJ, USA, 2002. [Google Scholar]
- United States Census Bureau. American Fact Finder. 2013. Available online: https://factfinder.census.gov/faces/nav/jsf/pages/community_facts.xhtml (accessed on 23 May 2015).
- Colorado Department of Public Health and Environment (CDPHE), Hazardous Materials and Waste Management Division (HMWMD). Analytical Results Report; #CON000802700; Colorado Smelter: Pueblo, CO, USA, 2011. Available online: https://www.epa.gov/sites/production/files/documents/ARR_Jun2011.pdf (accessed on 23 May 2015).
- Landrigan, P.J.; Gehlbach, S.H.; Rosenblum, B.F.; Shoults, J.M.; Candelaria, R.M.; Barthel, W.F.; Liddle, J.A.; Smrek, A.L.; Staehling, N.W.; Sanders, J. Epidemic lead absorption near an ore smelter. The role of particulate lead. N. Engl. J. Med. 1975, 292, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Yankel, A.J.; von Lindern, I.H.; Walter, S.D. The Silver Valley lead study: The relationship between childhood blood lead levels and environmental exposure. J. Air Pollut. Control Assoc. 1977, 27, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J.; Baker, E.L. Exposure of children in heavy metals from smelters: Epidemiology and toxic consequences. Environ. Res. 1981, 25, 204–224. [Google Scholar] [CrossRef]
- Brunekreef, B.; Veenstra, S.J.; Biersteker, K.; Boleij, J.S. The Arnhem Lead Study. I. Lead uptake by 1- to 3-year-old children living in the vicinity of a secondary lead smelter in Arnhem, The Netherlands. Environ. Res. 1981, 25, 441–448. [Google Scholar] [CrossRef]
- Bornschein, R.L.; Clark, C.S.; Grote, J.; Peace, B.; Roda, S.; Succop, P. Soil lead—Blood lead relationship in a former lead mining town. In Lead in Soil: Issues and Guidelines; Davies, B.E., Wixson, B.G., Eds.; Science Review Ltd.: Northwood, UK, 1988; pp. 149–160. [Google Scholar]
- Rabinowitz, M.B.; Bellinger, D.C. Soil lead—blood lead relationship among Boston children. Bull. Environ. Contam. Toxicol. 1988, 41, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.; Chappell, W.R.; Hoffman, R.E.; Mangione, E.J. Assessment of blood lead levels in children living in a historic mining and smelting community. Am. J. Epidemiol. 1993, 137, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Malcoe, L.H.; Lynch, R.A.; Keger, M.C.; Skaggs, V.J. Lead sources, behaviors, and socioeconomic factors in relation to blood lead of Native American and white children: A community-based assessment of a former mining area. Environ. Health Perspect. 2002, 110, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.D.; Quah, R.F.; Meigs, J.W.; Delouise, E.R. The relationship of environmental lead to blood-lead levels in children. Environ. Res. 1982, 27, 372–383. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Matte, T.D.; Rogers, J.; Clickner, R.P.; Dietz, B.; Bornschein, R.L.; Succop, P.; Mahaffey, K.R.; Dixon, S.; Galke, W.; et al. The contribution of lead-contaminated house dust and residential soil to children’s blood lead levels. A pooled analysis of 12 epidemiologic studies. Environ. Res. 1998, 79, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Canfield, R.L.; Henderson, C.R., Jr.; Cory-Slechta, D.A.; Cox, C.; Jusko, T.A.; Lanphear, B.P. Intellectual impairment in children with blood lead concentrations below 10 µg per deciliter. N. Engl. J. Med. 2003, 348, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Needleman, H.L.; Gunnoe, C.; Leviton, A.; Reed, R.; Peresie, H.; Maher, C.; Barrett, P. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. N. Engl. J. Med. 1979, 300, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Needleman, H.L.; Schell, A.; Bellinger, D.; Leviton, A.; Allred, E.N. The long-term effects of exposure to low doses of lead in childhood. An 11-year follow-up report. N. Engl. J. Med. 1990, 322, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Pirkle, J.L.; Brody, D.J.; Gunter, E.W.; Kramer, R.A.; Paschal, D.C.; Flegal, K.M.; Matte, T.D. The decline in blood lead levels in the United States. The National Health and Nutrition Examination Surveys (NHANES). JAMA 1994, 272, 284–291. [Google Scholar] [CrossRef] [PubMed]
- United States Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report: Update: Blood lead levels—United States, 1991–1994. Weekly 1997, 46, 141–146. [Google Scholar]
- Finkelstein, Y.; Markowitz, M.E.; Rosen, J.F. Low-level lead-induced neurotoxicity in children: An update on central nervous system effects. Brain Res. Brain Res. Rev. 1998, 27, 168–176. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Dietrich, K.; Auinger, P.; Cox, C. Cognitive deficits associated with blood lead concentrations <10 μg/dL in US children and adolescents. Public Health Rep. 2000, 115, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Lidsky, T.I.; Schneider, J.S. Lead neurotoxicity in children: Basic mechanisms and clinical correlates. Brain 2003, 126, 5–19. [Google Scholar] [CrossRef] [PubMed]
- United States Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report: Blood lead levels in children aged 1–5 years—United States, 1999–2002. Weekly 2005, 54, 513–516. [Google Scholar]
- United States Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report: Blood lead levels in children aged 1–5 years United States, 1999–2010. Weekly 2013, 62, 245–248. [Google Scholar]
- United States Centers for Disease Control and Prevention. Preventing Lead Poisoning in Young Children. 2005. Available online: https://www.cdc.gov/nceh/lead/publications/prevleadpoisoning.pdf (accessed on 10 September 2015).
- United States Centers for Disease Control and Prevention. Low Level Lead Exposure Harms Children: A Renewed Call of Primary Prevention. CDC Response to Advisory Committee on Childhood Lead Poisoning Prevention Recommendations. 2012. Available online: https://www.cdc.gov/nceh/lead/acclpp/final_document_010412.pdf (accessed on 19 May 2015).
- Sakai, T.; Yanagihara, S.; Kunugi, Y.; Ushio, K. Relationships between distribution of lead in erythrocytes in vivo and in vitro and inhibition of ALA-D. Br. J. Ind. Med. 1982, 39, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Bergdahl, I.A.; Grubb, A.; Schutz, A.; Desnick, R.J.; Wetmur, J.G.; Sassa, S.; Skerfving, S. Lead binding to delta-aminolevulinic acid dehydratase (ALAD) in human erythrocytes. Pharmacol. Toxicol. 1997, 81, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Bergdahl, I.A.; Sheveleva, M.; Schutz, A.; Artamonova, V.G.; Skerfving, S. Plasma and blood lead in humans: Capacity-limited binding to delta-aminolevulinic acid dehydratase and other lead-binding components. Toxicol. Sci. 1998, 46, 247–253. [Google Scholar] [PubMed]
- Xie, Y.; Chiba, M.; Shinohara, A.; Watanabe, H.; Inaba, Y. Studies on lead-binding protein and interaction between lead and selenium in the human erythrocytes. Ind. Health 1998, 36, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Astrin, K.H.; Bishop, D.F.; Wetmur, J.G.; Kaul, B.; Davidow, B.; Desnick, R.J. Delta-aminolevulinic acid dehydratase isozymes and lead toxicity. Ann. N. Y. Acad. Sci. 1987, 514, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Wetmur, J.G.; Lehnert, G.; Desnick, R.J. The delta-aminolevulinate dehydratase polymorphism: Higher blood lead levels in lead workers and environmentally exposed children with the 1-2 and 2-2 isozymes. Environ. Res. 1991, 56, 109–119. [Google Scholar] [CrossRef]
- Fleming, D.E.; Chettle, D.R.; Wetmur, J.G.; Desnick, R.J.; Robin, J.P.; Boulay, D.; Richard, N.S.; Gordon, C.L.; Webber, C.E. Effect of the delta-aminolevulinate dehydratase polymorphism on the accumulation of lead in bone and blood in lead smelter workers. Environ. Res. 1998, 77, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Scinicariello, F.; Murray, H.E.; Moffett, D.B.; Abadin, H.G.; Sexton, M.J.; Fowler, B.A. Lead and delta-aminolevulinic acid dehydratase polymorphism: Where does it lead? A meta-analysis. Environ. Health Perspect. 2007, 115, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Miyaki, K.; Lwin, H.; Masaki, K.; Song, Y.; Takahashi, Y.; Muramatsu, M.; Nakayama, T. Association between a polymorphism of aminolevulinate dehydrogenase (ALAD) gene and blood lead levels in Japanese subjects. Int. J. Environ. Res. Public Health 2009, 6, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.M.; Wang, X.; Hu, H.; Kelsey, K.T. A polymorphism in the delta-aminolevulinic acid dehydratase gene may modify the pharmacokinetics and toxicity of lead. Environ. Health Perspect. 1995, 103, 248–253. [Google Scholar] [PubMed]
- Hsieh, L.L.; Liou, S.H.; Chen, Y.H.; Tsai, L.C.; Yang, T.; Wu, T.N. Association between aminolevulinate dehydrogenase genotype and blood lead levels in Taiwan. J. Occup. Environ. Med. 2000, 42, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Wu, M.T.; Cheng, Y.; Sparrow, D.; Weiss, S.; Kelsey, K. The delta-aminolevulinic acid dehydratase (ALAD) polymorphism and bone and blood lead levels in community-exposed men: The normative aging study. Environ. Health Perspect. 2001, 109, 827–832. [Google Scholar] [PubMed]
- Sobin, C.; Parisi, N.; Schaub, T.; de la Riva, E. A Bland–Altman comparison of the Lead Care® System and inductively coupled plasma mass spectrometry for detecting low-level lead in child whole blood samples. J. Med. Toxicol. 2011, 7, 24–32. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. Method 3052 Microwave Assisted Acid Digestion of Siliceous and Organically Based Matrices. 1996. Available online: https://www.epa.gov/sites/production/files/2015-12/documents/3052.pdf (accessed on 1 June 2014).
- Crock, J.G.; Lichte, F.E.; Briggs, P.H. Determination of elements in National Bureau of Standards geological reference materials SRM 278 obsidian and SRM 688 basalt by inductively coupled plasma-atomic emission spectroscopy. Geostand. Newslett. Res. 1983, 7, 335–340. [Google Scholar] [CrossRef]
- Shen, X.M.; Wu, S.H.; Yan, C.H.; Zhao, W.; Ao, L.M.; Zhang, Y.W.; He, J.M.; Ying, J.M.; Li, R.Q.; Wu, S.M.; et al. Delta-aminolevulinate dehydratase polymorphism and blood lead levels in Chinese children. Environ. Res. 2001, 85, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Samuels, M.L.; Witmer, J.A.; Schaffner, A.A. Statistics for the Life Sciences; Pearson Education: Boston, MA, USA, 2012; p. 654. [Google Scholar]
- Dignam, T.; Pomales, A.; Werner, L.; Newbern, E.C.; Hodge, J.; Nielsen, J.; Grober, A.; Scruton, K.; Young, R.; Kelly, J.; et al. Assessment of child lead exposure in a Philadelphia community, 2014. J. Public Health Manag. Pract. 2018. [Google Scholar] [CrossRef] [PubMed]
- Burns, M.S.; Gerstenberger, S.L. Implications of the new Centers for Disease Control and Prevention blood lead reference value. Am. J. Public Health 2014, 104, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Gonzales, C.R.; Powell, E.; Jartun, M.; Mielke, P.W., Jr. Nonlinear association between soil lead and blood lead of children in metropolitan New Orleans, Louisiana: 2000–2005. Sci. Total Environ. 2007, 388, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Weitz, S.; Clickner, R.P.; Blackburn, A.; Buches, D. Comprehensive and Workable Plan for the Abatement of Lead-based Paint in Privately Owned Housing: Report to Congress; U.S. Department of Housing and Urban Development: Washington, DC, USA, 1990; p. 227.
- Bradham, K.D.; Nelson, C.M.; Kelly, J.; Pomales, A.; Scruton, K.; Dignam, T.; Misenheimer, J.C.; Li, K.; Obenour, D.R.; Thomas, D.J. Relationship between total and bioaccessible lead on children’s blood lead levels in urban residential Philadelphia soils. Environ. Sci. Technol. 2017, 51, 10005–10011. [Google Scholar] [CrossRef] [PubMed]
- United States Environment Protection Agency. Fuels and Fuel Additives. 2011. Available online: https://www.epa.gov/gasoline-standards (accessed on 19 May 2015).
- Linton, R.W.; Natusch, D.F.S.; Solomon, R.L.; Evans, C.A. Physicochemical characterization of lead in urban dusts. A microanalytical approach to lead tracing. Environ. Sci. Technol. 1980, 14, 159–164. [Google Scholar] [CrossRef]
- Mielke, H.W.; Anderson, J.C.; Berry, K.J.; Mielke, P.W.; Chaney, R.L.; Leech, M. Lead concentrations in inner-city soils as a factor in the child lead problem. Am. J. Public Health 1983, 73, 1366–1369. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Laidlaw, M.A.; Gonzales, C. Lead (Pb) legacy from vehicle traffic in eight California urbanized areas: Continuing influence of lead dust on children’s health. Sci. Total Environ. 2010, 408, 3965–3975. [Google Scholar] [CrossRef] [PubMed]
- Scokart, P.O.; Meeus-Verdinne, K.; De Borger, R. Mobility of heavy metals in polluted soils near zinc smelters. Water Air Soil Pollut. 1983, 20, 451–463. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Lead; Agency for Toxic Substances and Disease Registry, Division of Toxicology and Environmental Medicine, Applied Toxicology Branch: Atlanta, GA, USA, 2007. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp13.pdf (accessed on 10 September 2014).
- Clark, J.J.; Knudsen, A.C. Extent, characterization, and sources of soil lead contamination in small-urban residential neighborhoods. J. Environ. Qual. 2013, 42, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- United States Environment Protection Agency. Protect Your Family from Exposure to Lead. 2014. Available online: https://www.epa.gov/lead/protect-your-family-exposures-lead (accessed on 21 September 2014).
- Wetmur, J.G.; Kaya, A.H.; Plewinska, M.; Desnick, R.J. Molecular characterization of the human delta-aminolevulinate dehydratase 2 (ALAD2) allele: Implications for molecular screening of individuals for genetic susceptibility to lead poisoning. Am. J. Hum. Genet. 1991, 49, 757–763. [Google Scholar] [PubMed]
- Battistuzzi, G.; Petrucci, R.; Silvagni, L.; Urbani, R.; Caiola, S. Delta-aminolevulinate dehydrase: A new genetic polymorphism in man. Ann. Hum. Genet. 1981, 45, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Huo, X.; Peng, L.; Qiu, B.; Zheng, L.; Yekeen, T.A.; Xu, X. ALAD genotypes and blood lead levels of neonates and children from e-waste exposure in Guiyu, China. Environ. Sci. Pollut. Res. 2014, 21, 6744–6750. [Google Scholar] [CrossRef] [PubMed]
- United States Environment Protection Agency. Colorado Smelter. 2015. Available online: https://cumulis.epa.gov/supercpad/cursites/csitinfo.cfm?id=0802700 (accessed on 12 May 2015).



{kind=link}
{kind=link}
| Zones of Lead Distribution in Topsoil | No. of Children with BLLs <3.3 µg/dL | No. of Children with BLLs 3.3–4.9 µg/dL | No. of Children with BLLs ≥5 µg/dL (Reportable) | Total Number of Children |
|---|---|---|---|---|
| Zone 1 (>200 mg/kg) | 25 (69.4%) | 6 (16. 7%) | 5 (13.9%) | 36 |
| Zone 2 (100–199 mg/kg) | 55 (63.2%) | 24 (27.6%) | 8 (9.1%) | 87 |
| Zone 3 (<100 mg/kg) | 98 (83.7%) | 14 (12.0%) | 5 (4.3%) | 117 |
| Total number of children | 178 | 44 | 18 | 240 |
| BLL (µg/dL) | ALAD1-1 | ALAD1-2 | Wilson-Adjusted Sample Proportion |
|---|---|---|---|
| <3.3 µg/dL | 157 | 12 | 95% confidence interval (−0.3305, 0.03350) |
| >3.3 µg/dL | 61 | 1 | |
| Total | 218 | 13 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diawara, M.M.; Shrestha, S.; Carsella, J.; Farmer, S. Smelting Remains a Public Health Risk Nearly a Century Later: A Case Study in Pueblo, Colorado, USA. Int. J. Environ. Res. Public Health 2018, 15, 932. https://doi.org/10.3390/ijerph15050932
Diawara MM, Shrestha S, Carsella J, Farmer S. Smelting Remains a Public Health Risk Nearly a Century Later: A Case Study in Pueblo, Colorado, USA. International Journal of Environmental Research and Public Health. 2018; 15(5):932. https://doi.org/10.3390/ijerph15050932
Chicago/Turabian StyleDiawara, Moussa M., Sofy Shrestha, Jim Carsella, and Shanna Farmer. 2018. "Smelting Remains a Public Health Risk Nearly a Century Later: A Case Study in Pueblo, Colorado, USA" International Journal of Environmental Research and Public Health 15, no. 5: 932. https://doi.org/10.3390/ijerph15050932