Exposure to Quartz in Finnish Workplaces Declined during the First Six Years after the Signing of the NEPSI Agreement, but Evened out between 2013 and 2017


Abstract
:1. Introduction
2. Methods
2.1. Sampling Sites
2.2. Sampling
2.3. FTIR and XRD Methodology
2.4. Analysis by FTIR
2.5. Analysis by XRD
2.6. Estimating the Amount of Workers Exposed to Respirable Crystalline Silica
2.7. Estimating the Amount of Workers with Silicosis or Cancers Attributable to Quartz Exposure
2.8. Estimating Statistical Significance of the Trend in Respirable Quartz Exposure from 2013 to 2017
3. Results
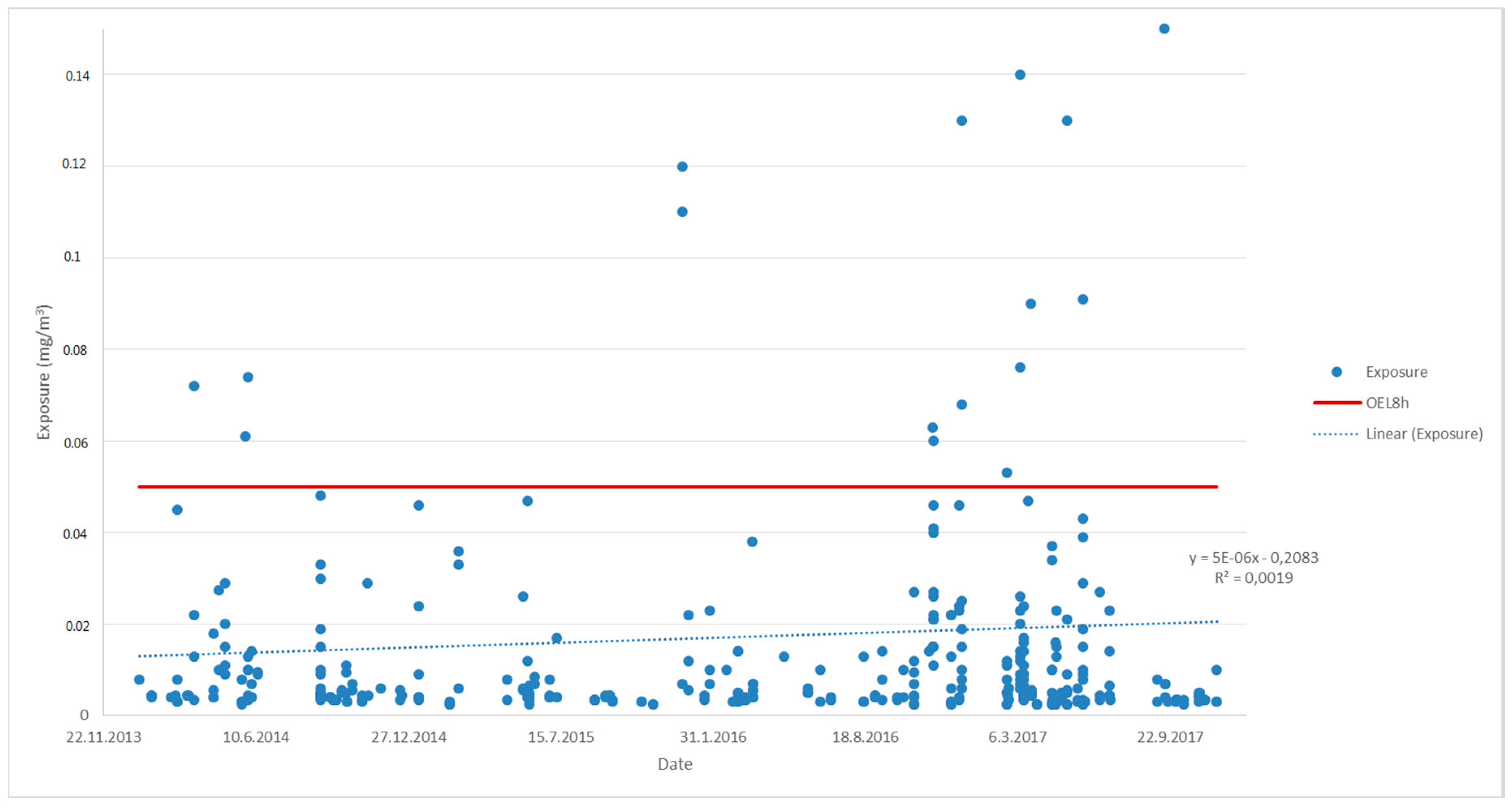
3.1. Measured Exposure (2006–2017)
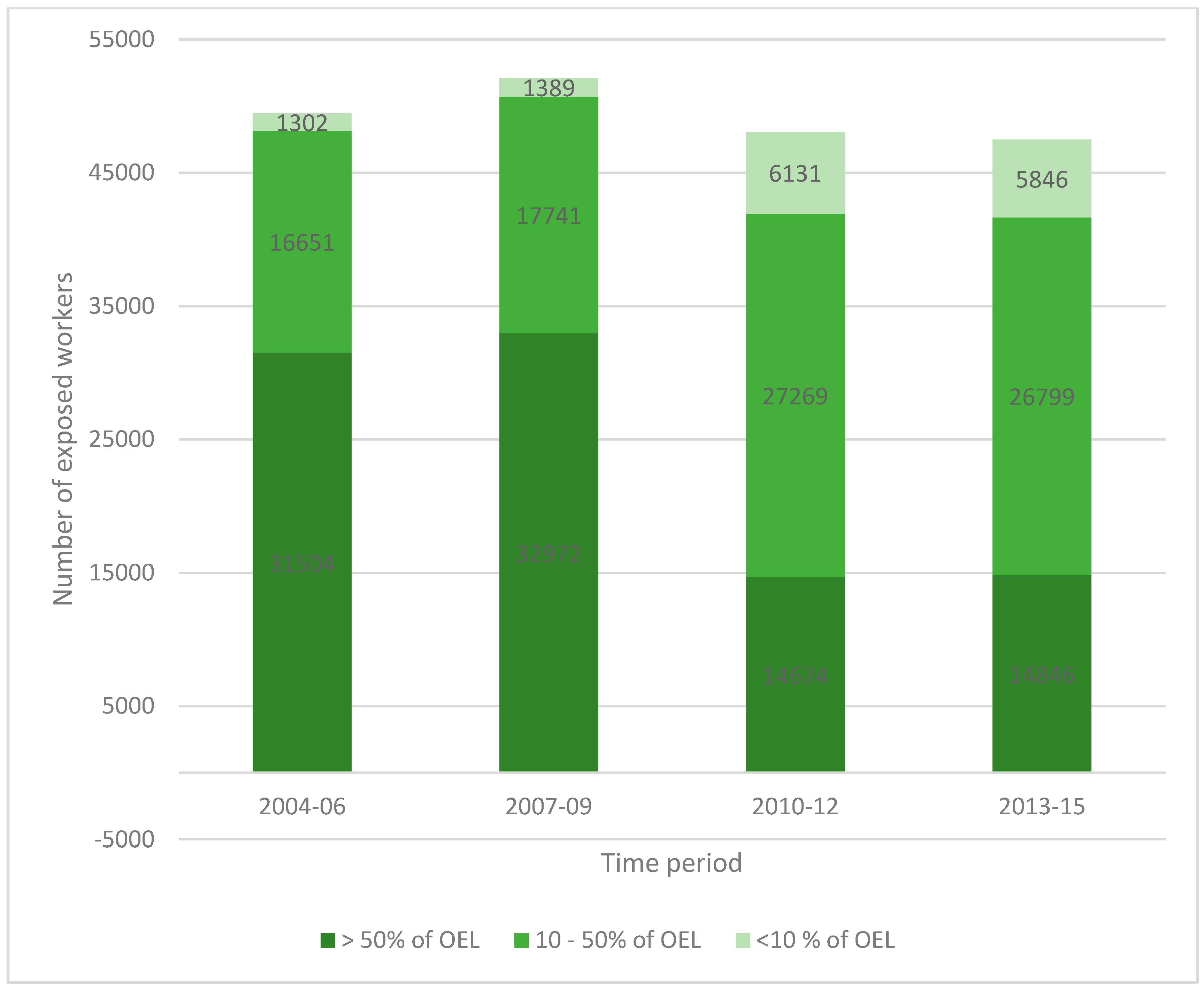
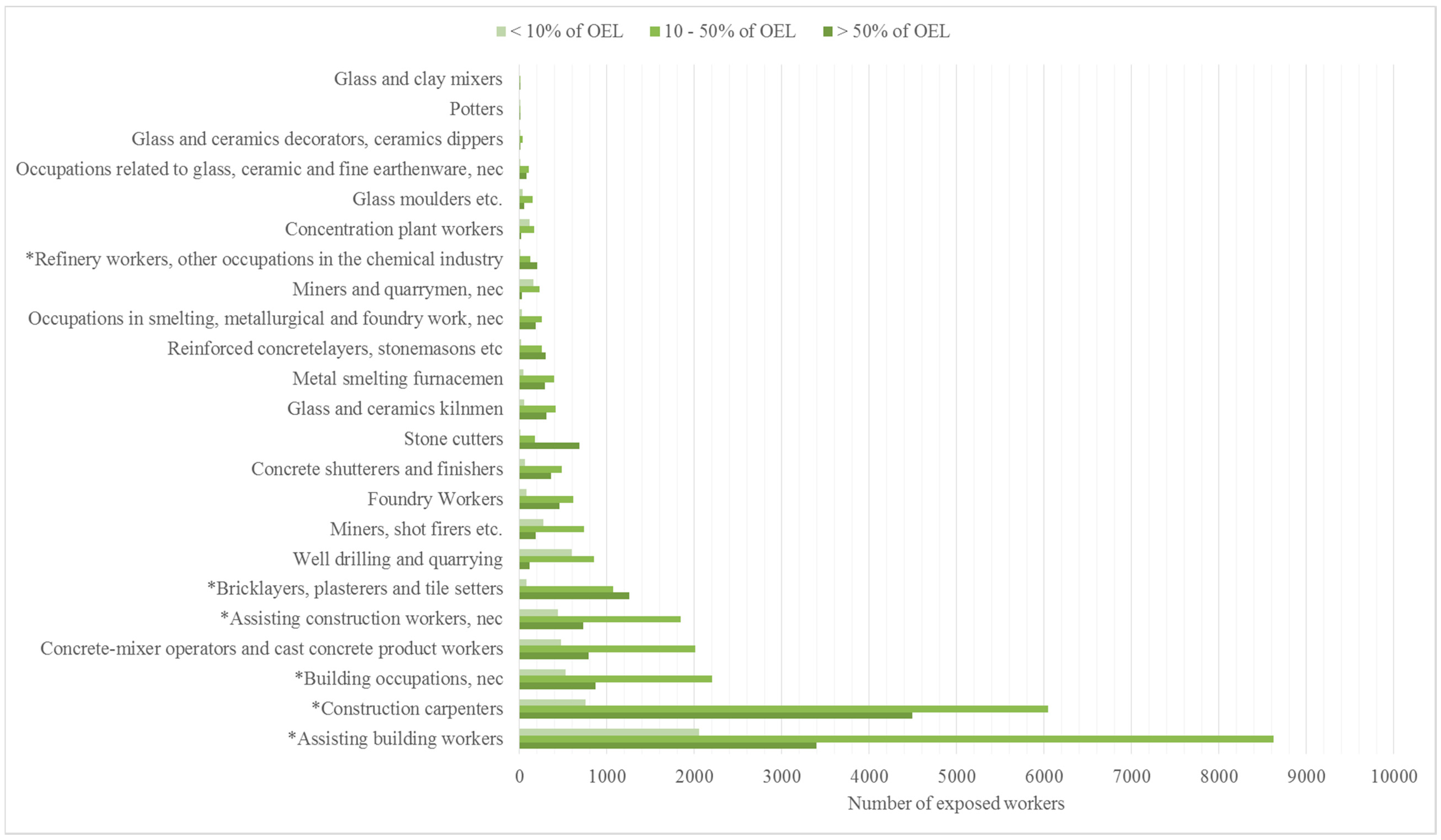
3.2. Exposure in Different Occupations (2013–2015) and the Number of Exposed Workers from 1995 to 2015
3.3. Annual Incidence Rate and Annual Prevalence of Work-Related Silicosis and Lung Cancer from Respirable Quartz Exposure between 2005 and 2014
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Klein, C. Rocks, Minerals, and a Dusty World. Rev. Mineral. 1993, 28, 7–59. [Google Scholar]
- The European Network on Silica (NEPSI). Agreement on Workers Health Protection through the Good Handling and Use of Crystalline Silica and Products Containing it. Annex 1, Good Practices (Good Practice Guide); NEPSI: Brussels, Belgium, 2013; Available online: https://www.nepsi.eu/good-practice-guide (accessed on 27 March 2018).
- International Agency for Research on Cancer (IARC). IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans. In A Review of Human Carcinogens. Arsenic, Metals, Fibres, and Dusts; Part C; International Agency for Research on Cancer (IARC): Lyon, France, 2012; Volume 100. [Google Scholar]
- Official Statistics of Finland (OSF). Labor Force Survey; Statistics Finland: Helsinki, Finland, 2018; ISSN 1798-7857. Available online: http://www.stat.fi/til/tyti/index_en.html (accessed on 26 March 2018).
- The Ministry of Economic Affairs and Employment in Finland (MEAE). Business Sector Services, Sector Reports, Mining Sector; MEAE: Helsinki, Finland, 2018; Available online: http://julkaisut.valtioneuvosto.fi/bitstream/handle/10024/160584/SectorReports_1_2018_MiningSector.pdf (accessed on 26 March 2018).
- The European Network on Silica (NEPSI). Agreement on Workers Health Protection through the Good Handling and Use of Crystalline Silica and Products Containing It; NEPSI: Brussels, Belgium, 2013; Available online: https://www.nepsi.eu/agreement (accessed on 27 March 2017).
- Tuomi, T.; Linnainmaa, M.; Väänänen, V.; Reijula, K. Application of good practices as described by the NEPSI agreement coincides with a strong decline in the exposure to respiratory crystalline silica in Finnish workplaces. Ann. Occup. Hyg. 2014, 58, 806–817. [Google Scholar] [PubMed]
- CEN (Comite Europe’n de Normalisation). Workplace Atmospheres: Size Fraction Definitions for Measurements of Airborne Particles; CEN Standard EN-481; Comite Europe’n de Normalisation: Brussels, Belgium, 1993. [Google Scholar]
- ISO (International Standards Organisation). Air Quality—Particle Size Fraction Definitions for Health-Related Sampling; ISO Standard 7708; International Standards Organisation: Geneva, Switzerland, 1995. [Google Scholar]
- International Agency for Research on Cancer (IARC). Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans. Silica, Some Silicates, Coal Dust and Para-Aramid Fibres; International Agency for Research on Cancer: Lyon, France, 1997; Volume 68. [Google Scholar]
- National Institute of Occupational Safety and Health (NIOSH). Hazard Review: Health Effects of Occupational Exposure to Respirable Crystalline Silica; Department of Health and Human Services, Centers for Disease Control and Prevention, NIOSH: Cincinnati, Ohio, 2002. Available online: https://www.cdc.gov/niosh/docs/2002-129/pdfs/2002-129.pdf (accessed on 27 March 2018).
- Saffiotti, U. Silicosis and Lung Cancer, a fifty-year perspective. Acta Biomed. 2005, 76 (Suppl. 2), 30–37. [Google Scholar] [PubMed]
- SCOEL. Recommendation from the Scientific Committee (SCOEL) on Occupational Exposure Limits for Silica, Crystalline (Respirable Dust); SCOEL/SUM/94; European Commission: Luxembourg, 2003; Available online: http://ec.europa.eu/social/BlobServlet?docId=3858&langId=en (accessed on 27 March 2018).
- Desphande, A.; Narayanan, P.; Lehnert, B. Silica-induced generation of extracellular factor(s) increases reactive oxygen species in human bronchial epithelial cells. Toxicol. Sci. 2002, 67, 275–283. [Google Scholar]
- Polimeni, M.; Gazzano, E.; Ghiazza, M.; Fenoglio, I.; Bosia, A.; Fubini, B.; Ghizo, D. Quartz Inhibits Glucose 6-Phosphate Dehydrogenase in Murine Alveolar Macrophages. Chem. Res. Toxicol. 2008, 21, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Knaapen, A.; Borm, P.; Albrecht, C.; Schins, R. Inhaled particles and lugn cancer. Part A: Mechanisms. Int. J. Cancer 2004, 109, 799–809. [Google Scholar] [CrossRef] [PubMed]
- European Commission (EC). Information Notices on Diagnosis of Occupational Diseases; Health and Safety Report 14768 EN; EC: Luxembourg, 1994; Available online: http://aei.pitt.edu/44055/1/A6293.pdf (accessed on 28 March 2018).
- Duffin, R.; Gilmour, P.; Schins, R.; Clouter, A.; Guy, K.; Brown, D.; MacNee, W.; Borm, P.; Donaldson, K.; Stone, V. Aluminium lactate treatment of dq12 quartz inhibits its ability to cause inflammation, chemokine expression, and nuclear factor-kappab activation. Toxicol. Appl. Pharmacol. 2001, 176, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Fubini, B.; Fenoglio, I.; Elias, Z.; Poirot, O. Variability of biological responses to silicas: Effect of origin, crystallinity, and state of surface on generation of reactive oxygen species and morphological transformation of mammalian cells. J. Environ. Pathol. Toxicol. Oncol. 2001, 20 (Suppl. 1), 95–108. [Google Scholar] [CrossRef]
- Occupational Health and Safety Administration (OSHA). Frequently Asked Questions: Respirable Silica Rule; OSHA: Washington, DC, USA, 2016. Available online: htps://www.osha.gov/silica/Silica_FAQs_2016-3-22.pdf (accessed on 26 March 2018).
- Kalberlah, F.; Bloser, M.; Wachholz, C. Toleranz-und Akzeptanzschwelle für Gesundheitsrisiken am Arbeitsplatz; Projektnummer F2010; Bundesanstalt für Arbeitsschutz und Arbeitsmedizin: Dortmund, Germany, 2005; Available online: https://www.baua.de/DE/Angebote/Publikationen/Berichte/F2010.pdf?__blob=publicationFile (accessed on 27 March 2018).
- European Chemicals Agency (ECHA). Guidance on Information Requirements and Chemical Safety Assessment Chapter 8: Characterisation of Dose [Concentration] Response for Human Health; ECHA-2010-G-19_EN; European Chemicals Agency: Helsinki, Finland, 2012; Available online: https://echa.europa.eu/documents/10162/13632/information_requirements_r8_en.pdf/e153243a-03f0-44c5-8808-88af66223258 (accessed on 27 March 2018).
- NIOSH (National Institute of Occupational Safety and Health). Silica, Crystalline by IR (KBr Pellet); Method 7602; National Institute of Occupational Safety and Health (NIOSH): Cincinnati, Ohio, 2003. [Google Scholar]
- Kauppinen, T.; Toikkanen, J.; Pukkala, E. From Cross-tabulations to Multipurpose Exposure Information Systems: A New Job-Exposure Matrix. Am. J. Ind. Med. 1998, 33, 409–417. [Google Scholar] [CrossRef]
- Pukkala, E.; Huo, J.; Kyyrönen, P.; Lindbohm, M.-L.; Sallmén, M.; Kauppinen, T. National Job-Exposure Matrix in Analyses of Census-Based Estimates of Occupational Cancer Risk. Scand. J. Work Environ. Health. 2005, 31, 97–107. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Regional Office for Europe. National Profile of Occupational Health System in Finland; WHO Regional Office for Europe: Copenhagen, Denmark, 2012; Available online: http://www.euro.who.int/__data/assets/pdf_file/0016/160522/e96482.pdf (accessed on 22 September 2017).
- Warner, R.M. Applied Statistics. From Bivariate to Multivariate Techniques, 2nd ed.; Sage Publications Inc.: Thousand Oaks, CA, USA; University of New Hampshire: Durham, NH, USA, 2013. [Google Scholar]
- European Commission (EC). Study on the Implementation of the Autonomous Agreement of Workers’ Health Protection through the Good Handling and Use of Crystalline Silica and Products Containing It; Final Report; EC: Luxembourg, 2016; Available online: https://r.search.yahoo.com/_ylt=AwrJS5VbG7pap2sA3DpbLAx.;_ylu=X3oDMTByZTJwYXBkBGNvbG8DaXIyBHBvcwM5BHZ0aWQDBHNlYwNzcg--/RV=2/RE=1522174939/RO=10/RU=http%3a%2f%2fec.europa.eu%2fsocial%2fBlobServlet%3fdocId%3d16939%26langId%3den/RK=2/RS=4Le_w6yqcU.oN8_rPVLNehxtyZQ- (accessed on 27 March 2018).
- Health and Safety Executive (HSE); Workplace Health Expert Committee (WHEC). Silica and Lung Cancer; Evidence Review Paper 3/17; Health and Safety Executive: Liverpool, UK, 2017. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Year | Number of Samples | Average (mg/m3) | Median (mg/m3) | 95% Percentile (mg/m3) | Nr. of Results > OEL8h |
|---|---|---|---|---|---|
| 1 2006 | 99 | 0.2036 | 0.0340 | 1.0100 | 44 |
| 1 2007 | 71 | 0.0365 | 0.0100 | 0.1400 | 15 |
| 1 2008 | 276 | 0.0443 | 0.0090 | 0.1325 | 41 |
| 1 2009 | 155 | 0.0213 | 0.0065 | 0.0586 | 13 |
| 1 2010 | 102 | 0.0158 | 0.0055 | 0.0596 | 8 |
| 1 2011 | 197 | 0.0656 | 0.0055 | 0.1720 | 33 |
| 1 2012 | 195 | 0.0180 | 0.0040 | 0.0522 | 11 |
| 1 2013 | 44 | 0.0134 | 0.0058 | 0.0430 | 2 |
| 2014 | 87 | 0.0111 | 0.0050 | 0.0414 | 3 |
| 2015 | 67 | 0.0252 | 0.0040 | 0.0911 | 4 |
| 2016 | 95 | 0.0163 | 0.0060 | 0.0502 | 5 |
| 2017 | 158 | 0.0181 | 0.0050 | 0.0781 | 10 |
| The Number of Exposed Workers Per Time-Period | |||||||
|---|---|---|---|---|---|---|---|
| Occupation | 2 1995–1997 | 2 1998–2000 | 2 2001–2003 | 2 2004–2006 | 2 2007–2009 | 2010–2012 | 2013–2015 |
| 1 Construction carpenters | 7563 | 11,262 | 11,307 | 12,115 | 12,374 | 11,602 | 11,299 |
| 1 Assisting building workers | 3802 | 5704 | 6745 | 8826 | 9568 | 15,732 | 14,071 |
| 1 Building occupations, nec | 3469 | 3569 | 5214 | 6420 | 7439 | 2961 | 3597 |
| 1 Assisting construction workers, nec | 1756 | 2633 | 3115 | 4075 | 4417 | 2798 | 3010 |
| 1 Bricklayers, plasterers, and tile setters | 2495 | 3334 | 3347 | 3586 | 3662 | 2309 | 2415 |
| Concrete-mixer operators and cast concrete product workers | 1771 | 2207 | 2401 | 2379 | 2960 | 2774 | 3279 |
| Foundry Workers | 1496 | 2049 | 2125 | 2381 | 1888 | 1382 | 1153 |
| Well drilling and quarrying | 588 | 883 | 725 | 1617 | 1726 | 2061 | 1559 |
| Metal smelting furnacemen | 1813 | 1812 | 1810 | 1255 | 1427 | 634 | 736 |
| Stone cutters | 766 | 1080 | 1353 | 1012 | 1154 | 654 | 865 |
| Miners, shot firers etc. | 678 | 606 | 746 | 704 | 1089 | 953 | 1199 |
| Occupations in smelting, metallurgical and foundry work, nec | 898 | 923 | 905 | 1354 | 920 | 408 | 475 |
| Glass molders etc. | 679 | 953 | 943 | 1108 | 746 | 258 | 241 |
| Reinforced concrete layers, stonemasons etc. | 487 | 651 | 654 | 700 | 715 | 436 | 577 |
| Concrete shutterers and finishers | 524 | 587 | 669 | 507 | 647 | 899 | 899 |
| Miners and quarrymen, nec | 551 | 701 | 433 | 456 | 321 | 422 | 1199 |
| Potters | 218 | 245 | 201 | 301 | 268 | 258 | 17 |
| Occupations related to glass, ceramic, and fine earthenware, nec | 310 | 217 | 201 | 109 | 240 | 219 | 196 |
| 1 Refinery workers, other occupations in the chemical industry | 257 | 280 | 189 | 241 | 231 | 308 | 336 |
| Concentration plant workers | 91 | 136 | 139 | 177 | 214 | 206 | 306 |
| Glass and ceramics decorators, ceramics dippers | 148 | 162 | 88 | 94 | 53 | 31 | 59 |
| Glass and ceramics kilnmen | 102 | 74 | 118 | 39 | 31 | 910 | 774 |
| Glass and clay mixers | 16 | 11 | 11 | 6 | 13 | 17 | 2 |
| Sum of all occupations (total number of workers) | 30,478 | 40,079 | 43,439 | 49,462 | 52,103 | 48,232 | 48,264 |
| Sum of workers covered by the NEPSI treaty | 11,136 | 13,297 | 13,522 | 14,199 | 14,412 | 12,522 | 13,526 |
| Year | Silicosis | Lung Cancers |
|---|---|---|
| 2005 | 8 | 0 |
| 2006 | 14 | 0 |
| 2007 | 9 | 1 |
| 2008 | 10 | 1 |
| 2009 | 5 | 0 |
| 2010 | 5 | 0 |
| 2011 | 8 | 2 |
| 2012 | 8 | 1 |
| 2013 | 5 | 0 |
| 2014 | 11 | 0 |
| Sum | 84 | 5 |
| Average | 7.7 | 0.45 |
| Annual prevalence | 2:10,000 | 1:100,000 |
| Occupations | Incidence |
|---|---|
| Miners; shot firers and quarrymen in mining | 30 |
| Shot firers in building industries | 6 |
| Painters; carpenters; assistant building workers; plumbers; percussion drillers and deep drillers; assisting building and construction workers; other occupations in building industries | 19 |
| Foundry workers; occupations in smelting and metallurgical work | 13 |
| Welders, boilermakers, metal workers | 6 |
| Production of stone- and concrete products, cement, and tiles | 8 |
| Others | 7 |
| Sum | 89 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuomi, T.; Linnainmaa, M.; Pennanen, S. Exposure to Quartz in Finnish Workplaces Declined during the First Six Years after the Signing of the NEPSI Agreement, but Evened out between 2013 and 2017. Int. J. Environ. Res. Public Health 2018, 15, 906. https://doi.org/10.3390/ijerph15050906
Tuomi T, Linnainmaa M, Pennanen S. Exposure to Quartz in Finnish Workplaces Declined during the First Six Years after the Signing of the NEPSI Agreement, but Evened out between 2013 and 2017. International Journal of Environmental Research and Public Health. 2018; 15(5):906. https://doi.org/10.3390/ijerph15050906
Chicago/Turabian StyleTuomi, Tapani, Markku Linnainmaa, and Sirpa Pennanen. 2018. "Exposure to Quartz in Finnish Workplaces Declined during the First Six Years after the Signing of the NEPSI Agreement, but Evened out between 2013 and 2017" International Journal of Environmental Research and Public Health 15, no. 5: 906. https://doi.org/10.3390/ijerph15050906
APA StyleTuomi, T., Linnainmaa, M., & Pennanen, S. (2018). Exposure to Quartz in Finnish Workplaces Declined during the First Six Years after the Signing of the NEPSI Agreement, but Evened out between 2013 and 2017. International Journal of Environmental Research and Public Health, 15(5), 906. https://doi.org/10.3390/ijerph15050906