Prevalence of Self-Reported Gluten-Related Disorders and Adherence to a Gluten-Free Diet in Salvadoran Adult Population



 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Questionnaire and Population Survey
2.2. Definitions
2.3. Statistical Analysis and Ethical Issues
3. Results
3.1. Demographic and Clinical Characteristics
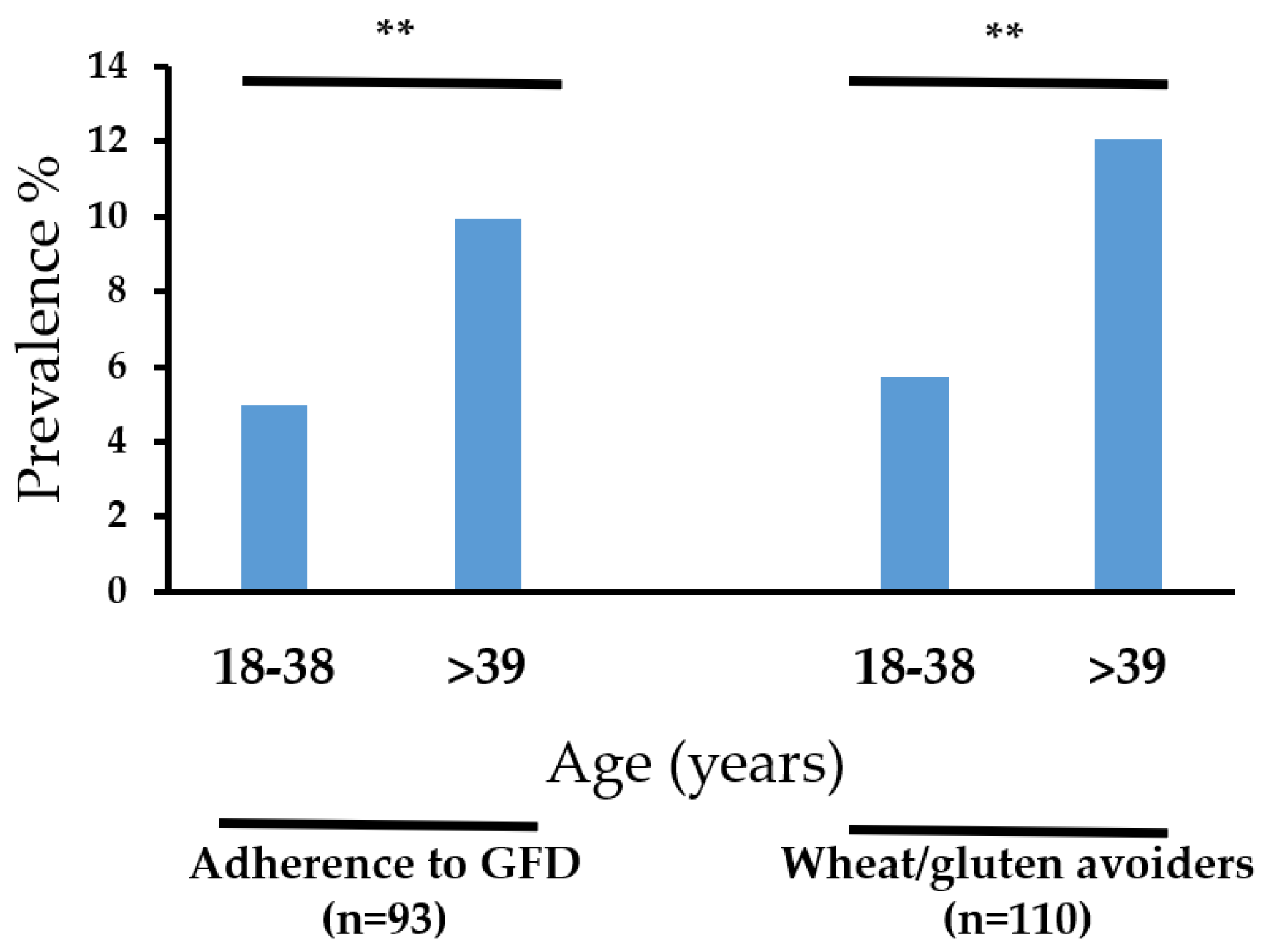
3.2. Prevalence Rates
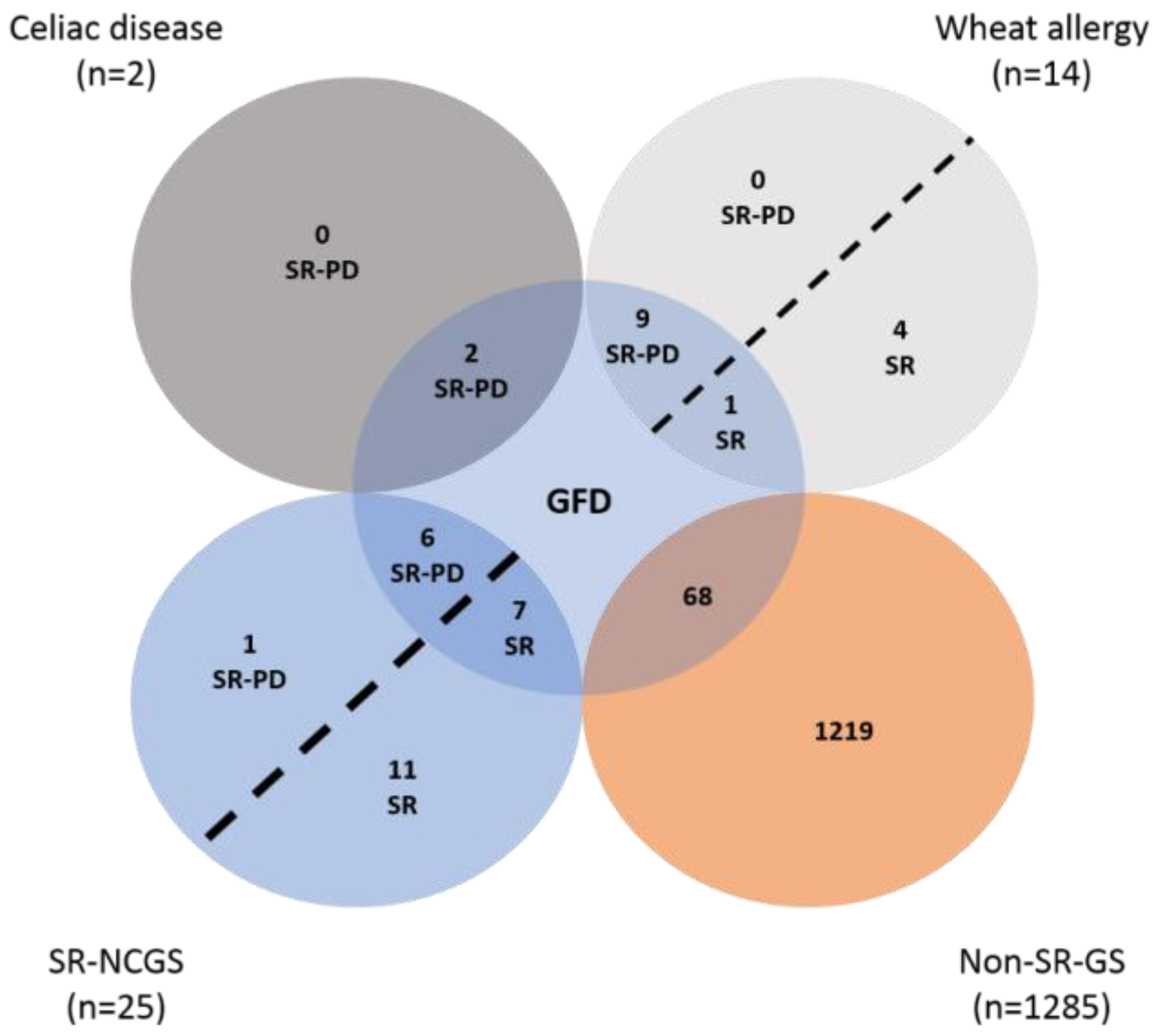
3.3. Cases with More than One Physician-Diagnosed Gluten-Related Disorder
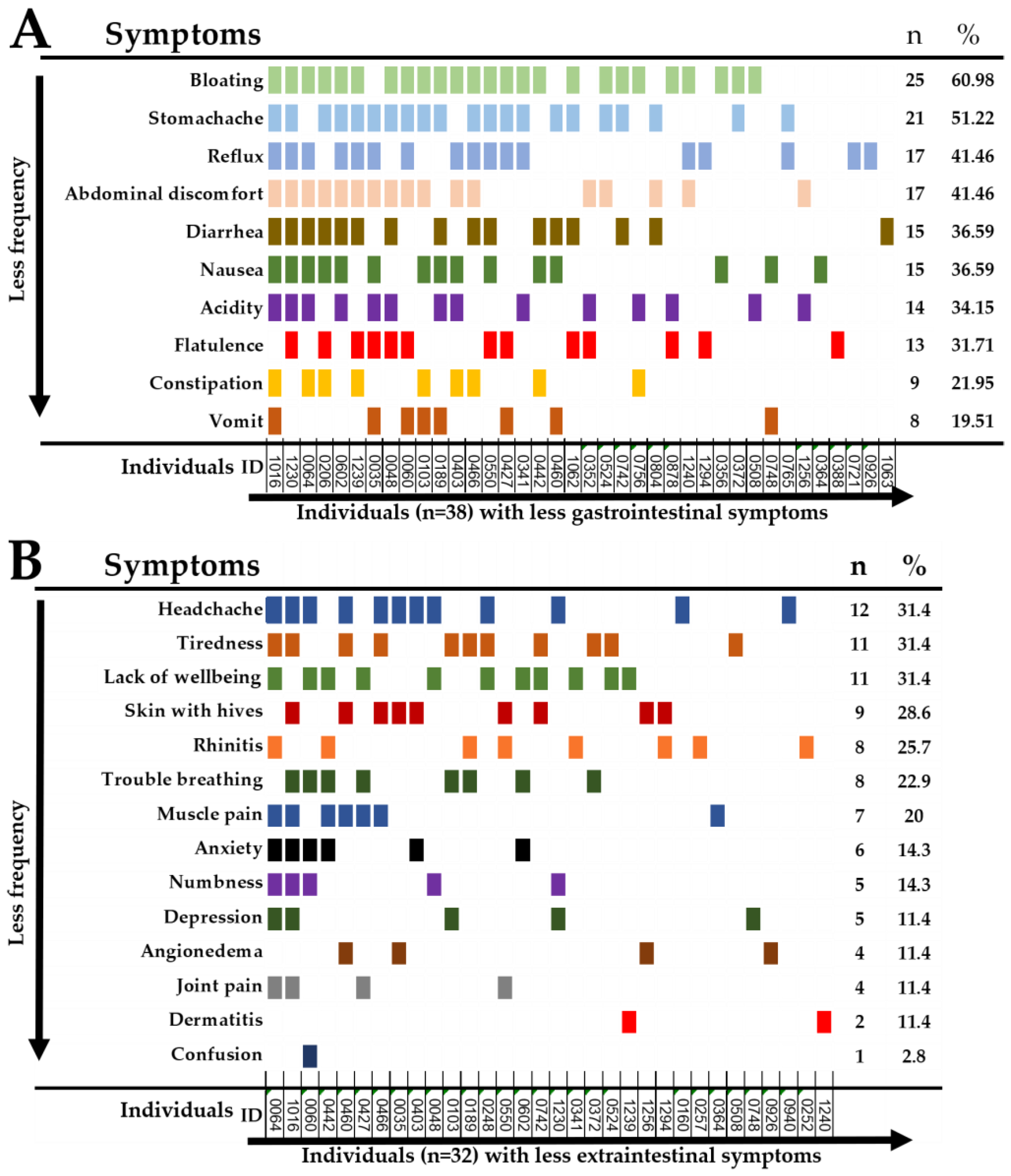
3.4. Self-Reported Gastrointestinal and Extra-Intestinal Symptoms Triggered after Gluten Ingestion in SR-GS Cases
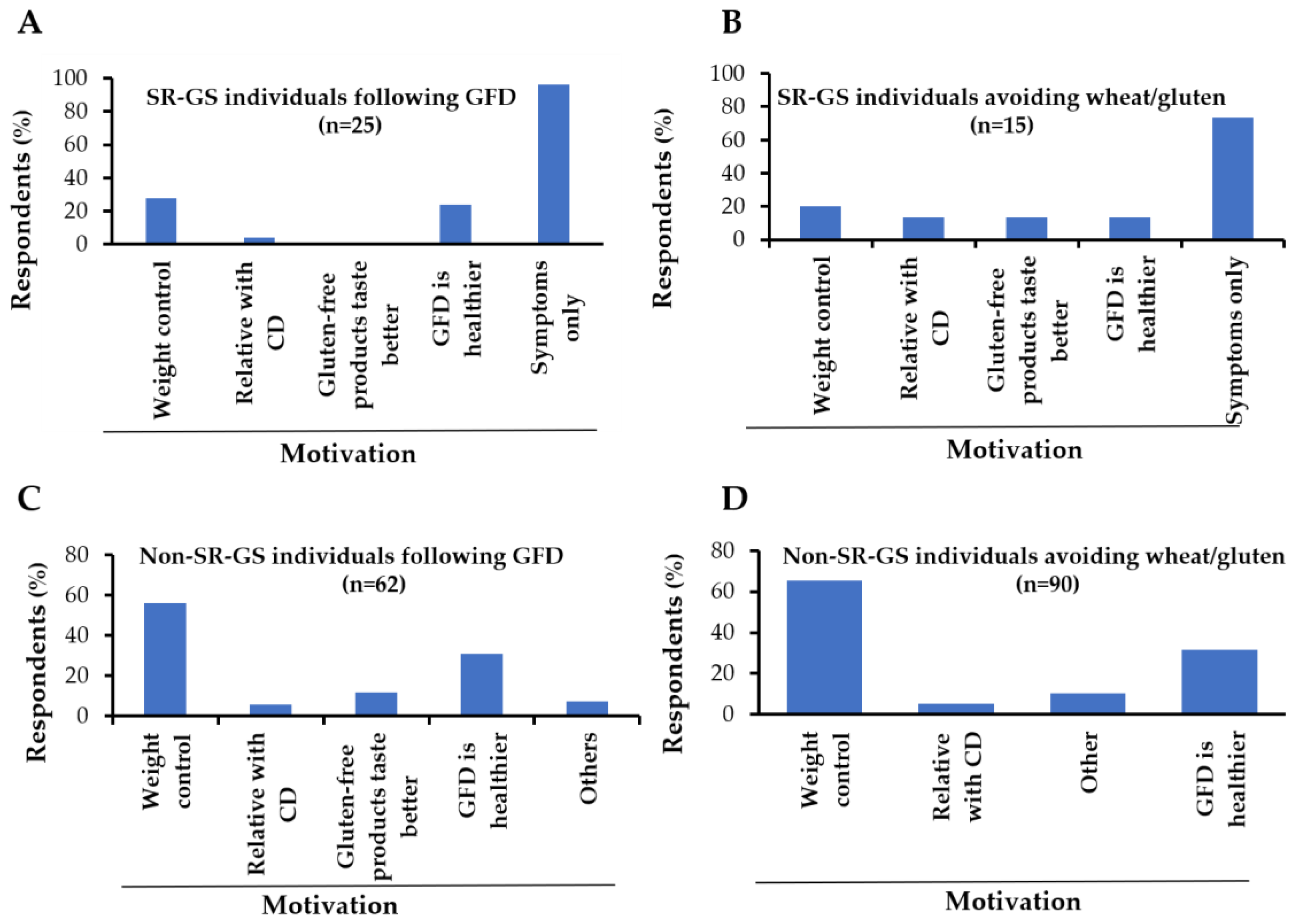
3.5. Reasons for Gluten-Free Dietary Non-Compliance and Motivations for Following a GFD
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ontiveros, N.; Flores-Mendoza, L.; Canizalez-Román, V.; Cabrera-Chavez, F. Food allergy: Prevalence and food technology approaches for the control of ige-mediated food allergy. Austin J. Nutr. Food Sci. 2014, 2, 1029. [Google Scholar]
- Sapone, A.; Bai, J.C.; Ciacci, C.; Dolinsek, J.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Rostami, K.; Sanders, D.S.; Schumann, M. Spectrum of gluten-related disorders: Consensus on new nomenclature and classification. BMC Med. 2012, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Hill, I.D.; Fasano, A.; Guandalini, S.; Hoffenberg, E.; Levy, J.; Reilly, N.; Verma, R. Naspghan clinical report on the diagnosis and treatment of gluten-related disorders. JPGN 2016, 63, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabo, I.; Mearin, M.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C. European society for pediatric gastroenterology, hepatology, and nutrition guidelines for the diagnosis of coeliac disease. JPGN 2012, 54, 136–160. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; Hardy, M.; Cabrera-Chavez, F. Assessing of celiac disease and nonceliac gluten sensitivity. Gastroenterol. Res. Pract. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinsek, J. Diagnosis of non-celiac gluten sensitivity (ncgs): The salerno experts’ criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef] [PubMed]
- Van Gils, T.; Nijeboer, P.; IJssennagger, C.E.; Sanders, D.S.; Mulder, C.J.; Bouma, G. Prevalence and characterization of self-reported gluten sensitivity in the netherlands. Nutrients 2016, 8, 714. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Lewis, N.R.; Hadjivassiliou, M.; Winfield, S.N.; Rugg, N.; Kelsall, A.; Newrick, L.; Sanders, D.S. A uk study assessing the population prevalence of self-reported gluten sensitivity and referral characteristics to secondary care. Eur. J. Gastroenterol. Hepatol. 2014, 26, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Chávez, F.; Dezar, G.V.; Islas-Zamorano, A.P.; Espinoza-Alderete, J.G.; Vergara-Jiménez, M.J.; Magaña-Ordorica, D.; Ontiveros, N. Prevalence of self-reported gluten sensitivity and adherence to a gluten-free diet in argentinian adult population. Nutrients 2017, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Chávez, F.; Granda-Restrepo, D.M.; Arámburo-Gálvez, J.G.; Franco-Aguilar, A.; Magaña-Ordorica, D.; Vergara-Jiménez, M.D.J.; Ontiveros, N. Self-reported prevalence of gluten-related disorders and adherence to gluten-free diet in colombian adult population. Gastroenterol. Res. Pract. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; López-Gallardo, J.A.; Vergara-Jiménez, M.J.; Cabrera-Chávez, F. Self-reported prevalence of symptomatic adverse reactions to gluten and adherence to gluten-free diet in an adult mexican population. Nutrients 2015, 7, 6000–6015. [Google Scholar] [CrossRef] [PubMed]
- Dall’Asta, C.; Scarlato, A.P.; Galaverna, G.; Brighenti, F.; Pellegrini, N. Dietary exposure to fumonisins and evaluation of nutrient intake in a group of adult celiac patients on a gluten-free diet. Mol. Nutr. Food Res. 2012, 56, 632–640. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Robins, G.; Burley, V.; Howdle, P. Evidence of high sugar intake, and low fibre and mineral intake, in the gluten-free diet. Aliment. Pharmacol. Ther. 2010, 32, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Hallert, C.; Grant, C.; Grehn, S.; Grännö, C.; Hultén, S.; Midhagen, G.; Ström, M.; Svensson, H.; Valdimarsson, T. Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years. Aliment. Pharmacol. Ther. 2002, 16, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- Curtis, B.C.; Rajaram, S.; Gómez, M. Bread Wheat: Improvement and Production; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2002; ISBN 9251048096. [Google Scholar]
- Peña, A.S.; Crusius, J.B.A. Central america in transition: From maize to wheat challenges and opportunities. Nutrients 2015, 7, 7163–7171. [Google Scholar] [CrossRef] [PubMed]
- Simons, F.E.R.; Ardusso, L.R.; Bilò, M.B.; El-Gamal, Y.M.; Ledford, D.K.; Ring, J.; Sanchez-Borges, M.; Senna, G.E.; Sheikh, A.; Thong, B.Y. World allergy organization guidelines for the assessment and management of anaphylaxis. World Allergy Org. J. 2011, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; Valdez-Meza, E.; Vergara-Jiménez, M.; Canizalez-Román, A.; Borzutzky, A.; Cabrera-Chávez, F. Parent-reported prevalence of food allergy in mexican schoolchildren: A population-based study. Allergol. Immunopathol. 2016, 44, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Abadie, V.; Sollid, L.M.; Barreiro, L.B.; Jabri, B. Integration of genetic and immunological insights into a model of celiac disease pathogenesis. Annu. Rev. Immunol. 2011, 29, 493–525. [Google Scholar] [CrossRef] [PubMed]
- CentralAmericaData.com. El Salvador: Más Producción de Harina de Trigo. Available online: https://www.centralamericadata.com/es/article/home/El_Salvador_Ms_produccin_de_harina_de_trigo (accessed on 4 February 2018).
- Dirección General de Estadística y Censos (DIGESTYC). Indice de Precios al Consumidor (ipc). Canasta Básica Alimentaria. Available online: http://www.digestyc.gob.sv/index.php/servicios/en-linea/canasta-basica-alimentaria.html (accessed on 4 February 2018).
- DiGiacomo, D.V.; Tennyson, C.A.; Green, P.H.; Demmer, R.T. Prevalence of gluten-free diet adherence among individuals without celiac disease in the USA: Results from the continuous national health and nutrition examination survey 2009–2010. Scand. J. Gastroenterol. Suppl. 2013, 48, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Branchi, F.; Pearson, K.; Priest, J.; Sanders, D.S. A study evaluating the bidirectional relationship between inflammatory bowel disease and self-reported non-celiac gluten sensitivity. Inflamm. Bowel. Dis. 2015, 21, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in fodmaps reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Am. J. Gastroenterol. 2011, 106, 508. [Google Scholar] [CrossRef] [PubMed]
- Gujral, N.; Freeman, H.J.; Thomson, A.B. Celiac disease: Prevalence, diagnosis, pathogenesis and treatment. World J. Gastroenterol. 2012, 18, 6036. [Google Scholar] [CrossRef] [PubMed]
- Assiri, A.M.; Saeed, A.; Saeed, E.; El-Mouzan, M.I.; Alsarkhy, A.A.; Al-Turaiki, M.; Al-Mehaidib, A.; Rashid, M.; Ullah, A. Assessment of knowledge of celiac disease among health care professionals. Saudi. Med. J. 2015, 36, 751. [Google Scholar] [CrossRef] [PubMed]
- Vieira, C.; Matos, M.; Quaresma, T.; de Oliveira, J.; Ferreira, C.D.; Silva, A.; Diniz-Santos, D.; Silva, L.R. What do brazilian pediatricians know about celiac disease? Dig. Dis. Sci. 2011, 56, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Cromeyer, M.; Gutiérrez, R.A.; Zaldívar, K.; Crusius, J.B.A.; Peña, A.S. Celiac disease in el salvador. In Celiac Disease and Non-Celiac Gluten Sensitvity; Rodrigo, L., Peña, A.S., Eds.; OmniaScience Monographs: Barcelona, Spain, 2014. [Google Scholar]
- Volta, U.; Bardella, M.T.; Calabrò, A.; Troncone, R.; Corazza, G.R. An italian prospective multicenter survey on patients suspected of having non-celiac gluten sensitivity. BMC Med. 2014, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Mahadev, S.; Simpson, S.; Lebwohl, B.; Lewis, S.K.; Tennyson, C.A.; Green, P.H. Is dietitian use associated with celiac disease outcomes? Nutrients 2013, 5, 1585–1594. [Google Scholar] [CrossRef] [PubMed]
- Pember, S.E.; Rush, S.E. Motivation for gluten-free diet adherence among adults with and without a clinically diagnosed gluten-related illness. Calif. J. Health Promot 2016, 14, 68–73. [Google Scholar]
- Golley, S.; Corsini, N.; Topping, D.; Morell, M.; Mohr, P. Motivations for avoiding wheat consumption in australia: Results from a population survey. Public Health Nutr. 2015, 18, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Burks, A.W.; Sampson, H.A. Clinical features of acute allergic reactions to peanut and tree nuts in children. Pediatrics 1998, 102, 6. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Definition | |
|---|---|---|
| Adverse reaction to food | Subjects who reported that the food-induced symptoms occurred always or most of the time (recurrent) or sometimes (non-recurrent). | |
| Self-reported physician-diagnosed (SR-PD *) celiac disease (CD *) | Subjects who reported that a physician or a health professional diagnosed celiac disease and were also following a GFD *. | |
| Wheat allergy | SR-PD wheat allergy (WA *) | Subjects who reported that a physician diagnosed wheat allergy and were also following a GFD * |
| SR-WA * | Subjects who reported recurrent adverse reactions convincing of food allergy. | |
| SR-GS * | Subjects who met criteria for recurrent adverse reactions to oral wheat/gluten and were also following a GFD *. | |
| NCGS ** | SR-PD NCGS * | Subjects who reported that a physician diagnosed them and were also following a GFD *. |
| SR-NCGS * | Subjects who met the following: (1) individuals who did not meet criteria for self-reported physician-diagnosed CD * or wheat allergy; (2) individuals who did not meet criteria for self-reported wheat allergy; and (3) individuals who met criteria for SR-GS *. | |
| Condition | (+) Cases * | Mean Age in Years (range) | Prevalence by Gender (95% CI) | p Value | General Prevalence (95% CI) |
|---|---|---|---|---|---|
| Adverse reaction to foods | Total = 272 | 37.14 (18–84) | M 9.7 (8.2–11.4) F 10.8 (9.2–12.6) | 0.222 | 20.5 (18.5–22.85) |
| M = 129 | |||||
| F = 144 | |||||
| Adverse reaction to wheat/gluten | Total = 60 | 42.23 (19–77) | M 1.8 (1.2–2.6) F 2.7 (1.9–3.7) | 0.112 | 4.5 (3.5–5.7) |
| M = 24 | |||||
| F = 36 | |||||
| (a) Self-Reported Gluten sensitivity (SR-GS **) | Total = 41 | 43.65 (20–72) | M 0.9 (0.5–1.6) F 2.1(1.4–3.0) | 0.011 | 3.1 (2.3–4.2) |
| M = 13 | |||||
| F = 28 | |||||
| (b) SR-PD ** Celiac disease | Total = 2 | 43.5 (26–61) | M 0.07(0.003–0.3) F 0.07(0.003–0.3) | 1.000 | 0.15 (0.04–0.5) |
| M = 1 | |||||
| F = 1 | |||||
| (c) Wheat allergy | Total = 10 | 48.1 (30–72) | M 0.3 (0.1–0.7) F 0.4 (0.2–0.9) | 0.542 | 0.75 (0.4–1.3) |
| M = 4 | |||||
| F = 6 | |||||
| (d) NCGS ** | Total = 13 | 43.69(27–55) | M 0.3 (0.1–0.7) F 0.6 (0.3–1.2) | 0.172 | 0.98 (0.5–1.6) |
| M = 4 | |||||
| F = 9 | |||||
| Adherence to GFD ** | Total = 93 | 41.75 (18–72) | M 3.5 (2.6–4.6) F 3.4 (2.6–4.5) | 1.000 | 7.0 (5.7–8.5) |
| M = 47 | |||||
| F = 46 | |||||
| Avoid wheat/gluten-containing foods | Total = 110 | 42.0 (18–77) | M 3.4 (2.5–4.5) F 4.9 (3.8–6.2) | 0.036 | 8.3 (6.9–9.9) |
| M = 45 | |||||
| F = 65 |
| Individual ID | Diagnosed by | Diagnosed Disorders | Following a GFD * | Excluded or Re-Classified | Criteria for Exclusion/Inclusion |
|---|---|---|---|---|---|
| 0042 | Homeopathic physician | WA * CD * NCGS * | Yes | Excluded | CD or WA does not co-exist with NCGS. The self-reported symptoms did not met criteria for WA |
| 0331 | Pediatrician | WA * NCGS * | Yes | Re-classified | The self-reported symptoms were convincing of WA |
| 0550 | Physician | ||||
| 0602 | Allergologist | ||||
| 0742 | Dietitian | WA * NCGS * | Yes | Excluded | CD or WA does not co-exist with NCGS. The self-reported symptoms did not met criteria for WA |
| 0743 | Physician | WA * CD * NCGS * | No | ||
| 1314 | Gastroenterologist | WA * CD * NCGS * | Yes |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ontiveros, N.; Rodríguez-Bellegarrigue, C.I.; Galicia-Rodríguez, G.; Vergara-Jiménez, M.D.J.; Zepeda-Gómez, E.M.; Arámburo-Galvez, J.G.; Gracia-Valenzuela, M.H.; Cabrera-Chávez, F. Prevalence of Self-Reported Gluten-Related Disorders and Adherence to a Gluten-Free Diet in Salvadoran Adult Population. Int. J. Environ. Res. Public Health 2018, 15, 786. https://doi.org/10.3390/ijerph15040786
Ontiveros N, Rodríguez-Bellegarrigue CI, Galicia-Rodríguez G, Vergara-Jiménez MDJ, Zepeda-Gómez EM, Arámburo-Galvez JG, Gracia-Valenzuela MH, Cabrera-Chávez F. Prevalence of Self-Reported Gluten-Related Disorders and Adherence to a Gluten-Free Diet in Salvadoran Adult Population. International Journal of Environmental Research and Public Health. 2018; 15(4):786. https://doi.org/10.3390/ijerph15040786
Chicago/Turabian StyleOntiveros, Noé, Cecilia Ivonne Rodríguez-Bellegarrigue, Gerardo Galicia-Rodríguez, Marcela De Jesús Vergara-Jiménez, Elia María Zepeda-Gómez, Jesús Gilberto Arámburo-Galvez, Martina Hilda Gracia-Valenzuela, and Francisco Cabrera-Chávez. 2018. "Prevalence of Self-Reported Gluten-Related Disorders and Adherence to a Gluten-Free Diet in Salvadoran Adult Population" International Journal of Environmental Research and Public Health 15, no. 4: 786. https://doi.org/10.3390/ijerph15040786
APA StyleOntiveros, N., Rodríguez-Bellegarrigue, C. I., Galicia-Rodríguez, G., Vergara-Jiménez, M. D. J., Zepeda-Gómez, E. M., Arámburo-Galvez, J. G., Gracia-Valenzuela, M. H., & Cabrera-Chávez, F. (2018). Prevalence of Self-Reported Gluten-Related Disorders and Adherence to a Gluten-Free Diet in Salvadoran Adult Population. International Journal of Environmental Research and Public Health, 15(4), 786. https://doi.org/10.3390/ijerph15040786