Public Health and Unconventional Oil and Gas Extraction Including Fracking: Global Lessons from a Scottish Government Review


Abstract
:1. Introduction
2. Materials and Methods
- (1)
- industry demands and planning applications, after the UK government granted licenses to extract UOGE in Scotland, to develop unconventional gas extraction which includes fracking but also coal bed methane and underground coal gasification;
- (2)
- “public demands” for the health and other related consequences, including direct and indirect costs, of UOGE to be assessed;
- (3)
- the existing evidence base on public health and related reports from other jurisdictions on UOGE either to inform national, regional or project specific “health impact assessment” decisions.
- (a)
- Occupational Health. Worker health and safety should be an integral part of any public health assessment of fracking in terms of exposure to risks. It could involve large numbers depending on wells drilled. Drillers may be the canaries of the industry. Checking on occupational health and safety where exposures may be wider and higher and longer than those experienced by the rest of the population could provide a means of assessing possible longer-term impacts on local communities.
- (b)
- Climate change. This impacts on global public health through methane emissions but also through emissions of other constituents, such as gasoline and diesel involved in extraction, production and distribution of shale gas and will directly or indirectly affect national, regional, and local health—in some places through flooding or fire. Linked to climate change and shale gas are potential public health problems: for example, shale gas use in plastics production and the impacts of plastic products. These are not currently considered in either policy or health assessments but may be in the future. A process ensuring independent and rigorous assessment of what fracking industry regulation does or can do in practice is again necessary.
- (c)
- Regulation. How exactly fracking is conducted, monitored and how safe or hazardous it is, may partly depend on regulations, enforcement, and regulatory resources. Therefore, assessments of regulation are critical not just to mitigation but to the policy approval process.
- (d)
- Industry practice. This has been suggested as a major factor in determining the public health threats of fracking and its acceptability, although the intrinsic technology and related materials along with the geology and hydrology of sites may sometimes be potentially greater factors. A process ensuring independent and rigorous assessment of what the fracking industry does in practice is again necessary. The role of consultants and independent experts in preparing health impact assessments for industry merits attention when assessing the policy process. In the UK, such consultants have prepared industry guidance at a national level on how fracking might be done safely.
- (e)
- Economic factors. Economic benefits or economic damage, linked to employment and trade, from the fracking industry may have positive and negative impacts on public health. Some governments may weight these factors more highly than public health in their policy decisions on the industry. Although difficult to measure and often with a large range of impacts, a detailed assessment of the economics is justified based on independent assessments open to scrutiny.
- (f)
- Vulnerable populations. These are of particular concern to bodies such as the WHO as well as many national governments. These populations may be disproportionately disadvantaged or theoretically benefitted by fracking. This flags the need for policy decisions to consider short-, medium-, and long-term effects of fracking—something relevant to all the headings listed so far. Hence it is important their position is addressed in the assessment process.
- (g)
- Social determinants of health. These merit inclusion and are a public health policy priority for many governments as well as municipal bodies. They are connected to a much bigger picture of social and economic development and decline especially regarding “boomtown” effects.
- (h)
- Peer review. Peer review should automatically occur with scientific journal papers but does not always happen with industry, commercial consultancy, or government reports. The necessity for such independent review is critical to the confidence that can be placed in findings. Several but not all the publications we examine rightly distinguished between peer reviewed and non-peer reviewed literature. Reports not only need to be perceived as open to such scrutiny but should demonstrate that they have undergone that process. This is one important mechanism in helping agencies and the public to have confidence in material used to make policy. The absence of peer review would not necessarily invalidate a publication, but its presence will usually enhance its credibility and should perhaps be integral to any policy process assessment.
- (i)
- Declaration of interests. This is needed to guarantee transparency in the policy making process and will ensure any conflict of interests in the preparation of fracking assessments is made clear at the outset. Again, the absence of a declaration of interests when there are competing interests would damage a publication, but its inclusion would not necessarily do so and hence such declarations should be viewed as essential to the policy evaluation process.
- (j)
- Public engagement. There is widespread recognition of the importance of consulting with various publics who may be impacted by the development of UOGE. From a governance perspective the outcomes of policy and regulatory decision making are seen to be more stable and legitimate if key stakeholders are consulted about proposals, in a timely and meaningful manner. In theory this can lead to effective partnership working and co-regulation by stakeholders. In relation to public health the inclusion of communities at early stages in the planning and during research phases of HIAs is not only considered best practice but can help identify and calibrate public health issues among various communities and vulnerable populations.
3. Results
3.1. The Context
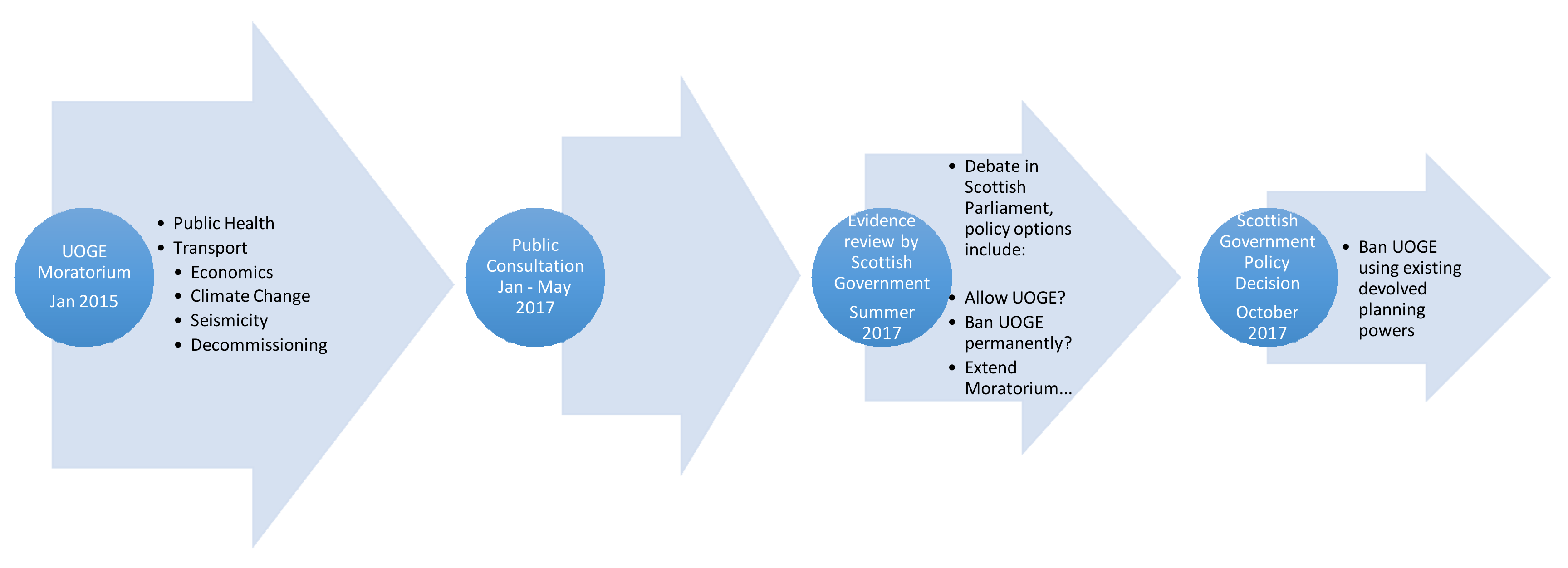
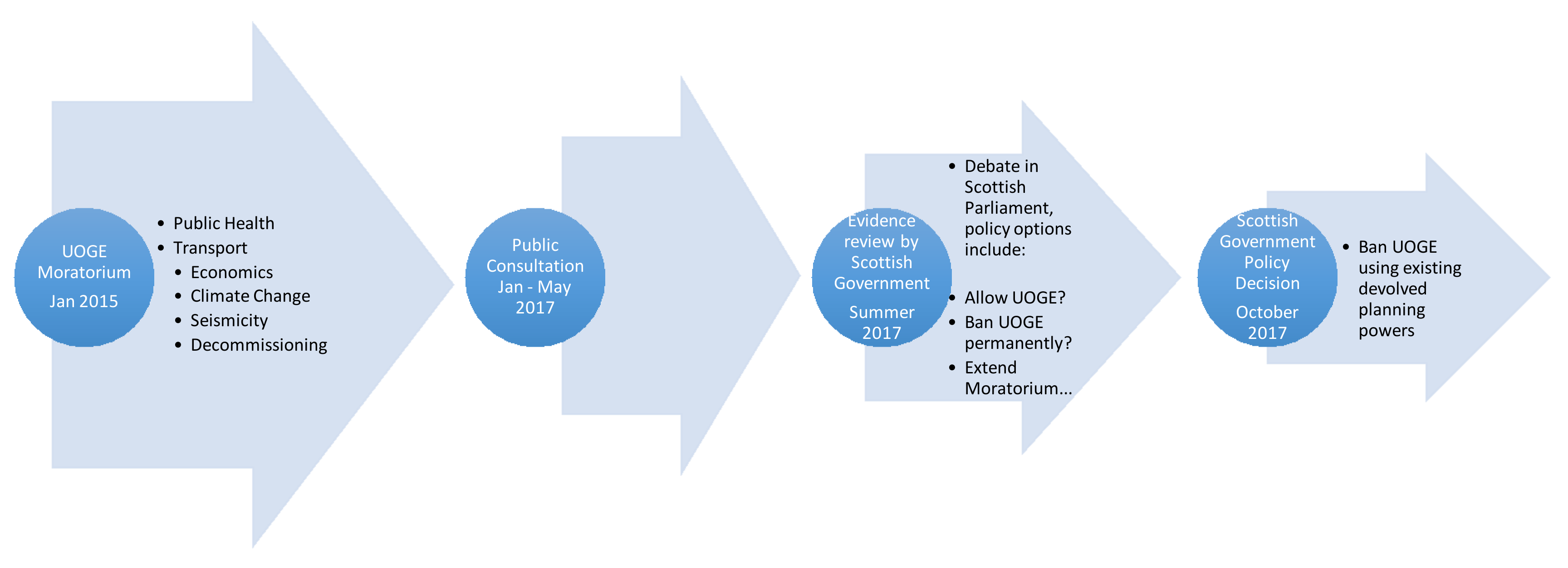
3.2. The Scottish Moratorium
3.2.1. The Health Impact Assessment
3.2.2. Wider Impact Assessments Conducted by the Scottish Government
3.2.3. The Public Consultation Exercise
3.2.4. The Scottish Government UOGE Review in a Global Context
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CBM | Coal Bed Methane |
| GDP | Gross Domestic Product |
| HIA | Health Impact Assessment |
| HIAUOGS | Health Impact Assessment of Unconventional Oil and Gas in Scotland |
| HPS | Health Protection Scotland |
| UCG | Underground Coal Gasification |
| UOGE | Unconventional Oil and Gas Extraction |
| UOG | Unconventional Oil and Gas |
References
- Saunders, P.J.; McCoy, D.; Goldstein, R.; Saunders, A.T.; Munroe, A. A review of the public health impacts of unconventional natural gas development. Environ. Geochem. Health 2016, 1–57. [Google Scholar] [CrossRef] [PubMed]
- Finkel, M.L. The Human and Environmental Impact of Fracking: How Fracturing Shale for Gas Affects Us and Our World; Praeger: Santa Barbara, CA, USA, 2015; ISBN 978-1-4408-3259-8. [Google Scholar]
- Public Health England. Review of the Public Health Impacts of Exposures to Chemical and Radioactive Pollutants as a Result of the Shale Gas Extraction Process; Centre for Radiation, Chemical and Environmental Hazards: Didcot, UK, 2014; ISBN 978-0-85951-752-2. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/332837/PHE-CRCE-009_3-7-14.pdf (accessed on 23 November 2017).
- Watterson, A.; Dinan, W. The UK’s ‘Dash for Gas’: A Rapid Evidence Assessment of Fracking for Shale Gas, Regulation and Public Health. New Solut. 2017, 27, 68–91. [Google Scholar] [CrossRef] [PubMed]
- Watterson, A.; Dinan, W. A Rapid Evidence Assessment of Regulation and Regulatory Practices Involved in Fracking and its Public Health Implications. 2016. Available online: http://www.regulatingscotland.org/report/frackingandregulation.pdf (accessed on 23 November 2017).
- Nyberg, D.; Wright, C.; Kirk, J. Re-producing a neoliberal political regime: Competing justifications and dominance in disputing fracking. In Justification, Evaluation and Critique in the Study of Organizations: Contributions from French Pragmatist Sociology; Cloutier, C., Gond, J.P., Leca, B., Eds.; Emerald Publishing Limited: Bingley, UK, 2017; Volume 52, pp. 143–171. ISBN 978-1-78714-379-1. [Google Scholar]
- Heusner, G.; Sloto, A.; Galperin, J. Defining and Closing the Hydraulic Fracturing Governance Gap. Den. L. Rev. 2016, 95, 191. [Google Scholar] [CrossRef]
- Kirkman, R.; Arson, C.F.; Stewart, L.; Harris, R.; Francis, A. The Risks of fracking & the responsibilities of engineers. Elem. Sci. Anth. 2017, 5, 1–12. [Google Scholar] [CrossRef]
- Ma, L.; Hurtado, A.; Eguilior, S.; Llamas Borrajo, J.F. A model for predicting organic compounds concentration change in water associated with horizontal hydraulic fracturing. Sci. Total Environ. 2018, 625, 1164–1174. [Google Scholar] [CrossRef]
- Wilson, M.P.; Worrall, F.; Davies, R.J.; Hart, A. Shallow Aquifer Vulnerability from Subsurface Fluid Injection at a Proposed Shale Gas Hydraulic Fracturing Site. Water Resour. Res. 2017, 53, 9922–9940. [Google Scholar] [CrossRef]
- Maguire, K.; Winters, J.V. Energy Boom and Gloom? Local Effects of Oil and Natural Gas Drilling on Subjective Well-Being. Growth Chang. A J. Urban Reg. Policy 2017, 48, 590–610. [Google Scholar] [CrossRef]
- Yu, M.; Quddus, N.; Peres, S.C.; Sachdeva, S.; Mannan, M.S. Development of a safety management system (SMS) for drilling and servicing operations within OSHA jurisdiction area of Texas. J. Loss Prev. Process Ind. 2017, 50, 266–274. [Google Scholar] [CrossRef]
- Fisher, M.P.; Mayer, A.; Vollet, K.; Hill, E.L.; Haynes, E.N. Psychosocial implications of unconventional natural gas development: Quality of life in Ohio’s Guernsey and Noble Counties. J. Environ. Psychol. 2018, 55, 90–98. [Google Scholar] [CrossRef]
- Sapouckey, S.A.; Kassotis, C.D.; Nagel, S.C.; Vandenberg, L.N. Prenatal Exposure to Unconventional Oil and Gas Operation Chemical Mixtures Altered Mammary Gland Development in Adult Female Mice. Endocrinology 2018, 159, 1277–1289. [Google Scholar] [CrossRef] [PubMed]
- Moortgat, J.; Schwartz, F.; Darrah, T.H. Numerical Modeling of Methane Leakage in Fractured Tight Formations. Groundwater 2018, 56. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.C.; Gilfilan, S.M.V.; Edlmann, K.; McDermott, C.I. Wastewater from hydraulic fracturing in the UK: assessing the viability and cost of management. Environ. Sci. Water Res. Technol. 2018, 4, 325–335. [Google Scholar] [CrossRef]
- BBC. Dart Energy Forth Valley Gas Inquiry Begins. 2014. Available online: http://www.bbc.co.uk/news/uk-scotland-tayside-central-26625385 (accessed on 23 November 2017).
- The Scottish Government. Independent Expert Scientific Panel—Report on Unconventional Oil and Gas; The Scottish Government: Edinburgh, Scotland, UK, 2014; ISBN 9781784126834. Available online: http://www.gov.scot/Resource/0045/00456579.pdf (accessed on 23 November 2017).
- Scottish Government. Moratorium Called on Fracking. 2015. Available online: https://news.gov.scot/news/moratorium-called-on-fracking#downloads (accessed on 24 November 2017).
- BBC. Scottish Government to ‘Block’ Underground Coal Gasification. 2016. Available online: http://www.bbc.co.uk/news/uk-scotland-scotland-politics-37565927 (accessed on 24 November 2017).
- Health Protection Scotland. Available online: http://www.hps.scot.nhs.uk/resourcedocument.aspx?resourceid=2049 (accessed on 18 February 2018).
- Health Protection Scotland. A Health Impact Assessment of Unconventional Oil and Gas in Scotland (2 Volumes). Glasgow, 2016. Available online: http://www.hps.scot.nhs.uk/enviro/unconventionalgas.aspx (accessed on 20 December 2016).
- Law, A.; Hays, J.; Shonkoff, S.; Finkel, M. Public Health England’s draft report on shale gas extraction. BMJ 2014, 348, 2728. [Google Scholar] [CrossRef] [PubMed]
- Reap, E. The risk of hydraulic fracturing on public health in the UK and the UK’s fracking legislation. Environ. Sci. Eur. 2015, 27, 27. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J. Fracking: Minding the Gaps. Environ. Law Rev. 2015, 17, 8–21. [Google Scholar] [CrossRef]
- Watterson, A.; Dinan, W. Health Impact Assessments, Regulation, and the Unconventional Gas Industry in the UK: Exploiting Resources, Ideology, and Expertise? New Solut. 2016, 25, 480–512. [Google Scholar] [CrossRef] [PubMed]
- Szolucha, A. The Human Dimension of Shale Gas Developments in Lancashire. University of Bergen, 2016. Available online: http://appgshalegas.uk/wp-content/uploads/2016/05/The-Human-Dimension-of-Shale-Gas-Developments-in-Lancashire.pdf (accessed on 7 February 2017).
- Ricardo Energy and Environment. Understanding and Mitigating Community Level Impacts from Transportation. Report for Scottish Government; 2016. Available online: http://www.gov.scot/Resource/0050/00509327.pdf (accessed on 7 February 2017).
- Hays, J.; McCawley, M.; Shonkoff, S.B. Public health implications of environmental noise associated with unconventional oil and gas development. Sci. Total Environ. 2016, 580, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Haswell, M.R.; Bethmont, A. Health concerns associated with unconventional gas mining in rural Australia. Rural Remote Health 2016, 16, 3825. [Google Scholar] [PubMed]
- British Geological Survey. Understanding and Monitoring Induced Seismic Activity. OR/10/042; Nottingham, 2016. Available online: http://www.gov.scot/Resource/0050/00509318.pdf (accessed on 20 December 2016).
- KPMG. Economic Impact Assessment of the Potential Development of Unconventional Oil and Gas in Scotland: A Report for the Scottish Government; Scottish Government: Edinburgh, Scotland, UK, 2016. Available online: http://www.gov.scot/Resource/0050/00509321.pdf (accessed on 7 February 2017).
- Scottish Government. Unconventional Oil and Gas Research Published. 2016. Available online: http://news.gov.scot/news/unconventional-oil-and-gas-research-published (accessed on 10 July 2017).
- Committee on Climate Change. Scottish Unconventional Oil and Gas: Compatibility with Scottish Greenhouse Gas Emissions Targets. 2016. Available online: http://www.gov.scot/Resource/0050/00509324.pdf (accessed on 24 November 2017).
- AECOM. Unconventional Oil and Gas: Decommissioning, Site Restoration and Aftercare—Obligations and Treatment of Financial Liabilities. 2016; ISBN 9781786523945. Available online: http://www.gov.scot/Resource/0050/00509373.pdf (accessed on 24 November 2017).
- Scottish Government. Talking ‘Fracking’: A Consultation on Unconventional Oil and Gas—Analysis of Responses. 2017. Available online: http//www.gov.scot/Publications/2017/10/9813 (accessed on 13 November 2017).
- Wheelhouse, P. Unconventional Oil and Gas—Statement. Scottish Government, 2017. Available online: http://news.gov.scot/speeches-and-briefings/unconventional-oil-and-gas-statement (accessed on 24 November 2017).
- INEOS. INEOS Challenges Scottish Government’s Ban. 2018. Available online: http://www.ineos.com/news/ineos-group/ineos-challenges-scottish-governments-ban/ (accessed on 18 February 2018).
- Victoria State Government. Onshore Gas Community Information. Available online: http://onshoregas.vic.gov.au (accessed on 24 November 2017).
- Carnegy, H. France’s Constitutional Council Upholds Ban on Fracking. 2013. Available online: http://www.ft.com/content/34b5dad6-3261-11e3-b3a7-00144feab7de (accessed on 24 November 2017).
- Task Force on Shale. Assessing the Impact of Shale Gas on the Local Environment and Health. 2015. Available online: http://www.taskforceonshalegas.uk/reports/assessing-the-impact-of-shale-gas-on-the-local-environment-and-health (accessed on 24 November 2017).
- Werner, A.K.; Wink, S.; Watt, K.; Jagals, P. Environmental Health Impacts of Unconventional Natural Gas Development: A Review of the Current Strength of Evidence. Sci. Total Environ. 2015, 501, 1127–1141. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine of the National Academies, Board on Population Health and Public Health Practice. Health Impact Assessment of Shale Gas Extraction: Workshop Summary; National Academies Press: Washington, DC, USA, 2014. [Google Scholar]
- Ben Cave Associates. Overview Report HIA Work Concerning Planning Applications for Temporary Shale Gas Exploration: Health Impact Assessment Support, Shale Gas Exploration LANCASHIRE County Council, 2 September 2014; Ben Cave Associates Ltd.: Leeds, UK, 2014; Available online: http://bit.ly/1BsZ3Au (accessed on 24 November 2017).
- Maryland Institute for Applied Environmental Health. Potential Public Health Impacts of Natural Gas Development and Production in the Marcellus Shale in Western Maryland. Report for the Maryland Department of the Environment and the Maryland Department of Health and Mental Hygiene. 2014. Available online: http://www.marcellushealth.org/final-report.html (accessed on 24 November 2017).
- New York State Department of Health. Public Health Review of High Volume Hydraulic Fracturing for Shale Gas Development. 2014. Available online: http://www.health.ny.gov/press/reports/docs/high_volume_hydraulic_fracturing.pdf (accessed on 24 November 2017).
- Bloomfield, M. Support to the Identification of Potential Risks for the Environment and Human Health Arising from Hydrocarbons Operations Involving Hydraulic Fracturing in Europe; AEA Technology plc: Didcot, UK, 2014; Available online: http://ec.europa.eu/environment/integration/energy/pdf/fracking%20study.pdf (accessed on 24 November 2017).
- Office of the Chief Medical Officer of Health. Recommendations Concerning Shale Gas Development in New Brunswick. Office of the Chief Medical Officer of Health: New Brunswick, 2012. Available online: http://leg-horizon.gnb.ca/e-repository/monographs/31000000047096/31000000047096.pdf (accessed on 16 February 2018).
- American Public Health Association. The Environmental and Occupational Health Impacts of High-Volume Hydraulic Fracturing of Unconventional Gas Reserves; American Public Health Association: Washington, DC, USA, 2012; Available online: http://www.apha.org/advocacy/policy/policysearch/default.htm?id=1439 (accessed on 24 November 2017).
- Witter, R.; McKenzie, L.; Towle, M.; Stinson, K.; Scott, K.; Newman, L.; Adgate, J. Health Impact Assessment for Battlement Mesa, Garfield County Colorado; University of Colorado, Colorado School of Public Health: Denver, CO, USA, 2010; Available online: http://www.garfield-county.com/public-health/documents/1%20%20%20Complete%20HIA%20without%20Appendix%20D.pdf (accessed on 16 February 2018).
- Gornall, J. Public Health England’s troubled trail. BMJ 2015, 351, h5826. [Google Scholar] [CrossRef] [PubMed]
- Witter, R.; Stinson, K.; Sackett, H.; Putter, S.; Kinney, G.; Teitelbaum, D.; Newman, L. Potential exposure-related human health effects of oil and gas development: A White Paper. In Colorado School of Public Health; University of Colorado: Denver, CO, USA, 2008; Available online: http://www.nrdc.org/sites/default/files/hea_08091702a.pdf (accessed on 24 November 2017).
- Gemmell, C. Independent Review of Underground Coal Gasification—Report to the Scottish Government. 2016. Available online: http://www.gov.scot/Resource/0050/00507473.pdf (accessed on 2 August 2017).
- Boyle, M.D.; Soneja, S.; Quirós-Alcalá, L.; Dalemarre, L.; Sapkota, A.R.; Sangaramoorthy, T.; Wilson, S.; Milton, D.; Sapkota, A. A pilot study to assess residential noise exposure near natural gas compressor stations. PLoS ONE 2017, 12, e0174310. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.K.; Smalley, K.B.; Selby-Nelson, E.M.; Hamel-Lambert, J.M.; Rosmann, M.R.; Barnes, T.A.; Abrahamson, D.; Meit, S.S.; GreyWolf, I.; Beckmann, S.; et al. Psychosocial Impact of Fracking: A Review of the Literature on the Mental Health Consequences of Hydraulic Fracturing. Int. J. Ment. Health Addict. 2017, 16, 1–15. [Google Scholar] [CrossRef]
- Meszaros, N.; Subedi, B.; Stamets, T.; Shifa, N. Assessment of Surface Water Contamination from Coalbed Methane Fracturing-Derived Volatile Contaminants in Sullivan County, Indiana, USA. Bull. Environ. Contam. Toxicol. 2017, 99, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Evanoski-Cole, A.R.; Gebhart, K.A.; Sive, B.C.; Zhou, Y.; Capps, S.L.; Day, D.E.; Prenni, A.J.; Schurman, M.I.; Sullivan, A.P.; Li, Y.; et al. Composition and sources of winter haze in the Bakken oil and gas extraction region. Atmos. Environ. 2017, 156, 77–87. [Google Scholar] [CrossRef]
- Maloney, K.O.; Baruch-Mordo, S.; Patterson, L.A.; Nicot, J.P.; Entrekin, S.A.; Fargione, J.E.; Kiesecker, J.M.; Konschnik, K.E.; Ryan, J.N.; Trainor, A.M.; et al. Unconventional oil and gas spills: Materials, volumes, and risks to surface waters in four states of the U.S. Sci. Total Environ. 2017, 581, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Casey, J.A.; Savitz, D.A.; Rasmussen, S.G.; Ogburn, E.L.; Pollak, J.; Mercer, D.G.; Schwartz, B.S. Unconventional Natural Gas Development and Birth Outcomes in Pennsylvania, USA. Epidemiology 2015, 27, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Jemielita, T.; Gerton, G.L.; Neidell, M.; Chillrud, S.; Yan, B.; Stute, M.; Howarth, M.; Saberi, P.; Fausti, N.; Penning, T.M. Unconventional Gas and Oil Drilling is Associated with Increased Hospital Utilization Rates. PLoS ONE 2015, 10, e0131093. [Google Scholar] [CrossRef]
- McKenzie, L.M.; Allshouse, W.B.; Byers, T.E.; Bedrick, E.J.; Serdar, B.; Adgate, J.L. Childhood hematologic cancer and residential proximity to oil and gas development. PLoS ONE 2017, 12, e0170423. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.G.; Ogburn, E.L.; McCormack, M.; Casey, J.A.; Bandeen-Roche, K.; Mercer, D.G. Association between unconventional natural gas development in the Marcellus shale and asthma exacerbations. JAMA Int. Med. 2016, 176, 1334–1343. [Google Scholar] [CrossRef] [PubMed]
- Stacy, S.L.; Brink, L.L.; Larkin, J.C.; Sadovsky, Y.; Goldstein, B.D.; Pitt, B.R.; Talbott, E.O. Perinatal Outcomes and Unconventional Natural Gas Operations in Southwest Pennsylvania. PLoS ONE 2015, 10, 0126425. [Google Scholar] [CrossRef] [PubMed]
- Tustin, A.W.; Hirsch, A.G.; Rasmussen, S.G.; Casey, J.A.; Bandeen-Roche, K.; Schwartz, B.S. Associations between Unconventional Natural Gas Development and Nasal and Sinus, Migraine Headache, and Fatigue Symptoms in Pennsylvania. Environ. Health Perspect. 2016, 125, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Solomon, G.M.; Morello-Frosch, R.; Zeise, L.; Faust, J.B. Cumulative Environmental Impacts: Science and Policy to Protect Communities. Annu. Rev. Public Health. 2016, 37, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Walser, T.; Bourqui, R.M.; Studer, C. Combination of life cycle assessment, risk assessment and human biomonitoring to improve regulatory decisions and policy making for chemicals. Environ. Impact Assess. Rev. 2017, 65, 156–163. [Google Scholar] [CrossRef]
- Shaffer, R.M.; Smith, M.N.; Faustman, E.M. Developing the Regulatory Utility of the Exposome: Mapping Exposures for Risk Assessment through Lifestage Exposome Snapshots (LEnS). Environ. Health Perspect. 2017, 125, 8. [Google Scholar] [CrossRef] [PubMed]
- Royal Society/Royal Academy of Engineering. Shale Gas Extraction in the UK: A Review of Hydraulic Fracturing. 2012. Available online: http://royalsociety.org/topics-policy/projects/shale-gas-extraction/report/ (accessed on 18 February 2018).
- Kemp, R. Shale Gas Planning Applications, Protesters, and Governance: Lessons from the UK. OGEL 2014, 12. Available online: www.ogel.org/article.asp?key=3470 (accessed on 7 February 2018).

{kind=link}
| Subject of Reports—All Published in the Winter of 2016 | Author | Key Findings |
|---|---|---|
| A Health Impact Assessment of Unconventional Oil and Gas in Scotland (HIAUOGS) [22] | Health Protection Scotland—NHS Scotland | Generic assessment. “Sufficient evidence” on a number of likely air and water environmental hazards and silica hazards to workers. Other evidence inadequate to decide if process poses a public health risk. |
| Climate change impacts [34] | Committee on Climate Change—independent body established under the Climate Change Act (2008) to advise the UK Government | Only compatible with Scotland’s climate change targets if (a) emissions limited through tight regulation; (b) Scottish UOGE production displaces imports (c) emissions from production of UOGE offset by reductions in other emissions in Scottish economy. |
| Decommissioning, site restoration and aftercare—obligations and treatment of financial liabilities [35] | AECOM—commercial consultant (provides design engineering services to oil and gas industry) | Assumes best practice and appropriate regulation and monitoring will ensure decommissioning succeeds. Notes a residual risk that a small proportion of wells may fail. |
| Understanding and mitigating community level impacts from transportation [28] | Ricardo Energy and Environment—commercial consultant | Assumes appropriate strategic policies are put in place, and appropriate mitigation is carried out, local communities would nevertheless experience an increase in traffic numbers, potentially for some years. |
| Understanding and monitoring induced seismic activity [31] | British Geological Survey—advises UK government on all aspects of geoscience, also provides geological advice to industry, academia, and the public | USA and Canada evidence suggests probability of induced earthquakes felt is small, although some examples exist of earthquakes large enough to be felt. |
| Economic impacts and scenario development [32] | KPMG | 1400 jobs created at peak in the Scottish economy bringing in, on average per year, 0.1% of Scottish GDP. Impacts on local house prices, road use, agriculture, visual amenity, environmental costs, and health costs. |
| Occup. Health | Climate Change | Regulation | Industry Practice | Economics and Employment | Vulnerable Populations | Social Determinants of Health | Peer Review | Decl of Interest | Public Engagement | |
|---|---|---|---|---|---|---|---|---|---|---|
| Scottish Government (2016) [33] | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ |
| Scottish Government (2014) [18] | . | √ | √ | . | . | x | . | x | √ | . |
| Finkel (2015) [2] | √ | √ | √ | √ | √ | . | √ | n/a | n/a | √ |
| Task Force on Shale (2015) [41] | . | √ | √ | . | √ | x | x | x | x | √ |
| Werner (2015) [42] | √ | . | √ | . | . | √ | √ | √ | √ | n/a |
| US Institute of Medicine (2014) [43] | √ | √ | √ | √ | √ | √ | √ | √ | n/a | x |
| Ben Cave Associates (2014) [44] | √ | √ | √ | √ | √ | √ | √ | n/a | √ | √ |
| Maryland Univ (2014) [45] | √ | √ | √ | √ | √ | √ | √ | √ | √ | x |
| PHE (2014) [3] | . | √ | . | . | x | x | x | n/a | n/a | |
| New York State (2014) [46] | √ | √ | √ | √ | . | x | √ | √ | n/a | . |
| AEA (2012) [47] | √ | √ | . | √ | . | x | x | x | n/a | n/a |
| New Brunswick (2012) [48] | √ | √ | √ | √ | √ | √ | n/a | . | ||
| APHA (2012) [49] | √ | √ | √ | √ | √ | √ | . | √ | n/a | x |
| Colorado Univ (2010) [50] | √ | x | . | √ | . | √ | √ | √ | √ | √ |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watterson, A.; Dinan, W. Public Health and Unconventional Oil and Gas Extraction Including Fracking: Global Lessons from a Scottish Government Review. Int. J. Environ. Res. Public Health 2018, 15, 675. https://doi.org/10.3390/ijerph15040675
Watterson A, Dinan W. Public Health and Unconventional Oil and Gas Extraction Including Fracking: Global Lessons from a Scottish Government Review. International Journal of Environmental Research and Public Health. 2018; 15(4):675. https://doi.org/10.3390/ijerph15040675
Chicago/Turabian StyleWatterson, Andrew, and William Dinan. 2018. "Public Health and Unconventional Oil and Gas Extraction Including Fracking: Global Lessons from a Scottish Government Review" International Journal of Environmental Research and Public Health 15, no. 4: 675. https://doi.org/10.3390/ijerph15040675
APA StyleWatterson, A., & Dinan, W. (2018). Public Health and Unconventional Oil and Gas Extraction Including Fracking: Global Lessons from a Scottish Government Review. International Journal of Environmental Research and Public Health, 15(4), 675. https://doi.org/10.3390/ijerph15040675