Physical Activity, a Critical Exposure Factor of Environmental Pollution in Children and Adolescents Health Risk Assessment

 ,
,
Abstract
:1. Introduction
2. Physical Activity, Environmental Pollution and Heath of Adolescents
2.1. Global Adolescents’ Physical Activity Level and Fitness
2.2. Air Pollution and Children’s Health
3. Exposure Factor in Environmental Health Assessment
4. Inhalation Exposure Factors of Children
4.1. Methods of Measuring Inhalation Rate
4.2. Data Collection of Physical Activity Patterns
5. Relationship between Physical Activity and Inhalation Exposure Factor of Children and Adolescents
5.1. Relationship between Physical Activity and Inhalation Rate
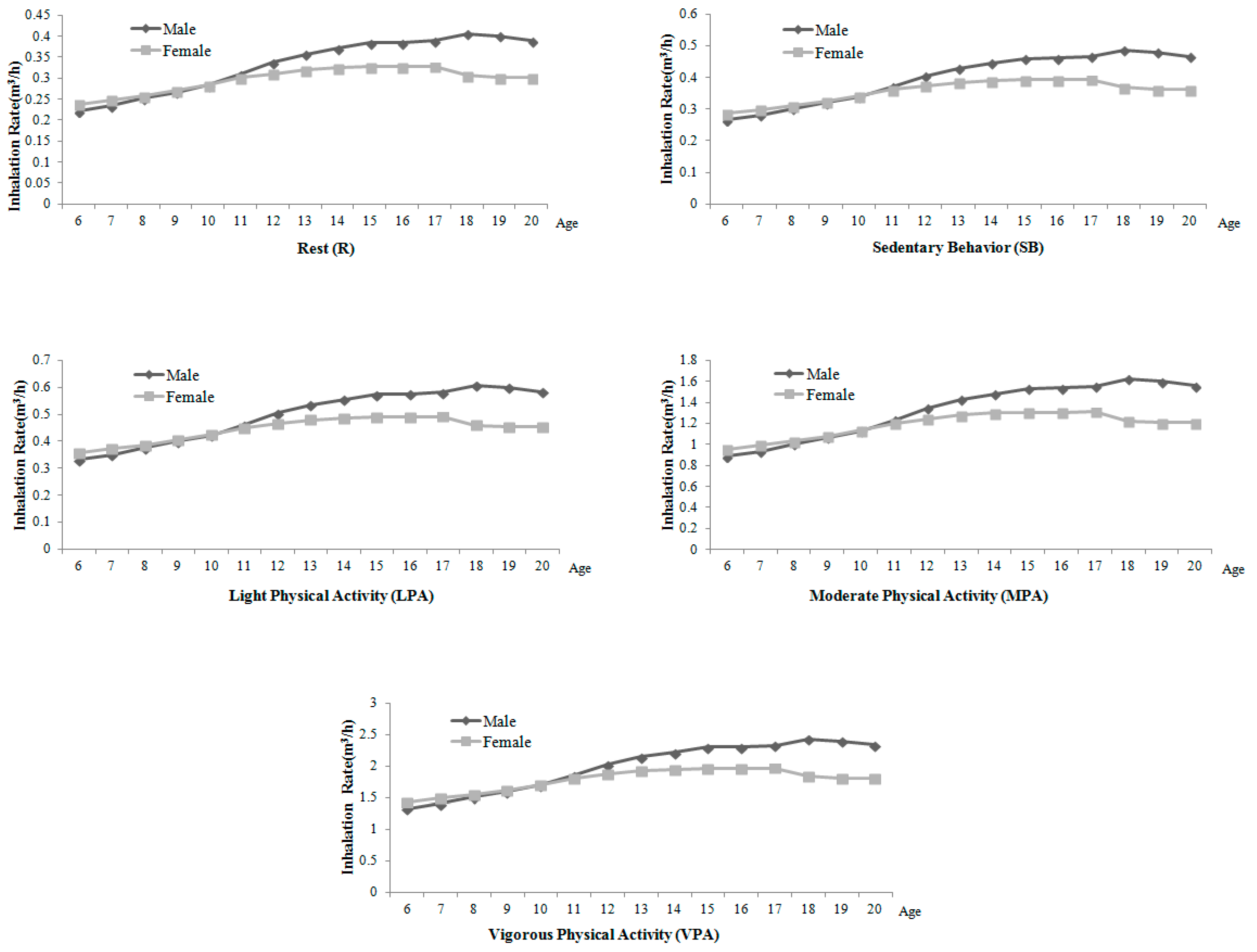
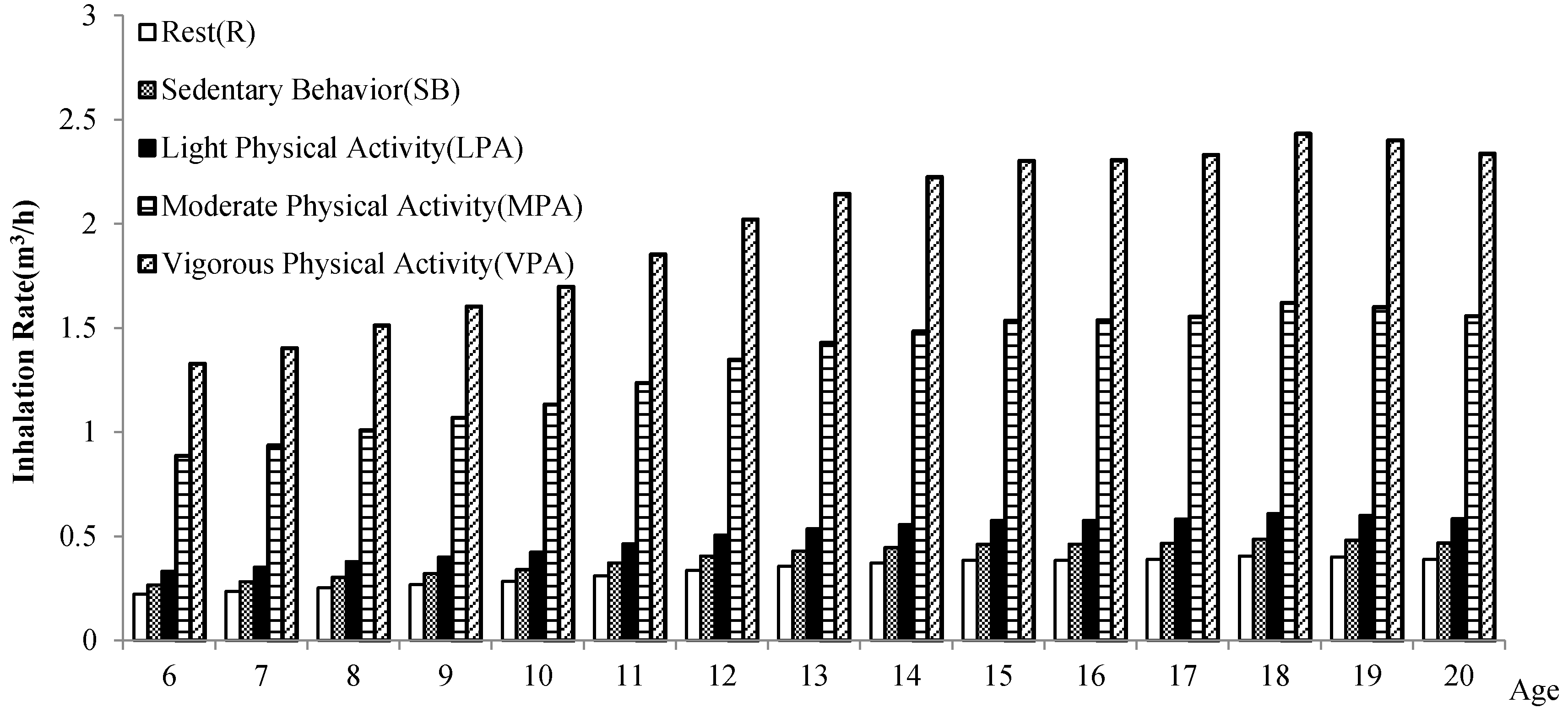
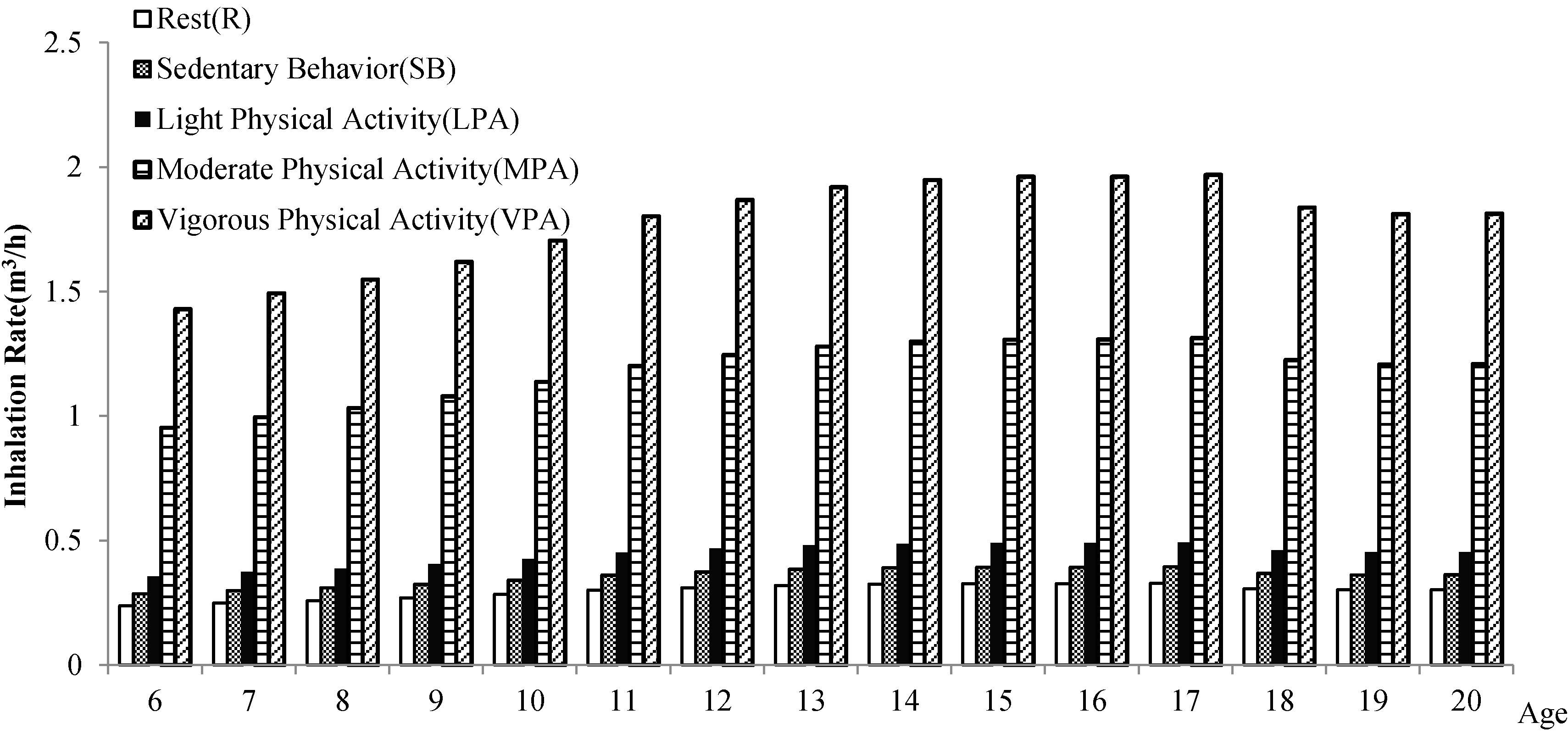
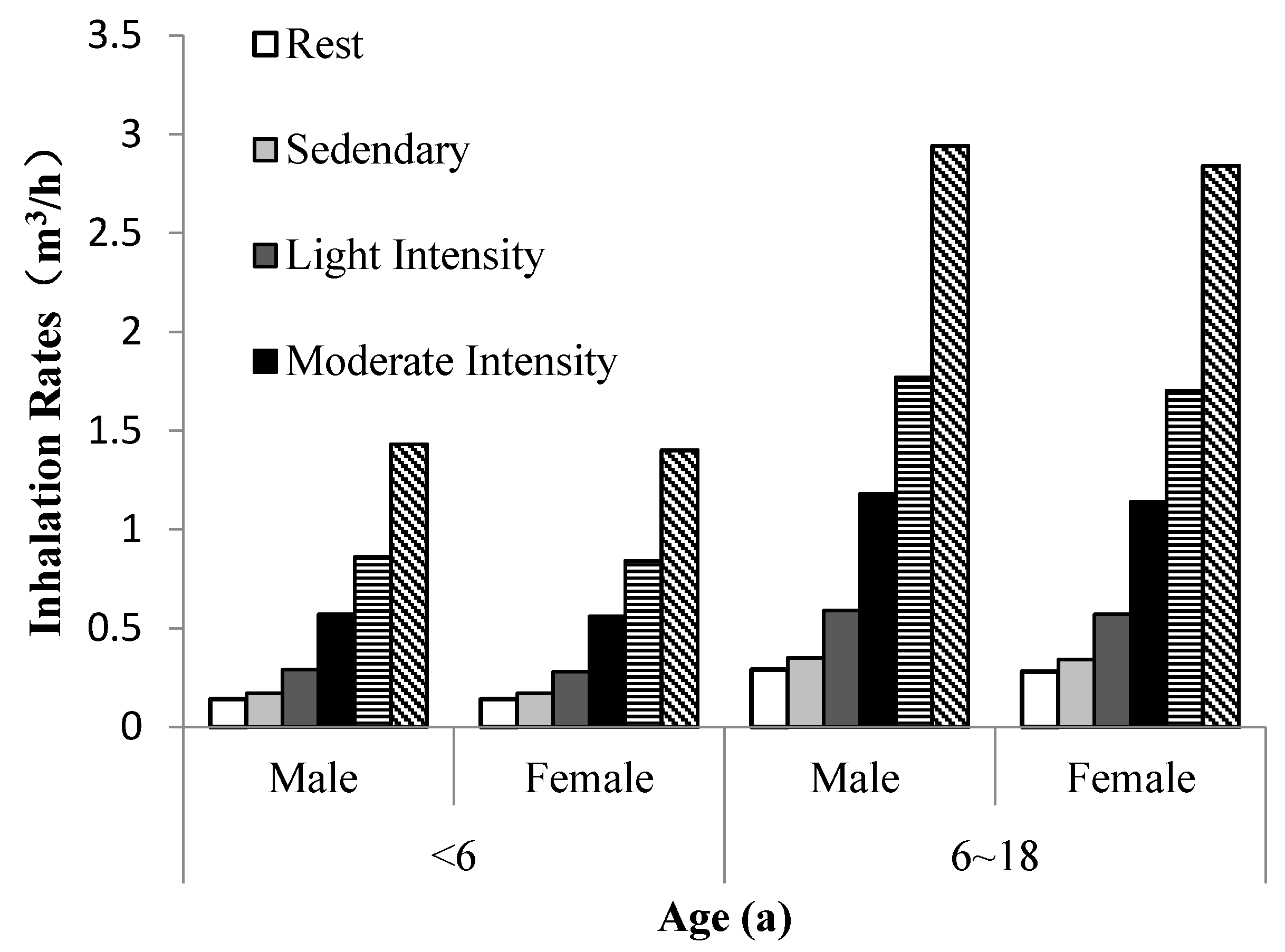
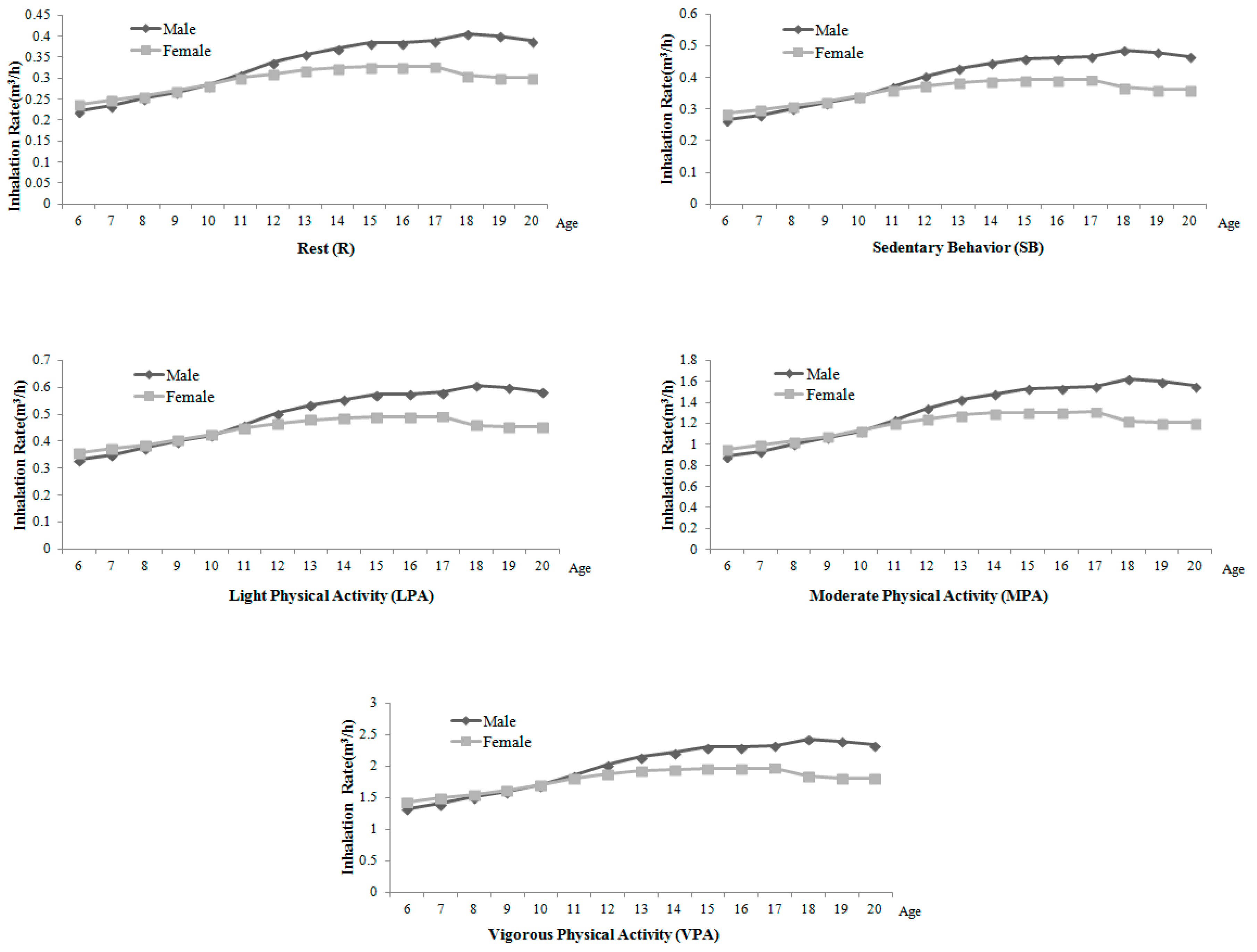
5.2. Research on Inhalation Rate in Different Physical Activities
6. Status of Children and Adolescents Respiratory Exposure Parameters in the World
6.1. Exposure Parameters in the World
6.2. Inhalation Exposure Factors of Chinese Children and Adolescents
6.3. Features of Inhalation Exposure Factors of Chinese Children and Adolescents
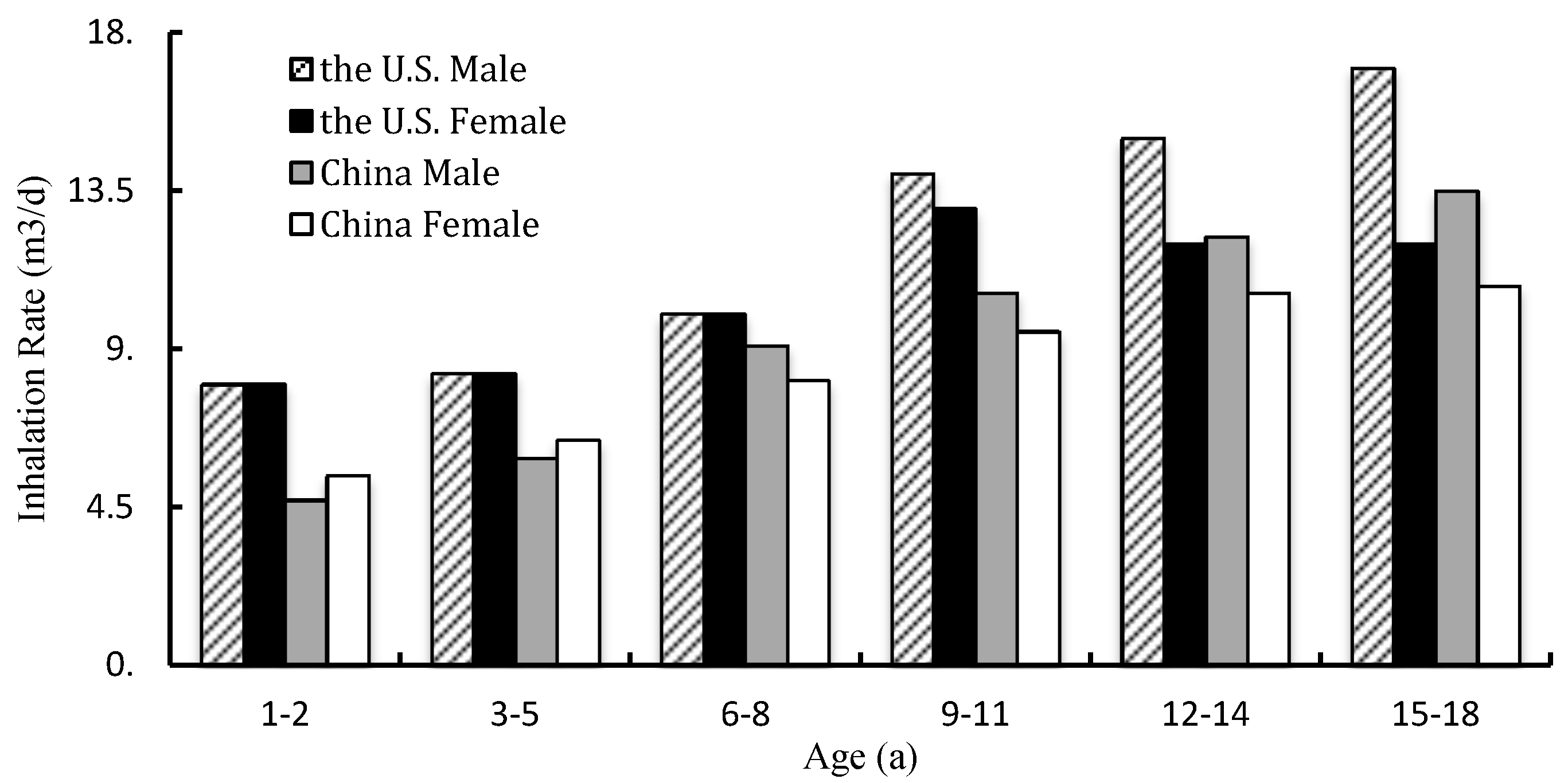
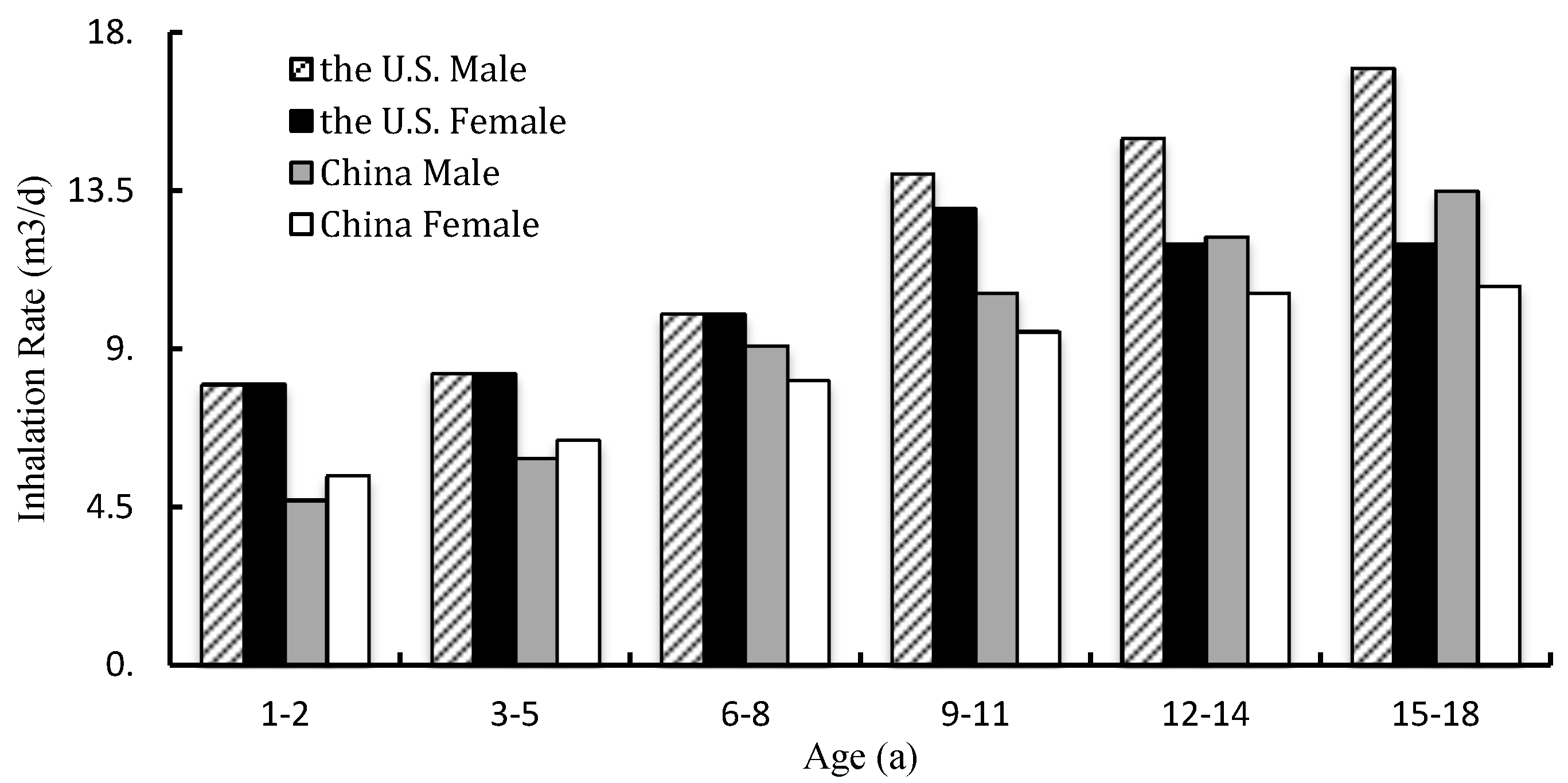
6.4. Comparison of Inhalation Exposure Factors of Children and Adolescents in the World
7. The Significance of Health Risk Assessment of Physical Activity in Polluted Environment
8. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lankhorst, K.; van der EndeKastelijn, K.; de Groot, J. Health in Adapted Youth Sports Study (HAYS): Health Effects of Sports Participation in Children and Adolescents with a Chronic Disease or Physical Disability. SpringerPlus 2015, 4, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Laye, M.J.; Lees, S.J.; Rector, R.S.; Thyfault, J.P. Reduced Physical Activity and Risk of Chronic Disease: The Biology behind the Consequences. Eur. J. Appl. Physiol. 2008, 102, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical Fitness in Childhood and Adolescence: A Powerful Marker of Health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive Validity of Health-Related Fitness in Youth: A Systematic Review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Finne, E.; Bucksch, J.; Lampert, T.; Kolip, P. Age, Puberty, Body Dissatisfaction, and Physical Activity Decline in Adolescents. Results of the German Health Interview and Examination Survey (KiGGS). Int. J. Behav. Nutr. Phys. Act. 2011, 27, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W. Physical Activity Change during Adolescence: A Systematic Review and a Pooled Analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, R.; Ceciliani, A.; Garulli, A.; Masotti, A.; Poletti, G.; Beltrami, P.; Leoni, E. Physical Fitness of Primary School Children in Relation to Overweight Prevalence and Physical Activity Habits. J. Sports Sci. 2012, 30, 633–664. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Chen, P.J.; Wu, Y.Q.; Shao, Z.Y.; Peng, N.N.; Zou, D.H. An Analysis of the Current Situation of Students’ Physical Quality in Shanghai and Its Influencing Factors. Chin. Sch. Health 2012, 33, 1007–1010. [Google Scholar]
- Ministry of Environmental Protection of the People’s Republic of China. China Environmental Status Bulletin (EB/OL). Available online: http://www.zhb.gov.cn/gkml/hbb/qt/201606/W020160602411685220884.pdf (accessed on 18 June 2016).
- Hankey, S.; Marshall, J.D.; Brauer, M. Health Impacts of the Built Environment: Within-Urban Variability in Physical Inactivity, Air Pollution, and Ischemic Heart Disease Mortality. Environ. Health Perspect. 2012, 120, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, A.; Sarmiento, O.L.; Duperly, J.; Wai, W.T.; Rojas, N.; Arango, C.M.; Maldonado, A.; Aristizabal, G.; Pérez, L.; Lobelo, F. Should They Play Outside? Cardiorespiratory Fitness and Air Pollution among Schoolchildren in Bogota. Rev. Salud Publica 2012, 14, 570–583. [Google Scholar] [PubMed]
- WHO. Health Statistics and Information Systems. A Response to the Need for Comprehensive, Consistent and Comparable Information on Health Risks at Global and Regional Level. Available online: http://www.who.int/healthinfo/global_burden_disease/global_health_risks/en/ (accessed on 5 January 2017).
- WHO. Global Health Observatory (GHO), Prevalence of Insufficient Physical Activity Data. Available online: http://www.who.int/gho/ncd/risk_factors/physical_activity_text/en/ (accessed on 10 January 2017).
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Lancet Physical Activity Series Working Group. Global Physical Activity Levels: Surveillance Progress, Pitfalls, and Prospects. Lancet 2012, 21, 247–257. [Google Scholar] [CrossRef]
- Wang, C. Recommendation of Physical Activity for Enhancing Health in Chinese Children and Adolescents; Shanghai University of Sport: Shanghai, China, 2013; pp. 65–72. [Google Scholar]
- WHO. Global School-Based Student Health Survey (2011). Available online: http://www.who.int/chp/gshs/en/ (accessed on 23 March 2017).
- WHO Europe. Inequalities in Young People’s Health: Health Behavior in School-Aged Children International Report from the 2005/2006 Survey; World Health Organization Europe: Copenhagen, Denmark, 2008; pp. 148–156.
- Thompson, A.M.; McHugh, T.L.; Blanchard, C.M.; Campagna, P.D.; Durant, M.A.; Rehman, L.A.; Murphy, R.J.; Wadsworth, L.A. Physical Activity of Children and Youth in Nova Scotia from 2001/02 and 2005/06. Prev. Med. 2009, 49, 407–409. [Google Scholar] [CrossRef] [PubMed]
- Melkevik, O.; Torsheim, T.; Iannotti, R.J.; Wold, B. Is Spending Time in Screen-Based Sedentary Behaviors Associated with Less Physical Activity: A Cross National Investigation. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigmundova, D. Secular Trends: A Ten-Year Comparison of the Amount and Type of Physical Activity and Inactivity of Random Samples of Adolescents in the Czech Republic. BMC Public Health 2011, 11, 731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raustorp, A.; Ludvigsson, J. Secular Trends of Pedometer-Determined Physical Activity in Swedish School Children. Acta Paediatr. 2007, 96, 1824–1828. [Google Scholar] [CrossRef] [PubMed]
- WHO. Ambient (Outdoor) Air Pollution in Cities Database 2014. Available online: http://www.who.int/phe/health_topics/outdoorair/databases/cities-2014/en/ (accessed on 20 March 2017).
- Mathew, J.; Goyal, R.; Taneja, K.K.; Arora, N. Air Pollution and Respiratory Health of School Children in Industrial, Commercial and Residential Areas of Delhi. Air Qual. Atmos. Health 2015, 8, 421–427. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid Health Transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- WHO. Quantification of the Disease Burden Attributable to Environmental Risk Factors (China Country Profile); World Health Organization: Geneva, Switzerland, 2009.
- Zhang, Q.F.; Robert, C. Toward an Environmentally Sustainable Future: Country Environmental Analysis of the People’s Republic of China; Asian Development Bank: Mandaluyong City, Philippines, 2012. [Google Scholar]
- Ashbolt, N.J.; Amézquit, A.; Backhaus, T.; Borriello, P.; Brandt, K.K.; Collignon, P.; Coors, A.; Finley, R.; Gaze, W.H.; Heberer, T.; et al. Human Health Risk Assessment (HHRA) for Environmental Development and Transfer of Antibiotic Resistance. Environ. Health Perspect. 2013, 121, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Luan, J.; Sherar, L.B.; Esliger, D.W.; Griew, P.; Cooper, A. International Children’s Accelerometry Database (ICAD) Collaborators. Moderate to Vigorous Physical Activity and Sedentary Time and Cardiometabolic Risk Factors in Children and Adolescents. JAMA 2012, 307, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Australian Department of Health. Environmental Health Risk Assessment—Guidelines for Assessing Human Health; Australian Department of Health: Canberra, Australia, 2012.
- Ege, M.J.; Mayer, M.; Normand, A.C.; Genuneit, J.; Cookson, W.O.; Braun-Fahrländer, C.; Heederik, D.; Piarroux, R.; von Mutius, E. GABRIELA Transregio 22 Study Group. Exposure to Environmental Microorganisms and Childhood Asthma. N. Engl. J. Med. 2011, 364, 701–709. [Google Scholar] [CrossRef] [PubMed]
- USEPA. Exposure Factors Handbook; EPA/600/R-090/05 2F; USEPA: Washington, DC, USA, 2011.
- USEPA. Exposure Factors Handbook; EPA/600/R-08/045F; USEPA: Washington, DC, USA, 2008.
- USEPA. Child-Specific Exposure Factors Handbook; EPA/600/R-06/096F; USEPA: Washington, DC, USA, 2010.
- Li, T.X.; Wang, Y.Q.; Duan, X.L.; Huang, N.; Wang, B.B.; Qian, Y. Exposure Factors of Activity Patterns in Environmental Health Risk Assessment. J. Environ. Health 2012, 29, 118–123. [Google Scholar]
- U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Available online: http://www.health.gov/paguidelines/guidelines/ (accessed on 12 October 2008).
- Duan, X.L. Research Methods of Exposure Factors and Its Application in Environmental Health Risk Assessment; Science Press: Beijing, China, 2012. [Google Scholar]
- Layton, D.W. Simulation of Average Energy Expenditures and Related Inhalation Rates for the U.S. Population. Air Qual. Atmos. Health 2013, 6, 527–539. [Google Scholar] [CrossRef]
- Yang, Y.; Yu, Y.J.; Li, D.L.; Yang, J.; Sun, H.W. Study of Residents’ Breath Exposure Parameter in Wenling Area. J. Environ. Health 2011, 28, 698–701. [Google Scholar]
- Arcus-Arth, A.; Blaisdell, R.J. Statistical Distributions of Daily Breathing Rates for Narrow Age Groups of Infants and Children. Risk Anal. 2007, 27, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Xia, L. Research on the Recommended Value of Outdoor Physical Activity Exposure Factor of Children and Adolescents in Polluted Air in Shanghai; Tongji University: Shanghai, China, 2017. [Google Scholar]
- Shanghai Bureau of Physical Education; Shanghai Education Commission; Shanghai Health and Family Planning Commission. Shanghai Citizen Fitness Monitoring Bulletin (EB). Available online: http://www.shsports.gov.cn/General/InfoPublicCatalogDetail/9993a348-ca89-4470-9ee0-95d3f18e109b (accessed on 29 December 2015).
- Maier, J.H.; Barry, R. Associations among Physical Activity, Diet, and Obesity Measures Change during Adolescence. J. Nutr. Metab. 2015, 2015, 805065. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.S.; Duan, X.L.; Liu, P.; Nie, J.; Huang, N.; Zhang, J.L. Human Exposure Factors of Chinese People in Environmental Health Risk Assessment. Res. Environ. Sci. 2009, 22, 1164–1170. [Google Scholar]
- Wang, Z.S.; Duan, X.L.; Liu, P. Discussion of Exposure Factor of Chinese Residents in Environment Health Risk Assessment. Environ. Health 2009, 22, 1164–1170. [Google Scholar]
- Snowden, J.M.; Mortimer, K.M.; Kang, D.M.; Tager, I.B. Population Intervention Models to Estimate Ambient NO2 Health Effects in Children with Asthma. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Averett, N. Exercising in Polluted Areas: Study Suggests Benefits Outweigh the Health Risks of NO2 Exposure. Environ. Health Perspect. 2015, 123, A158. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Z.J.; Nazelle, A.D.; Mendez, M.A.; Garcia-Aymerich, J.; Hertel, O.; Tjønneland, A.; Overvad, K.; Raaschou-Nielsen, O.; Nieuwenhuijsen, M.J. A Study of the Combined Effects of Physical Activity and Air Pollution on Mortality in Elderly Urban Residents: The Danish Diet, Cancer, and Health Cohort. Environ. Health Perspect. 2015, 123, 557–563. [Google Scholar] [CrossRef] [PubMed]
- USEPA. Risk Assessment Guidance for Superfund Volume I Human Health Evaluation Manual (Part A); EPA/540/1-89/002; USEPA: Washington, DC, USA, 1989.
- USEPA. Social Demographic Data Used for Identifying Potentially Highly Exposed Populations; EPA/600/R-99/060; USEPA: Washington, DC, USA, 1999.
- USEPA. Options for Development of Parametric Probability Distributions for Exposure Factors; EPA/600/R-00/058; USEPA: Washington, DC, USA, 2000.
- USEPA. Food Intake Distributions; EPA/600/R-03/0929; USEPA: Washington, DC, USA, 2003.
- National Institute of Advanced Industrial Science and Technology. Japanese Exposure Factors Handbook. Available online: http://unit.aist.go.jp/riss/crm/exposurefactors/english_summary.html (accessed on 24 April 2017).
- Kim, S.; Cheong, H.K.; Choi, K. Development of Korean Exposure Factors Handbook for Exposure Assessment. Epidemiology 2006, 17, 460–468. [Google Scholar] [CrossRef]
- Australian Department of Health. Australian Exposure Factor Guidance: Guidelines for Assessing Human Health Risks from Environmental Hazards; NO. D0702; Australian Department of Health: Canberra, Australia, 2012.
- Ministry of Environmental Protection of China. Exposure Factors Handbook of Chinese Population; China Environmental Science Press: Beijing, China, 2013. [Google Scholar]
- Ministry of Health of the Republic of China. 2012 China Health Statistics Yearbook; Peking Union Medical College Press: Beijing, China, 2012. [Google Scholar]
- Lu, C.; Stolk, R.P.; Sauer, P.J.J.; Sijtsma, A.; Wiersma, R.; Huang, G.; Corpeleijn, E. Factors of Physical Activity among Chinese Children and Adolescents: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education of the People’s Republic of China; General Administration of Sport of China; Ministry of Health of the Republic of China; State Ethnic Affairs Commission; Ministry of Science and Technology of the People’s Republic of China and Physical Fitness; Ministry of Finance of the Republic of China. Health Research of Chinese School Students; Higher Education Press: Beijing, China, 2013.
- CDC. National Center for Health Statistics, 2004. Available online: https://www.cdc.gov/nchs/surveys.htm (accessed on 6 November 2015).
- Ridley, K.; Ainsworth, B.E.; Olds, T.S. Development of a Compendium of Energy Expenditures for Youth. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tittlbach, S.A.; Sygusch, R.; Brehm, W.; Woll, A.; Lampert, T.; Abele, A.E.; Bos, K. Association between Physical Activity and Health in German Adolescents. Eur. J. Sport Sci. 2011, 11, 283–291. [Google Scholar] [CrossRef]
- Can, H.; Qian, Q.; Weng, T.; Yuan, C.; Sun, Y.; Wang, H.; Tao, F. Screen Time, Physical Activity and Mental Health among Urban Adolescents in China. Prev. Med. 2011, 53, 316–321. [Google Scholar]
- Ekenga, C.C.; Parks, C.G.; Sandler, D.P. A Prospective Study of Occupational Physical Activity and Breast Cancer Risk. Cancer Causes Control 2015, 26, 1779–1789. [Google Scholar] [CrossRef] [PubMed]
- Klausen, S.H.; Andersen, L.L.; Søndergaard, L.; Jakobsen, J.C.; Zoffmann, V.; Dideriksen, K.; Kruse, A.; Mikkelsen, U.R.; Wetterslev, J. Effects of Ehealth Physical Activity Encouragement in Adolescents with Complex Congenital Heart Disease: The PReVaiL Randomized Clinical Trial. Int. J. Cardiol. 2016, 221, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.K.; Sharma, V.K.; Arunachalam, V.; Balasubramanium, S.; Radhakrishnan, K. WHO Recommended Structured Physical Activity Intervention Improves Psychomotor Speed and Neuro-Cognitive Functions in Adolescent Students. Med. Sci. Sports Exerc. 2016, 48 (Suppl. 1), 916–917. [Google Scholar] [CrossRef]
- Roberts, J.D.; Voss, J.D.; Knight, B. The Association of Ambient Air Pollution and Physical Inactivity in the United States. PLoS ONE 2014, 9, e90143. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.J.; Balluz, L.S.; Shire, J.D.; Mokdad, A.H.; Kohl, H.W.I. Association of Self-Reported Leisure-Time Physical Inactivity with Particulate Matter 2.5 Air Pollution. J. Environ. Health 2009, 72, 40–44. [Google Scholar] [PubMed]
- Le Tertre, A.; Medina, S.; Samoli, E.; Forsberg, B.; Michelozzi, P.; Boumghar, A.; Vonk, J.M.; Bellini, A.; Atkinson, R.; Ayres, J.G.; et al. Short-Term Effects of Particulate Air Pollution on Cardiovascular Diseases in Eight European Cities. J. Epidemiol. Community Health 2002, 56, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.; Langrish, J.P.; Nair, H.; McAllister, D.A.; Hunter, A.L.; Donaldson, K.; Newby, D.E.; Mills, N.L. Global Association of Air Pollution and Heart Failure: A Systematic Review and Meta-Analysis. Lancet 2013, 382, 1039–1048. [Google Scholar] [CrossRef]
- Rd, P.C.; Ezzati, M.; Dockery, D.W. Fine-Particulate Air Pollution and Life Expectancy in the United States. N. Engl. J. Med. 2009, 360, 376–386. [Google Scholar]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung Cancer, Cardiopulmonary Mortality, and Long-Term Exposure to Fine Particulate Air Pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Liu, Y.; Lü, J.; Liang, L.; Harmer, P. Ambient Air Pollution in China Poses a Multifaceted Health Threat to Outdoor Physical Activity. J. Epidemiol. Community Health 2015, 69, 201–209. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Organizer | Date | Location | Sample | Age | Duration (Month) | Method |
|---|---|---|---|---|---|---|---|
| CAPS | CARB | 1987–1988 | California | 1762 | >12 | 12 | 24-h retrospective diaries |
| 1989–1990 | California | 1200 | <12 | 12 | 24-h retrospective diaries | ||
| NHAPS | EPA | 1992–1994 | 48 states of the U.S. | 9386 | The total population | 24 | 24-h retrospective diaries |
| EPA | 2004–2008 | 48 states of the U.S. | 23,028 | The total population | 24 | GPS | |
| EPRI | 1994–1995 | The U.S. | 1200 | The total population | 12 | 24-h retrospective diaries | |
| CHAPS | EPA | 1994–1995 | Canada | 2381 | Thetotal population | 9 | 24-h retrospective diaries |
| Age (Year) | Gender | Rest (R) X ± S | Sedentary Behavior (SB) X ± S | Light Physical Activity (LPA) X ± S | Moderate Physical Activity (MPA) X ± S | Vigorous Physical Activity (VPA) X ± S |
|---|---|---|---|---|---|---|
| 6 | Male | 0.22 ± 0.03 | 0.27 ± 0.01 | 0.33 ± 0.01 | 0.89 ± 0.05 | 1.33 ± 0.12 |
| Female | 0.24 ± 0.03 | 0.29 ± 0.03 | 0.36 ± 0.01 | 0.95 ± 0.08 | 1.43 ± 0.15 | |
| 7 | Male | 0.23 ± 0.04 | 0.28 ± 0.03 | 0.35 ± 0.05 | 0.94 ± 0.07 | 1.4 ± 0.13 |
| Female | 0.25 ± 0.02 | 0.30 ± 0.01 | 0.37 ± 0.03 | 1.00 ± 0.08 | 1.49 ± 0.17 | |
| 8 | Male | 0.25 ± 0.02 | 0.30 ± 0.03 | 0.38 ± 0.03 | 1.01 ± 0.05 | 1.51 ± 0.12 |
| Female | 0.26 ± 0.01 | 0.310 | 0.39 ± 0.01 | 1.03 ± 0.11 | 1.55 ± 0.17 | |
| 9 | Male | 0.267 ± 0.01 | 0.321 | 0.40 ± 0.04 | 1.07 ± 0.11 | 1.60 ± 0.12 |
| Female | 0.270 ± 0.05 | 0.324 | 0.41 ± 0.02 | 1.08 ± 0.12 | 1.62 ± 0.21 | |
| 10 | Male | 0.283 ± 0.03 | 0.340 | 0.42 ± 0.03 | 1.13 ± 0.07 | 1.70 ± 0.14 |
| Female | 0.284 ± 0.04 | 0.341 | 0.42 ± 0.03 | 1.14 ± 0.19 | 1.71 ± 0.16 | |
| 11 | Male | 0.31 ± 0.02 | 0.371 | 0.46 ± 0.04 | 1.24 ± 0.08 | 1.85 ± 0.13 |
| Female | 0.30 ± 0.03 | 0.361 | 0.45 ± 0.02 | 1.21 ± 0.12 | 1.80 ± 0.17 | |
| 12 | Male | 0.34 ± 0.05 | 0.404 | 0.51 ± 0.05 | 1.35 ± 0.15 | 2.02 ± 0.15 |
| Female | 0.31 ± 0.11 | 0.374 | 0.47 ± 0.02 | 1.25 ± 0.13 | 1.87 ± 0.18 | |
| 13 | Male | 0.36 ± 0.04 | 0.429 | 0.54 ± 0.03 | 1.43 ± 0.17 | 2.14 ± 0.20 |
| Female | 0.32 ± 0.02 | 0.384 | 0.48 ± 0.04 | 1.28 ± 0.16 | 1.92 ± 0.15 | |
| 14 | Male | 0.37 ± 0.05 | 0.445 | 0.57 ± 0.04 | 1.48 ± 0.17 | 2.22 ± 0.12 |
| Female | 0.31 ± 0.04 | 0.390 | 0.49 ± 0.07 | 1.30 ± 0.15 | 1.95 ± 0.19 | |
| 15 | Male | 0.38 ± 0.02 | 0.460 | 0.58 ± 0.05 | 1.54 ± 0.12 | 2.30 ± 0.16 |
| Female | 0.33 ± 0.05 | 0.392 | 0.49 ± 0.04 | 1.31 ± 0.15 | 1.96 ± 0.18 | |
| 16 | Male | 0.38 ± 0.07 | 0.461 | 0.58 ± 0.08 | 1.54 ± 0.19 | 2.31 ± 0.22 |
| Female | 0.33 ± 0.01 | 0.392 | 0.49 ± 0.06 | 1.31 ± 0.12 | 1.96 ± 0.20 | |
| 17 | Male | 0.39 ± 0.03 | 0.466 | 0.58 ± 0.05 | 1.55 ± 0.19 | 2.33 ± 0.18 |
| Female | 0.33 ± 0.08 | 0.394 | 0.49 ± 0.08 | 1.31 ± 0.14 | 1.97 ± 0.16 | |
| 18 | Male | 0.41 ± 0.02 | 0.486 | 0.61 ± 0.07 | 1.62 ± 0.18 | 2.43 ± 0.22 |
| Female | 0.31 ± 0.01 | 0.368 | 0.46 ± 0.05 | 1.23 ± 0.13 | 1.84 ± 0.14 | |
| 19 | Male | 0.40 ± 0.03 | 0.480 | 0.60 ± 0.07 | 1.60 ± 0.11 | 2.40 ± 0.25 |
| Female | 0.30 ± 0.06 | 0.362 | 0.45 ± 0.06 | 1.21 ± 0.12 | 1.81 ± 0.23 | |
| 20 | Male | 0.39 ± 0.05 | 0.467 | 0.58 ± 0.07 | 1.56 ± 0.17 | 2.34 ± 0.27 |
| Female | 0.30 ± 0.01 | 0.363 | 0.45 ± 0.05 | 1.21 ± 0.12 | 1.81 ± 0.16 |
| Age (Year) | Male | Female | ||
|---|---|---|---|---|
| Sample | Inhalation Rate (m3/d) | Sample | Inhalation Rate (m3/d) | |
| 1–2 | 35 | 4.7 ± 0.15 | 34 | 5.4 ± 0.16 |
| 3–5 | 168 | 5.9 ± 0.26 | 124 | 6.4 ± 0.42 |
| 6–8 | 161 | 9.1 ± 0.42 | 155 | 8.1 ± 0.67 |
| 9–11 | 193 | 10.6 ± 0.88 | 171 | 9.5 ± 0.91 |
| 12–14 | 206 | 12.2 ± 0.69 | 239 | 10.6 ± 1.02 |
| 15–18 | 239 | 13.5 ± 1.23 | 162 | 10.8 ± 0.88 |
| Age (Year) | Gender | Rest | Sedentary | Light Intensity | Moderate Intensity | High Intensity | Extremely High Intensity |
|---|---|---|---|---|---|---|---|
| <6 | Male | 0.14 ± 0.02 | 0.17 ± 0.04 | 0.29 ± 0.04 | 0.57 ± 0.03 | 0.86 ± 0.07 | 1.43 ± 0.1 |
| Female | 0.14 ± 0.05 | 0.17 ± 0.08 | 0.28 ± 0.05 | 0.56 ± 0.06 | 0.84 ± 0.05 | 1.40 ± 0.12 | |
| 6–18 | Male | 0.29 ± 0.05 | 0.35 ± 0.29 | 0.59 ± 0.07 | 1.18 ± 0.1 | 1.77 ± 0.13 | 2.94 ± 0.23 |
| Female | 0.28 ± 0.04 | 0.34 ± 0.04 | 0.57 ± 0.03 | 1.14 ± 0.09 | 1.70 ± 0.12 | 2.84 ± 0.36 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, J.; Zhang, S.; Xia, L.; Yu, Y.; Hu, S.; Sun, J.; Zhou, P.; Chen, P. Physical Activity, a Critical Exposure Factor of Environmental Pollution in Children and Adolescents Health Risk Assessment. Int. J. Environ. Res. Public Health 2018, 15, 176. https://doi.org/10.3390/ijerph15020176
Dong J, Zhang S, Xia L, Yu Y, Hu S, Sun J, Zhou P, Chen P. Physical Activity, a Critical Exposure Factor of Environmental Pollution in Children and Adolescents Health Risk Assessment. International Journal of Environmental Research and Public Health. 2018; 15(2):176. https://doi.org/10.3390/ijerph15020176
Chicago/Turabian StyleDong, Jingmei, Su Zhang, Li Xia, Yi Yu, Shuangshuang Hu, Jingyu Sun, Ping Zhou, and Peijie Chen. 2018. "Physical Activity, a Critical Exposure Factor of Environmental Pollution in Children and Adolescents Health Risk Assessment" International Journal of Environmental Research and Public Health 15, no. 2: 176. https://doi.org/10.3390/ijerph15020176
APA StyleDong, J., Zhang, S., Xia, L., Yu, Y., Hu, S., Sun, J., Zhou, P., & Chen, P. (2018). Physical Activity, a Critical Exposure Factor of Environmental Pollution in Children and Adolescents Health Risk Assessment. International Journal of Environmental Research and Public Health, 15(2), 176. https://doi.org/10.3390/ijerph15020176