An Assessment of Magnitudes and Patterns of Socioeconomic Inequalities across Various Health Problems: A Large National Cross-Sectional Survey in Korea

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Measures
2.2.1. Health Conditions and States
2.2.2. Socioeconomic Position Indicators
2.3. Statistical Analysis
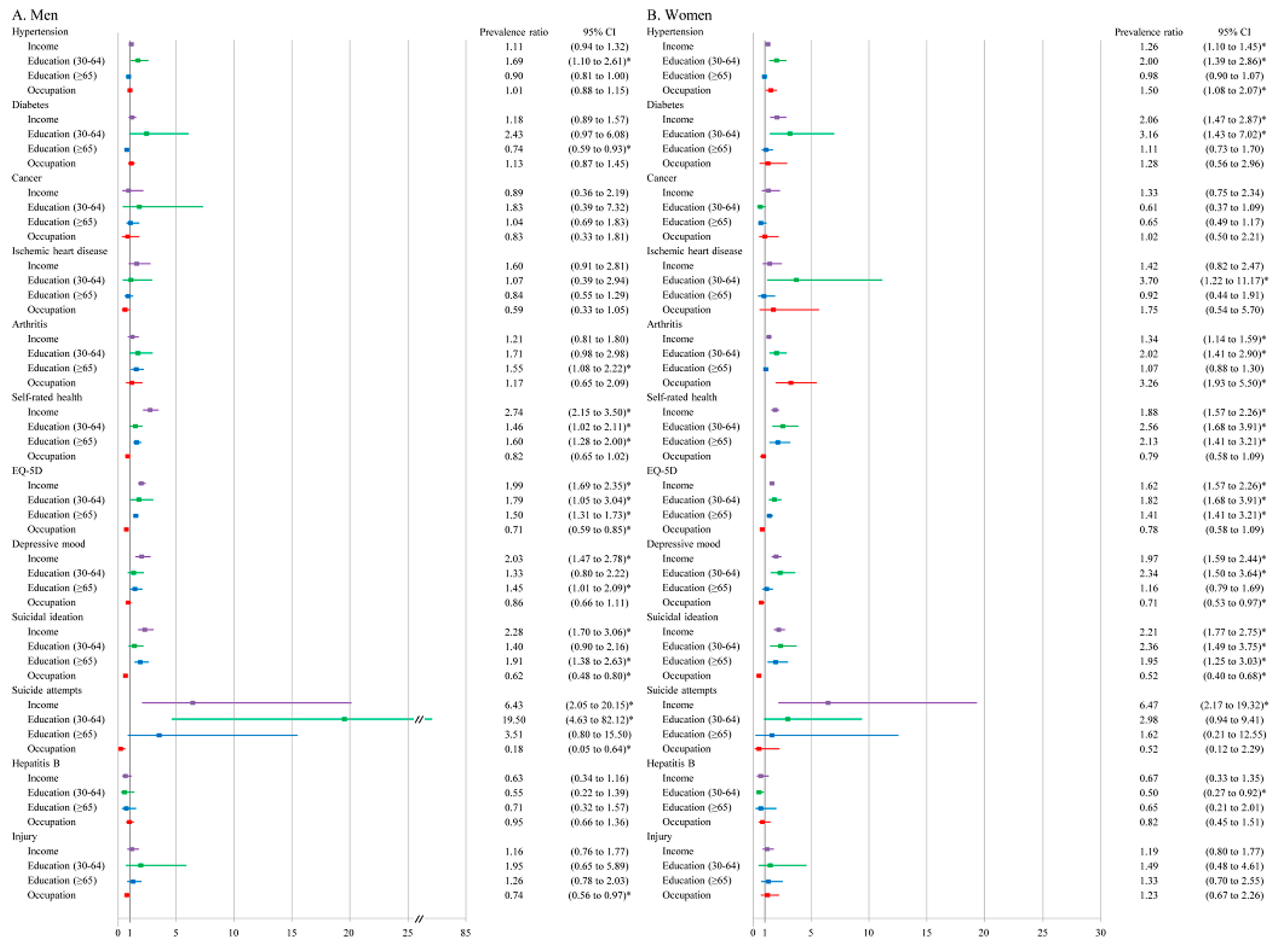
3. Results
4. Discussion
4.1. Comparison with Previous Studies
4.1.1. Socioeconomic Inequalities in NCDs and Mental Health and Gender Differences
4.1.2. Socioeconomic Inequalities in Cancer, Injuries, and Communicable Diseases
4.1.3. Socioeconomic Inequalities in Health States and Differences in Three SEP Measures
4.1.4. Implications of Similarities and Differences of Health Inequalities among 12 Health Conditions
4.2. Methodological Consideration
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bajekal, M.; Scholes, S.; Love, H.; Hawkins, N.; O’Flaherty, M.; Raine, R.; Capewell, S. Analysing recent socioeconomic trends in coronary heart disease mortality in England, 2000-2007: A population modelling study. PLoS Med. 2012, 9, e1001237. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Giesecke, J. Intervening to reduce inequalities in infections in Europe. Am. J. Public Health 2008, 98, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, M.; Khang, Y.H.; Asaria, P.; Blakely, T.; Cowan, M.J.; Farzadfar, F.; Guerrero, R.; Ikeda, N.; Kyobutungi, C.; Msyamboza, K.P.; et al. Inequalities in non-communicable diseases and effective responses. Lancet 2013, 381, 585–597. [Google Scholar] [CrossRef]
- Asada, Y.; Whipp, A.; Kindig, D.; Billard, B.; Rudolph, B. Inequalities in multiple health outcomes by education, sex, and race in 93 US counties: Why we should measure them all. Int. J. Equity Health 2014, 13, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalstra, J.A.; Kunst, A.E.; Borrell, C.; Breeze, E.; Cambois, E.; Costa, G.; Geurts, J.J.; Lahelma, E.; Van Oyen, H.; Rasmussen, N.K.; et al. Socioeconomic differences in the prevalence of common chronic diseases: An overview of eight European countries. Int. J. Epidemiol. 2005, 34, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Kunst, A.E.; Cavelaars, A.E.; Groenhof, F.; Geurts, J.J. Socioeconomic inequalities in morbidity and mortality in western Europe. The EU Working Group on Socioeconomic Inequalities in Health. Lancet 1997, 349, 1655–1659. [Google Scholar] [CrossRef]
- Sommer, I.; Griebler, U.; Mahlknecht, P.; Thaler, K.; Bouskill, K.; Gartlehner, G.; Mendis, S. Socioeconomic inequalities in non-communicable diseases and their risk factors: An overview of systematic reviews. BMC Public Health 2015, 15, 914. [Google Scholar] [CrossRef]
- Hughes, G.J.; Gorton, R. Inequalities in the incidence of infectious disease in the North East of England: A population-based study. Epidemiol. Infect. 2015, 143, 189–201. [Google Scholar] [CrossRef]
- Langford, A.; Johnson, B.; Al-Hamad, A. Social inequalities in female mortality by region and by selected causes of death, England and Wales, 2001–03. Health Stat. Q. 2009, 44, 7–26. [Google Scholar] [CrossRef]
- Avendano, M.; Kunst, A.E.; Huisman, M.; Lenthe, F.V.; Bopp, M.; Regidor, E.; Glickman, M.; Costa, G.; Spadea, T.; Deboosere, P.; et al. Socioeconomic status and ischaemic heart disease mortality in 10 western European populations during the 1990s. Heart 2006, 92, 461–467. [Google Scholar] [CrossRef]
- Manrique-Garcia, E.; Sidorchuk, A.; Hallqvist, J.; Moradi, T. Socioeconomic position and incidence of acute myocardial infarction: A meta-analysis. J. Epidemiol. Community Health 2011, 65, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.L.; Marmot, M.G.; Farley, T.M.; Poulter, N.R. The influence of economic development on the association between education and the risk of acute myocardial infarction and stroke. J. Clin. Epidemiol. 2002, 55, 741–747. [Google Scholar] [CrossRef]
- Khang, Y.H.; Lynch, J.W.; Kaplan, G.A. Health inequalities in Korea: Age- and sex-specific educational differences in the 10 leading causes of death. Int. J. Epidemiol. 2004, 33, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Kagamimori, S.; Gaina, A.; Nasermoaddeli, A. Socioeconomic status and health in the Japanese population. Soc. Sci. Med. 2009, 68, 2152–2160. [Google Scholar] [CrossRef] [PubMed]
- Gopfert, A.; Sethi, D.; Rakovac, I.; Mitis, F. Growing inequalities in child injury deaths in Europe. Eur. J. Public Health 2015, 25, 660–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mari-Dell’Olmo, M.; Gotsens, M.; Palencia, L.; Burstrom, B.; Corman, D.; Costa, G.; Deboosere, P.; Diez, E.; Dominguez-Berjon, F.; Dzurova, D.; et al. Socioeconomic inequalities in cause-specific mortality in 15 European cities. J. Epidemiol. Community Health 2015, 69, 432–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huisman, M.; Kunst, A.E.; Bopp, M.; Borgan, J.K.; Borrell, C.; Costa, G.; Deboosere, P.; Gadeyne, S.; Glickman, M.; Marinacci, C.; et al. Educational inequalities in cause-specific mortality in middle-aged and older men and women in eight western European populations. Lancet 2005, 365, 493–500. [Google Scholar] [CrossRef]
- Vellakkal, S.; Subramanian, S.V.; Millett, C.; Basu, S.; Stuckler, D.; Ebrahim, S. Socioeconomic inequalities in non-communicable diseases prevalence in India: Disparities between self-reported diagnoses and standardized measures. PLoS ONE 2013, 8, e68219. [Google Scholar] [CrossRef]
- Matthews, S.; Manor, O.; Power, C. Social inequalities in health: Are there gender differences? Soc. Sci. Med. 1999, 48, 49–60. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Lee, Y.K.; Nam, H.S.; Chuang, L.H.; Kim, K.Y.; Yang, H.K.; Kwon, I.S.; Kind, P.; Kweon, S.S.; Kim, Y.T. South Korean time trade-off values for EQ-5D health states: Modeling with observed values for 101 health states. Value Health 2009, 12, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Deaton, A.; Lubotsky, D. Mortality, inequality and race in American cities and states. Soc. Sci. Med. 2003, 56, 1139–1153. [Google Scholar] [CrossRef]
- KNSO. Korea Standard Classification of Occupations; Korea National Statistical Office: Seoul, Korea, 2007.
- Gart, J.J.; Nam, J.-M. Approximate interval estimation of the ratio of binomial parameters: A review and corrections for skewness. Biometrics 1988, 44, 323–338. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.M.; Ferrer, R.L.; Cho, S.I.; Sung, J.; Ebrahim, S.; Davey Smith, G. Socioeconomic status and cardiovascular disease among men: The Korean national health service prospective cohort study. Am. J. Public Health 2006, 96, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Devaux, M.; Sassi, F. Social inequalities in obesity and overweight in 11 OECD countries. Eur. J. Public Health 2013, 23, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.S.; Ki, M.; Kim, K.H.; Ju, Y.S.; Paek, D.; Lee, W. Working hours and self-rated health over 7 years: Gender differences in a Korean longitudinal study. BMC Public Health 2015, 15, 1287. [Google Scholar] [CrossRef]
- Lee, H.; Cho, J.; Shin, D.W.; Lee, S.P.; Hwang, S.S.; Oh, J.; Yang, H.K.; Hwang, S.H.; Son, K.Y.; Chun, S.H.; et al. Association of cardiovascular health screening with mortality, clinical outcomes, and health care cost: A nationwide cohort study. Prev. Med. 2015, 70, 19–25. [Google Scholar] [CrossRef]
- Seon, J.J.; Lim, Y.J.; Lee, H.W.; Yoon, J.M.; Kim, S.J.; Choi, S.; Kawachi, I.; Park, S.M. Cardiovascular health status between standard and nonstandard workers in Korea. PLoS ONE 2017, 12, e0178395. [Google Scholar] [CrossRef]
- McMunn, A.; Nazroo, J.; Breeze, E. Inequalities in health at older ages: A longitudinal investigation of the onset of illness and survival effects in England. Age Ageing 2009, 38, 181–187. [Google Scholar] [CrossRef]
- Huisman, M.; Read, S.; Towriss, C.A.; Deeg, D.J.; Grundy, E. Socioeconomic Inequalities in Mortality Rates in Old Age in the World Health Organization Europe Region. Epidemiol. Rev. 2013, 35, 84–97. [Google Scholar] [CrossRef] [Green Version]
- Lorant, V.; Croux, C.; Weich, S.; Deliege, D.; Mackenbach, J.; Ansseau, M. Depression and socio-economic risk factors: 7-year longitudinal population study. Br. J. Psychiatry 2007, 190, 293–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorant, V.; Kunst, A.E.; Huisman, M.; Costa, G.; Mackenbach, J.; EU Working Group on Socio-Economic Inequalities in Health. Socio-economic inequalities in suicide: A European comparative study. Br. J. Psychiatry 2005, 187, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD. Health at a Glance 2015: OECD Indicators; Organization for Economic Co-operation and Development: Paris, France, 2015. [Google Scholar]
- Lundqvist, A.; Andersson, E.; Ahlberg, I.; Nilbert, M.; Gerdtham, U. Socioeconomic inequalities in breast cancer incidence and mortality in Europe-a systematic review and meta-analysis. Eur. J. Public Health 2016, 26, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Orton, E.; Kendrick, D.; West, J.; Tata, L.J. Persistence of health inequalities in childhood injury in the UK: A population-based cohort study of children under 5. PLoS ONE 2014, 9, e111631. [Google Scholar] [CrossRef] [PubMed]
- CDC. Health Disparities and Inequalities Report—United States; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013.
- Park, B.; Choi, K.S.; Lee, H.Y.; Jun, J.K.; Park, E.C. Socioeconomic inequalities in completion of hepatitis B vaccine series among Korean women: Results from a nationwide interview survey. Vaccine 2012, 30, 5844–5848. [Google Scholar] [CrossRef] [PubMed]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Davey Smith, G. Indicators of socioeconomic position (part 2). J. Epidemiol. Community Health 2006, 60, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahelma, E.; Martikainen, P.; Rahkonen, O.; Roos, E.; Saastamoinen, P. Occupational class inequalities across key domains of health: Results from the Helsinki Health Study. Eur. J. Public Health 2005, 15, 504–510. [Google Scholar] [CrossRef] [Green Version]
- Lorenc, T.; Petticrew, M.; Welch, V.; Tugwell, P. What types of interventions generate inequalities? Evidence from systematic reviews. J. Epidemiol. Community Health 2013, 67, 190–193. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Bakker, M.J.; European Network on Interventions and Policies to Reduce Inequalities in Health. Tackling socioeconomic inequalities in health: Analysis of European experiences. Lancet 2003, 362, 1409–1414. [Google Scholar] [CrossRef]
- Harper, S.; Strumpf, E.C.; Burris, S.; Smith, G.D.; Lynch, J. The Effect of Mandatory Seat Belt Laws on Seat Belt Use by Socioeconomic Position. J. Policy Anal. Manag. 2014, 33, 141–161. [Google Scholar] [CrossRef]
- Baicker, K.; Taubman, S.L.; Allen, H.L.; Bernstein, M.; Gruber, J.H.; Newhouse, J.P.; Schneider, E.C.; Wright, B.J.; Zaslavsky, A.M.; Finkelstein, A.N.; et al. The Oregon experiment—Effects of Medicaid on clinical outcomes. N. Engl. J. Med. 2013, 368, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- McLaren, L.; McIntyre, L.; Kirkpatrick, S. Rose’s population strategy of prevention need not increase social inequalities in health. Int. J. Epidemiol. 2010, 39, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Franks, P.; Fiscella, K. Reducing disparities downstream: Prospects and challenges. J. Gen. Intern. Med. 2008, 23, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Harper, H.; Lynch, J. Measuring health inequalities. In Methods in Social Epidemiology; Oakes, M.J., Kaufman, J.S., Eds.; Jossey-Bass: San Francisco, CA, USA, 2006. [Google Scholar]
- Erreygers, G.; Kessels, R. Socioeconomic Status and Health: A New Approach to the Measurement of Bivariate Inequality. Int. J. Environ. Res. Public Health 2017, 14, 673. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men | Women | Total | ||
|---|---|---|---|---|
| N (%) | N (%) | p-Value † | N (%) | |
| Number of individuals | 7515 (43.5) | 9777 (56.5) | 17,292 (100) | |
| Age | ||||
| 30–64 | 5484 (73.0) | 7066 (72.3) | 12,550 (72.6) | |
| ≥65 | 2031 (27.0) | 2711 (27.7) | 0.3048 | 4742 (27.4) |
| Income | ||||
| Low | 1416 (19.1) | 2221 (23.1) | 3637 (21.4) | |
| Mid-low | 1934 (26.1) | 2504 (26.0) | 4438 (26.1) | |
| Mid-high | 2013 (27.2) | 2460 (25.6) | 4473 (26.3) | |
| High | 2041 (27.6) | 2435 (25.3) | <0.001 | 4476 (26.3) |
| Education | ||||
| Age (30–64) | ||||
| Low | 500 (10.3) | 1269 (19.2) | 1769 (15.4) | |
| Middle | 2281 (46.8) | 3296 (49.7) | 5577 (48.5) | |
| High | 2095 (43.0) | 2062 (31.1) | <0.001 | 4157 (36.1) |
| Age (≥65) | ||||
| Low | 837 (45.5) | 1996 (81.9) | 2833 (66.2) | |
| Middle | 316 (17.2) | 206 (8.5) | 522 (12.2) | |
| High | 688 (37.4) | 234 (9.6) | <0.001 | 922 (21.6) |
| Occupation | ||||
| Manager or office job | 1827 (35.6) | 1162 (28.0) | 2989 (32.2) | |
| Service or sales | 687 (13.4) | 1183 (28.5) | 1870 (20.2) | |
| Manual work | 2618 (51.0) | 1801 (43.4) | <0.001 | 4419 (47.6) |
| Diabetes | ||||
| Yes | 878 (14.0) | 822 (9.8) | 1700 (11.6) | |
| No | 5394 (86.0) | 7561 (90.2) | <0.001 | 12,955 (88.4) |
| Hypertension | ||||
| Yes | 2493 (37.3) | 2956 (32.7) | 5449 (34.6) | |
| No | 4192 (62.7) | 6097 (67.4) | <0.001 | 10,289 (65.4) |
| Cancer | ||||
| Yes | 74 (1.1) | 157 (1.7) | 231 (1.5) | |
| No | 6648 (98.9) | 8926 (98.3) | <0.001 | 15,574 (98.5) |
| Ischemic heart disease | ||||
| Yes | 251 (3.7) | 252 (2.8) | 503 (3.2) | |
| No | 6472 (96.3) | 8834 (97.2) | 0.3501 | 15,306 (96.8) |
| Arthritis | ||||
| Yes | 361 (9.1) | 1813 (33.9) | 2714 (23.3) | |
| No | 3629 (91.0) | 3528 (66.1) | <0.001 | 7157 (76.7) |
| Self-rated health status | ||||
| Good | 5595 (83.2) | 6951 (76.5) | 12,546 (79.3) | |
| Poor | 1129 (16.8) | 2137 (23.5) | <0.001 | 3266 (20.7) |
| EQ-5D | ||||
| Below median | 2613 (34.8) | 4497 (46.0) | 7110 (41.1) | |
| Above median | 4902 (65.2) | 5280 (54.0) | <0.001 | 10,182 (58.9) |
| Depressive mood | ||||
| Yes | 627 (9.3) | 1517 (16.7) | 2144 (13.6) | |
| No | 6098 (90.7) | 7543 (83.3) | <0.001 | 13,641 (86.4) |
| Suicide ideation | ||||
| Yes | 711 (10.6) | 1612 (17.8) | 2323 (14.7) | |
| No | 6017 (89.4) | 7447 (82.2) | <0.001 | 13,460 (85.3) |
| Suicide attempts | ||||
| Yes | 51 (0.8) | 65 (0.7) | 116 (0.7) | |
| No | 6673 (99.2) | 8991 (99.3) | 0.7671 | 15,664 (99.3) |
| Hepatitis B | ||||
| Yes | 287 (4.3) | 303 (3.5) | 590 (3.8) | |
| No | 6379 (95.7) | 8436 (96.5) | 0.0072 | 14,815 (96.2) |
| Injury experience | ||||
| Yes | 468 (7.0) | 601 (6.6) | 1069 (6.8) | |
| No | 6250 (93.0) | 8472 (93.4) | 0.3970 | 14,722 (93.2) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, J.-Y.; Lim, J.; Ki, M.; Song, Y.-J.; Chun, H.; Kim, D. An Assessment of Magnitudes and Patterns of Socioeconomic Inequalities across Various Health Problems: A Large National Cross-Sectional Survey in Korea. Int. J. Environ. Res. Public Health 2018, 15, 2868. https://doi.org/10.3390/ijerph15122868
Shin J-Y, Lim J, Ki M, Song Y-J, Chun H, Kim D. An Assessment of Magnitudes and Patterns of Socioeconomic Inequalities across Various Health Problems: A Large National Cross-Sectional Survey in Korea. International Journal of Environmental Research and Public Health. 2018; 15(12):2868. https://doi.org/10.3390/ijerph15122868
Chicago/Turabian StyleShin, Ji-Yeon, Jiseun Lim, Myung Ki, Yeong-Jun Song, Heeran Chun, and Dongjin Kim. 2018. "An Assessment of Magnitudes and Patterns of Socioeconomic Inequalities across Various Health Problems: A Large National Cross-Sectional Survey in Korea" International Journal of Environmental Research and Public Health 15, no. 12: 2868. https://doi.org/10.3390/ijerph15122868