Estimation of Neonatal Intestinal Perforation Associated with Necrotizing Enterocolitis by Machine Learning Reveals New Key Factors

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approvals
2.2. Dataset
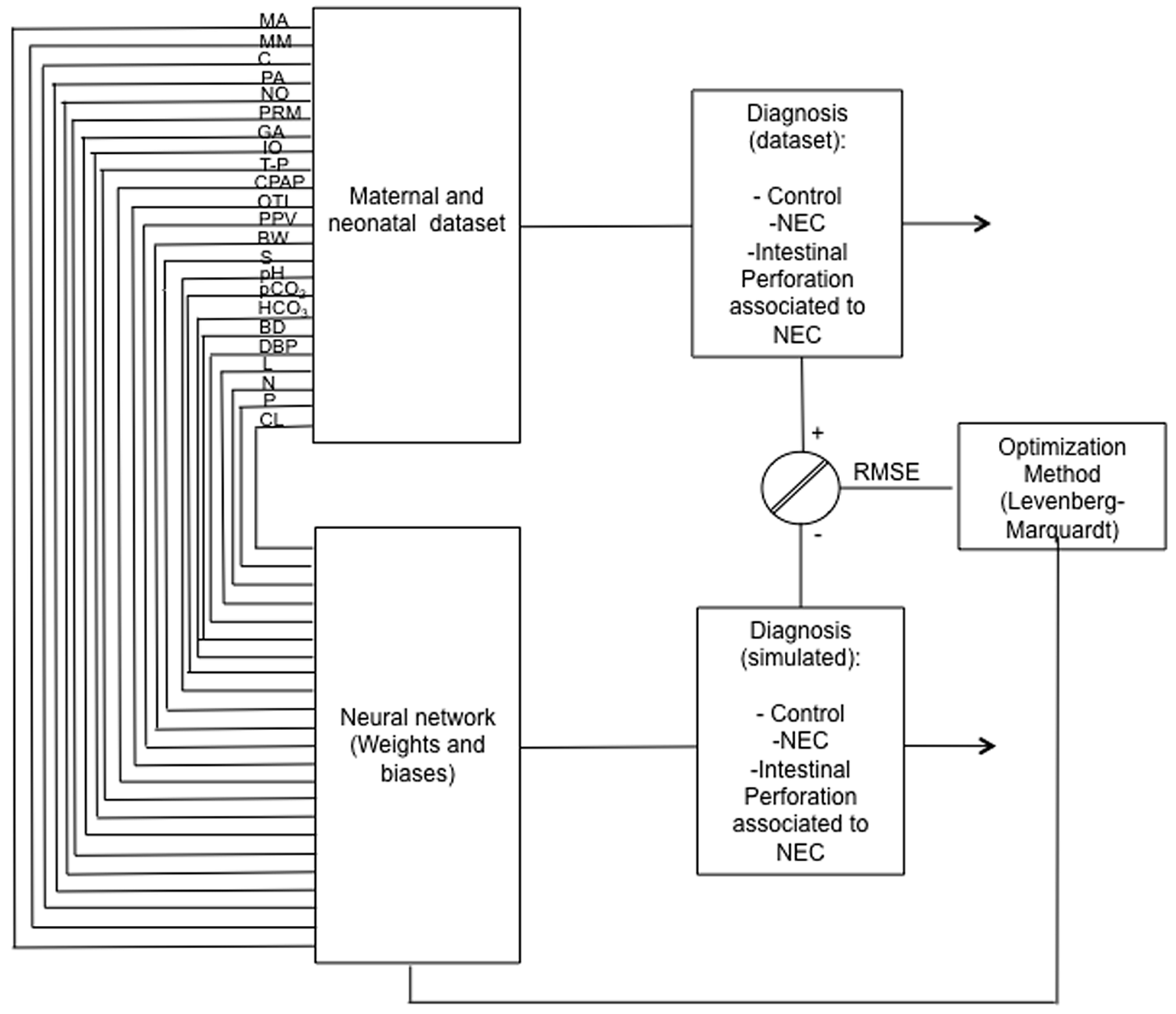
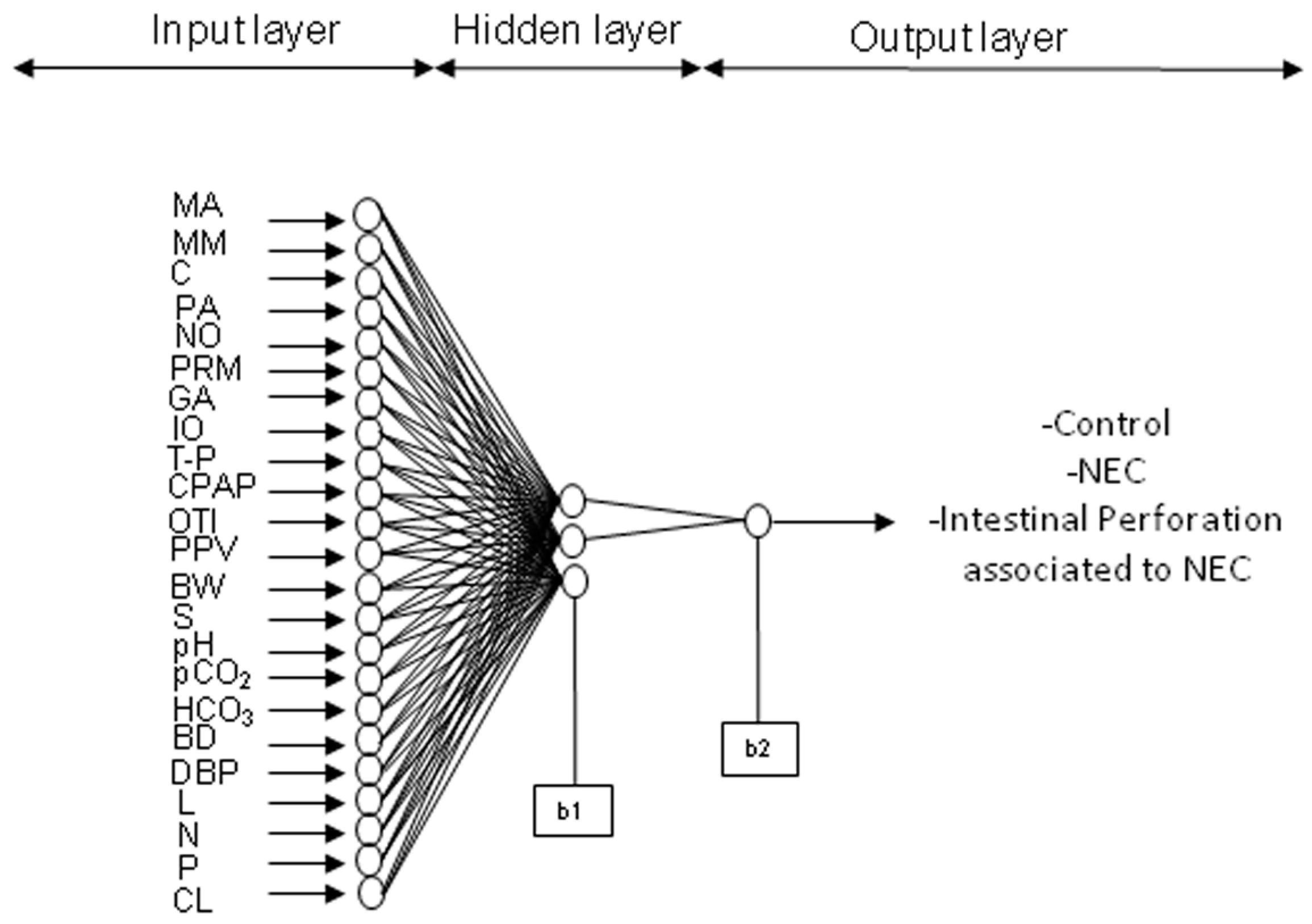
2.3. ANN (Learning, Testing, and Validation)
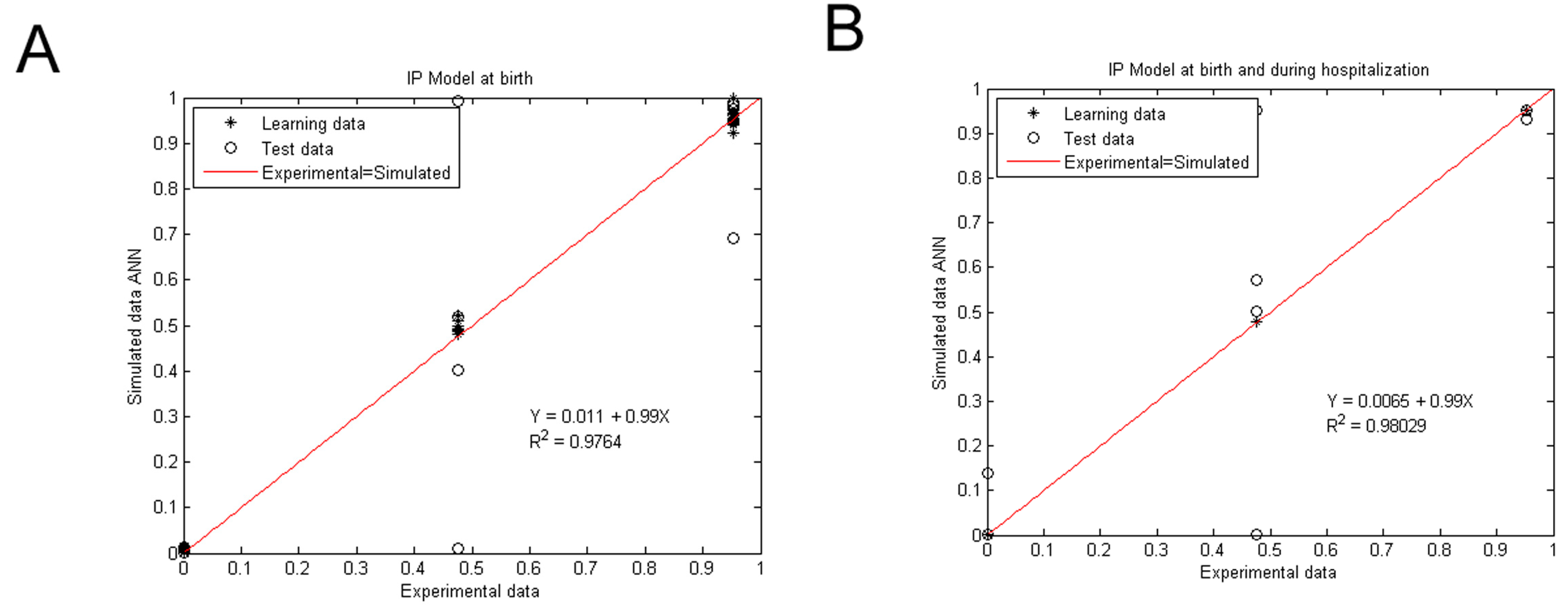
2.3.1. IP ANN Model at Birth
2.3.2. IP ANN Model at Birth and during Hospitalization
2.3.3. Statistical Test for ANN Model Validation
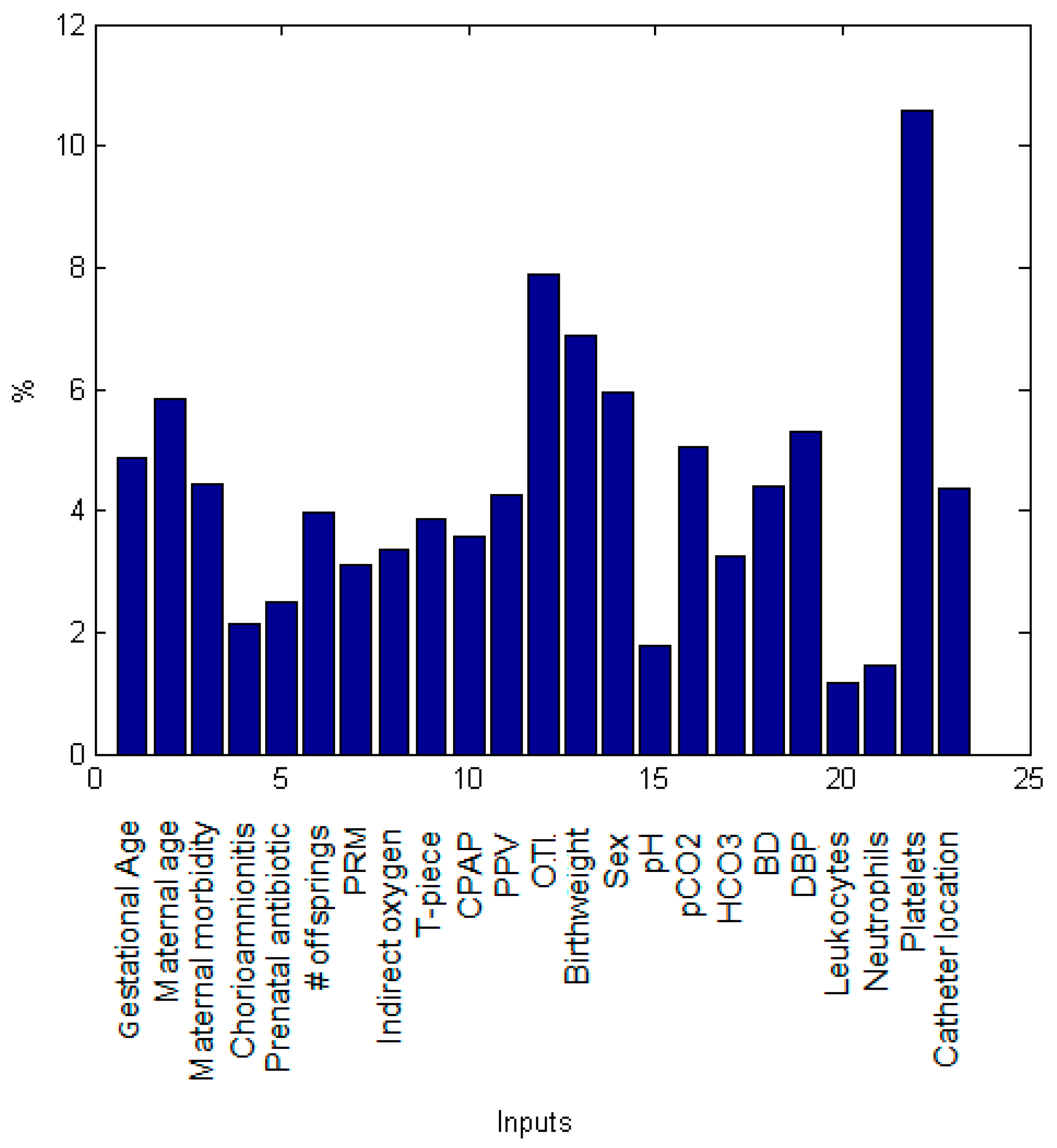
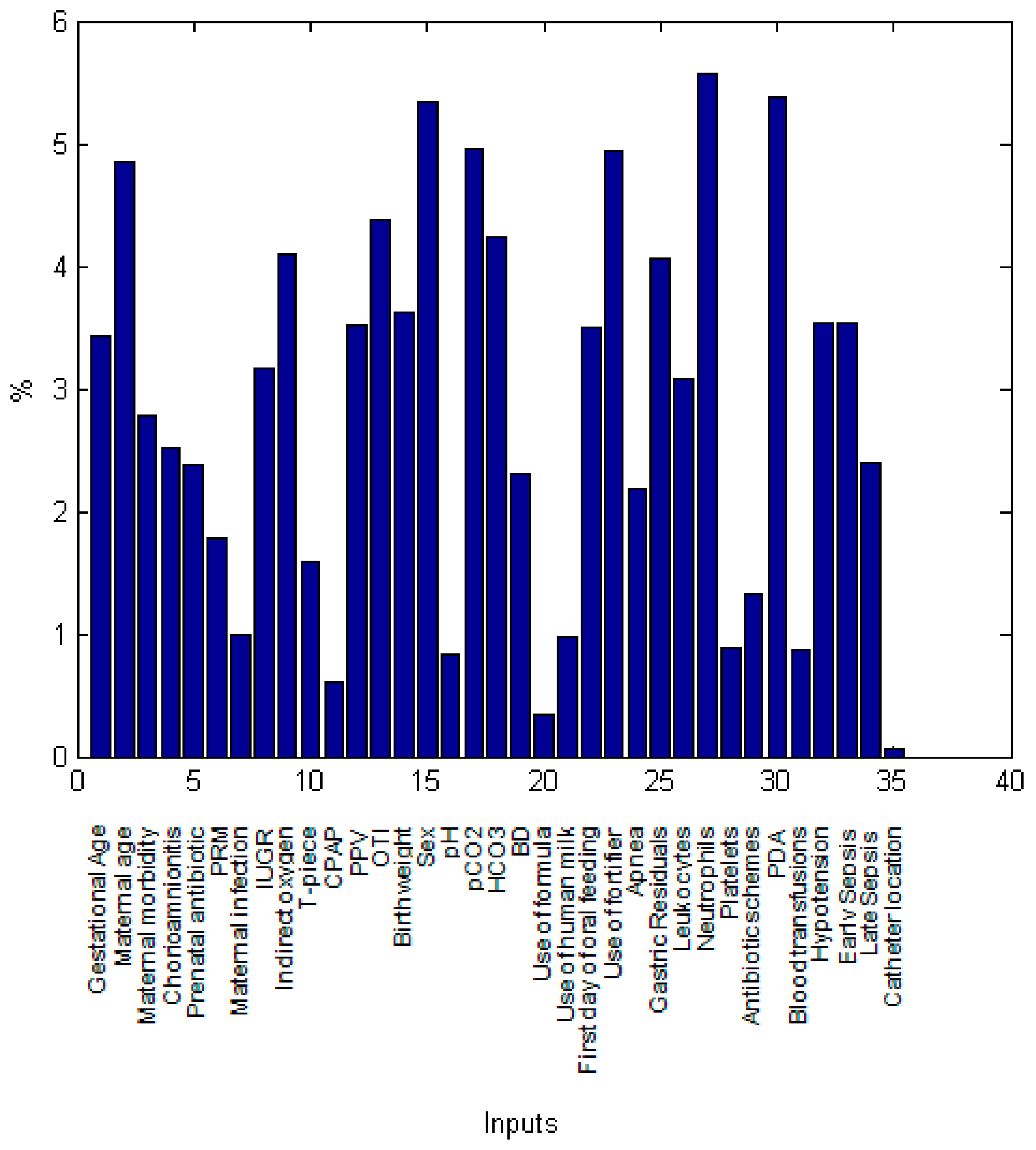
2.4. Sensitivity Analysis
3. Results
4. Discussion
4.1. Maternal Burden
4.2. First Day of Life
4.3. During Hospitalization
4.4. Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- 1:
- Preeclampsia
- 2:
- Hypertension
- 3:
- Gestational Diabetes Mellitus
- 4:
- Overweight
- 5:
- Adolescence
- 6:
- Hypothyroidism
- 7:
- Gestational Diabetes Mellitus and Hypothyroidism
- 8:
- Type II Diabetes and preeclampsia and overweight and hypertension
- 9:
- Polycystic ovary
- 10:
- Cervicovaginitis
- 11:
- Gestational Diabetes Mellitus and Preeclampsia
- 12:
- Preeclampsia and overweight
- 13:
- Hypothyroidism and overweight
- 14:
- Diabetes and candidiasis
- 15:
- Preeclampsia and carbohydrate intolerance
Appendix B
- J is the Jacobian matrix (first derivative)
- e is a vector of network errors
- μ is the combination coefficient with a value of 0.001
- I is the identity matrix.
- Q is the number of data points (n = 76),
- is the experimental data,
- is the network prediction.
- is the relative importance of the input variable on the output variable,
- is the number of input neurons,
- is the number of hidden neurons,
- is the connection weight,
- And the superscripts , and refer to input, hidden and output layer.
Appendix C

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wi{s,k} | |||
|---|---|---|---|
| Wi{s,1} | 1.3267125 | 3.1584473 | −1.0502622 |
| Wi{s,2} | −1.7146594 | −1.8984633 | 2.2922617 |
| Wi{s,3} | 4.8419826 | 0.346469 | 0.172989 |
| Wi{s,4} | 0.7706828 | −1.8081623 | −0.1177451 |
| Wi{s,5} | −0.6644504 | −1.4773511 | 0.641453 |
| Wi{s,6} | 1.7169406 | 1.6965454 | −0.980111 |
| Wi{s,7} | 1.4663105 | 0.5359049 | 1.1481214 |
| Wi{s,8} | 0.5342111 | 3.4738356 | 0.2333177 |
| Wi{s,9} | 2.5968973 | 1.9983119 | −0.1671108 |
| Wi{s,10} | 0.0638118 | 0.9084672 | −2.1722897 |
| Wi{s,11} | −0.4195773 | 2.0502619 | −1.7919031 |
| Wi{s,12} | 1.5347326 | −1.6982282 | 4.0750083 |
| Wi{s,13} | 3.4133979 | −3.0526489 | −1.3469327 |
| Wi{s,14} | 1.7925231 | 1.4563156 | −2.5644274 |
| Wi{s,15} | 0.5678812 | −0.7150829 | −0.5980426 |
| Wi{s,16} | 2.661324 | 2.4458136 | −0.7857453 |
| Wi{s,17} | 0.0671341 | 0.8060811 | −1.9744531 |
| Wi{s,18} | −3.7567751 | 0.823349 | −0.531168 |
| Wi{s,19} | −4.0508192 | 1.2459655 | −0.7937825 |
| Wi{s,20} | −0.8384736 | 0.3953479 | 0.1355509 |
| Wi{s,21} | −1.5220229 | 0.0202477 | −0.1580771 |
| Wi{s,22} | −4.7012854 | −5.0669983 | −2.2215755 |
| Wi{s,23} | −2.8142496 | −0.4138948 | 1.3408794 |
| Wo{1,1} | Wo{1,2} | Wo{1,3} | |
| Wo{l,s} | −5.5289631 | 4.3969459 | 5.5399183 |
| b1{23,1} | b1{s,1} | ||
| 1.6391183 | |||
| −2.673269 | |||
| 5.3597672 | |||
| b2{l,s} | |||
| b2{1,1} | −0.2889819 |
| Wi{s,k} | ||
|---|---|---|
| Wi{s,1} | −0.3751959 | −7.3554209 |
| Wi{s,2} | 8.7757177 | 0.8013817 |
| Wi{s,3} | 3.8650996 | 1.8292029 |
| Wi{s,4} | −3.5645456 | −1.5785954 |
| Wi{s,5} | 1.6843183 | 3.4310907 |
| Wi{s,6} | −1.0314863 | −2.8521103 |
| Wi{s,7} | 1.7744987 | −0.1751799 |
| Wi{s,8} | −6.0887131 | −0.1231969 |
| Wi{s,9} | 2.9294796 | −5.9005369 |
| Wi{s,10} | −1.6834391 | 1.6662543 |
| Wi{s,11} | −0.2871787 | −1.0537841 |
| Wi{s,12} | −1.7927934 | −5.9023226 |
| Wi{s,13} | 8.3022116 | −0.2731127 |
| Wi{s,14} | −2.7479431 | 5.0231616 |
| Wi{s,15} | −5.5854112 | 5.6349576 |
| Wi{s,16} | 1.2288445 | 0.4765211 |
| Wi{s,17} | −4.9111278 | −5.5446961 |
| Wi{s,18} | −6.0798957 | 2.5347047 |
| Wi{s,19} | −2.9004902 | −1.8560627 |
| Wi{s,20} | −0.3563622 | 0.3671644 |
| Wi{s,21} | 0.4792034 | −1.6491173 |
| Wi{s,22} | −0.7248806 | 7.1122093 |
| Wi{s,23} | −0.7406803 | 10.360829 |
| Wi{s,24} | 0.1160807 | 4.8359502 |
| Wi{s,25} | 0.4699811 | −8.6634359 |
| Wi{s,26} | 2.1030666 | −4.5441764 |
| Wi{s,27} | 3.309815 | 8.8156683 |
| Wi{s,28} | 0.6025175 | 1.3123462 |
| Wi{s,29} | 2.1301649 | −0.5153287 |
| Wi{s,30} | 4.0466436 | −7.5138313 |
| Wi{s,31} | −1.4889536 | 0.2544955 |
| Wi{s,32} | 2.287042 | −5.3644162 |
| Wi{s,33} | 4.4242002 | −2.8862814 |
| Wi{s,34} | 1.6291247 | −3.5560135 |
| Wi{s,35} | 0.0894362 | −0.0343897 |
| Wo{1,1} | Wo{1,2} | |
| Wo{l,s} | 7.952817 | −9.1921023 |
| b1{35,1} | b1{s,1} | |
| 2.3093149 1.7504724 | ||
| b2{l,s} | ||
| b2{1,1} | −14.149185 |
| Birth Variables | |
|---|---|
| alower | aupper |
| −0.0395 | 0.0607 |
| blower | bupper |
| 0.9074 | 1.0703 |
| Birth and Hospitalization Variables | |
|---|---|
| alower | aupper |
| −0.0394 | 0.0524 |
| blower | bupper |
| 0.9191 | 1.0683 |
References
- Talavera, M.M.; Bixler, G.; Cozzi, C.; Dail, J.; Miller, R.R.; McClead, R., Jr.; Reber, K. Quality Improvement Initiative to Reduce the Necrotizing Enterocolitis Rate in Premature Infants. Pediatrics 2016, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanaroff, A.A.; Stoll, B.J.; Wright, L.L.; Carlo, W.A.; Ehrenkranz, R.A.; Stark, A.R.; Bauer, C.R.; Donovan, E.F.; Korones, S.B.; Laptook, A.R.; et al. Trends in neonatal morbidity and mortality for very low birthweight infants. Am. J. Obstet. Gynecol. 2007, 196, 147.e1–147.e8. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbons, S.C.; Ching, Y.; Yu, D.; Carpenter, J.; Kenny, M.; Weldon, C.; Lillehei, C.; Valim, C.; Horbar, J.D.; Jaksic, T. Mortality of necrotizing enterocolitis expressed by birth weight categories. J. Pediatr. Surg. 2009, 44, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Kochanek, K.D.; Murphy, S.L.; Tejada-Vera, B. Deaths: Final data for 2007. Natl. Vital Stat. Rep. 2010, 58, 1–19. [Google Scholar] [PubMed]
- Frost, B.L.; Modi, B.P.; Jaksic, T.; Caplan, M.S. New Medical and Surgical Insights into Neonatal Necrotizing Enterocolitis: A Review. JAMA Pediatr. 2017, 171, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.R.; Rellinger, E.J.; Hatch, L.D.; Weitkamp, J.-H.; Speck, K.E.; Danko, M.; Blakely, M.L. Surgical necrotizing enterocolitis. Semin. Perinatol. 2017, 41, 70–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.W.; Nasr, T.R.; Stoll, B.J. Necrotizing enterocolitis: Recent scientific advances in pathophysiology and prevention. Semin. Perinatol. 2008, 32, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, S.O.; Gordon, P.V.; Thomas, V.; Thorp, J.A.; Peabody, J.; Clark, R.H. Necrotizing enterocolitis among neonates in the United States. J. Perinatol. 2003, 23, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Holman, R.C.; Stehr-Green, J.K.; Zelasky, M.T. Necrotizing enterocolitis mortality in the United States, 1979–85. Am. J. Public Health 1989, 79, 987–989. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.W.; Stoll, B.J. Necrotising enterocolitis. Lancet 2006, 368, 1271–1283. [Google Scholar] [CrossRef]
- Gordon, P.; Christensen, R.; Weitkamp, J.-H.; Maheshwari, A. Mapping the New World of Necrotizing Enterocolitis (NEC): Review and Opinion. EJ Neonatol. Res. 2012, 2, 145–172. [Google Scholar] [PubMed]
- Bisquera, J.A.; Cooper, T.R.; Berseth, C.L. Impact of necrotizing enterocolitis on length of stay and hospital charges in very low birth weight infants. Pediatrics 2002, 109, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Gephart, S.M.; Spitzer, A.R.; Effken, J.A.; Dodd, E.; Halpern, M.; McGrath, J.M. Discrimination of GutCheck(NEC): A clinical risk index for necrotizing enterocolitis. J. Perinatol. 2014, 34, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Hintz, S.R.; Kendrick, D.E.; Stoll, B.J.; Vohr, B.R.; Fanaroff, A.A.; Donovan, E.F.; Poole, W.K.; Blakely, M.L.; Wright, L.; Higgins, R.; et al. Neurodevelopmental and growth outcomes of extremely low birth weight infants after necrotizing enterocolitis. Pediatrics 2005, 115, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.M.; Pierro, A.; Eaton, S. Neurodevelopmental outcomes of neonates with medically and surgically treated necrotizing enterocolitis. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F193–F198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neu, J.; Walker, W.A. Necrotizing enterocolitis. N. Engl. J. Med. 2011, 364, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Stanescu, A.L.; Liszewski, M.C.; Lee, E.Y.; Phillips, G.S. Neonatal Gastrointestinal Emergencies: Step-by-Step Approach. Radiol. Clin. N. Am. 2017, 55, 717–739. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.R.; Fullerton, B.S.; Modi, B.P. Neonatal Short Bowel Syndrome. Neoreviews 2017, 18, e480–e487. [Google Scholar] [CrossRef]
- Gephart, S.M.; McGrath, J.M.; Effken, J.A.; Halpern, M.D. Necrotizing enterocolitis risk: State of the science. Adv. Neonatal Care 2012, 12, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Mohri, M.; Rostamizadeh, A.; Talwalkar, A. Foundations of Machine Learning; MIT Press: Cambridge, MA, USA, 2012; ISBN 9780262018258. [Google Scholar]
- Cross, S.S.; Harrison, R.F.; Kennedy, R.L. Introduction to neural networks. Lancet 1995, 346, 1075–1079. [Google Scholar] [CrossRef]
- Liew, P.-L.; Lee, Y.-C.; Lin, Y.-C.; Lee, T.-S.; Lee, W.-J.; Wang, W.; Chien, C.-W. Comparison of artificial neural networks with logistic regression in prediction of gallbladder disease among obese patients. Dig. Liver Dis. 2007, 39, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Frize, M.; Ennett, C.M.; Stevenson, M.; Trigg, H.C.E. Clinical decision support systems for intensive care units: Using artificial neural networks. Med. Eng. Phys. 2001, 23, 217–225. [Google Scholar] [CrossRef]
- Malak, J.S.; Zeraati, H.; Nayeri, F.S.; Safdari, R.; Shahraki, A.D. Neonatal intensive care decision support systems using artificial intelligence techniques: A systematic review. Artif. Intell. Rev. 2018, 2012, 4919. [Google Scholar] [CrossRef]
- Rumelhart, D.E.; Zipser, D. Feature Discovery by Competitive Learning*. Cogn. Sci. 1985, 9, 75–112. [Google Scholar] [CrossRef] [Green Version]
- Guzmán-Bárcenas, J.; Hernández, J.A.; Arias-Martínez, J.; Baptista-González, H.; Ceballos-Reyes, G.; Irles, C. Estimation of umbilical cord blood leptin and insulin based on anthropometric data by means of artificial neural network approach: Identifying key maternal and neonatal factors. BMC Pregnancy Childbirth 2016, 16, 179. [Google Scholar] [CrossRef] [PubMed]
- Solis-Paredes, M.; Estrada-Gutierrez, G.; Perichart-Perera, O.; Montoya-Estrada, A.; Guzmán-Huerta, M.; Borboa-Olivares, H.; Bravo-Flores, E.; Cardona-Pérez, A.; Zaga-Clavellina, V.; Garcia-Latorre, E.; et al. Key Clinical Factors Predicting Adipokine and Oxidative Stress Marker Concentrations among Normal, Overweight and Obese Pregnant Women Using Artificial Neural Networks. Int. J. Mol. Sci. 2017, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.J.; Ternberg, J.L.; Feigin, R.D.; Keating, J.P.; Marshall, R.; Barton, L.; Brotherton, T. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.C.; Kliegman, R.M. Necrotizing Enterocolitis: Treatment Based on Staging Criteria. Pediatr. Clin. N. Am. 1986, 33, 179–201. [Google Scholar] [CrossRef]
- Levenberg, K. A method for the solution of certain non-linear problems in least squares. Q. Appl. Math. 1944, 2, 164–168. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.P.; Andaverde, J.; Santoyo, E. Application of the error propagation theory in estimates of static formation temperatures in geothermal and petroleum boreholes. Energy Convers. Manag. 2006, 47, 3659–3671. [Google Scholar] [CrossRef]
- Yu, L.; Tian, J.; Zhao, X.; Cheng, P.; Chen, X.; Yu, Y.; Ding, X.; Zhu, X.; Xiao, Z. Bowel Perforation in Premature Infants with Necrotizing Enterocolitis: Risk Factors and Outcomes. Gastroenterol. Res. Pract. 2016, 2016, 6134187. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Dong, W.; Zhang, L.; Zhai, X.; Li, Q.; Lei, X. Correlative Factors of the Deterioration of Necrotizing Enterocolitis in Small for Gestational Age Newborns. Sci. Rep. 2018, 8, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuels, N.; van de Graaf, R.A.; de Jonge, R.C.J.; Reiss, I.K.M.; Vermeulen, M.J. Risk factors for necrotizing enterocolitis in neonates: A systematic review of prognostic studies. BMC Pediatr. 2017, 17, 105. [Google Scholar] [CrossRef] [PubMed]
- Moss, R.L.; Kalish, L.A.; Duggan, C.; Johnston, P.; Brandt, M.L.; Dunn, J.C.Y.; Ehrenkranz, R.A.; Jaksic, T.; Nobuhara, K.; Simpson, B.J.; et al. Clinical parameters do not adequately predict outcome in necrotizing enterocolitis: A multi-institutional study. J. Perinatol. 2008, 28, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Ling, X.B.; Zhao, Y.; Hu, Z.; Zheng, X.; Xu, Z.; Wen, Q.; Kastenberg, Z.J.; Li, P.; Abdullah, F.; et al. A data-driven algorithm integrating clinical and laboratory features for the diagnosis and prognosis of necrotizing enterocolitis. PLoS ONE 2014, 9, e89860. [Google Scholar] [CrossRef] [PubMed]
- Berkhout, D.J.C.; Klaassen, P.; Niemarkt, H.J.; de Boode, W.P.; Cossey, V.; van Goudoever, J.B.; Hulzebos, C.V.; Andriessen, P.; van Kaam, A.H.; Kramer, B.W.; et al. Risk Factors for Necrotizing Enterocolitis: A Prospective Multicenter Case-Control Study. Neonatology 2018, 114, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Drenckpohl, D.; Knaub, L.; Schneider, C.; McConnell, C.; Wang, H.; Macwan, K. Risk Factors That May Predispose Premature Infants to Increased Incidence of Necrotizing Enterocolitis. Infant Child Adolesc. Nutr. 2010, 2, 37–44. [Google Scholar] [CrossRef]
- Carter, B.M.; Holditch-Davis, D. Risk factors for necrotizing enterocolitis in preterm infants: How race, gender, and health status contribute. Adv. Neonatal Care 2008, 8, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Duci, M.; Fascetti-Leon, F.; Erculiani, M.; Priante, E.; Cavicchiolo, M.E.; Verlato, G.; Gamba, P. Neonatal independent predictors of severe NEC. Pediatr. Surg. Int. 2018, 34, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Park, K.-H.; Kim, A.; Yang, H.-R.; Jung, E.-Y.; Cho, S.-H. Maternal and Placental Risk Factors for Developing Necrotizing Enterocolitis in Very Preterm Infants. Pediatr. Neonatol. 2017, 58, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-P.; Lei, X.-P.; Luo, L.-J.; Dong, W.-B. Risk factors for necrotizing enterocolitis in very preterm infants: A case-control study in southwest China. J. Matern. Fetal Neonatal Med. 2017, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bashiri, A.; Zmora, E.; Sheiner, E.; Hershkovitz, R.; Shoham-Vardi, I.; Mazor, M. Maternal hypertensive disorders are an independent risk factor for the development of necrotizing enterocolitis in very low birth weight infants. Fetal Diagn. Ther. 2003, 18, 404–407. [Google Scholar] [CrossRef] [PubMed]
- March, M.I.; Gupta, M.; Modest, A.M.; Wu, L.; Hacker, M.R.; Martin, C.R.; Rana, S. Maternal risk factors for neonatal necrotizing enterocolitis. J. Matern. Fetal Neonatal Med. 2014, 28, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jilling, T.; Ambalavanan, N.; Cotten, C.M.; Martin, C.A.; Maheshwari, A.; Schibler, K.; Levy, J.; Page, G.P. Surgical necrotizing enterocolitis in extremely premature neonates is associated with genetic variations in an intergenic region of chromosome 8. Pediatr. Res. 2018, 83, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Manogura, A.C.; Turan, O.; Kush, M.L.; Berg, C.; Bhide, A.; Turan, S.; Moyano, D.; Bower, S.; Nicolaides, K.H.; Galan, H.L.; et al. Predictors of necrotizing enterocolitis in preterm growth-restricted neonates. Am. J. Obstet. Gynecol. 2008, 198, 638.e1–638.e5. [Google Scholar] [CrossRef] [PubMed]
- Tepas, J.J., 3rd; Sharma, R.; Leaphart, C.L.; Celso, B.G.; Pieper, P.; Esquivia-Lee, V. Timing of surgical intervention in necrotizing enterocolitis can be determined by trajectory of metabolic derangement. J. Pediatr. Surg. 2010, 45, 310–313. [Google Scholar] [CrossRef] [PubMed]





| Variables | Control Group (n = 27) | NEC (n = 23) | IP (n = 26) | P |
|---|---|---|---|---|
| Age (years) | 28.04 ± 1.77 | 25.74 ± 1.60 | 31.31 ± 1.41 | 0.06 |
| Preeclampsia (%) | 14.81 | 30.43 | 26.92 | 0.39 |
| Hypertension (%) | 7.407 | 8.63 | 11.54 | 0.87 |
| Overweight/Obesity (%) | 11.11 | 0 | 11.54 | 0.24 |
| Hypothyroidism (%) | 18.52 | 4.34 | 3.84 | 0.11 |
| Chorioamnionitis (%) | 11.11 | 17.39 | 11.54 | 0.77 |
| No. Offsprings (range) | 1–3 | 1–2 | 1–3 | |
| Intra Uterine Growth Restriction (%) | 11.11 | 39.13 | 26.92 | 0.07 |
| Variables | Control (n = 27) | NEC (n = 23) | IP (n = 26) | P |
|---|---|---|---|---|
| Gestational age (weeks) | 30.8 ± 0.42 | 30.3 ± 0.52 | 30.3 ± 0.46 | 0.71 |
| Birthweight (g) | 1384 ± 95.5 | 1085 ± 65.8 | 1141 ± 65.21 | 0.01 1 |
| Height (cm) | 39.76 ± 0.82 | 36.72 ± 0.77 | 37.29 ± 0.89 | 0.02 1 |
| Sex (male, %) | 59.26 | 43.48 | 57.71 | 0.48 |
| Input Variable | Range |
|---|---|
| Gestational age (weeks) | 25–34.4 |
| Maternal age (years) | 14–44 |
| Maternal morbidity | 0–15 (see Appendix A) |
| Chorioaminionitis (y/n) | 0–1 |
| Prenatal antibiotic (y/n) | 0–1 |
| Number of offsprings | 0–3 |
| Premature rupture of membranes (y/n) | 0–1 |
| Indirect oxygen (y/n) | 0–1 |
| T-piece (y/n) | 0–1 |
| CPAP (y/n) | 0–1 |
| PPV (y/n) | 0–1 |
| OTI (y/n) | 0–1 |
| Birth weight (g) | 560–3125 |
| Sex (female/male, 1/2) | 1–2 |
| Arterial pH value | 6.96–7.41 |
| Arterial CO2 (mm Hg) | 19.4–72.1 |
| Arterial HCO3 (mmol/L) | 9.6–34.5 |
| Arterial Base Deficit (mEq/L) | −16.9–7.9 |
| Diastolic arterial blood pressure | 20–56 |
| Leukocytes (cells/mm3) | 2800–39,940 |
| Neutrophils (cells/mm3) | 1008–24,000 |
| Platelets (cells/mm3) | 12,200–439,000 |
| Catheter location (absence, 0; high or low placed umbilical arterial, 1 or 2) | 0–2 |
| Input Variable | Range |
|---|---|
| Gestational age (weeks) | 25–34.4 |
| Maternal Age (years) | 14–44 |
| Maternal morbidity | 0–15 (see Appendix A) |
| Chorioaminionitis (y/n) | 0–1 |
| Prenatal antibiotic (y/n) | 0–1 |
| Premature rupture of membranes (y/n) | 0–1 |
| Maternal infection (y/n) | 0–1 |
| IUGR (y/n) | 0–1 |
| Indirect oxygen (y/n) | 0–1 |
| T-piece (y/n) | 0–1 |
| CPAP (y/n) | 0–1 |
| PVV (y/n) | 0–1 |
| OTI (y/n) | 0–1 |
| Birth weight (g) | 560–3125 |
| Sex (female/male, 1/2) | 1–2 |
| Arterial pH value | 6.96–7.41 |
| Arterial CO2 (mm Hg) | 19.4–72.1 |
| Arterial HCO3 (mmol/L) | 9.6–34.5 |
| Arterial Base Deficit (mEq/L) | −16.9–7.9 |
| Use of formula (y/n) | 0–1 |
| Use of human milk (y/n) | 0–1 |
| First day of oral feeding (day) | 1–3 |
| Apnea (y/n) | 0–1 |
| Gastric residuals (y/n) | 0–1 |
| Diastolic arterial blood pressure | 20–56 |
| Leukocytes (cells/mm3) | 2800–39,940 |
| Neutrophils (cells/mm3) | 1008–24,000 |
| Platelets (cells/mm3) | 12,200–439,000 |
| Catheter location (absence, low, high, hepatic) | 0–3 |
| Antibiotic schemes | 1–2 |
| PDA (y/n) | 0–1 |
| Blood transfusions (y/n) | 0–1 |
| Hypotension (y/n) | 0–1 |
| Early sepsis (y/n) | 0–1 |
| Late sepsis (y/n) | 0–1 |
| Catheter location (absence, 0; high or low placed umbilical arterial, 1 or 2) | 0–2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irles, C.; González-Pérez, G.; Carrera Muiños, S.; Michel Macias, C.; Sánchez Gómez, C.; Martínez-Zepeda, A.; Cordero González, G.; Laresgoiti Servitje, E. Estimation of Neonatal Intestinal Perforation Associated with Necrotizing Enterocolitis by Machine Learning Reveals New Key Factors. Int. J. Environ. Res. Public Health 2018, 15, 2509. https://doi.org/10.3390/ijerph15112509
Irles C, González-Pérez G, Carrera Muiños S, Michel Macias C, Sánchez Gómez C, Martínez-Zepeda A, Cordero González G, Laresgoiti Servitje E. Estimation of Neonatal Intestinal Perforation Associated with Necrotizing Enterocolitis by Machine Learning Reveals New Key Factors. International Journal of Environmental Research and Public Health. 2018; 15(11):2509. https://doi.org/10.3390/ijerph15112509
Chicago/Turabian StyleIrles, Claudine, Gabriela González-Pérez, Sandra Carrera Muiños, Carolina Michel Macias, César Sánchez Gómez, Anahid Martínez-Zepeda, Guadalupe Cordero González, and Estibalitz Laresgoiti Servitje. 2018. "Estimation of Neonatal Intestinal Perforation Associated with Necrotizing Enterocolitis by Machine Learning Reveals New Key Factors" International Journal of Environmental Research and Public Health 15, no. 11: 2509. https://doi.org/10.3390/ijerph15112509