Does Hospital Competition Harm Inpatient Quality? Empirical Evidence from Shanxi, China

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
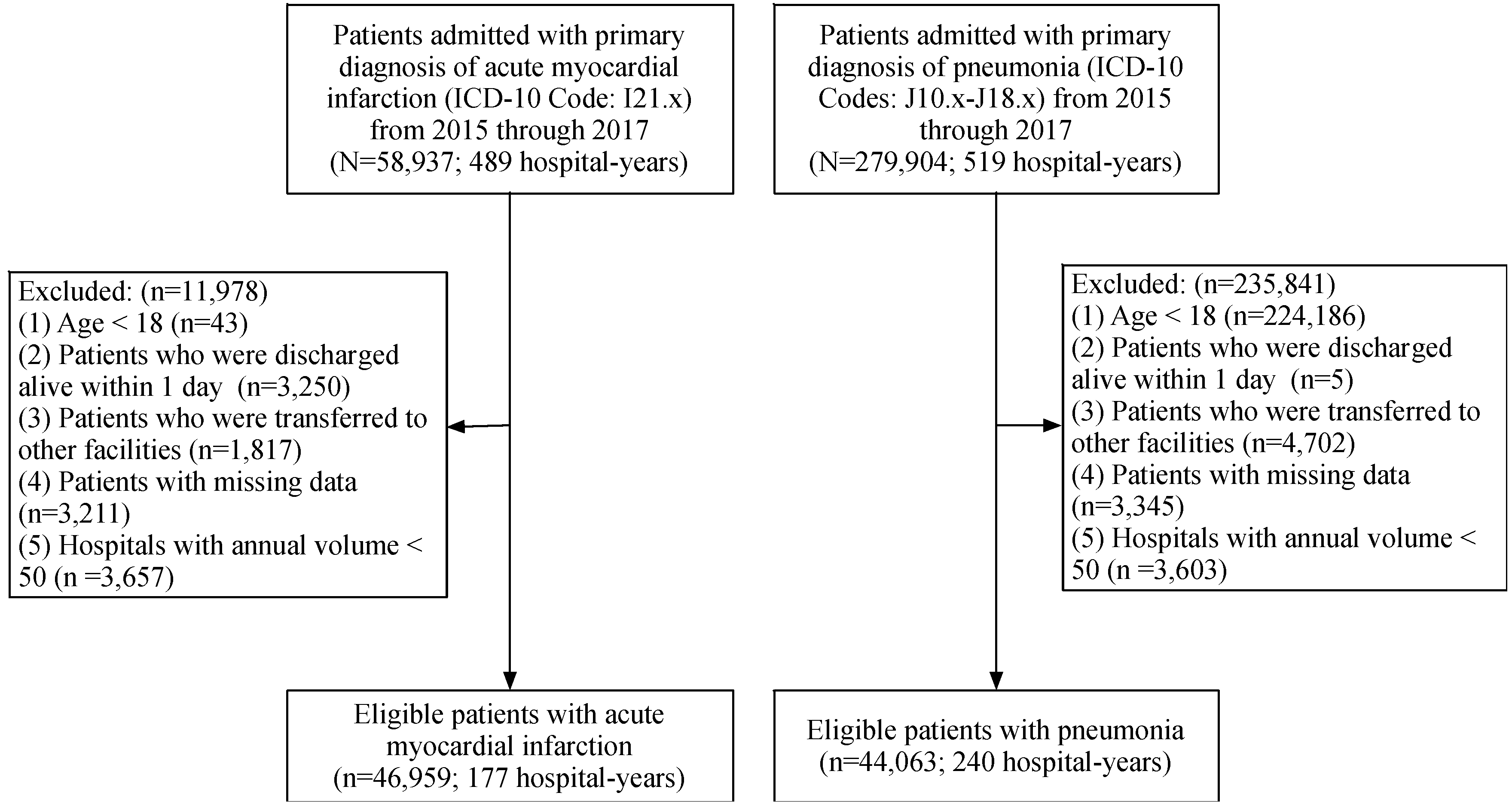
2.2. Study Population
2.3. Variables of Interest
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AMI | Acute Myocardial Infarction |
| CI | Confidence Interval |
| ECI | Elixhauser Comorbidity Index |
| HHI | Herfindahl-Hirschman Index |
| ICD-9 | The International Classification of Disease, Ninth Revision |
| ICD-10 | The International Classification of Disease, Tenth Revision |
| NCMS | The Rural New Cooperative Medical Scheme |
| OR | Odds Ratio |
| UEBMI | The Urban Employee-based Basic Medical Insurance Scheme |
| URBMI | The Urban Resident-based Basic Medical Insurance Scheme |
References
- Yip, W.; Hsiao, W.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Yip, W.; Hsiao, W. Harnessing the privatisation of China’s fragmented health-care delivery. Lancet 2014, 384, 805–818. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, Y.; Shu, T.; Yang, W.; Liang, M. Variations in the quality of care at large public hospitals in Beijing, China: A condition-based outcome approach. PLoS ONE 2015, 10, e0138948. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Liu, E.; Tao, H.; Qian, Z.; Lin, X. Does level of hospital matter? A study of mortality of acute myocardial infarction patients in Shanxi, China. Am. J. Med. Qual. 2018, 33, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Qin, X.; Hsieh, C.R. Is the pro-competition policy an effective solution for China’s public hospital reform? Health Econ. Policy Law 2016, 11, 337–357. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Qin, X.; Li, Q.; Messina, J.P.; Delamater, P.L. Does hospital competition improve health care delivery in China? China Econ. Rev. 2015, 33, 179–199. [Google Scholar] [CrossRef]
- The Standing Conference of State Council of China Adopted Guidelines for Furthering the Reform of Health-Care System in Principle. Available online: http://www.gov.cn/jrzg/2009-04/06/content_1278721.htm (accessed on 4 June 2018).
- Announcement of Strategic Plan on National Health Care Service System (2015–2020). Available online: http://www.gov.cn/zhengce/content/2015-03/30/content_9560.htm (accessed on 4 June 2018).
- Liu, G.; Vortherms, S.; Hong, X. China’s health reform update. Annu. Rev. Public Health 2017, 38, 431–448. [Google Scholar] [CrossRef] [PubMed]
- Eggleston, K.; Ling, L.; Qingyue, M.; Lindelow, M.; Wagstaff, A. Health service delivery in China: A literature review. Health Econ. 2008, 17, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Liu, G.G. The determinants of Chinese provincial government health expenditures: Evidence from 2002–2006 data. Health Econ. 2012, 21, 757–777. [Google Scholar] [CrossRef] [PubMed]
- Eggleston, K. “Kan bing nan, kan bing gui”: Challenges for China’s healthcare system thirty years into reform. In Growing Pains: Tensions and Opportunities in China’s Transformation; Walter H. Shorenstein Asia-Pacific Research Center: Stanford, CA, USA, 2010. [Google Scholar]
- Porter, M.E.; Teisberg, E.O. Redefining Health Care: Creating Value-Based Competition on Results, 1st ed.; Harvard Business Review Press: Brighton, MA, USA, 2006. [Google Scholar]
- Gaynor, M.; Moreno-Serra, R.; Propper, C. Can competition improve outcomes in UK health care? Lessons from the past two decades. J. Health Serv. Res. Policy 2012, 17, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Croes, R.R.; Krabbe-Alkemade, Y.J.F.M.; Mikkers, M.C. Competition and quality indicators in the health care sector: Empirical evidence from the Dutch hospital sector. Eur. J. Health Econ. 2017, 19, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Mutter, R.L.; Wong, H.S.; Goldfarb, M.G. The effects of hospital competition on inpatient quality of care. Inquiry 2008, 45, 263–279. [Google Scholar] [CrossRef] [PubMed]
- Ghiasi, A.; Zengul, F.D.; Ozaydin, B.; Oner, N.; Breland, B.K. The impact of hospital competition on strategies and outcomes of hospitals: A systematic review of the U.S. Hospitals 1996–2016. J. Health Care Financ. 2018, 44, 22–42. [Google Scholar]
- Kessler, D.P.; McClellan, M.B. Is hospital competition socially wasteful? Q. J. Econ. 2000, 115, 577–615. [Google Scholar] [CrossRef]
- Cooper, Z.; Gibbons, S.; Jones, S.; McGuire, A. Does hospital competition save lives? Evidence from the english nhs patient choice reforms. Econ. J. 2011, 121, F228–F260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaynor, M.; Moreno-Serra, R.; Propper, C. Death by market power: Reform, competition, and patient outcomes in the national health service. Am. Econ. J. Econ. Policy 2013, 5, 134–166. [Google Scholar] [CrossRef]
- Bloom, N.; Propper, C.; Seiler, S.; Van Reenen, J. The impact of competition on management quality: Evidence from public hospitals. Rev. Econ. Stud. 2013, 82, 457–489. [Google Scholar] [CrossRef]
- Propper, C.; Burgess, S.; Green, K. Does competition between hospitals improve the quality of care? J. Public Econ. 2004, 88, 1247–1272. [Google Scholar] [CrossRef]
- Gowrisankaran, G.; Town, R.J. Competition, payers, and hospital quality. Health Serv. Res. 2003, 38, 1403–1422. [Google Scholar] [CrossRef]
- Palangkaraya, A.; Yong, J. Effects of competition on hospital quality: An examination using hospital administrative data. Eur. J. Health Econ. 2012, 14, 415–429. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.S.; Zhan, C.; Mutter, R. Do different measures of hospital competition matter in empirical investigations of hospital behavior? Rev. Ind. Organ. 2005, 26, 61–87. [Google Scholar] [CrossRef]
- Maeda, J.L.K.; Lo Sasso, A.T. The relationship between hospital market competition, evidence-based performance measures, and mortality for chronic heart failure. Inquiry 2012, 49, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Colla, C.; Bynum, J.; Austin, A.; Skinner, J. Hospital competition, quality, and expenditures in the US Medicare population. NBER 2016. [Google Scholar] [CrossRef]
- Yang, Q.; Pan, J. Control under times of uncertainty: The relationship between hospital competition and physician-patient disputes. Int. J. Equity Health 2017, 16, 205. [Google Scholar] [CrossRef] [PubMed]
- Shanxi Provincial Bureau of Statistics. Shanxi Statistical Yearbook 2017; China Statistics Press: Beijing, China, 2018.
- Cannon, C.P.; Gibson, C.M.; Lambrew, C.T.; Shoultz, D.A.; Levy, D.; French, W.J.; Gore, J.M.; Weaver, W.D.; Rogers, W.J.; Tiefenbrunn, A.J. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA 2000, 283, 2941–2947. [Google Scholar] [CrossRef] [PubMed]
- Yurkovich, M.; Avina-Zubieta, J.A.; Thomas, J.; Gorenchtein, M.; Lacaille, D. A systematic review identifies valid comorbidity indices derived from administrative health data. J. Clin. Epidemiol. 2015, 68, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Sharabiani, M.; Aylin, P.; Bottle, A. Systematic review of comorbidity indices for administrative data. Med. Care 2012, 50, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Van Walraven, C.; Austin, P.C.; Jennings, A.; Quan, H. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med. Care 2009, 47, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Hentschker, C.; Mennicken, R. The volume-outcome relationship revisited: Practice indeed makes perfect. Health Serv. Res. 2018, 53, 15–34. [Google Scholar] [CrossRef] [PubMed]
- Hartz, A.J.; Krakauer, H.; Kuhn, E.M.; Young, M.; Jacobsen, S.J.; Gay, G.; Muenz, L.; Katzoff, M.; Bailey, R.C.; Rimm, A.A. Hospital characteristics and mortality rates. N. Engl. J. Med. 1989, 321, 1720–1725. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Park, E.-C.; Kim, S.J.; Han, K.-T.; Jang, S.-I. How did market competition affect outpatient utilization under the diagnosis-related group-based payment system? J. Qual. Health Care 2017, 29, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Doyle, J.; Graves, J.; Gruber, J.; Kleiner, S. Measuring returns to hospital care: Evidence from ambulance referral patterns. J. Political Econ. 2015, 123, 170–214. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhang, Z. Skilled doctors in tertiary hospitals are already overworked in China. Lancet Glob. Health 2015, 3, e737. [Google Scholar] [CrossRef]
- Needleman, J.; Buerhaus, P.; Pankratz, V.S.; Leibson, C.L.; Stevens, S.R.; Harris, M. Nurse staffing and inpatient hospital mortality. N. Engl. J. Med. 2011, 364, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.J.; Young, R.S.; Brice, J.; Aguiar, R.; Kolm, P. Effect of hospitalist workload on the quality and efficiency of care. JAMA Intern. Med. 2014, 174, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, X.; Wang, Q.; Hu, S.; Wang, Y.; Masoudi, F.A.; Spertus, J.A.; Krumholz, H.M.; Jiang, L.; China PEACE Collaborative Group. ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): A retrospective analysis of hospital data. Lancet 2015, 385, 441–451. [Google Scholar] [CrossRef]
- Lin, X.; Cai, M.; Tao, H.; Liu, E.; Cheng, Z.; Xu, C.; Wang, M.; Xia, S.; Jiang, T. Insurance status, inhospital mortality and length of stay in hospitalised patients in Shanxi, China: A cross-sectional study. BMJ Open 2017, 7, e015884. [Google Scholar] [CrossRef] [PubMed]
- State Council of People’s Republic of China. Guideline for Integration of Basic Medical Insurance for Urban Employees and the New Rural Cooperative Medical Scheme. 2016. Available online: http://www.gov.cn/zhengce/content/2016-01/12/content_10582.htm (accessed on 4 June 2018).



{kind=link}
{kind=link}
| Acute Myocardial Infarction | Pneumonia | |||||
|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | |
| Main Interest | ||||||
| Competition (−ln of HHI) | 1.55 ± 0.50 | 1.63 ± 0.46 | 1.60 ± 0.46 | 1.50 ± 0.67 | 1.66 ± 0.70 | 1.53 ± 0.64 |
| Outcome variable | ||||||
| Death, n (%) | 393 (2.7) | 471 (2.8) | 346 (2.2) | 197 (1.7) | 325 (1.9) | 215 (1.4) |
| Patient characteristics | ||||||
| Age (year), mean ± SD | 61.52 ± 12.66 | 61.84 ± 12.81 | 61.79 ± 12.48 | 65.21 ± 17.42 | 64.70 ± 18.14 | 65.14 ± 17.58 |
| Female, n (%) | 3736 (25.3) | 4163 (24.9) | 3727 (24.1) | 4558 (40.1) | 7282 (43.1) | 6659 (42.1) |
| Insurance | ||||||
| NCMS, n (%) | 6593 (44.7) | 7727 (46.2) | 7425 (48.0) | 4156 (36.6) | 5698 (33.7) | 5648 (35.7) |
| URBMI, n (%) | 948 (6.4) | 1227 (7.3) | 993 (6.4) | 850 (7.5) | 1515 (9.0) | 1437 (9.1) |
| UEBMI, n (%) | 5114 (34.7) | 5528 (33.1) | 5084 (32.8) | 4716 (41.5) | 7098 (42.0) | 6402 (40.5) |
| Self-payment, n (%) | 1347 (9.1) | 1364 (8.2) | 1380 (8.9) | 972 (8.6) | 1393 (8.2) | 1275 (8.1) |
| Other, n (%) | 755 (5.1) | 873 (5.2) | 601 (3.9) | 662 (5.8) | 1192 (7.1) | 1049 (6.6) |
| Emergency visit, n (%) | 6851 (46.4) | 7752 (46.4) | 7565 (48.9) | 1941 (17.1) | 3096 (18.3) | 2971 (18.8) |
| Admission status | ||||||
| General, n (%) | 8470 (57.4) | 9035 (54.0) | 8077 (52.2) | 9996 (88.0) | 14613 (86.5) | 13612 (86.1) |
| Acute, n (%) | 3360 (22.8) | 4288 (25.6) | 4220 (27.3) | 1111 (9.8) | 1804 (10.7) | 1655 (10.5) |
| Urgent, n (%) | 2927 (19.8) | 3396 (20.3) | 3186 (20.6) | 249 (2.2) | 479 (2.8) | 544 (3.4) |
| Severity | ||||||
| Low severity, n (%) | 1549 (10.5) | 1455 (8.7) | 1074 (6.9) | 3532 (31.1) | 5047 (29.9) | 4288 (27.1) |
| Moderate severity, n (%) | 7353 (49.8) | 7786 (46.6) | 7035 (45.4) | 5030 (44.3) | 7116 (42.1) | 6524 (41.3) |
| High severity, n (%) | 5855 (39.7) | 7478 (44.7) | 7374 (47.6) | 2794 (24.6) | 4733 (28.0) | 4999 (31.6) |
| Elixhauser index, mean ± SD | 7.24 ± 5.96 | 7.85 ± 5.88 | 7.82 ± 5.89 | 3.97 ± 5.36 | 4.13 ± 5.44 | 4.32 ± 5.55 |
| Length of stay (days), mean ± SD | 12.01 ± 6.01 | 11.68 ± 5.91 | 11.19 ± 5.53 | 12.30 ± 7.41 | 12.26 ± 7.15 | 12.06 ± 7.08 |
| Hospital characteristics | ||||||
| Tertiary hospital, n (%) | 12213 (82.8) | 13853 (82.9) | 12996 (83.9) | 7046 (62.0) | 9521 (56.4) | 8614 (54.5) |
| Public hospital, n (%) | 12999 (88.1) | 14644 (87.6) | 13416 (86.6) | 8975 (79.0) | 14472 (85.7) | 13651 (86.3) |
| Bed size, mean ± SD | 1023.58 ± 472.29 | 1048.01 ± 497.81 | 1115.27 ± 490.16 | 953.00 ± 547.65 | 930.22 ± 578.98 | 919.77 ± 563.66 |
| Number of doctors per 100 beds, mean ± SD | 39.22 ± 7.74 | 39.88 ± 8.61 | 40.30 ± 8.44 | 38.64 ± 7.91 | 40.65 ± 10.45 | 40.60 ± 9.53 |
| Number of nurses per 100 beds, mean ± SD | 59.53 ± 15.73 | 63.66 ± 13.14 | 64.78 ± 13.65 | 55.59 ± 18.29 | 61.89 ± 18.51 | 61.02 ± 17.72 |
| Expected volume, mean ± SD | 382.54 ± 151.26 | 436.69 ± 171.86 | 405.15 ± 162.85 | 246.84 ± 119.36 | 290.30 ± 136.90 | 260.15 ± 115.86 |
| Total, n (%) | 14,757 (31.4) | 16,719 (35.6) | 15,483 (33.0) | 11,356 (25.8) | 16,896 (38.3) | 15,811 (35.9) |
| Acute Myocardial Infarction | Pneumonia | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Competition (−ln of HHI) | 0.94 | (0.77–1.11) | 1.99 | (1.51–2.64) |
| Age | 1.06 | (1.05–1.07) | 1.05 | (1.04–1.06) |
| Gender | ||||
| Male | Ref. | Ref. | ||
| Female | 1.38 | (1.21–1.57) | 0.78 | (0.65–0.93) |
| Admission source | ||||
| Outpatient visit | Ref. | Ref. | ||
| Emergency visit | 1.56 | (1.35–1.79) | 1.45 | (1.20–1.73) |
| Admission status | ||||
| General | Ref. | Ref. | ||
| Acute | 0.96 | (0.80–1.16) | 1.66 | (1.33–2.06) |
| Urgent | 2.76 | (2.36–3.24) | 6.86 | (5.48–8.59) |
| Insurance | ||||
| NCMS | Ref. | Ref. | ||
| URBMI | 1.62 | (1.30–2.01) | 2.26 | (1.53–3.32) |
| UEBMI | 1.78 | (1.53–2.07) | 2.94 | (2.18–3.96) |
| Self-payment | 0.98 | (0.74–1.30) | 1.79 | (1.18–2.73) |
| Others | 1.44 | (1.04–2.01) | 3.33 | (2.30–4.82) |
| Elixhauser index | 1.03 | (1.02–1.04) | 1.09 | (1.08–1.10) |
| Length of stay | 0.87 | (0.67–0.97) | 1.00 | (0.99–1.01) |
| Hospital grade | ||||
| Secondary hospital | Ref. | Ref. | ||
| Tertiary hospital | 1.38 | (0.77–2.47) | 1.55 | (0.92–2.64) |
| Ownership | ||||
| Private hospital | Ref. | Ref. | ||
| Public hospital | 1.73 | (1.12–2.67) | 1.91 | (1.24–2.95) |
| Beds | 0.95 | (0.92–0.98) | 0.99 | (0.95–1.04) |
| Number of doctors per 100 beds | 1.00 | (0.99–1.01) | 1.01 | (0.99–1.03) |
| Number of nurses per 100 beds | 1.00 | (0.99–1.01) | 1.01 | (0.99–1.02) |
| Expected volume (per 100 cases) | 1.01 | (0.99–1.02) | 1.00 | (0.99–1.01) |
| Year | ||||
| 2015 | Ref. | Ref. | ||
| 2016 | 0.97 | (0.73–1.30) | 0.78 | (0.54–1.14) |
| 2017 | 0.84 | (0.63–1.13) | 0.54 | (0.37–0.78) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, X.; Cai, M.; Fu, Q.; He, K.; Jiang, T.; Lu, W.; Ni, Z.; Tao, H. Does Hospital Competition Harm Inpatient Quality? Empirical Evidence from Shanxi, China. Int. J. Environ. Res. Public Health 2018, 15, 2283. https://doi.org/10.3390/ijerph15102283
Lin X, Cai M, Fu Q, He K, Jiang T, Lu W, Ni Z, Tao H. Does Hospital Competition Harm Inpatient Quality? Empirical Evidence from Shanxi, China. International Journal of Environmental Research and Public Health. 2018; 15(10):2283. https://doi.org/10.3390/ijerph15102283
Chicago/Turabian StyleLin, Xiaojun, Miao Cai, Qiang Fu, Kevin He, Tianyu Jiang, Wei Lu, Ziling Ni, and Hongbing Tao. 2018. "Does Hospital Competition Harm Inpatient Quality? Empirical Evidence from Shanxi, China" International Journal of Environmental Research and Public Health 15, no. 10: 2283. https://doi.org/10.3390/ijerph15102283
APA StyleLin, X., Cai, M., Fu, Q., He, K., Jiang, T., Lu, W., Ni, Z., & Tao, H. (2018). Does Hospital Competition Harm Inpatient Quality? Empirical Evidence from Shanxi, China. International Journal of Environmental Research and Public Health, 15(10), 2283. https://doi.org/10.3390/ijerph15102283