User-Centred Healing-Oriented Conditions in the Design of Hospital Environments


Abstract
1. Introduction
2. Materials and Methods
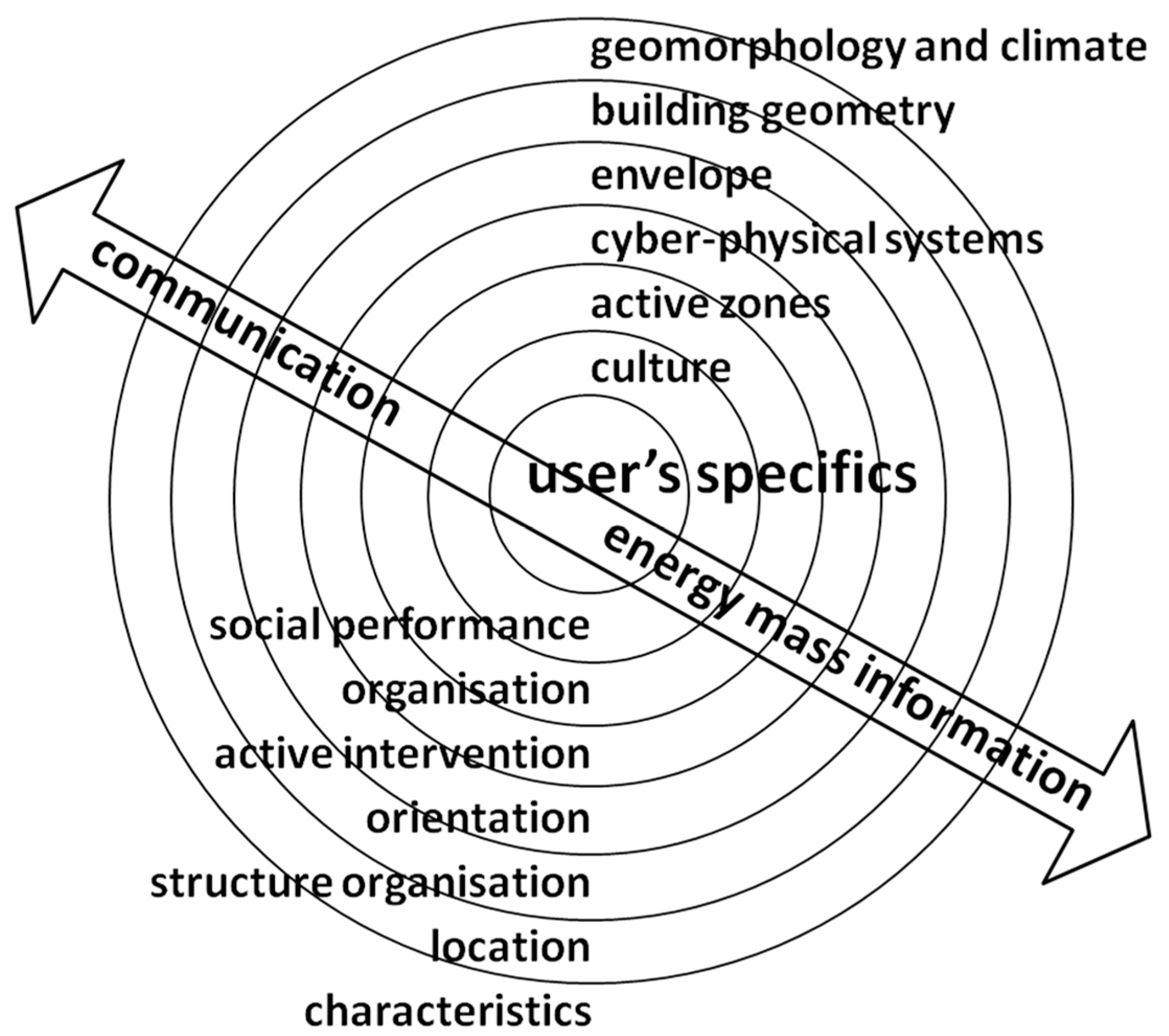
2.1. Design Morphology of a Healing Environment
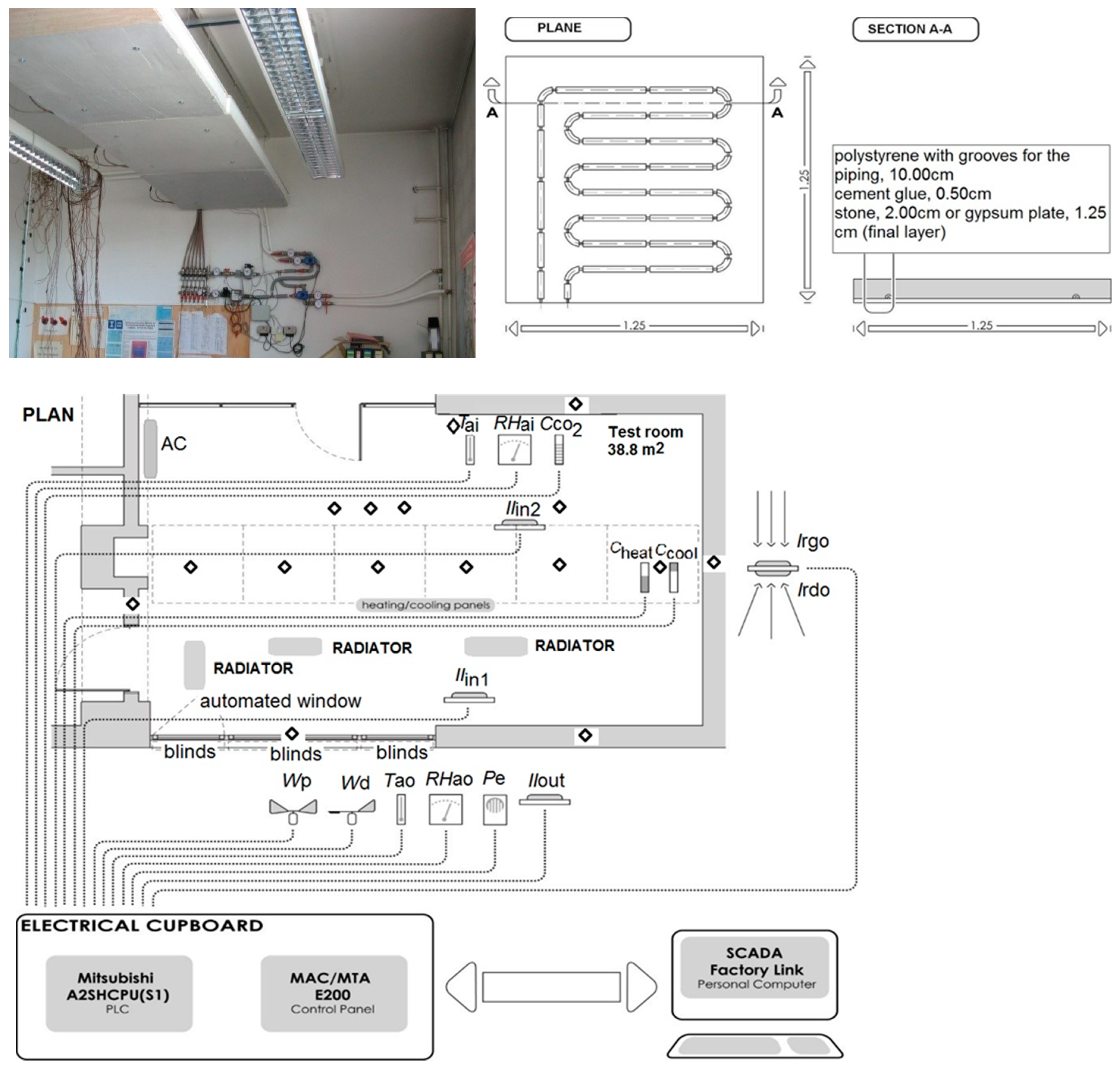
2.2. Experimental Part
2.3. Setting Thermal Exergy Balance of Burn Patient Body
3. Results
3.1. Design Morphology of Healing Environment
3.2. A Set of Influencing Parameters for Hospital Design
3.3. Definition of Specific User Needs and Demands
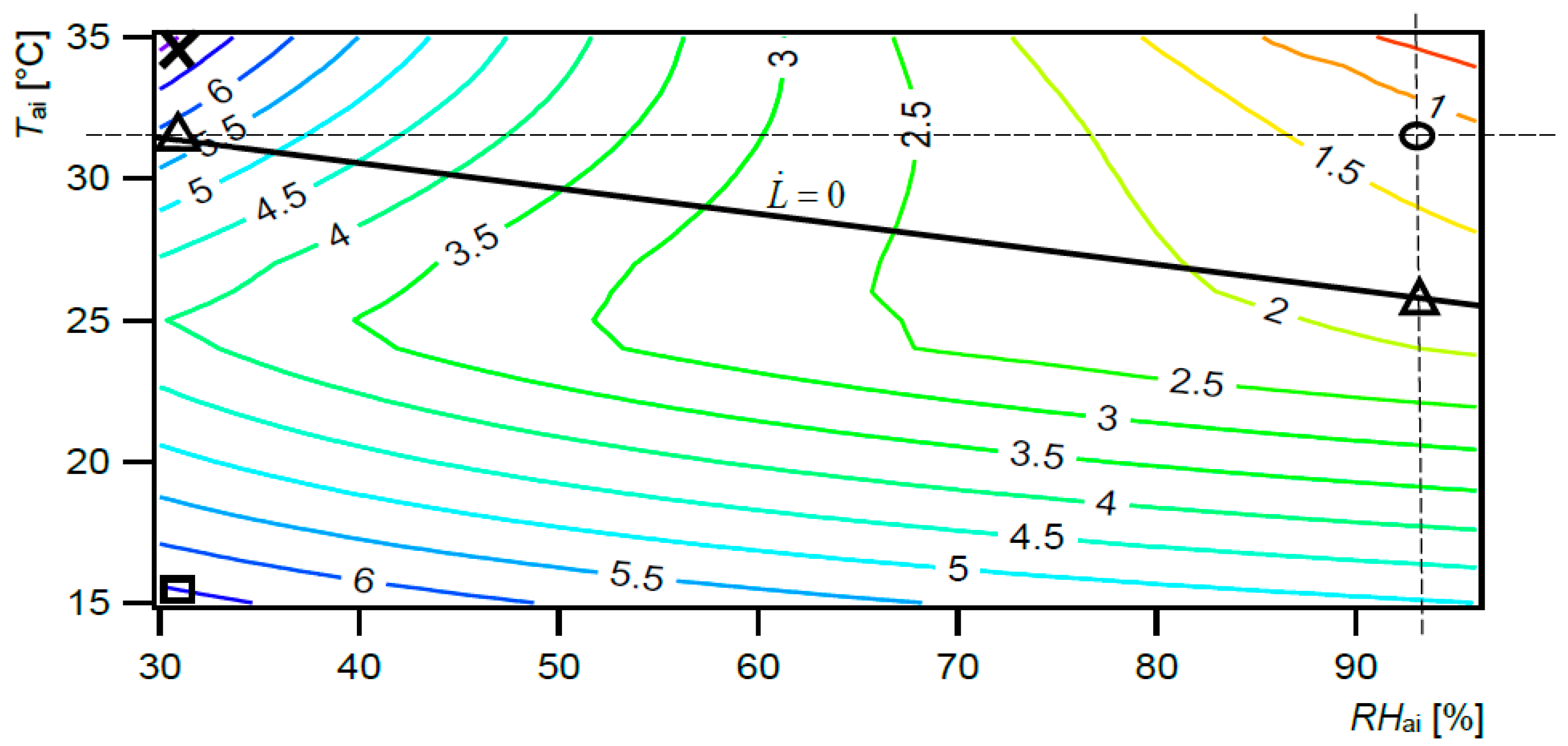
- Requirements for burn patient zone crated by conventional system. A ward for severe burn injuries should have temperature controls that permit adjusting the room temperature up to 32 °C and relative humidity up to 95% [9]. Tai and RHai should be maintained at 30–33 °C and 80%, respectively, in order to decrease energy demands and evaporative heat losses [23,24].
- Requirements for zone for a visitor and healthcare worker created by conventional system. The required air temperatures range from 20 °C to 26 °C due to the specifics of the ward facility [9,33,34] recommends maintaining the relative humidity in occupied spaces in the range from 30% to 60% and air temperature between 20 °C and 25 °C.
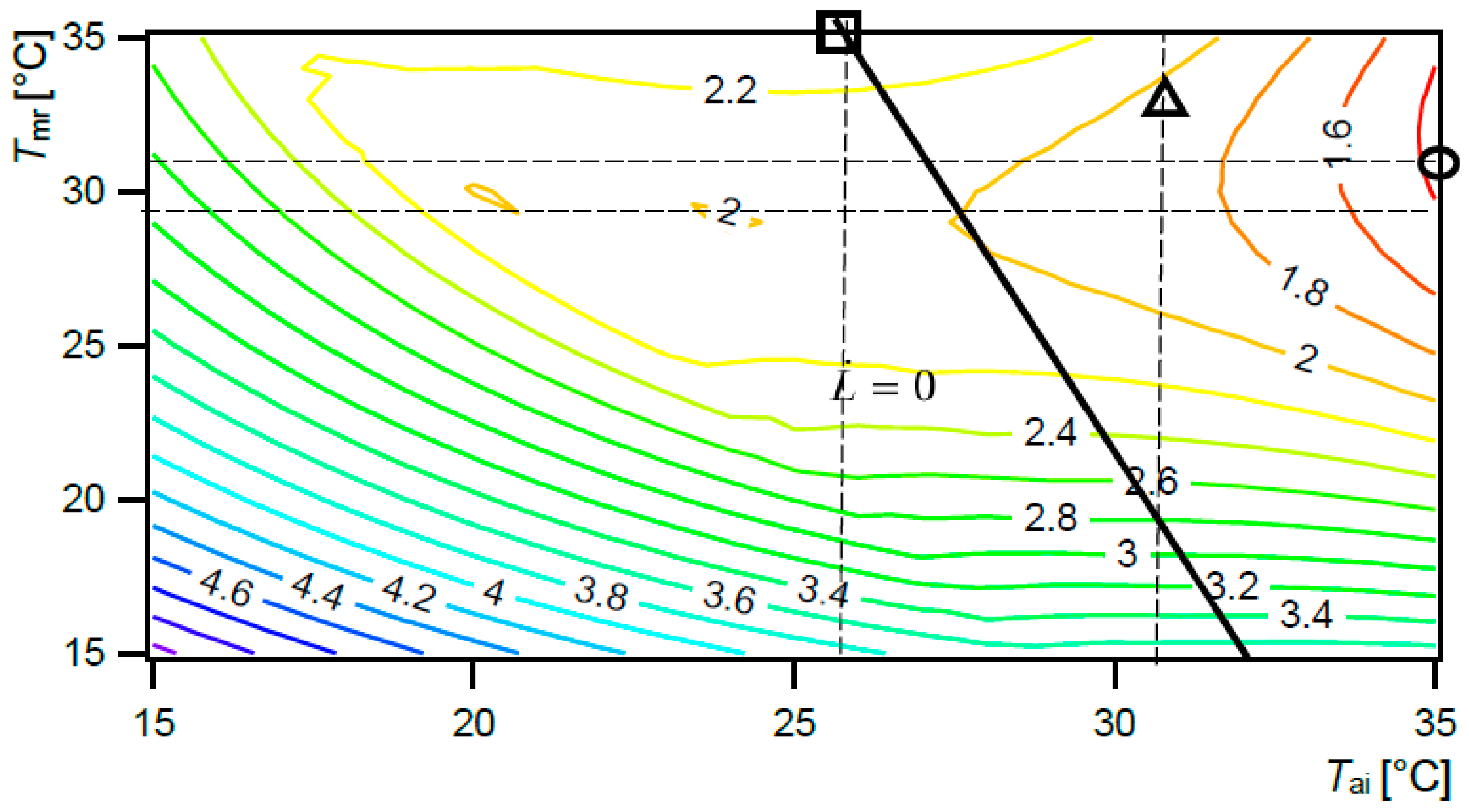
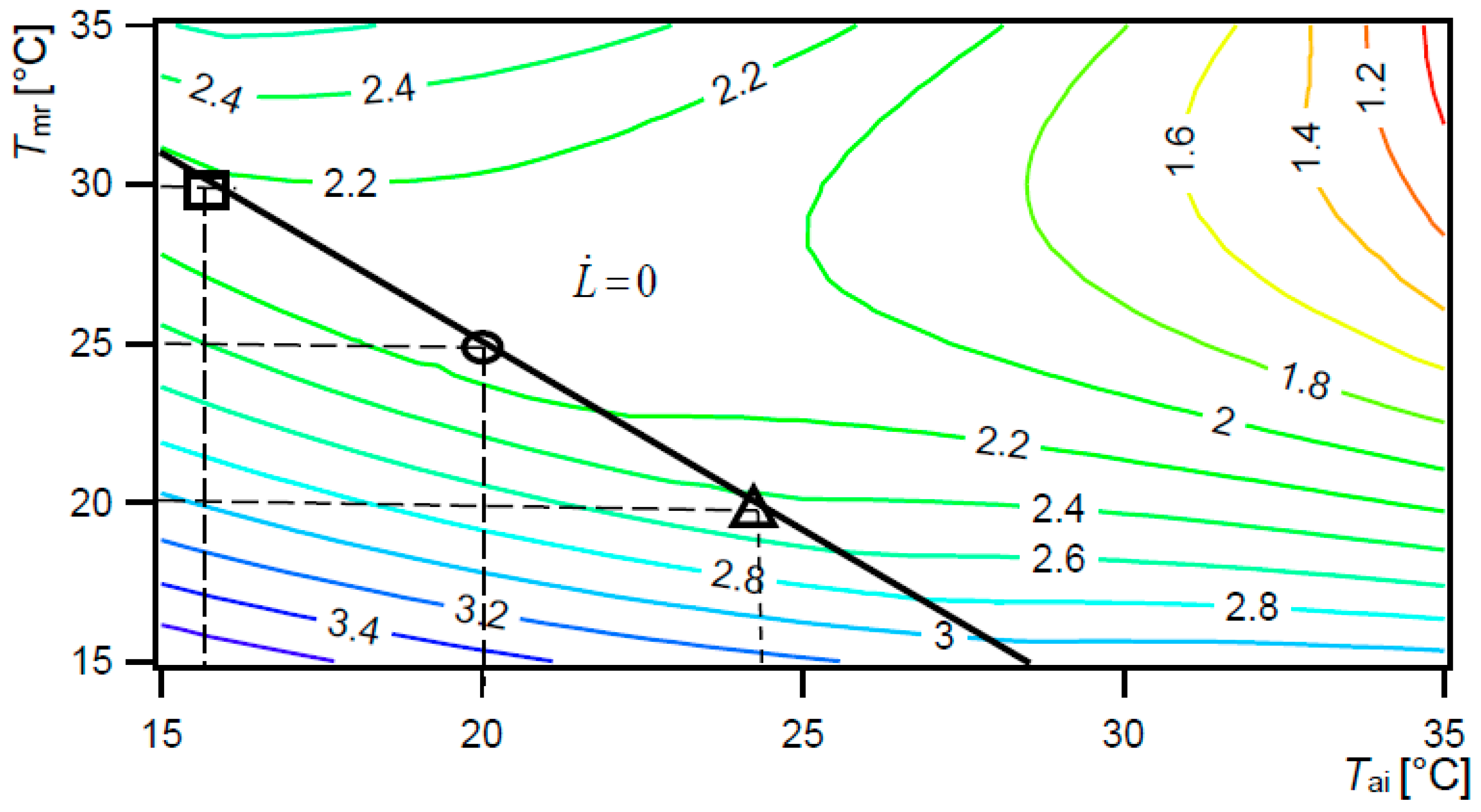
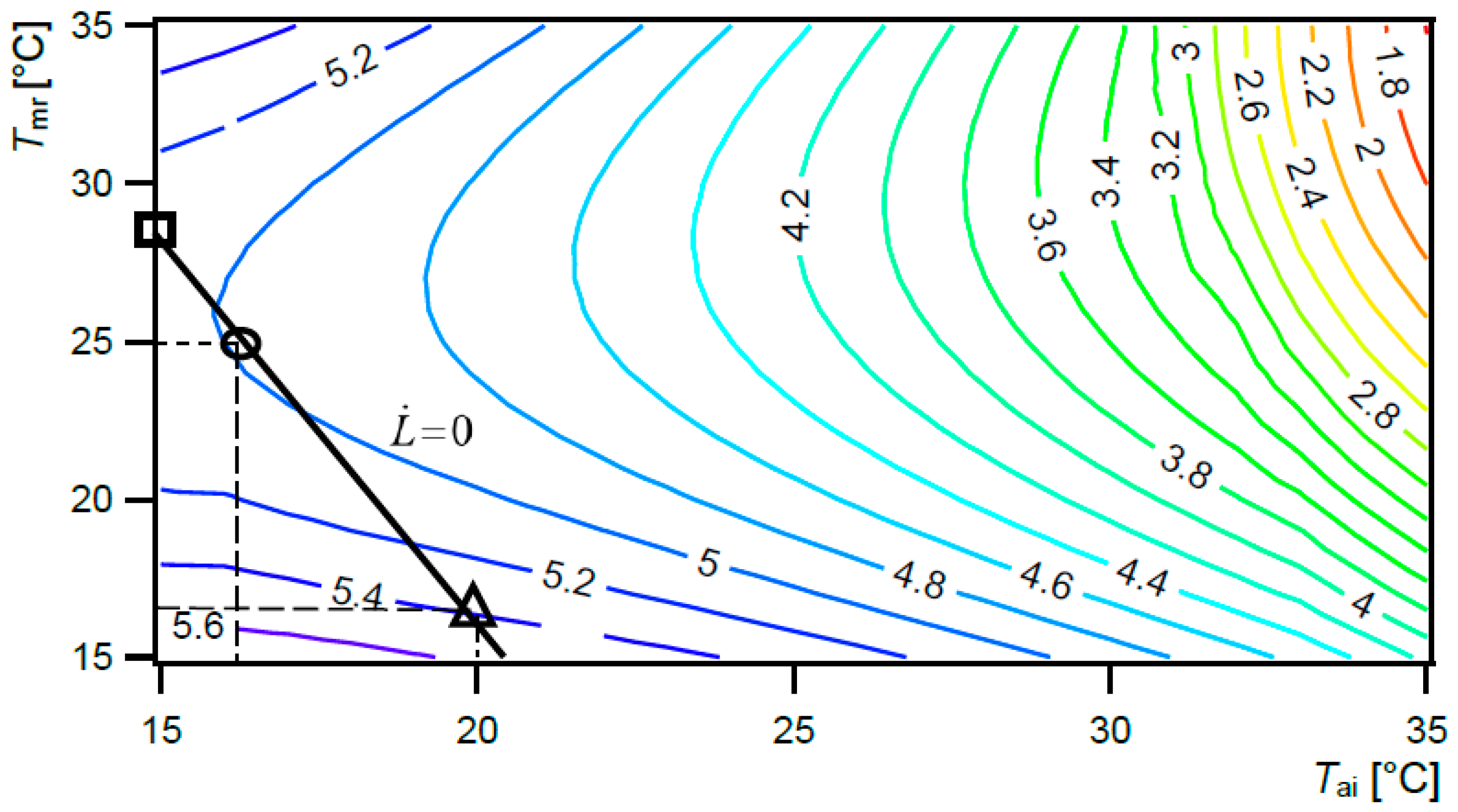
- Requirements for healing and comfort conditions created by UCCPS. Regulations and recommendations for hospital environment define requirements for Tai and RHai that are useful for a room equipped with the conventional system. For the room with the UCCPS, To was introduced and presents together with 80% RHai the required condition (To = 32 °C, RHai = 80%) [35]. To was created as a combination between mean radiant temperature Tmr and Tai.
3.4. Why Is the Creation of the Required Environmental Conditions Important for Burn Patients?
3.5. Has the Selected Type of the Heating and Cooling System Impacted on the Thermodynamic Response of Burn Patients?
3.6. Is It Possible to Actively Regulate Conditions in a Healing Environment by Taking into Consideration the Needs, Demands and Characteristics of Individual Users?
4. Discussion
Strengths and Limitations
5. Conclusions
- Each action towards building energy efficiency has to take into account the complexity of the reciprocal interaction between the treated environment and the user, and it has to be not only directed towards healthy and comfortable conditions, but also towards healing environments supported by energy efficient systems.
- Any deviation of environmental conditions from the required values results in deteriorated patient treatment outcome, uncomfortable conditions and decreased productivity. This is especially important for burn patients, where mortality, morbidity and hospitalization can be significantly decreased with optimal environmental conditions. Therefore, in burn patient rooms every deviation from the required values results in a higher human body exergy consumption rate valid for thermoregulation, besides higher metabolic thermal exergy rate and also higher exergy rates of exhalation and evaporation of sweat, radiation and convection. In order to improve patient treatment outcomes, these conditions have to be prevented.
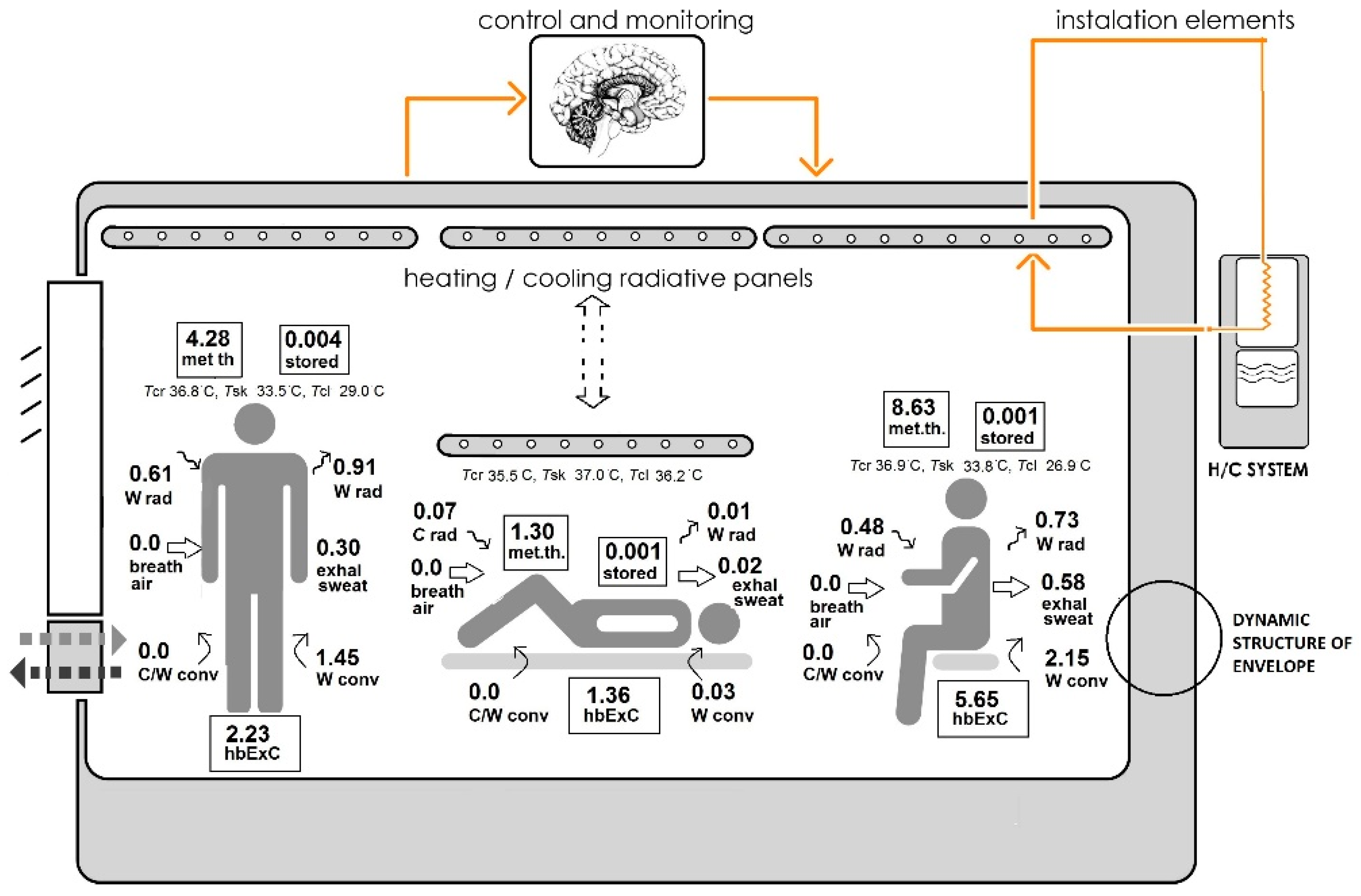
- An innovative user-centred cyber-physical system (UCCPS) in a healing environment enables us to attain optimal thermal balance that may be individually regulated according to the user. Set up system parameters for burn patients result in the lowest possible human body exergy consumption rate valid for thermoregulation, a lower metabolic thermal exergy rate and also lower exergy rates of exhalation and evaporation of sweat, radiation and convection. Set up system parameters for healthcare workers and visitors result in thermally comfortable conditions with minimal hbExC rate and neutral thermal load on their body.
- The thermodynamic response of the human body is influenced not only by the installed heating and cooling system but also by the characteristics of the building envelope. Therefore, it is necessary to create a multi-levelled and dynamic process for the design of a healing environment. A hospital design that includes a dynamic building envelope with efficient systems results not only in improved indoor environmental conditions but also in a significant reduction of energy use.
- Information on this is an aid in the design of any other living and working environment with vulnerable population groups.
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| - | Not detected influential level |
| AC | Air-conditioning |
| breath air | Sum of exergies contained by the inhaled humid air |
| BRI | Building-related illness |
| C | Heat capacity of material |
| C/W conv in/out | Warm/cool convective exergy absorbed by/discharged from the whole skin and clothing surfaces into the surrounding air |
| C/W rad in/out | Warm/cool radiant exergy absorbed by/discharged from the whole skin and clothing surfaces; exhal sweat, exhalation and evaporation of sweat |
| C/W | Cool/warm exergy |
| CH2O | Formaldehyde |
| Clo | Clothing insulation |
| CO2 | Carbon dioxide |
| C | Concentration of CO2 |
| Cheat | Energy use for heating |
| Ccool | Energy use for cooling |
| CS | Circadian stimulus |
| db | Dry bulb |
| DF | Daylight factor |
| DGP | Daylight glare probability |
| Eh | Horizontal illumination |
| Ev | Vertical illumination |
| g | Total solar energy transmittance |
| H | High influential level |
| hbExC | Human body exergy consumption valid for thermoregulation |
| HVAC | Heating, ventilation and air-conditioning systems |
| IEQ | Indoor environmental quality |
| Ilin1 | Internal work plane illumination 1 |
| Ilin2 | Internal work plane illumination 2 |
| Ilout | External illumination |
| Irgo | Direct solar radiation |
| Irdo | Reflected solar radiation |
| L | Low influential level |
| LowEx | Low exergy |
| Rate of thermal load on the body surface area | |
| LAeg | Equivalent continuous sound level |
| Lw | Weighted impact sound pressure level of indoor building elements |
| M | Medium influential level |
| met th | Metabolic thermal exergy, stored, stored exergy in the core and in the shell |
| Met | Metabolic rate |
| MS | Melatonin suppression |
| Pe | Precipitation detection |
| REE | Resting energy expenditure |
| RHai | Relative humidity of indoor air |
| RHao | Relative humidity of outdoor air |
| Rw | Weighted sound reduction index of indoor elements |
| Rw,f | Weighted sound reduction index of facade |
| SHGC | Solar heat gain coefficient |
| Tai | Temperature of indoor air |
| Tao | Temperature of outdoor air |
| TBSA | Percentage of the total body surface area that is affected by a burn |
| TCP | Colour temperature |
| Tcl | Clothing temperature |
| Tcr | Body core temperature |
| Tmedium | Temperature of medium |
| Tmr | Mean radiant temperature |
| To | Operative temperature |
| Trev | Reverberation time |
| Tset up | Set temperature |
| Tsk | Skin temperature |
| Tsurf | Surface temperature |
| SBS | Sick building syndrome |
| UCCPS | User-centred cyber-physical system |
| Unt | Thermal transmittance of non-transparent parts of building envelope |
| Uo | Uniformity ratio |
| Utr | Thermal transmittance of transparent parts of building envelope |
| vai | Indoor air velocity |
| VH | Very high influential level |
| VL | Very influential level |
| VOCs | Volatile organic compounds |
| Wp | Wind speed |
| Wd | Wind direction |
| Xdiff | Material moisture content due to diffusivity |
| η | Phase shift |
| ν | Thermal damping factor |
| τao | Light transmittance |
References
- WHO. Indoor Air Pollutants: Exposure and Health Effects. Euro Reports and Studies, No. 78, WHO Regional Office for Europe; WHO: Copenhagen, Denmark, 1983. [Google Scholar]
- ECA (Commission of the European Communities). European Concerted Action Indoor Air Quality & Its Impact on Man. Cost Project 61 3. Environment and Quality of Life Report No. 4. Sick Building Syndrome. A Practical Guide. Commission of the European Communities. Directorate General for Science. Research and Development. Joint Research Centre—Institute for the Environment; ECA: Luxembourg, 1989; 38p. [Google Scholar]
- WHO. Dampness and Mould; WHO: Copenhagen, Denmark, 2009; p. 248. [Google Scholar]
- Földváry, V.; Bekö, G.; Langer, S.; Arrhenius, K.; Petráš, D. Effect of energy renovation on indoor air quality in multifamily residential buildings in Slovakia. Build. Environ. 2017, 122, 363–372. [Google Scholar] [CrossRef]
- Manuel, J. Avoiding Health Pitfalls of Home Energy-Efficiency Retrofits. Environ. Health Perspect. 2011, 119, A76–A79. [Google Scholar] [CrossRef] [PubMed]
- OG RS (Official Gazette of the Republic of Slovenia). Rules on the Ventilation and Air-Conditioning of Building. OG RS, No 42/02 with Chang; Office of the Government of the RS: Ljubljana, Slovenia, 2002.
- Satish, U.; Mendell, M.J.; Shakhar, K.; Hotchi, T.; Sullivan, D.; Streufert, A.; Fisk, W.J. Is CO2 an indoor pollutant? Direct effects of low-to-moderate CO2 concentrations on human decision-making performance. Environ. Health Perspect. 2012, 120, 1671–1677. [Google Scholar] [CrossRef] [PubMed]
- BPIE (Buildings Performance Institute Europe). Europe’s Buildings Under the Microscope. A Country-By-Country Review of the Energy Performance of Buildings; BPIE: Bruxelles, Belgium, 2011; p. 132. [Google Scholar]
- ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers Inc.). ASHRAE Handbook HVAC Applications: Health Care Facilities; ASHRAE: Atlanta, GA, USA, 2007. [Google Scholar]
- Hey, E.N.; Katz, G. Optimum thermal environment for naked babies. Arch. Dis. Child. 1970, 45, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, R.S.; Zimring, C.; Zhu, X.; DuBose, J.; Seo, H.B.; Choi, Y.S.; Quan, X.; Joseph, A. A review of the research literature on evidence-based healthcare design. HERD 2008, 1, 61–125. [Google Scholar] [CrossRef] [PubMed]
- Dovjak, M.; Kukec, A. Prevention and control of sick building syndrome (SBS). Part 2, Design of a preventive and control strategy to lower the occurrence of SBS. Int. J. Sanit. Eng. Res. 2014, 8, 41–55. [Google Scholar]
- Keyvani, S.; Mohammadyan, M.; Mohamadi, S.; Etemadinezhad, S. Sick Building Syndrome and its Associating Factors at a Hospital in Kashan, Iran. Iran. J. Med. Sci. 2017, 5, 19–24. [Google Scholar] [CrossRef]
- Vafaeenasab, M.R.; Morowatisharifabad, M.A.; Taghi Ghaneian, M.; Hajhosseini, M.; Ehrampoush, M.H. Assessment of sick building syndrome and its associating factors among nurses in the educational hospitals of Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Glob. J. Health Sci. 2014, 16, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Malkin, J. The Business Case for Creating a Healing Environment; Center for Health Design Business Briefing, Hospital Engineering & Facilities Management, Center for Health Design: Concord, CA, USA, 2003; Available online: http://www.capch.org/wp-content/uploads/2012/10/hosp031_r_malkin1.pdf (accessed on 1 August 2018).
- Nightingale, F. Notes on Nursing: What It Is and What It Is Not; Blackie & Son Ltd.: Glasgow/London, UK, 1859; p. 100. [Google Scholar]
- Malkin, J. A Visual Reference for Evidence-Based Design; Center for Health Design: Concord, CA, USA, 2008; 166p. [Google Scholar]
- Stichler, J.F. Creating Healing Environments in Critical Care Units. Crit. Care Nurs. Q. 2001, 24, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Devlin, A.S.; Arneill, A.B. Health care environments and patient outcomes: A review of literature. Environ. Behav. 2003, 35, 665–694. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Quan, X.; Zimring, C.; Joseph, A.; Choudhary, R. The Role of the Physical Environment in the Hospital of 21st Century: A Once-In-A-Lifetime Opportunity; Center for Health Design: Concord, CA, USA, 2004; 69p. [Google Scholar]
- Dijkstra, K. Understanding Healing Environments: Effects of Physical Environmental Stimuli on Patients’ Health and Well-Being; Faculty of Behavioural, Management and Social Sciences: Enschede, The Netherlands, 2009. [Google Scholar]
- Huisman, E.R.C.M.; Morales, E.; van Hoof, J.; Kort, H.S.M. Healing environment: A review of the impact of physical environmental factors on users. Build. Environ. 2012, 58, 70–80. [Google Scholar] [CrossRef]
- Herndon, D.N. Total Burn Care, 1st ed.; Sunders: London, UK, 1996; 597p. [Google Scholar]
- Wilmore, D.W.; Mason, A.D.; Johnson, D.W.; Pruitt, B.A. Effect of ambient temperature on heat production and heat loss in burn patients. J. Appl. Physiol. 1975, 38, 593–597. [Google Scholar] [CrossRef] [PubMed]
- CIP-IEE-PROMO-P. Call for Proposals 2009. Promotion/Dissemination Projects: Save, Altener, Steer and Integrated Initiatives, 2009. Available online: http://ec.europa.eu/cip/iee/index_en.htm (accessed on 1 May 2018).
- Shukuya, M.; Iwamatsu, T.; Asada, H. Development of human-body exergy balance model for a better understanding of thermal comfort in the built environment. Int. J. Exergy 2012, 11, 493–507. [Google Scholar] [CrossRef]
- Shukuya, M.; Saito, M.; Isawa, K.; Iwamatsu, T.; Asada, H. Low-Exergy Systems for High Performance Systems and Communities. In Working Report of IEA ECBS; Annex 49; Human Body Exergy Balance and Thermal Comfort, 2010; Available online: https://www.annex49.com/download/Annex49_HBE.pdf (accessed on 1 August 2018).
- Shukuya, M. Exergy. Theory and Applications in the Built Environment; Springer: London, UK, 2013; 365p. [Google Scholar]
- Dahl, R. Cooling concepts: Alternatives to air conditioning for a warm world. Environ. Health Perspect. 2013, 121, A18–A25. [Google Scholar] [CrossRef] [PubMed]
- Krainer, A. Vernacular Buildings in Slovenia: Genesis of Bioclimatic Growth of Vernacular Buildings in Slovenia; European Commission: London, UK, 1993; 102p. [Google Scholar]
- Krainer, A. Toward Smart Buildings; European Commission: London, UK, 1993; 84p. [Google Scholar]
- Asimow, M. Fundamentals of Engineering Design: Introduction to Design, 1st ed.; Prentice Hall Inc.: New York, NY, USA, 1962; p. 135. [Google Scholar]
- ANSI/ASHRAE/ASHE (American Society of Heating, Refrigerating and Air-Conditioning Engineers Inc.). ANSI/ASHRAE/ASHE Standard 170. Ventilation of Health Care Facilities; ASHRAE: Atlanta, GA, USA, 2008. [Google Scholar]
- ANSI/ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers Inc.). ANSI/ASHRAE Standard 55. Thermal Environmental Conditions for Human Occupancy; ASHRAE: Atlanta, GA, USA, 2004. [Google Scholar]
- Dovjak, M. Individualisation of Personal Space in Hospital Environment. Ph.D. Thesis, University of Nova Gorica, Nova Gorica, Slovenia, 2012. Available online: https://repozitorij.ung.si/IzpisGradiva.php?id=839&lang=eng (accessed on 1 May 2018).
- Ramos, G.E.; Resta, M.; Patińo, O.; Bolgiani, A.N.; Prezzavento, G.; Grillo, R.; Chacón Pazmińo, G.; Benaim, F.; Rutan, R.L. Peri-operative hypothermia in burn patients subjected to non–extensive surgical procedures. Ann. Burns Fire Disasters 2002, 15, 1–6. [Google Scholar]
- Shiozaki, T.; Kishikawa, M.; Hiraide, A.; Shimazu, T.; Sugimoto, H.; Yoshioka, T.; Sugimoto, T. Recovery from post-operative hypothermia predicts survival in extensively burned patients. Am. J. Surg. 1993, 165, 326–330. [Google Scholar] [CrossRef]
- Wilmore, D.W.; Long, J.M.; Mason, A.D.; Skreen, R.W.; Pruitt, B.A. Cateholamines: Mediators of hypermetabolic response to thermal injury. Ann. Surg. 1974, 180, 653–668. [Google Scholar] [CrossRef] [PubMed]
- Fanger, P.O. Thermal Comfort; Danish Technical Press: Copenhagen, Denmark, 1970; 244p. [Google Scholar]
- ISO (International Organization for Standardization). ISO 7730. Ergonomics of the Thermal Environment–Analytical Determination and Interpretation of Thermal Comfort Using Calculation of the Pmv and Ppd Indices and Local Thermal Comfort Criteria; ISO: Geneva, Switzerland, 2005. [Google Scholar]
- ISO (International Organization for Standardization). ISO 8996. 2004. Ergonomics of the Thermal Environment—Determination of Metabolic Rate; ISO: Geneva, Switzerland, 2004. [Google Scholar]
- Martin, C.J.; Ferguson, J.C.; Rayner, C. Environmental conditions for treatment of burned patients by the exposure method. Burns 1992, 18, 273–282. [Google Scholar] [CrossRef]
- Sudoł–Szopińska, I.; Tarnowski, W. Thermal comfort in the operating suite. Borgis New Med. 2007, 2, 40–46. [Google Scholar]
- Corallo, J.; King, B.; Pizano, L.; Namias, N.; Schulman, C. Core warming of a burn patient during excision to prevent hypothermia. Burns 2007, 34, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Herndon, D.N.; Curreri, P.W.; Abston, S.; Rutan, T.C.; Barrow, R.E. Treatment of burns. Curr. Probl. Surg. 1987, 2, 347–397. [Google Scholar] [CrossRef]
- Cope, O.; Nathanson, I.T.; Rourke, G.M.; Wilson, H. Metabolic observations. Ann. Surg. 1953, 19, 191–201. [Google Scholar] [CrossRef]
- LeDuc, P.A.; Reardon, M.J.; Persson, J.L.; Gallagher, S.M.; Dunkin, S.L.; Fuller, D.R.; Lucier, G.E. Aircrew Health and Performance Division August 2002. Heat Stress Evaluation of Air Warrior Block I MOPP0 and MOPP4 Esembles with and without Microclimate Cooling; USSARL Report No.2002-19; U.S. Army Aeromedical Research Laboratory, Department of the Army: Fort Rucker, AL, USA, 2002; 56p, Available online: https://www.dtic.mil/cgi-bin/GetTRDoc?AD=ADA405658&Location=U2&doc=GetTRDoc.pdf (accessed on 1 August 2018).
- Simmers, L. Diversified Health Occupations, 2nd ed.; Delmar Publishers: Albany, NY, USA, 1988. [Google Scholar]
- Sund-Levander, M.; Forsberg, C.; Wahren, L.K. Normal oral, rectal, tympanic and axillary body temperature in adult men and women: A systematic literature review. Scand. J. Caring Sci. 2002, 16, 122–128. [Google Scholar] [CrossRef] [PubMed]
- ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers Inc.). ASHRAE Handbook & Product Directory. 1977 Fundamentals; ASHRAE: Atlanta, GA, USA, 1977. [Google Scholar]
- Skoog, J.; Fransson, N.; Jagemar, L. Thermal environment in Swedish hospitals summer and winter measurements. Energy Build. 2005, 37, 872–877. [Google Scholar] [CrossRef]
- Arturson, G.; Danielsson, U.; Wennberg, L. The effects on the metabolic rate and nutrition of patients with severe burns following treatment with infrared heat. Burns 1978, 5, 164–168. [Google Scholar] [CrossRef]
- Caldwell, F.T. Energy metabolism following thermal burns. Arch. Surg. 1976, 111, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, F.T. Etiology and control of post-burn hypermetabolism. J. Burn Care Rehabil. 1991, 12, 385–401. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, F.T.; Wallace, B.H.; Cone, J.B.; Manuel, L. Control of the hypermetabolic response to burn injury using environmental factors. Ann. Surg. 1992, 215, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Carlson, D.E.; Cioffi, W.G.; Mason, A.D.; McManus, W.F.; Pruitt, B.A. Resting energy expenditure in patients with thermal injuries. Surg. Gynecol. Obstet. 1992, 174, 270–276. [Google Scholar] [PubMed]
- Clark, A.; Imran, J.; Madni, T.; Wolf, S.E. Nutrition and metabolism in burn patients. Burns Trauma 2017, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Cone, J.B.; Wallace, B.H.; Caldwell, F.T. The effect of staged burn wound closure on the rates of heat production and heat loss of burned children and young adults. J. Traum. 1988, 28, 968–972. [Google Scholar] [CrossRef]
- Danielsson, U.; Arturson, G.; Wennberg, L. The elimination of hypermetabolism in burned patients: A method suitable for clinical use. Burns 1976, 2, 110–114. [Google Scholar] [CrossRef]
- Herndon, D.N. Mediators of metabolism. J. Traum. 1981, 21, 701–705. [Google Scholar] [CrossRef]
- Herndon, D.N.; Langner, F.; Thompson, P.; Linares, H.A.; Stein, M.; Traber, D.L. Pulmonary injury in burned patients. Surg. Clin. N. Am. 1987, 67, 31–46. [Google Scholar] [CrossRef]
- Herndon, D.N.; Barrow, R.E.; Linares, H.; Rutan, R.L.; Prien, T.; Traber, L.D.; Traber, D.L. Inhalation injury in burned patients: Effects and treatment. Burns 1988, 14, 349–356. [Google Scholar] [CrossRef]
- Herndon, D.N.; Parks, D.H. Comparison of serial debridement and autografting and early massive excision with cadaver skin overlay in the treatment of large burns. J. Burn Care Rehabil. 1992, 13, 391–395. [Google Scholar] [CrossRef]
- Herndon, D.N.; Tompkins, R.G. Support of the metabolic response to burn injury. Lancet 2004, 363, 1895–1902. [Google Scholar] [CrossRef]
- Kelemen, J.J.; Cioffi, W.G.; Mason, A.D.; Mozingo, D.W.; McManus, W.F.; Pruitt, B.A. Effect of ambient temperature on metabolic rate after thermal injury. Ann. Surg. 1996, 223, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Wallace, B.H.; Caldwell, F.T.; Cone, J.B. The interrelationships between wound management, thermal stress, energy metabolism, and temperature profiles of patients with burns. J. Burn Care Rehabil. 1994, 15, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Zawaski, B.E.; Spitzer, K.W.; Mason, A.D.; Johns, L.A. Does increased evaporative water loss cause hypermetabolism in burned patients? Ann. Surg. 1970, 176, 171–236. [Google Scholar] [CrossRef]
- Mady, C.E.K.; Ferreira, M.S.; Yanagihara, J.I.; Saldiva, P.H.N.; de Oliveira Junior, S. Modeling the exergy behavior of human body. Energy 2012, 45, 546–553. [Google Scholar] [CrossRef]
- Mady, C.E.K.; Ferreira, M.S.; Yanagihara, J.I.; de Oliveira Junior, S. Human body exergy analysis and the assessment of thermal comfort conditions. Int. J. Heat Mass. Trans. 2014, 77, 577–584. [Google Scholar] [CrossRef]
- Ala-Juusela, M.; Shukuya, M. Human body exergy consumption and thermal comfort of an office worker in typical and extreme weather conditions in Finland. Energy Build. 2014, 76, 249–257. [Google Scholar] [CrossRef]
- Wu, X.; Zhao, J.; Olesen, B.W.; Fang, L. A novel human body exergy consumption formula to determine indoor thermal conditions for optimal human performance in office buildings. Energy Build. 2013, 56, 48–55. [Google Scholar] [CrossRef]
- Dovjak, M.; Shukuya, M.; Krainer, A. Connective thinking on building envelope—Human body exergy analysis. Int. J. Heat Mass. Tran. 2015, 90, 1015–1025. [Google Scholar] [CrossRef]
- Buyak, N.A.; Deshko, V.I.; Sukhodub, I.O. Buildings energy use and human thermal comfort according to energy and exergy approach. Energy Build. 2017, 146, 172–181. [Google Scholar] [CrossRef]
- Prek, M.; Butala, V. Comparison between Fanger’s thermal comfort model and human exergy loss. Energy 2017, 138, 228–237. [Google Scholar] [CrossRef]
- Schweiker, M.; Kolarik, J.; Dovjak, M.; Shukuya, M. Unsteady-state human-body exergy consumption rate and its relation to subjective assessment of dynamic thermal environments. Energy Build. 2016, 116, 164–180. [Google Scholar] [CrossRef]
- Mady, C.E.K.; Albuquerque, C.; Fernandes, T.L.; Hernandez, A.J.; Saldiva, P.H.N.; Yanagihara, J.I.; de Oliveira Junior, S. Exergy performance of human body under physical activities. Energy 2013, 62, 370–378. [Google Scholar] [CrossRef]
- Henriques, I.B.; Mady, C.E.K.; de Oliveira Junior, S. Exergy model of the human heart. Energy 2016, 117, 612–619. [Google Scholar] [CrossRef]
- Khodakaram, J.; Nasrollahi, N. Thermal comfort in hospitals—A literature review. Renew. Sustain. Energy Rev. 2012, 16, 4071–4077. [Google Scholar] [CrossRef]
- Henriques, I.B.; Mady, C.E.K.; de Oliveira Junior, S. Assessment of thermal comfort conditions during physical exercise by means of exergy analysis. Energy 2017, 128, 609–617. [Google Scholar] [CrossRef]
- Hudobivnik, B.; Pajek, L.; Kunič, R.; Košir, M. FEM thermal performance analysis of multi-layer external walls during typical summer conditions considering high intensity passive cooling. Appl. Energy 2016, 178, 363–375. [Google Scholar] [CrossRef]
- Pajek, L.; Hudobivnik, B.; Kunič, R.; Košir, M. Improving thermal response of lightweight timber building envelopes during cooling season in three European locations. J. Clean. Prod. 2017, 156, 939–952. [Google Scholar] [CrossRef]
- Kunič, R. Carbon footprint of thermal insulation materials in building envelopes. Energy Effic. 2017, 10, 1511–1528. [Google Scholar] [CrossRef]
- Kunič, R. Forest-based bioproducts used for construction and its impact on the environmental performance of a building in the whole life cycle. In Environmental Impacts of Traditional and Innovative Forest-Based Bioproducts, (Environmental Footprints and Eco-Design of Products and Processes); Kutnar, A., Muthu, S.S., Eds.; Springer Nature: Singapore, 2016; pp. 173–204. [Google Scholar]
- Juan, Y.-K.; Cheng, Y.-C.; Perng, Y.-H.; Castro-Lacouture, D. Optimal Decision Model for Sustainable Hospital Building Renovation—A Case Study of a Vacant School Building Converting into a Community Public Hospital. Int. J. Environ. Res. Public Health 2016, 13, 630. [Google Scholar] [CrossRef] [PubMed]
- Melikov, A.K.; Cermak, R.; Majer, M. Personalized ventilation: Evaluation of different air terminal devices. Energy Build. 2002, 34, 829–836. [Google Scholar] [CrossRef]
- EPBD Proposal. Proposal for a Directive of the European Parliament and of the Council Amending Directive 2010/31/EU on the Energy Performance of Buildings. 2016. Available online: https://ec.europa.eu/energy/sites/ener/files/documents/1_en_act_part1_v10.pdf (accessed on 1 May 2018).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Building and System Components | Parameter | Building Envelope | System | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Transparent | Transparent | Heating/Cooling | Ventilation | Air Conditioning | ||||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |||
| IEQ Issues | Unt [W/(m2K)] | C [kJ/(kgK)] | ν [-] | η [h] | Xdiff [%] | Air Tightness [h−1] | Utr [W/(m2K)]] | g [-] | τao [-] | SHGC [-] | Tmedium [°C] | Tsurf [°C] | Ventilation Rate [m3/h per Person] | RHai [%] | ||
| Thermal Comfort | 1 | Tai [°C] | 1/1 H | 1/2 H | 1/3 H | 1/4 H | 1/5 VL | 1/6 VL | 1/7 H | - | - | 1/10 H | 1/11 H | 1/12 VH | - | 1/14 H |
| 2 | Tmr [°C] | 2/1 VH | 2/2 VH | 2/3VH | 2/4 VH | 2/5 VL | 2/6 VL | 2/7 VH | - | 2/10 VH | 2/11 VH | 2/12 VH | - | 2/14 M | ||
| 3 | To [°C] | 3/1 VH | 3/2 VH | 3/3 VH | 3/4 VH | 3/5 VL | 3/6 VL | 3/7 VH | - | - | 3/10 VH | 3/11 VH | 3/12 VH | - | 3/14 M | |
| 4 | RHai [°C] | 4/1 VL | 4/2 VL | 4/3 VL | 4/4 VL | 4/5 M | 4/6 VL | 4/7 VL | - | - | 4/10nVL | 4/11 H | 4/12 L | - | 4/14 VH | |
| 5 | vai [°C] | 5/1 VL | 5/2 VL | 5/3 VL | 5/4 VL | 5/5 VL | 5/6 H | 5/7 VL | - | - | 5/10 VL | 5/11 VL | 5/12 VL | 5/13 VH | 5/14 VL | |
| 6 | Met [met] | 6/1 VL | 6/2 VL | 6/3 VL | 6/4 VL | 6/5 VL | 6/6 VL | 6/7 VL | - | - | 6/10 VL | 6/11 VL | 6/12 VL | - | 6/14 VL | |
| 7 | Clo [clo] | 7/1 L | 7/2 L | 7/3 VL | 7/4 VL | 7/5 VL | 7/6 VL | 7/7 VL | - | - | 7/10 VL | 7/11 VL | 7/12 M | - | 7/14 M | |
| Indoor Air Quality | 8 | Bioeffluents, Bioaerosols (e.q. CO2) [mg/m3, ppm] | 8/1 VL | 8/2 VL | - | - | 8/5 VL | 8/6 M | 8/7 VL | - | - | 8/10 VL | 8/11 VL | 8/12 VL | 8/13 VH | 8/14 L |
| 9 | Hidden Olfs, Emission from Construction Products (e.g., VOCs, CH2O, phthalate esters) [mg/m3, ppm] | 9/1 VL | 9/2 VL | - | - | 9/5 H | 9/6 M | 9/7 VL | - | - | 9/10 VL | 9/11 M | 9/12 H | 9/13 H | 9/14 H | |
| 10 | Radon [Bq/m3] | 10/1 VL | 10/2 VL | - | - | 10/5 VL | 10/6 VH | 10/7 VL | - | - | 10/10 VL | 10/11 VL | 10/12 VL | 10/13 VH | 10/14 VL | |
| 11 | Bacteria, Moulds, Viruses | 11/1 M | 11/2 M | - | - | 11/5 VH | 11/6 VL | 11/7 M | 11/8 M | 11/9 M | 11/10 M | 11/11 M | 11/12 H | 11/13 VH | 11/14 VH | |
| Visual Comfort and Non-Image Forming Effects | 12 | Eh, Ev [lx] | - | - | - | - | - | 12/7 VH | 12/8 VH | 12/9 VH | 12/10 VH | - | - | - | - | |
| 13 | DF [%] | - | - | - | - | - | - | 13/7 VH | 13/8 VH | 13/9 VH | 13/10 VH | - | - | - | - | |
| 14 | TCP [K] | - | - | - | - | - | - | 14/7 VH | 14/8 VH | 14/9 VH | 14/10 VH | - | - | - | - | |
| 15 | Uo [-] | - | - | - | - | - | - | 15/7 VH | 15/8 VH | 15/9 VH | 15/10 VH | - | - | - | - | |
| 16 | DGP [-] | - | - | - | - | - | - | 16/7 VH | 16/8 VH | 16/9 VH | 16/10 VH | - | - | - | - | |
| 17 | Wavelength, Time Availability, Spatial Distribution, CS, MS | - | - | - | - | - | - | 17/7 VH | 17/8 VH | 17/9 VH | 17/10 VH | - | - | - | - | |
| Room Acoustic Noise, Vibrations | 18 | LAeg [dB(A)] | 18/1 H | 18/2 H | - | - | - | 18/6 L | 18/7 H | - | - | - | - | - | 18/13 H | 18/14 H |
| 19 | Rw,f [dB(A]] | 19/1 H | 19/2 H | - | - | - | 19/6 L | 19/7 H | - | - | - | - | - | - | - | |
| 20 | Lw [dB(A]] | 20/1 H | 20/2 H | - | - | - | 20/6 L | 20/7 H | - | - | - | - | - | - | - | |
| 21 | Rw [dB(A]] | 21/1 H | 21/2 H | - | - | - | 21/6 L | 21/7 H | - | - | - | - | - | - | - | |
| 22 | Trev [s] | 22/1 VL | 22/2 VL | - | - | - | 22/6 VL | 22/7 VL | - | - | - | - | - | - | - | |
| Ergonomics and Universal Design | 23 | Dimension, Location, Dynamic, Static Aspects | 23/1 H | 23/2 H | - | - | - | 23/6 VL | 23/7 M | 23/8 M | 23/9 M | 23/10 M | 23/11 M | 23/12 H | 23/13 H | 23/14 H |
| Parameter | Burn Patient | Visitor, Healthcare Worker |
|---|---|---|
| Individual Characteristics | ||
| Tsk | “…the body tries to raise the skin and core temperature by 2 °C secondary to a hypothalamic reset…” [23] (p. 422) “…burn patient strives for temperatures of about 38 °C…” [23] (p. 492) | “…after 3 h in a hot room (50 °C), skin temperature differentials amounted to only 2.5 °C (= 35 °C–37.5 °C), with an average core/surface gradient of ~1 °C. With normal clothing in a room at 15–20 °C, mean skin temperature is 32–5 °C…” [36] |
| Tcr | “…in patients their core body temperature declines below 35.5 °C…” [37] “…in the general surgical population, approximately one half of patients in routine peri-operative thermal care develop a core body temperature of less than 36 °C during the peri-operative period, and a further one-third exhibit core temperatures of less than 35 °C…” [38] “…burn patients are by far the most susceptible to intra– and post–operative hypothermia, since the damaged skin is no longer able to prevent the loss of body heat…” [38] “…core temperature is generally expected to be 0.5 °C higher than body surface temperatures…” [23] (p. 530) “…in normal individuals the threshold range is generally near 36.5 °C–37.5 °C.” “In patient the threshold set point is higher and the increase is proportional to the size of the burn, 0.003 °C/% total body size area regarding the size of the burns…” [23] (p. 205) “… hypothermia of less than 35 °C occurs in 89% of the total operations performed in extensively burned patients…” [39] “…hypothermia is a particular hazard in children, with their relatively larger surface area, and in all patients with extensive burns [23] (p. 94) | “… the normal range for body temperature is 36.1–37.8 °C …” [40,41] |
| Metabolic Rate | “…numerous recent reports using indirect calorimetry document metabolic rates, which are 120–150% of normal [42] (p. 399) “…increased metabolic rate takes place after thermal injury. Within the range of 70–80% of TBSA burn injury the hypermetabolism tends to be proportional to the size of burn wound…” [23] (p. 205) “…using indirect calorimetry in acute patient with major burn injuries that are treated according to current standards, resting energy expenditures 110–150% above predicted values are frequently measured…” [23] (p. 205) “REE in adults might be 200–300% greater than predicted basal values” [42] | “standing relaxed 1 met, standing under stress 2 met” [43,44,45,46,47] |
| Metabolism | “Metabolic rate is increased after burn injury up to about 150% of normal levels when burn size is greater than 20–30% TBSA” [42] “The increase in metabolic rate approaches twice the normal” [48] “…metabolic rate was increased by a factor of 1.5 times basal metabolic rate…” [49] “…measured energy expenditure reached 2.7 ± 0.9 times the basal energy expenditure in extensively burned patients with hypothermia of less than 35 °C…” [39] | |
| Effective Clothing Insulation | “…naked 0 clo…” [43] “…artificial skin on very large burns covered over 80% of TBSA…” [23] (p. 6) | “… the insulation of different sets varies within the range of 0.54 ± 0.01 clo to 0.95 ± 0.01 clo…” [44,45,46,47], [50] (pp. 40–46) |
| Required/Recommended Indoor Environmental Conditions | ||
| Tai RHai | “…ambient temperature and humidity should be maintained at 30–33 °C and 80%, respectively, in order to decrease energy demands and evaporative heat losses…” [23] (p. 492) “…the hypermetabolic response may be reduced by warming the ambient temperature to thermal neutrality (33 °C), at which point the heat for evaporation is derived from the environment, taking the burden away from the patient…” [23] (p. 425) “… patients need a hot environment and high relative humidity. A ward for severe burn victims should have temperature controls that permit adjusting the room temperature up to 32 °C db and relative humidity up to 95%…” [9] “Patients can be treated at ambient temperatures of 32–35 °C in the intensive care room with a specially designed airflow system…” [51] | ANSI/ASHRAE Standard 55 [34] recommends that the relative humidity in occupied spaces is controlled in the ranges from 30% up to 60% and at air temperatures between 20 °C and 25 °C. |
| Tset up | Input Exergy Rates [W/m2] | Stored [W/m2] | Output Exergy Rates [W/m2] | HbExC Rate [W/m2] | |||||
|---|---|---|---|---|---|---|---|---|---|
| Met th | C/W Rad | C/W Conv | Breath Air | C/W Rad | C/W Conv | Exhal Sweat | |||
| Conventional System | |||||||||
| Tai = 32 °C Tmr = 32 °C | 2.29 | C = 0 W = 0 | 0 | 0 | 0.006 | C = 0 W = 0.12 | C = 0 W = 0.32 | 0.05 | 1.79 |
| UCCPS | |||||||||
| Tai = 35 °C Tmr = 31 °C | 1.30 | C = 0.07 W = 0 | 0 | 0 | 0.001 | C = 0 W = 0.01 | C = 0 W = 0.03 | 0.02 | 1.36 |
| Tset up | Input Exergy Rates [W/m2] | Stored [W/m2] | Output Exergy Rates [W/m2] | HbExC Rate [W/m2] | |||||
|---|---|---|---|---|---|---|---|---|---|
| Met th | C/W Rad | C/W Conv | Breath Air | C/W Rad | C/W Conv | Exhal Sweat | |||
| UCCPS | |||||||||
| Tai = 35 °C Tmr = 31 °C | 1.30 | C = 0.07 W = 0 | 0 | 0 | 0.001 | C = 0 W = 0.01 | C = 0 W = 0.03 | 0.02 | 1.36 |
| Tai = 31 °C Tmr = 33 °C | 2.66 | C = 0 W = 0.03 | 0 | 0 | 0.007 | C = 0 W = 0.19 | C = 0 W = 0.50 | 0.06 | 1.93 |
| Tai = 26 °C Tmr = 35 °C | 4.36 | C = 0 W = 0.64 | 0 | 0 | 0.006 | C = 0 W = 0.67 | C = 0 W = 1.80 | 0.16 | 2.37 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dovjak, M.; Shukuya, M.; Krainer, A. User-Centred Healing-Oriented Conditions in the Design of Hospital Environments. Int. J. Environ. Res. Public Health 2018, 15, 2140. https://doi.org/10.3390/ijerph15102140
Dovjak M, Shukuya M, Krainer A. User-Centred Healing-Oriented Conditions in the Design of Hospital Environments. International Journal of Environmental Research and Public Health. 2018; 15(10):2140. https://doi.org/10.3390/ijerph15102140
Chicago/Turabian StyleDovjak, Mateja, Masanori Shukuya, and Aleš Krainer. 2018. "User-Centred Healing-Oriented Conditions in the Design of Hospital Environments" International Journal of Environmental Research and Public Health 15, no. 10: 2140. https://doi.org/10.3390/ijerph15102140
APA StyleDovjak, M., Shukuya, M., & Krainer, A. (2018). User-Centred Healing-Oriented Conditions in the Design of Hospital Environments. International Journal of Environmental Research and Public Health, 15(10), 2140. https://doi.org/10.3390/ijerph15102140