Differences in the Incidence of Symptomatic Cervical and Lumbar Disc Herniation According to Age, Sex and National Health Insurance Eligibility: A Pilot Study on the Disease’s Association with Work



Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Methods
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
3.1. Mean Number of Subscribers by Gender, Age, and National Health Insurance Eligibilty
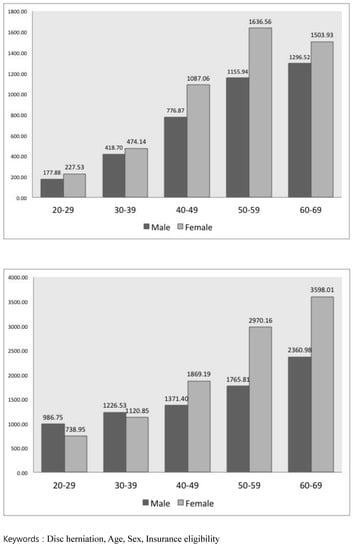
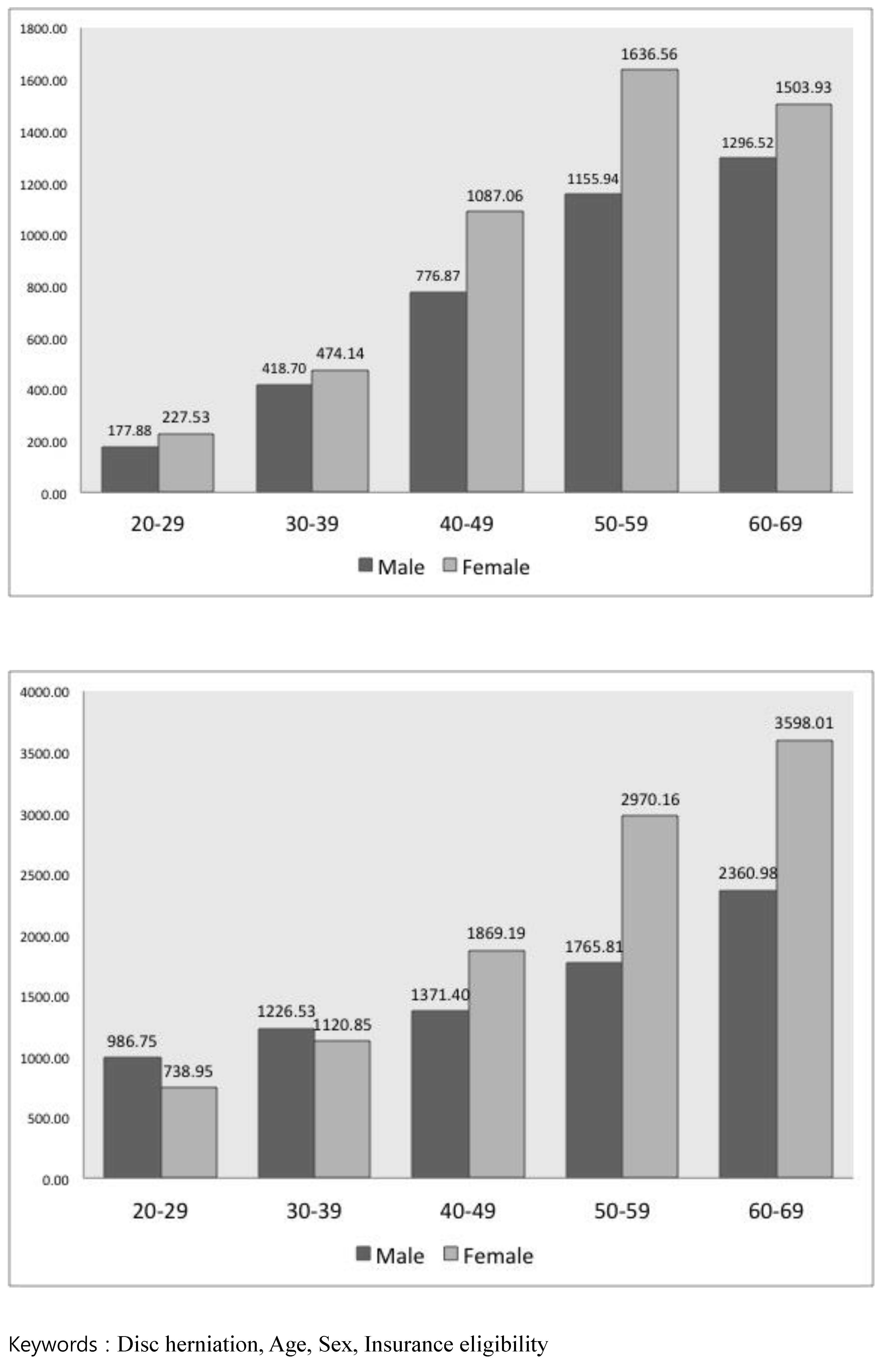
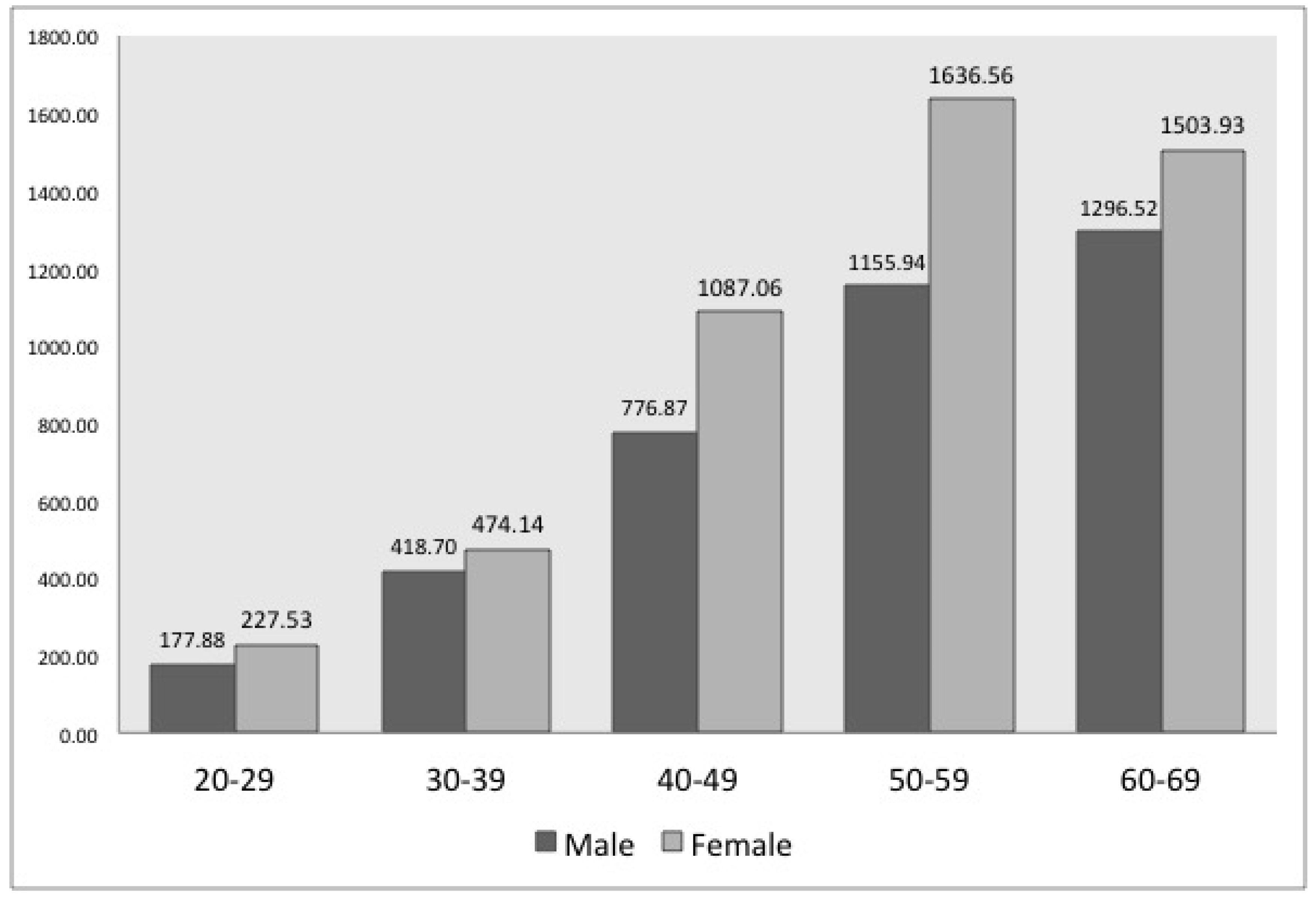
3.2. Number of Examinees with CDH According to Gender, Age and Health Insurance Eligibility
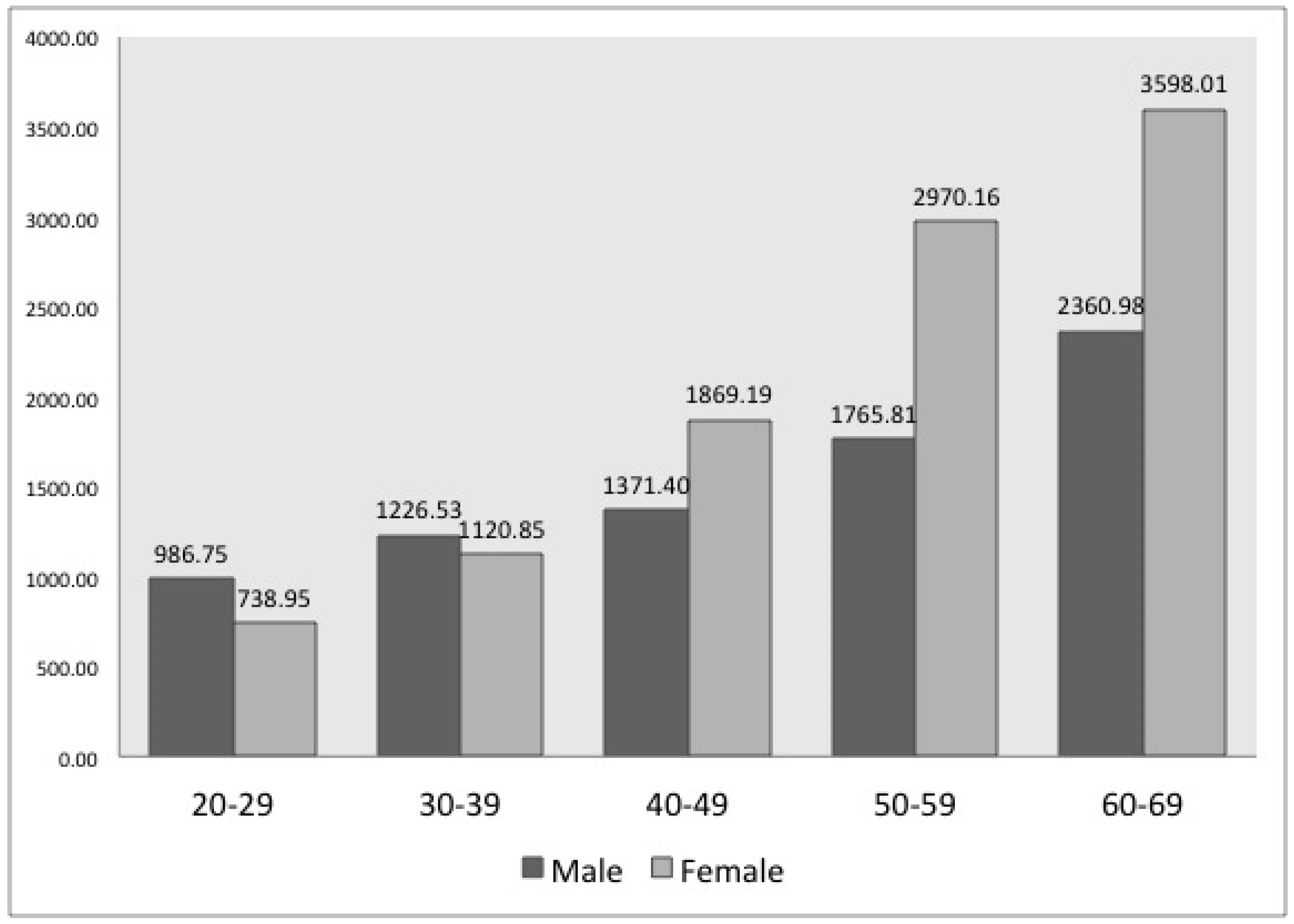
3.3. Number of Patients with LDH According to Gender, Age, and Health Insurance Eligibility
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jordon, J.; Konstantinou, K.; O’Dowd, J. Herniated lumbar disc. BMJ Clin. Evid. 2009, 209, 1118. [Google Scholar]
- Deyo, R.A.; Tsui-Wu, Y.J. Descriptive epidemiology of low-back pain and its related medical care in the United States. Spine 1987, 12, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Saicheua, P. Occupational lumbar disc herniation among Thai workers claimed for compensation. J. Med. Assoc. Thail. 2001, 8, 253–257. [Google Scholar]
- Radhakrishnan, K.; Kitchy, W.J.; O’Fallon, M.; Kurland, L.T. Epidemiology of cervical radiculopathy: A population-based study from Rochester, Minnesota, 1976 through 1990. Brain 1994, 117, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.W.; Lee, J.E.; Lee, S.H.; Kwon, H.K. Kinematic analysis of the lumbar spine by digital videofluoroscopy in 18 asymptomatic subjects and 9 patients with herniated nucleus pulposus. J. Manip. Physiol. Ther. 2011, 34, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Boden, S.D.; McCowin, P.R.; Davis, D.O.; Dina, T.S.; Mark, A.S.; Wiesel, S. Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects. A prospective investigation. J. Bone Jt. Surg. Am. 1990, 72, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Al-Ryalat, N.T.; Saleh, S.A.; Mahafza, W.S.; Samara, O.A.; Ryalat, A.T.; Al-Hadidy, A.M. Myelopathy associated with age-related cervical disc herniation: A retrospective review of magnetic resonance images. Ann. Saudi Med. 2017, 37, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Huang, C.C.; Hsu, C.C.; Lin, H.J.; Guo, H.R.; Su, S.B.; Wang, J.J.; Weng, S.F. Higher risk for cervical herniated intervertebral disc in physicians: A retrospective nationwide population-based cohort study with claims analysis. Medicine (Baltimore) 2016, 95, e5055. [Google Scholar] [CrossRef] [PubMed]
- Lan, F.Y.; Liou, Y.W.; Huang, K.Y.; Guo, H.R.; Wang, J.D. An investigation of a cluster of cervical herniated discs among container truck drivers with occupational exposure to whole-body vibration. J. Occup. Health 2016, 58, 118–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzeng, Y.S.; Chen, S.G.; Chen, T.M. Herniation of the cervical disc in plastic surgeons. Ann. Plast. Surg. 2012, 69, 672–674. [Google Scholar] [CrossRef] [PubMed]
- Shi, N.N.; Shen, G.Q.; He, S.Y.; Guo, R.B. Epidemiology investigation and biomechanics analyses for the correlation between sacroiliac joint disorder and lumbar intervertebral disc degeneration. Zhongguo Gu Shang 2014, 27, 560–564. (In Chinese) [Google Scholar] [PubMed]
- Zhang, Y.G.; Sun, Z.; Zhang, Z.; Liu, J.; Guo, X. Risk factors for lumbar intervertebral disc herniation in Chinese population: A case-control study. Spine 2009, 34, e918–e922. [Google Scholar] [CrossRef] [PubMed]
- Leino-Arjas, P.; Kalla-Kangas, L.; Kauppinen, T.; Notkola, V.; Keskmaki, I.; Mutanen, P. Occupational exposures and inpatient hospital care for lumbar intervertebral disc disorders among Finns. Am. J. Ind. Med. 2004, 46, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Zitting, P.; Rantakallio, P.; Vanharanta, H. Cumulative incidence of lumbar disc diseases leading to hospitalization up to the age of 28 years. Spine 1998, 23, 2337–2343. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S.G.; de la Torre-Diez, I.; Rodrigues, J.J.P.C.; Hamrioui, S.; Lopez-Coronado, M. A systematic review of techniques and sources of big data in the healthcare sector. J. Med. Syst. 2017, 41, 183. [Google Scholar] [CrossRef] [PubMed]
- Zigouris, A.; Batistatou, A.; Alexiou, G.A.; Pachatouridis, D.; Mihos, E.; Drosos, D.; Fotakopoulos, G.; Doukas, M.; Voulgaris, S.; Kyritsis, A.P. Correlation of matrix metalloproteinases-1 and -3 with patient age and grade of lumbar disc herniation. J. Neurosurg. Spine 2011, 14, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Matveeva, N.; Zivadinovik, J.; Zdravkovska, M.; Jovevska, S.; Bojadzieva, B. Histological composition of lumbar disc herniation related to the type of herniation and to the age. Bratisl. Lek. Listy. 2012, 113, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Dammers, R.; Koehler, P.J. Lumbar disc herniation: Level increases with age. Surg. Neurol. 2002, 58, 209–212. [Google Scholar] [CrossRef]
- Ma, D.; Liang, Y.; Wang, D.; Liu, Z.; Zhang, W.; Ma, T.; Zhang, L.; Lu, X.; Cai, Z. Trend of the incidence of lumbar disc herniation: Decreasing with aging in the elderly. Clin. Interv. Aging 2013, 8, 1047–1050. [Google Scholar] [PubMed]
- Slipped Disk: Overview. Available online: https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072656/ (accessed on 1 June 2018).
- Hasvik, E.; Iordanova, S.E.; Grøvle, L.; Julsrud, H.A.; Røe, C.; Gjerstad, J. Subjective health complaints in patients with lumbar radicular pain and disc herniation are associated with a sex—OPRM1 A118G polymorphism interaction: A prospective 1-year observational study. BMC Musculoskelet. Disord. 2014, 15, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidler, A.; Bergmann, A.; Jager, M.; Ellegast, R.; Ditchen, D.; Elsner, G.; Grifka, J.; Haerting, J.; Hofmann, F.; Linhardt, O.; et al. Cumulative occupational lumbar load and lumbar disc disease—Results of a German multicenter case-control study (EPILIFT). BMC Musculoskelet. Disord. 2009, 10, 48. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, M.K.; Matin, T.; Ali, M.Y.; Ali, M.I.; Awwai, M.A.; Sakeb, N. Relationship between physical work load and lumbar disc herniation. Mymensingh Med. J. 2013, 22, 533–540. [Google Scholar] [PubMed]
- Petit, A.; Roquelaure, Y. Low back pain, intervertebral disc and occupational diseases. Int. J. Occup. Saf. Ergon. 2015, 21, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Gender | Age | Region | Company | Government Office and Private School | Medical Care | p-Value * |
|---|---|---|---|---|---|---|
| Male | 20–29 | 281,506 | 1,169,017 | 136,223 | 20,221 | <0.001 |
| 30–39 | 1,135,868 | 2,287,096 | 285,904 | 42,423 | ||
| 40–49 | 1,759,028 | 1,710,430 | 321,634 | 120,896 | ||
| 50–59 | 1,142,273 | 881,303 | 213,928 | 103,216 | ||
| 60–69 | 570,752 | 342,511 | 18,992 | 78,225 | ||
| Female | 20–29 | 213,898 | 1,178,690 | 150,430 | 145,31 | <0.001 |
| 30–39 | 485,794 | 923,692 | 211,537 | 55,115 | ||
| 40–49 | 661,224 | 695,133 | 146,633 | 99,192 | ||
| 50–59 | 411,267 | 332,118 | 51,620 | 67,926 | ||
| 60–69 | 268,635 | 91,770 | 3988 | 101,613 |
| Gender | Age | Region | Company | Government Office and Private School | Medical Care | p-Value |
|---|---|---|---|---|---|---|
| Male | 20–29 | 187.87 | 229.29 | 205.34 | 186.51 | |
| 30–39 | 351.90 | 466.49 | 449.85 | 465.38 | ||
| 40–49 | 659.89 | 882.93 | 828.85 | 889.43 | ||
| 50–59 | 1023.90 | 1288.37 | 1187.45 | 1153.89 | ||
| 60–69 | 1227.78 | 1438.70 | 1812.04 | 1137.38 | ||
| Total | 3451.34 | 4305.78 | 4483.53 | 3852.59 | <0.001 * | |
| Female | 20–29 | 224.07 | 55.00 | 222.69 | 291.99 | |
| 30–39 | 492.10 | 534.39 | 428.16 | 739.23 | ||
| 40–49 | 1040.88 | 1179.16 | 994.90 | 1527.05 | ||
| 50–59 | 1522.20 | 1838.00 | 1548.13 | 1871.57 | ||
| 60–69 | 1422.27 | 1679.67 | 2460.95 | 1405.89 | ||
| Total | 4701.52 | 5286.22 | 5654.83 | 5835.73 | <0.001 * |
| Gender | Age | Region | Company | Government Office and Private School | Medical Care | p-Value |
|---|---|---|---|---|---|---|
| Male | 20–29 | 877.42 | 1179.71 | 1059.08 | 965.76 | |
| 30–39 | 1061.13 | 1325.50 | 1156.03 | 1433.18 | ||
| 40–49 | 1216.15 | 1465.05 | 1276.52 | 1959.42 | ||
| 50–59 | 1566.40 | 1815.45 | 1621.91 | 2321.48 | ||
| 60–69 | 2194.27 | 2374.11 | 2927.55 | 2374.65 | ||
| Total | 6915.37 | 8159.82 | 8041.09 | 9054.49 | <0.001 * | |
| Female | 20–29 | 716.90 | 868.97 | 698.85 | 1023.43 | |
| 30–39 | 1125.99 | 1151.90 | 924.05 | 1784.32 | ||
| 40–49 | 1780.81 | 1932.13 | 1296.16 | 2819.21 | ||
| 50–59 | 2640.41 | 3225.92 | 2037.97 | 3618.64 | ||
| 60–69 | 3472.58 | 3876.77 | 4323.69 | 3451.75 | ||
| Total | 9736.69 | 11055.69 | 9280.72 | 12697.35 | <0.001 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-K.; Kang, D.; Lee, I.; Kim, S.-Y. Differences in the Incidence of Symptomatic Cervical and Lumbar Disc Herniation According to Age, Sex and National Health Insurance Eligibility: A Pilot Study on the Disease’s Association with Work. Int. J. Environ. Res. Public Health 2018, 15, 2094. https://doi.org/10.3390/ijerph15102094
Kim Y-K, Kang D, Lee I, Kim S-Y. Differences in the Incidence of Symptomatic Cervical and Lumbar Disc Herniation According to Age, Sex and National Health Insurance Eligibility: A Pilot Study on the Disease’s Association with Work. International Journal of Environmental Research and Public Health. 2018; 15(10):2094. https://doi.org/10.3390/ijerph15102094
Chicago/Turabian StyleKim, Young-Ki, Dongmug Kang, Ilho Lee, and Se-Yeong Kim. 2018. "Differences in the Incidence of Symptomatic Cervical and Lumbar Disc Herniation According to Age, Sex and National Health Insurance Eligibility: A Pilot Study on the Disease’s Association with Work" International Journal of Environmental Research and Public Health 15, no. 10: 2094. https://doi.org/10.3390/ijerph15102094