Perfluorooctanoic Acid (PFOA) Exposure in Early Life Increases Risk of Childhood Adiposity: A Meta-Analysis of Prospective Cohort Studies

Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis and Heterogeneity
3. Results
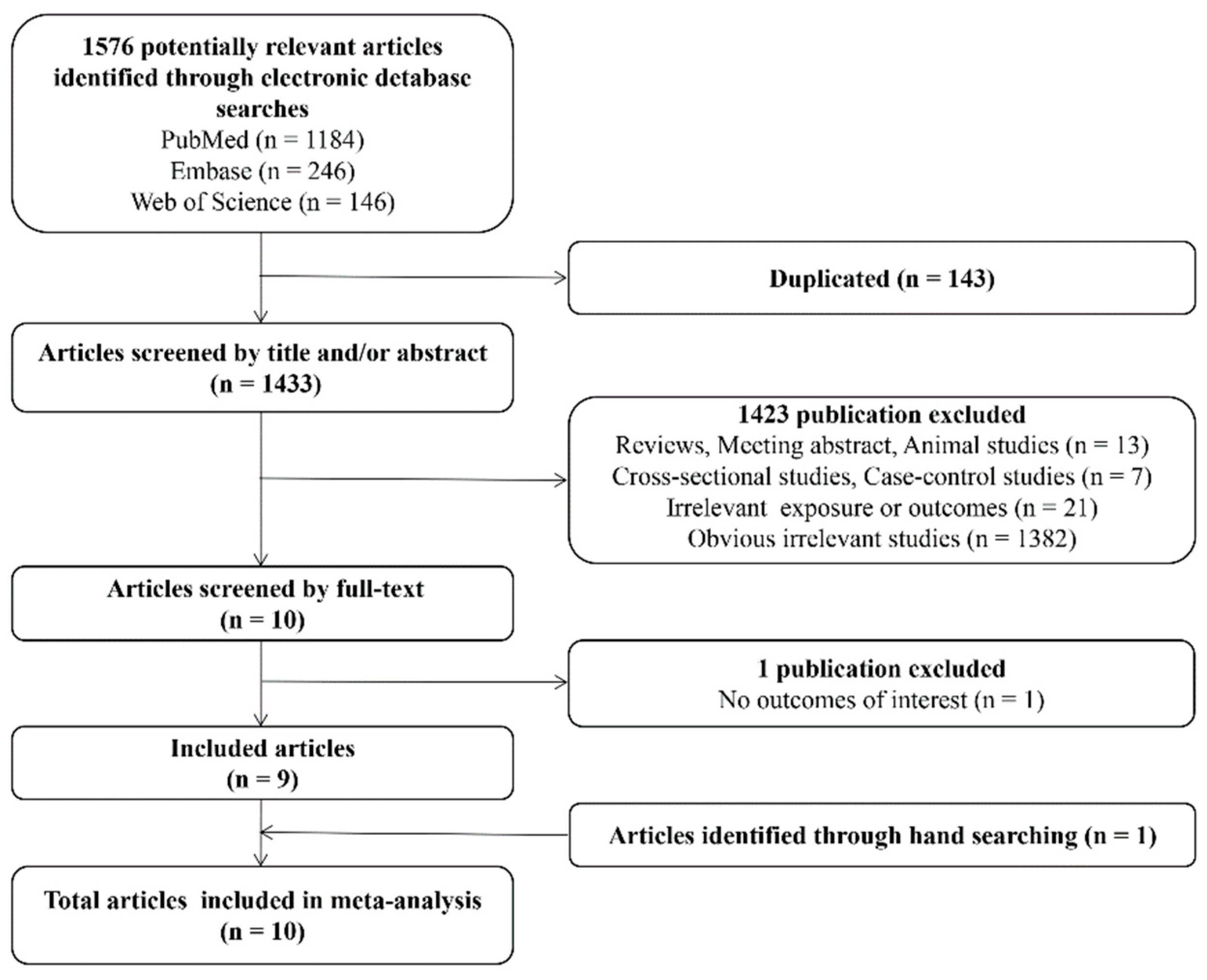
3.1. Study Selection Flow
3.2. Details of Included Studies
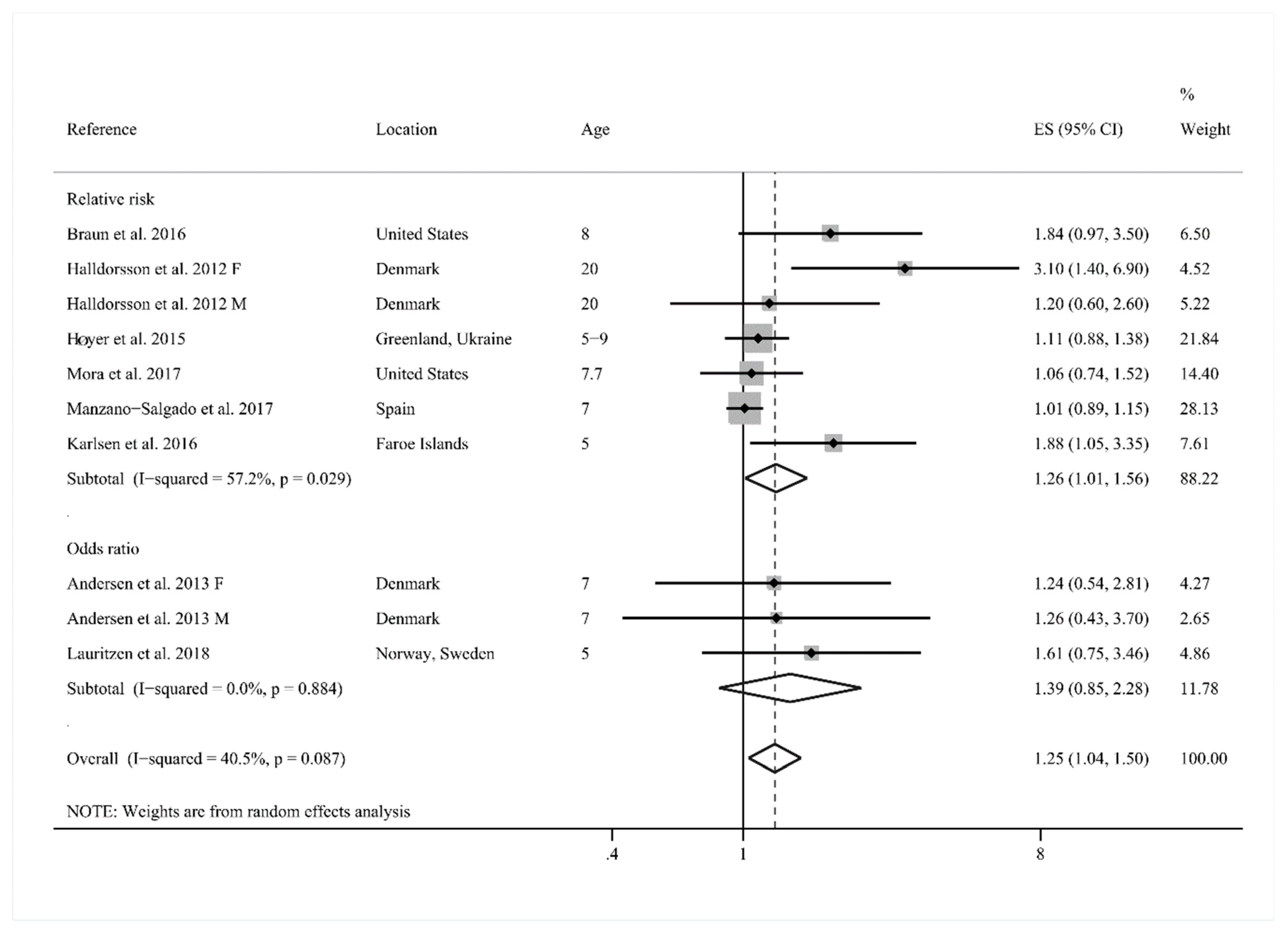
3.3. Meta-Analysis of PFOA Exposure in Early Life in Relation to Childhood Overweight
3.4. Meta-Analysis of PFOA Exposure in Early Life in Relation to Childhood BMI
3.5. Sensitivity Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Fact Sheet: Obesity and Overweight. Available online: http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 17 July 2018).
- Shao, X.; Ding, X.; Wang, B.; Li, L.; An, X.; Yao, Q.; Song, R.; Zhang, J.A. Antibiotic exposure in early life increases risk of childhood obesity: A systematic review and meta-analysis. Front. Endocrinol. (Lausanne) 2017, 8, 170. [Google Scholar] [CrossRef] [PubMed]
- Pringle, K.G.; Lee, Y.Q.; Weatherall, L.; Keogh, L.; Diehm, C.; Roberts, C.T.; Eades, S.; Brown, A.; Smith, R.; Lumbers, E.R.; et al. Influence of maternal adiposity, preterm birth and birth weight centiles on early childhood obesity in an Indigenous Australian pregnancy-through-to-early-childhood cohort study. J. Dev. Orig. Health Dis. 2018, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wassenaar, P.N.H.; Trasande, L.; Legler, J. Systematic review and meta-analysis of early-life exposure to bisphenol A and obesity-related outcomes in rodents. Environ. Health Perspect. 2017, 125, 106001. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.M.; Wong, L.Y.; Kuklenyik, Z.; Reidy, J.A.; Needham, L.L. Polyfluoroalkyl chemicals in the U.S. population: Data from the National Health and Nutrition Examination Survey (NHANES) 2003–2004 and comparisons with NHANES 1999–2000. Environ. Health Perspect. 2007, 115, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Maisonet, M.; Terrell, M.L.; McGeehin, M.A.; Christensen, K.Y.; Holmes, A.; Calafat, A.M.; Marcus, M. Maternal concentrations of polyfluoroalkyl compounds during pregnancy and fetal and postnatal growth in British girls. Environ. Health Perspect. 2012, 120, 1432–1437. [Google Scholar] [CrossRef] [PubMed]
- VanNoy, B.N.; Lam, J.; Zota, A.R. Breastfeeding as a predictor of serum concentrations of per- and polyfluorinated alkyl substances in reproductive-aged women and young children: A rapid systematic review. Curr. Environ. Health Rep. 2018, 5, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Woods, M.M.; Lanphear, B.P.; Braun, J.M.; McCandless, L.C. Gestational exposure to endocrine disrupting chemicals in relation to infant birth weight: A Bayesian analysis of the HOME Study. Environ. Health 2017, 16, 115. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, M.; Grandjean, P.; Weihe, P.; Steuerwald, U.; Oulhote, Y.; Valvi, D. Early-life exposures to persistent organic pollutants in relation to overweight in preschool children. Reprod. Toxicol. 2016, 68, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Wang, P.; Meng, J.; Liu, J.; Lu, Y.; Khim, J.S.; Giesy, J.P. A review of sources, multimedia distribution and health risks of perfluoroalkyl acids (PFAAs) in China. Chemosphere 2015, 129, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Houde, M.; De Silva, A.O.; Muir, D.C.; Letcher, R.J. Monitoring of perfluorinated compounds in aquatic biota: An updated review. Environ. Sci. Technol. 2011, 45, 7962–7973. [Google Scholar] [CrossRef] [PubMed]
- Olsen, G.W.; Burris, J.M.; Ehresman, D.J.; Froehlich, J.W.; Seacat, A.M.; Butenhoff, J.L.; Zobel, L.R. Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ. Health Perspect. 2007, 115, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.; Anitole, K.; Hodes, C.; Lai, D.; Pfahles-Hutchens, A.; Seed, J. Perfluoroalkyl acids: A review of monitoring and toxicological findings. Toxicol. Sci. 2007, 99, 366–394. [Google Scholar] [CrossRef] [PubMed]
- McKee, R.H.; Calafat, A.M. The applicability of biomonitoring data for perfluorooctanesulfonate (PFOS) to the environmental public health continuum. Environ. Health Perspect. 2006, 114, 1776–1782. [Google Scholar] [CrossRef]
- Li, Y.; Oliver, D.P.; Kookana, R.S. A critical analysis of published data to discern the role of soil and sediment properties in determining sorption of per and polyfluoroalkyl substances (PFASs). Sci. Total Environ. 2018, 628–629, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Barry, V.; Darrow, L.A.; Klein, M.; Winquist, A.; Steenland, K. Early life perfluorooctanoic acid (PFOA) exposure and overweight and obesity risk in adulthood in a community with elevated exposure. Environ. Res. 2014, 132, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Strynar, M.; Dagnino, S.; Mcmahen, R.; Liang, S.; Lindstrom, A.; Andersen, E.; Mcmillan, L.; Thurman, M.; Ferrer, I.; Ball, C. Identification of novel perfluoroalkyl ether carboxylic acids (PFECAs) and sulfonic acids (PFESAs) in natural waters using accurate mass time-of-flight mass spectrometry (TOFMS). Environ. Sci. Technol. 2015, 49, 11622–11630. [Google Scholar] [CrossRef] [PubMed]
- Mora, A.M.; Oken, E.; Rifas-Shiman, S.L.; Webster, T.F.; Gillman, M.W.; Calafat, A.M.; Ye, X.; Sagiv, S.K. Prenatal exposure to perfluoroalkyl substances and adiposity in early and mid-childhood. Environ. Health Perspect. 2017, 125, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Salgado, C.B.; Casas, M.; Lopez-Espinosa, M.J.; Ballester, F.; Iñiguez, C.; Martinez, D.; Romaguera, D.; Fernández-Barrés, S.; Santa-Marina, L.; Basterretxea, M.; et al. Prenatal exposure to perfluoroalkyl substances and cardiometabolic risk in children from the Spanish INMA birth cohort study. Environ. Health Perspect. 2017, 125, 097018. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 April 2018).
- Cano-Sancho, G.; Salmon, A.G.; La Merrill, M.A. Association between exposure to p,p’-DDT and its metabolite p,p’-DDE with obesity: Integrated systematic review and meta-analysis. Environ. Health Perspect. 2017, 125, 096002. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Adgent, M.; Su, P.H.; Chen, H.Y.; Chen, P.C.; Hsiung, C.A.; Wang, S.L. Prenatal exposure to perfluorocarboxylic acids (PFCAs) and fetal and postnatal growth in the Taiwan maternal and infant cohort study. Environ. Health Perspect. 2016, 124, 1794–1800. [Google Scholar] [CrossRef] [PubMed]
- Halldorsson, T.I.; Rytter, D.; Haug, L.S.; Bech, B.H.; Danielsen, I.; Becher, G.; Henriksen, T.B.; Olsen, S.F. Prenatal exposure to perfluorooctanoate and risk of overweight at 20 years of age: A prospective cohort study. Environ. Health Perspect. 2012, 120, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Gyllenhammar, I.; Diderholm, B.; Gustafsson, J.; Berger, U.; Ridefelt, P.; Benskin, J.P.; Lignell, S.; Lampa, E.; Glynn, A. Perfluoroalkyl acid levels in first-time mothers in relation to offspring weight gain and growth. Environ. Int. 2018, 111, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Chen, A.; Romano, M.E.; Calafat, A.M.; Webster, G.M.; Yolton, K.; Lanphear, B.P. Prenatal perfluoroalkyl substance exposure and child adiposity at 8 years of age: The HOME study. Obesity (Silver Spring) 2016, 24, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Høyer, B.B.; Ramlauhansen, C.H.; Vrijheid, M.; Valvi, D.; Pedersen, H.S.; Zviezdai, V.; Jönsson, B.A.; Lindh, C.H.; Bonde, J.P.; Toft, G. Anthropometry in 5- to 9-year-old Greenlandic and Ukrainian children in relation to prenatal exposure to perfluorinated alkyl substances. Environ. Health Perspect. 2015, 123, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.S.; Fei, C.; Gamborg, M.; Nohr, E.A.; Sørensen, T.I.A.; Olsen, J. Prenatal exposures to perfluorinated chemicals and anthropometry at 7 years of age. Am. J. Epidemiol. 2013, 178, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Ng, S.; Hsieh, C.J.; Lin, C.C.; Hsieh, W.S.; Chen, P.C. The impact of prenatal perfluoroalkyl substances exposure on neonatal and child growth. Sci. Total. Environ. 2017, 607–608, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Lauritzen, H.B.; Larose, T.L.; Øien, T.; Sandanger, T.M.; Odland, J.Ø.; van de Bor, M.; Jacobsen, G.W. Prenatal exposure to persistent organic pollutants and child overweight/obesity at 5-year follow-up: A prospective cohort study. Environ. Health 2018, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Kulig, M.; Perleth, M.; Langer, G.; Meerpohl, J.J.; Gartlehner, G.; Kaminski-Hartenthaler, A.; Schünemann, H.J. Grade guidelines: 6. Rating the quality of evidence: Imprecision. Z. Evid. Fortbild. Qual. Gesundhwes. 2012, 106, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Janesick, A.; Blumberg, B. Endocrine disrupting chemicals and the developmental programming of adipogenesis and obesity. Birth Defects Res. C. Embryo Today 2011, 93, 34–50. [Google Scholar] [CrossRef] [PubMed]
- White, S.S.; Fenton, S.E.; Hines, E.P. Endocrine disrupting properties of perfluorooctanoic acid. J. Steroid Biochem. Mol. Biol. 2011, 127, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.A.; Leffers, H. Emerging endocrine disrupters: Perfluoroalkylated substances. Int. J. Androl. 2008, 31, 161. [Google Scholar] [CrossRef] [PubMed]
- Hines, E.P.; White, S.S.; Stanko, J.P.; Gibbs-Flournoy, E.A.; Lau, C.; Fenton, S.E. Phenotypic dichotomy following developmental exposure to perfluorooctanoic acid (PFOA) in female CD-1 mice: Low doses induce elevated serum leptin and insulin, and overweight in mid-life. Mol. Cell Endocrinol. 2009, 304, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Vanden Heuvel, J.P.; Thompson, J.T.; Frame, S.R.; Gillies, P.J. Differential activation of nuclear receptors by perfluorinated fatty acid analogs and natural fatty acids: A comparison of human, mouse, and rat peroxisome proliferator-activated receptor-α, -β, and -γ, liver X receptor-β, and retinoid X receptor-α. Toxicol. Sci. 2006, 92, 476–489. [Google Scholar] [CrossRef] [PubMed]
- Walters, M.W.; Bjork, J.A.; Wallace, K.B. Perfluorooctanoic acid stimulated mitochondrial biogenesis and gene transcription in rats. Toxicology 2009, 264, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Moon, S.; Oh, B.C.; Jung, D.; Ji, K.; Choi, K.; Park, Y.J. Association between perfluoroalkyl substances exposure and thyroid function in adults: A meta-analysis. PLoS ONE 2018, 13, e0197244. [Google Scholar] [CrossRef] [PubMed]
- Fei, C.; McLaughlin, J.K.; Tarone, R.E.; Olsen, J. Perfluorinated chemicals and fetal growth: A study within the Danish National Birth Cohort. Environ. Health Perspect. 2007, 115, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, R.M.; Osmond, C.; Phillips, D.I.W.; Godfrey, K.M. Maternal bmi, parity, and pregnancy weight gain: Influences on offspring adiposity in young adulthood. J. Clin. Endocrinol. Metab. 2010, 95, 5365–5369. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Choi, K.; Ji, K.; Seo, J.; Kho, Y.; Park, J.; Kim, S.; Park, S.; Hwang, I.; Jeon, J.; et al. Trans-placental transfer of thirteen perfluorinated compounds and relations with fetal thyroid hormones. Environ. Sci. Technol. 2011, 45, 7465–7472. [Google Scholar] [CrossRef] [PubMed]
- Longnecker, M.P.; Klebanoff, M.A.; Gladen, B.C.; Berendes, H.W. Serial levels of serum organochlorines during pregnancy and postpartum. Arch. Environ. Health 1999, 54, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S. Quantitative methods in the review of epidemiologic literature. Epidemiol. Rev. 1987, 9, 1–30. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cohort | Reference | Location (Baseline Time) | Study Design | N | Gender | Age | Analysis of PFOA | Measurement Timing | Sample Matrix | Confounders | Outcomes of Interest |
|---|---|---|---|---|---|---|---|---|---|---|---|
| POPUP | Gyllenhammar et al. 2018 [27] | Uppsala County (Sweden) (1996–2011) | Prospective cohort | 200 | FM | 5 | UPLC-MS/MS | 3 weeks postpartum | Maternal serum | Sampling year, maternal age, pre-pregnancy BMI, gestational weight gain, maternal weight loss after delivery, education, breastfeeding | BMI standard deviation scores |
| HOME Study | Braun et al. 2016 [28] | Cincinnati, Ohio (USA) (2003–2006) | Prospective cohort | 204 | FM | 8 | HPLC-ID/MS/MS | 16, 26 weeks or birth | Maternal serum | Maternal age, race, education, income, parity, employment, marital status, depressive symptoms, BMI at 16 weeks gestation, fruit consumption, vegetable consumption, fish consumption, prenatal vitamin use, maternal serum cotinine | Overweight or obesity; BMI z-score |
| Aarhus Birth Cohort | Halldorsson et al. 2012 [26] | Denmark (1988–1989) | Prospective cohort | 665 | F/M | 20 | cLC-MS/MS | 30 weeks | Maternal serum | Maternal age, education, pre-pregnancy BMI, smoking, parity, birth weight, age | Overweight or obesity |
| INUENDO | Høyer et al. 2015 [29] | Greenland Ukraine (2002–2004) | Prospective cohort | 531 491 | F/M/FM | 8.3 7 | LC-MS/MS | 25 weeks 23 weeks | Maternal serum | Maternal age, pre-pregnancy BMI, smoking, education, parity | Overweight; BMI z-score |
| Project Viva | Mora et al. 2017 [18] | Massachusetts (USA) (1999–2002) | Prospective pre-birth cohort | 876 | F/M/FM | 7.7 | HPLC-ID/MS/MS | 9.6 weeks | Maternal plasma | Maternal age, race, education, parity, pre-pregnancy BMI, gestational age, income, sex, age | Overweight; Obesity; BMI z-score |
| Danish National Birth Cohort | Andersen et al. 2013 [30] | Denmark (1996–2002) | Prospective cohort | 811 | F/M | 7 | HPLC-MS/MS | 8 weeks | Maternal plasma | Age, maternal age, parity, pre-pregnancy BMI, smoking, socioeconomic status, gestational age | Overweigh or obesity; BMI z-score |
| TBPS | Chen et al. 2017 [31] | Taiwan (China) (2004–2005) | Prospective cohort | 429 | F/M/FM | 9 | UHPLC-MS/MS 1 | At birth | Cord blood | Maternal age, pre-pregnancy BMI, education, log (Ln) transformed cord blood cotinine levels, sex, preterm birth | BMI z-score |
| INMA | Manzano-Salgado et al. 2017 [19] | Gipuzkoa Sabadell Valencia (Spain) (2003–2008) | Prospective cohort | 280 382 424 | F/M/FM | 7 | cLC-MS/MS | 1st trimester | Maternal plasma | Maternal region of residence, birth country, previous breastfeeding, maternal age, pre-pregnancy BMI, age, sex | BMI z-score, Overweight |
| Faroe Islands Cohort | Karlsen et al. 2016 [9] | Faroe Islands (2007–2009) | Prospective cohort | 371 | FM | 5 | LC-MS | 2 weeks postpartum | Maternal serum | Maternal region of residence, maternal age, pre-pregnancy BMI, gestational weight gain, parity, smoking, fish consumption, type of delivery, sex, birth weight | BMI z-score; Overweight |
| SGA Study | Lauritzen et al. 2018 [32] | Norway Sweden (1986–1988) | Prospective cohort | 254 158 | FM | 5 | UHPLC-MS/MS 2 | 2nd trimester | Maternal serum | Maternal age, education, smoking, pre- pregnancy BMI, weight gain at 17 weeks, inter-pregnancy interval, previous breastfeeding, maternal region of residence | BMI z-score; Overweight or obesity |
| Subgroup | Reference (Participants) | β | 95% CI | I2 (%) | p-Value for Heterogeneity |
|---|---|---|---|---|---|
| Total studies | 11 (6076) | 0.10 | 0.03, 0.17 | 27.9 | 0.179 |
| Prenatal exposure | 9 (5505) | 0.09 | 0.02, 0.17 | 36.3 | 0.128 |
| Postnatal exposure | 2 (571) | 0.16 | 0.01, 0.30 | 0 | 0.989 |
| Europe | 7 (3545) | 0.10 | 0.02, 0.17 | 8.4 | 0.364 |
| Northern America | 3(2102) | 0.19 | −0.05, 0.42 | 71.4 | 0.030 |
| Asia | 1 (429) | 0.03 | −0.21, 0.27 | NA | NA |
| Adjusted by maternal parity Yes | 7 (3949) | 0.13 | 0.02, 0.24 | 47.4 | 0.077 |
| Adjusted by maternal parity No | 4 (2127) | 0.07 | −0.01, 0.15 | 0 | 0.491 |
| Adjust birth weight Yes | 1 (371) | 0.16 | −0.05, 0.36 | NA | NA |
| Adjust birth weight NO | 10 (5705) | 0.10 | 0.03, 0.17 | 31.9 | 0.153 |
| Female | 4(1549) | 0.06 | −0.01, 0.13 | 0 | 0.573 |
| Male | 4(1628) | −0.01 | −0.10, 0.08 | 0 | 0.712 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, P.; Yang, F.; Wang, Y.; Yuan, Z. Perfluorooctanoic Acid (PFOA) Exposure in Early Life Increases Risk of Childhood Adiposity: A Meta-Analysis of Prospective Cohort Studies. Int. J. Environ. Res. Public Health 2018, 15, 2070. https://doi.org/10.3390/ijerph15102070
Liu P, Yang F, Wang Y, Yuan Z. Perfluorooctanoic Acid (PFOA) Exposure in Early Life Increases Risk of Childhood Adiposity: A Meta-Analysis of Prospective Cohort Studies. International Journal of Environmental Research and Public Health. 2018; 15(10):2070. https://doi.org/10.3390/ijerph15102070
Chicago/Turabian StyleLiu, Pingping, Fang Yang, Yongbo Wang, and Zhanpeng Yuan. 2018. "Perfluorooctanoic Acid (PFOA) Exposure in Early Life Increases Risk of Childhood Adiposity: A Meta-Analysis of Prospective Cohort Studies" International Journal of Environmental Research and Public Health 15, no. 10: 2070. https://doi.org/10.3390/ijerph15102070
APA StyleLiu, P., Yang, F., Wang, Y., & Yuan, Z. (2018). Perfluorooctanoic Acid (PFOA) Exposure in Early Life Increases Risk of Childhood Adiposity: A Meta-Analysis of Prospective Cohort Studies. International Journal of Environmental Research and Public Health, 15(10), 2070. https://doi.org/10.3390/ijerph15102070