All-Cause and Cancer Mortality Trends in Macheng, China (1984–2013): An Age-Period-Cohort Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Statistical Analysis
3. Results
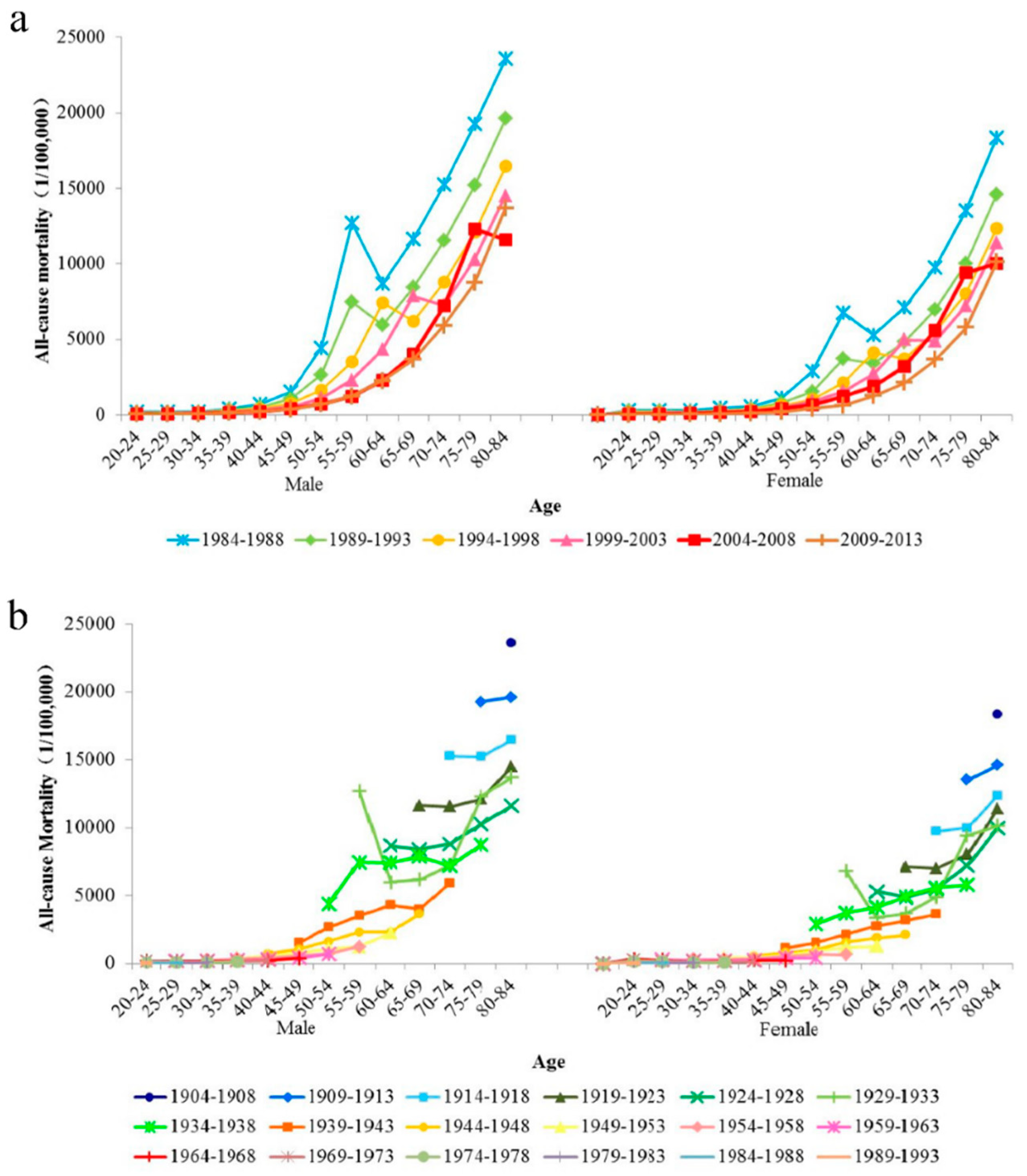
3.1. Descriptive Analysis of All-Cause and Cancer Mortality Trends
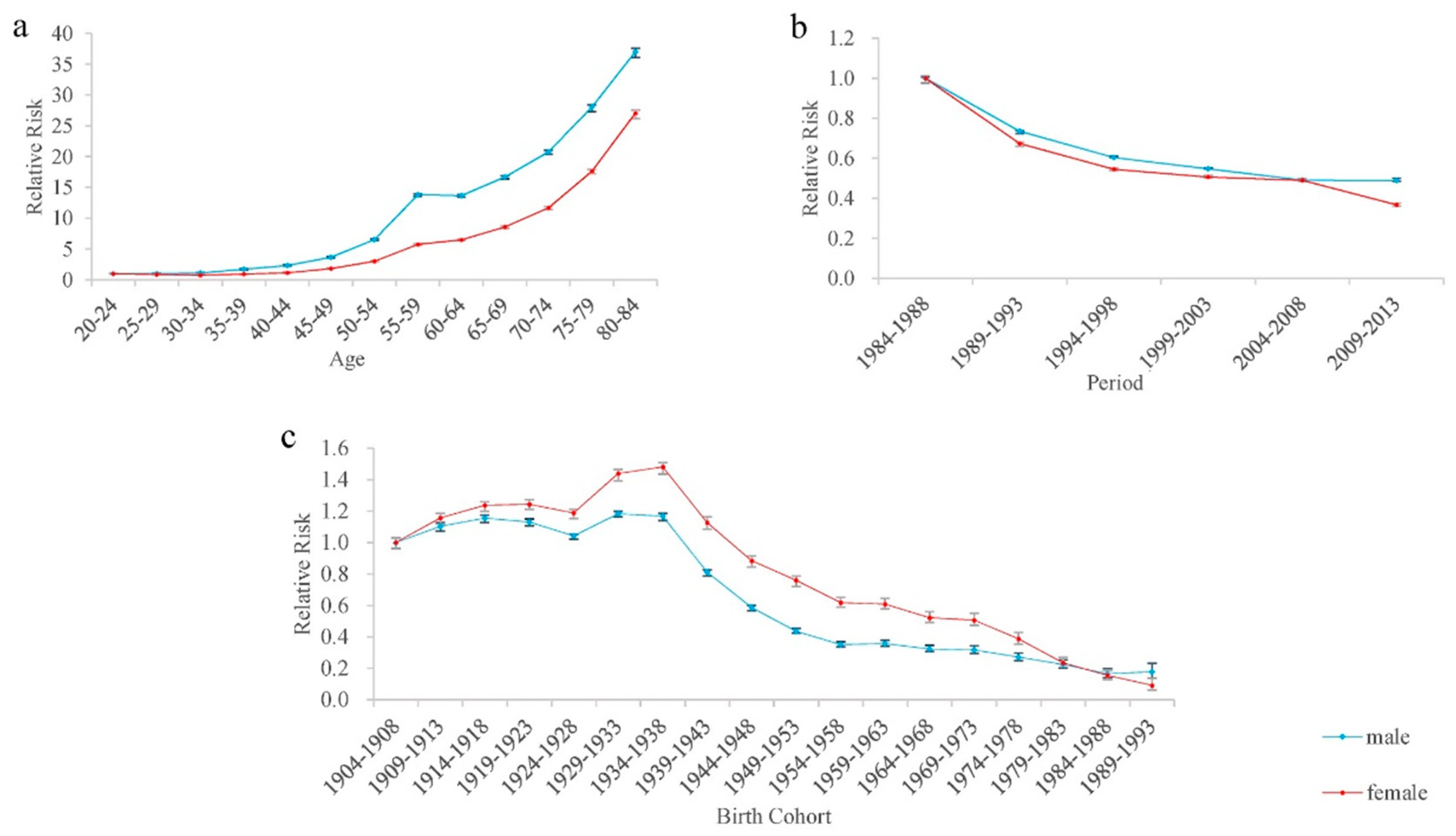
3.2. Age, Period, and Birth Cohort Effects of All-Cause Mortality
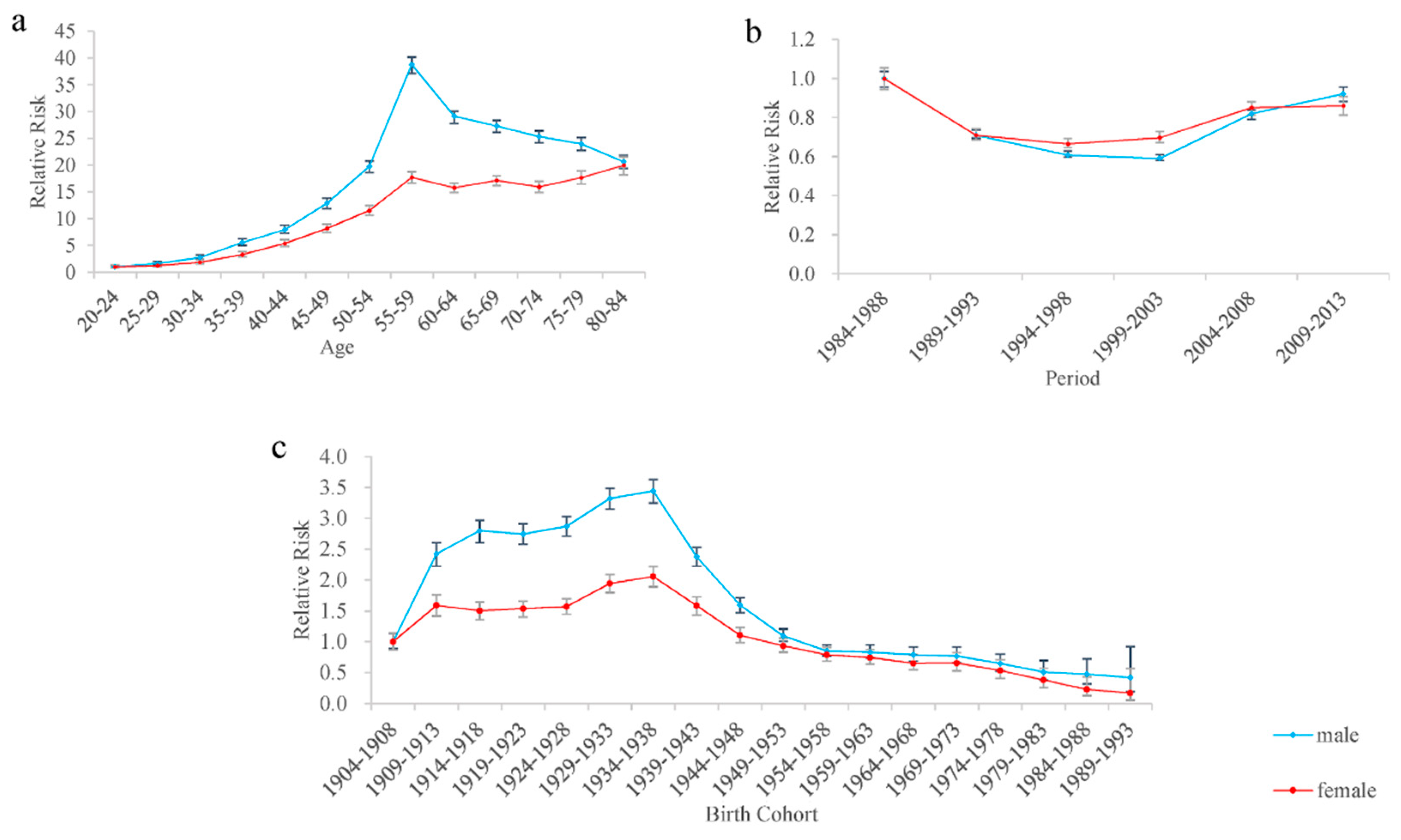
3.3. Age, Period, and Birth Cohort Effects of Cancer Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | 1984–1988 | 1989–1993 | 1994–1998 | 1999–2003 | 2004–2008 | 2009–2013 |
|---|---|---|---|---|---|---|
| 20–24 | 1318 | 1148 | 691 | 387 | 238 | 257 |
| 25–29 | 828 | 1067 | 867 | 539 | 298 | 244 |
| 30–34 | 857 | 676 | 780 | 753 | 451 | 287 |
| 35–39 | 951 | 1047 | 767 | 963 | 867 | 574 |
| 40–44 | 1096 | 1063 | 1186 | 997 | 1088 | 1056 |
| 45–49 | 1503 | 1612 | 1558 | 1667 | 1356 | 1528 |
| 50–54 | 2276 | 2342 | 2277 | 2241 | 2211 | 1877 |
| 55–59 | 3465 | 3458 | 3160 | 3326 | 2697 | 2988 |
| 60–64 | 6157 | 5642 | 5099 | 4872 | 3928 | 4131 |
| 65–69 | 6052 | 5990 | 5152 | 5431 | 4666 | 5234 |
| 70–74 | 5982 | 6359 | 6128 | 5895 | 5097 | 5864 |
| 75–79 | 3038 | 3483 | 3347 | 4372 | 3666 | 4939 |
| 80–84 | 2162 | 2043 | 2281 | 2888 | 2915 | 3359 |
| Total | 35,685 | 35,930 | 33,293 | 34,331 | 29,478 | 32,338 |
| Age Group | 1984–1988 | 1989–1993 | 1994–1998 | 1999–2003 | 2004–2008 | 2009–2013 |
|---|---|---|---|---|---|---|
| 20–24 | 42 | 46 | 48 | 25 | 29 | 29 |
| 25–29 | 42 | 71 | 69 | 56 | 58 | 37 |
| 30–34 | 88 | 64 | 103 | 131 | 118 | 56 |
| 35–39 | 122 | 156 | 152 | 251 | 273 | 165 |
| 40–44 | 185 | 203 | 265 | 253 | 347 | 380 |
| 45–49 | 311 | 329 | 356 | 413 | 376 | 542 |
| 50–54 | 421 | 468 | 427 | 438 | 606 | 575 |
| 55–59 | 575 | 615 | 611 | 591 | 662 | 894 |
| 60–64 | 776 | 674 | 671 | 723 | 856 | 954 |
| 65–69 | 514 | 569 | 540 | 629 | 798 | 963 |
| 70–74 | 354 | 426 | 432 | 457 | 612 | 888 |
| 75–79 | 125 | 142 | 147 | 233 | 302 | 561 |
| 80–84 | 37 | 59 | 74 | 94 | 166 | 220 |
| Total | 3592 | 3822 | 3895 | 4294 | 5203 | 6264 |
| Index | All-Cause | Cancer | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| Deviance | 3708.55 | 1759.00 | 764.75 | 255.84 |
| AIC | 57.39 | 32.15 | 17.74 | 10.55 |
| BIC | 3516.86 | 1567.30 | 573.06 | 64.15 |
References
- McGuire, S. World Cancer Report 2014. Geneva, Switzerland: World Health Organization, International Agency for Research on Cancer, WHO Press 2015. Adv. Nutr. 2016, 7, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Barber, R.M.; Foreman, K.J.; Abbasoglu Ozgoren, A.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Abraham, J.P.; Abubakar, I.; Abu-Raddad, L.J.; et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: Quantifying the epidemiological transition. Lancet 2015, 386, 2145–2191. [Google Scholar] [CrossRef]
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Center, M.M.; DeSantis, C.; Ward, E.M. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1893–1907. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (accessed on 22 July 2018).
- Zhao, P.; Dai, M.; Chen, W.; Li, N. Cancer trends in China. Jpn. J. Clin. Oncol. 2010, 40, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zhang, Y.; Zhang, M.; Zeng, H.; Zhang, L.; Zhang, Q.J. Data Analysis of the Third National Retrospective Sampling Death Survey I: Main Death of Hubei Population. Cancer Prev. Res. 2008, 35, 31–33. (In Chinese) [Google Scholar]
- Zhang, Y.; Zhang, M.; Li, G.; Zeng, H.; Zhang, L.; Zhang, Q.J. Data Analysis of the Third National Retrospective Sampling Death Survey II: Death Actuality and Epidemic Trend of Malignant Tumor in Hubei Province Population. Cancer Prev. Res. 2008, 35, 34–36. (In Chinese) [Google Scholar]
- Zhang, M.; Zhang, Y.; Li, G.; Zeng, H.; Zhang, L.; Zhang, Q.J. Data Analysis of the Third National Retrospective Sampling Death Survey III Characteristics of Death of Malignant Tumors of Hubei Population. Cancer Prev. Res. 2008, 35, 37–39. (In Chinese) [Google Scholar]
- Wong, I.O.; Schooling, C.M.; Cowling, B.J.; Leung, G.M. Breast cancer incidence and mortality in a transitioning Chinese population: Current and future trends. Br. J. Cancer 2015, 112, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, Y.; Li, M.; Cheng, K.; Zhao, X.; Zheng, Y.; Liu, Y.; Lei, S.; Wang, L. Long-term trends of liver cancer mortality by gender in urban and rural areas in China: An age-period-cohort analysis. BMJ Open 2018, 8, e020490. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Yu, C.; Wang, P. An age-period-cohort analysis of female breast cancer mortality from 1990–2009 in China. Int. J. Equity Health 2015, 14, 76. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Parkin, D.M.; Li, L.; Chen, Y. Time trends in cancer mortality in China: 1987–1999. Int. J. Cancer 2003, 106, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Parkin, D.M.; Li, L.; Chen, Y.; Bray, F. Estimation and projection of the national profile of cancer mortality in China: 1991–2005. Br. J. Cancer 2004, 90, 2157–2166. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.G.; Xu, C.L.; Yu, C.H. Age-period-cohort analysis on the cancer mortality in rural China: 1990–2010. Int. J. Equity Health 2014, 13, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.W.; Wu, X.L.; Lopez, A.D.; Wang, L.; Cai, Y.; Page, A.; Yin, P.; Liu, Y.; Li, Y.; Liu, J.; et al. An integrated national mortality surveillance system for death registration and mortality surveillance. China Bull. World Health Org. 2016, 94, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Hu, J.; Rao, K.Q.; Ma, J.; Rao, C.; Lopez, A.D. Mortality registration and surveillance in China: History, current situation and challenges. Pop. Health Metr. 2005, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.J.; Zhang, L.; Zhang, Q.J.; He, T.J.; Fu, Y.; Ren, S.C. Underreporting of death in disease surveillance system in Hubei, 2009–2011 (in Chinese). Dis. Surv. 2013, 28, 478–480. [Google Scholar]
- Su, J.; Peng, F. The review of parameter estimation methods of age-period-cohort model. Stat. Decis. 2014, 23, 21–26. [Google Scholar]
- Fu, W.J. Ridge estimator in singular design with application to age-period-cohort analysis of disease rates. Commun. Stat.-Theory Methods 2000, 29, 263–278. [Google Scholar] [CrossRef]
- Yang, Y.; Schulhofer-Wohl, S.; Fu, W.J.; Land, K.C. The intrinsic estimator for age-period-cohort analysis: What it is and how to use it. Am. J. Sociol. 2008, 113, 1697–1736. [Google Scholar] [CrossRef]
- Yang, Y.; Land, K.C. Age-Period-Cohort Analysis New Models, Methods, and Empirical Applications; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Li, Z.; Wang, P.; Gao, G.; Xu, C.; Chen, X. Age-period-cohort analysis of infectious disease mortality in urban-rural China, 1990–2010. Int. J. Equity Health 2016, 15, 55. [Google Scholar] [CrossRef] [PubMed]
- Kupper, L.L.; Janis, J.M.; Karmous, A.; Greenberg, B.G. Statistical age-period-cohort analysis: A review and critique. J. Chronic Dis. 1985, 38, 811–830. [Google Scholar] [CrossRef]
- Chen, W.Q.; Zheng, R.S.; Zhang, S.W.; Zeng, H.M.; Zou, X.N.; He, J. Analysis of cancer incidence and mortality in elderly population in China, 2013. Chin. J. Oncol. 2017, 39, 60–66. (In Chinese) [Google Scholar]
- Gouveia, N.; Fletcher, T. Time series analysis of air pollution and mortality: Effects by cause, age and socioeconomic status. J. Epidemiol. Community Health 2000, 54, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.P. Age-specific and year of birth changes in hospital admissions during a period of unexplained higher deaths in England. Eur. J. Internal Med. 2017, 45, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Kvakkestad, K.M.; Wang, M.F.; Eritsland, J.; Halvorsen, S. Gender differences in all-cause, cardiovascular and cancer mortality during long-term follow-up after acute myocardial infarction: A prospective cohort study. BMC Cardiovasc. Disord. 2017, 17, 75. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Ma, J.M.; Ward, E.M.; Siegel, R.L.; Jemal, A. Temporal Trends in Mortality in the United States, 1969–2013. J. Am. Med. Assoc. 2015, 314, 1731–1739. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Yang, M. Impact of Urbanization on the Health of Chinese Residents: An Empirical Study Based on Provincial Panel Data. China Pop. Resour. Environ. 2015, 25, 89–96. (In Chinese) [Google Scholar]
- Wang, L.; Kong, L.; Wu, F.; Bai, Y.; Burton, R. Preventing chronic diseases in China. Lancet 2005, 366, 1821–1824. [Google Scholar] [CrossRef]
- Tang, S.L.; Ehiri, J.; Long, Q. China’s biggest, most neglected health challenge: Non-communicable diseases. Infect. Dis. Poverty 2013, 6, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, R.; Zhang, S.; Zeng, H.; Xia, C.; Zuo, T.; Yang, Z.; Zou, X.; He, J. Cancer incidence and mortality in China, 2013. Cancer Lett. 2017, 401, 63–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, G.H.; Kong, L.Z.; Zhao, W.H.; Wan, X.; Zhai, Y.; Chen, L.C. Koplan J.P. Emergence of chronic non-communicable diseases in China. Lancet 2008, 372, 8–14. [Google Scholar] [CrossRef]
- Hagger-Johnson, G.; Batty, G.D.; Deary, I.J.; von Stumm, S. Childhood socioeconomic status and adult health: Comparing formative and reflective models in the Aberdeen Children of the 1950s Study (prospective cohort study). J. Epidemiol. Community Health 2011, 65, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Wong, I.O.L.; Cowling, B.J.; Law, S.C.K.; Mang, O.W.; Schooling, C.M.; Leung, G.M. Understanding sociohistorical imprint on cancer risk by age-period-cohort decomposition in Hong Kong. J. Epidemiol. Community Health 2010, 64, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, M.B.; McGlynn, K.A.; Devesa, S.S.; Freedman, N.D.; Anderson, W.F. Sex disparities in cancer mortality and survival. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Kunst, A.E.; Cavelarrs, A.E.; Groenhof, F.; Geurts, J.J. Socioeconomic inequalities in morbidity and mortality in western Europe. Lancet 1997, 349, 1655–1659. [Google Scholar] [CrossRef] [Green Version]
- Huisman, M.; Kunst, A.E.; Boop, M.; Borgan, J.K.; Borrell, C.; Costa, G.; Deboosere, P.; Gadeyne, S.; Glickman, M.; Marinacci, C.; et al. Educational inequalities in cause-specific mortality in middle-aged and older men and women in eight western European populations. Lancet 2005, 365, 493–500. [Google Scholar] [CrossRef]
- Zeng, J.X.; Pang, X.P.; Zhang, L.X.; Medina, A.; Rozelle, S. Gender inequality in education in China: A meta-regression analysis. Contemp. Econ. Policy 2014, 32, 474–491. [Google Scholar] [CrossRef]
- Wang, J.B.; Jiang, Y.; Liang, H.; Li, P.; Xiao, H.J.; Ji, J.; Xiang, W.; Shi, J.F.; Fan, Y.G.; Li, L.; et al. Attributable causes of cancer in China. Ann. Oncol. 2012, 23, 2983–2989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, G.H. Marketing ‘less harmful, low-tar’ cigarettes is a key strategy of the industry to counter tobacco control in China. Tobacco Control 2014, 23, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.H.; Ma, J.M.; Liu, N.; Zhou, L.N. Smoking and passive smoking in Chinese, 2002. Chin. J. Epidemiol. 2005, 26, 77–83. (In Chinese) [Google Scholar]
- Zhang, J.; Ou, J.X.; Bai, C.X. Tobacco smoking in China: Prevalence, disease burden, challenges and future strategies. Respirology 2011, 16, 1165–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Wen, L.; Cui, W.; Yuan, W.; Yang, Z.; Jiang, K.; Jiang, X.; Huo, M.; Sun, Z.; Han, H.; et al. Prevalence of Cigarette Smoking and Nicotine Dependence in Men and Women Residing in Two Provinces in China. Front. Psychiatry 2017, 8, 254. [Google Scholar] [CrossRef] [PubMed]
- Goss, P.E.; Strasser-Weippl, K.; Lee-Bychkovsky, B.L.; Fan, L.; Li, J.; Chavarri-Guerra, Y.; Liedke, P.E.; Pramesh, C.S.; Badovinac-Crnjevic, T.; Sheikine, Y.; et al. Challenges to effective cancer control in China, India, and Russia. Lancet Oncol. 2014, 15, 489–538. [Google Scholar] [CrossRef]
- Gao, H. Chinese Government admits existence of cancer villages. Lancet Oncol. 2013, 14, 284. [Google Scholar] [CrossRef]
- Liu, L. Rural-urban inequities in deaths and cancer mortality amid rapid economic and environmental changes in China. Int. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Eyles, J.; Consitt, N. What’s at risk? Environmental influences on human health. Environment 2004, 46, 25–39. [Google Scholar] [CrossRef]
- Kahn, M.E. Domestic pollution havens: Evidence from cancer deaths in border counties. J. Urban Econ. 2004, 56, 51–69. [Google Scholar] [CrossRef]
- Chao, A.; Edwards, B.K. Cancer surveillance and research on environmental contributions to cancer. Rev. Environ. Health 2016, 31, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Han, Y.; Tang, X.; Zhu, J.; Zhu, T. Estimating adult mortality attributable to PM2.5 exposure in China with assimilated PM2.5 concentrations based on a ground monitoring network. Sci. Total Environ. 2016, 568, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Danaei, G.; Vander Hoorn, S.; Lopez, A.D.; Murray, C.J.; Ezzati, M. Comparative Risk Assessment collaborating group (Cancers). Causes of cancer in the world: Comparative risk assessment of nine behavioural and environmental risk factors. Lancet 2005, 366, 1784–1793. [Google Scholar] [CrossRef]
- Feng, Z.M.; Shi, D.F. Chinese food consumption and nourishment in the latest 20 years. Resour. Sci. 2006, 28, 2–8. (In Chinese) [Google Scholar]
- Qin, W.; Liu, F.; Wan, C. A U-shaped association of body mass index and all-cause mortality in heart failure patients: A dose-response meta-analysis of prospective cohort studies. Cardiovasc. Ther. 2017, 35. [Google Scholar] [CrossRef] [PubMed]
- Rojas, J.S.M.; Mulas, A.L.; Galeano, H.P. Physical Exercise Minimizes the Toxic Triad for Cancer: Physical Inactivity, Low Fitness, and Obesity. Eur. J. Hum. Mov. 2016, 36, 1–35. [Google Scholar]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2017, 2819372. [Google Scholar] [CrossRef] [PubMed]
- Weiderpass, E.; Botteri, E. Ovarian cancer mortality trends: Which factors are involved? Ann. Oncol. 2016, 27, 1977–1978. [Google Scholar] [CrossRef] [PubMed]
- Martin-Dunlap, T.M.; Wachtel, M.S.; Margenthaler, J.A. Outcomes for patients who are diagnosed with breast and endometrial cancer. Oncol. Lett. 2013, 6, 1103–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Characteristic | All-Cause | Cancer | ||||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | |||||
| Coef. | 95% CI | Coef. | 95% CI | Coef. | 95% CI | Coef. | 95% CI | |
| Age | ||||||||
| 20–24 | −1.75 *** | (−1.82, −1.67) | −1.21 *** | (−1.27, −1.15) | −2.35 *** | (−2.62, −2.08) | −1.94 *** | (−2.24, −1.65) |
| 25–29 | −1.74 *** | (−1.81, −1.67) | −1.36 *** | (−1.42, −1.30) | −1.86 *** | (−2.06, −1.66) | −1.74 *** | (−1.98, −1.49) |
| 30–34 | −1.65 *** | (−1.71, −1.58) | −1.48 *** | (−1.54, −1.42) | −1.34 *** | (−1.50, −1.18) | −1.33 *** | (−1.53, −1.13) |
| 35–39 | −1.21 *** | (−1.25, −1.15) | −1.27 *** | (−1.33, −1.22) | −0.64 *** | (−0.75, −0.52) | −0.75 *** | (−0.90, −0.60) |
| 40–44 | −0.90 *** | (−0.94, −0.85) | −1.06 *** | (−1.11, −1.02) | −0.28 *** | (−0.37, −0.18) | −0.27 *** | (−0.38, −0.15) |
| 45–49 | −0.44 *** | (−0.47, −0.41) | −0.60 *** | (−0.63, −0.56) | 0.20 *** | (0.12, 0.27) | 0.15 ** | (0.05, 0.24) |
| 50–54 | 0.13 *** | (0.10, 0.15) | −0.10 *** | (−0.13, −0.08) | 0.63 *** | (0.57, 0.68) | 0.49 *** | (0.41, 0.57) |
| 55–59 | 0.88 *** | (0.86, 0.89) | 0.53 *** | (0.51, 0.55) | 1.30 *** | (1.26, 1.34) | 0.92 *** | (0.86, 0.98) |
| 60–64 | 0.87 *** | (0.85, 0.88) | 0.65 *** | (0.63, 0.67) | 1.01 *** | (0.97, 1.05) | 0.80 *** | (0.75, 0.86) |
| 65–69 | 1.07 *** | (1.05, 1.08) | 0.93 *** | (0.91, 0.95) | 0.95 *** | (0.91, 0.99) | 0.89 *** | (0.83, 0.94) |
| 70–74 | 1.29 *** | (1.27, 1.30) | 1.24 *** | (1.22, 1.26) | 0.87 *** | (0.83, 0.92) | 0.82 *** | (0.75, 0.88) |
| 75–79 | 1.59 *** | (1.56, 1.60) | 1.65 *** | (1.63, 1.67) | 0.82 *** | (0.77, 0.87) | 0.92 *** | (0.85, 0.99) |
| 80–84 | 1.87 *** | (1.84, 1.88) | 2.08 *** | (2.05, 2.10) | 0.67 *** | (0.61, 0.73) | 1.04 *** | (0.95, 1.12) |
| Period | ||||||||
| 1984–1988 | 0.47 *** | (0.45, 0.48) | 0.56 *** | (0.54, 0.58) | 0.27 *** | (0.23, 0.31) | 0.23 *** | (0.18, 0.29) |
| 1989–1993 | 0.17 *** | (0.15, 0.17) | 0.17 *** | (0.15, 0.18) | −0.06 *** | (−0.09, −0.03) | −0.10 *** | (−0.14, −0.06) |
| 1994–1998 | −0.03 *** | (−0.03, −0.02) | −0.04 *** | (−0.05, −0.03) | −0.22 *** | (−0.24, −0.19) | −0.17 *** | (−0.20, −0.13) |
| 1999–2003 | −0.13 *** | (−0.13, −0.12) | −0.11 *** | (−0.12, −0.10) | −0.25 *** | (−0.27, −0.22) | −0.12 *** | (−0.16, −0.08) |
| 2004–2008 | −0.24 *** | (−0.25, −0.22) | −0.14 *** | (−0.16, −0.13) | 0.07 *** | (0.04, 0.10) | 0.07 ** | (0.03, 0.11) |
| 2009–2013 | −0.24 *** | (−0.25, −0.22) | −0.43 *** | (−0.45, −0.41) | 0.19 *** | (0.15, 0.23) | 0.08 ** | (0.03, 0.14) |
| Birth Cohort | ||||||||
| 1904–1908 | 0.64 *** | (0.60, 0.67) | 0.42 *** | (0.39, 0.46) | −0.23 *** | (−0.35, −0.11) | 0.14 * | (0.00, 0.28) |
| 1909–1913 | 0.74 *** | (0.71, 0.76) | 0.57 *** | (0.54, 0.60) | 0.64 *** | (0.56, 0.72) | 0.60 *** | (0.49, 0.71) |
| 1914–1918 | 0.78 *** | (0.76, 0.80) | 0.64 *** | (0.61, 0.66) | 0.79 *** | (0.72, 0.85) | 0.54 *** | (0.45, 0.64) |
| 1919–1923 | 0.76 *** | (0.74, 0.78) | 0.64 *** | (0.62, 0.67) | 0.77 *** | (0.71, 0.83) | 0.57 *** | (0.48, 0.65) |
| 1924–1928 | 0.68 *** | (0.66, 0.69) | 0.60 *** | (0.57, 0.62) | 0.81 *** | (0.76, 0.87) | 0.59 *** | (0.51, 0.67) |
| 1929–1933 | 0.81 *** | (0.79, 0.82) | 0.79 *** | (0.76, 0.81) | 0.96 *** | (0.91, 1.01) | 0.80 *** | (0.73, 0.88) |
| 1934–1938 | 0.80 *** | (0.77, 0.81) | 0.82 *** | (0.79, 0.84) | 0.99 *** | (0.94, 1.05) | 0.86 *** | (0.78, 0.94) |
| 1939–1943 | 0.43 *** | (0.40, 0.45) | 0.54 *** | (0.51, 0.58) | 0.62 *** | (0.56, 0.69) | 0.60 *** | (0.50, 0.69) |
| 1944–1948 | 0.11 *** | (0.07, 0.13) | 0.30 *** | (0.26, 0.34) | 0.22 *** | (0.15, 0.30) | 0.24 *** | (0.13, 0.35) |
| 1949–1953 | −0.19 *** | (−0.22, −0.15) | 0.15 *** | (0.10, 0.19) | −0.14 ** | (−0.23, −0.05) | 0.07 | (−0.04, 0.20) |
| 1954–1958 | −0.41 *** | (−0.45, −0.36) | −0.05 | (−0.10, 0.00) | −0.39 *** | (−0.50, −0.29) | −0.09 | (−0.23, 0.05) |
| 1959–1963 | −0.39 *** | (−0.44, −0.33) | −0.06 * | (−0.12, −0.01) | −0.42 *** | (−0.54, −0.29) | −0.15 | (−0.31, 0.01) |
| 1964–1968 | −0.49 *** | (−0.54, −0.42) | −0.22 *** | (−0.28, −0.15) | −0.47 *** | (−0.61, −0.33) | −0.28 ** | (−0.46, −0.09) |
| 1969–1973 | −0.51 *** | (−0.58, −0.43) | −0.25 *** | (−0.32, −0.17) | −0.49 *** | (−0.66, −0.33) | −0.27 * | (−0.49, −0.05) |
| 1974–1978 | −0.66 *** | (−0.75, −0.57) | −0.51 *** | (−0.61, −0.42) | −0.67 *** | (−0.88, −0.46) | −0.48 ** | (−0.76, −0.20) |
| 1979–1983 | −0.86 *** | (−0.97, −0.73) | −1.01 *** | (−1.14, −0.88) | −0.91 *** | (−1.21, −0.60) | −0.82 *** | (−1.21, −0.42) |
| 1984–1988 | −1.15 *** | (−1.32, 0.98) | −1.43 *** | (−1.61, −1.24) | −0.98 *** | (−1.39, −0.56) | −1.32 *** | (−1.94, −0.70) |
| 1989–1993 | −1.09 *** | (−1.34, −0.82) | −1.95 *** | (−2.34, −1.56) | −1.10 ** | (−1.88, −0.32) | −1.62 ** | (−2.81, −0.43) |
| Intercept | 7.09 *** | (7.06, 7.11) | 6.73 *** | (6.71, 6.76) | 5.10 *** | (5.05, 5.16) | 4.42 *** | (4.34, 4.51) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.; Hu, S.; Yu, C. All-Cause and Cancer Mortality Trends in Macheng, China (1984–2013): An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2018, 15, 2068. https://doi.org/10.3390/ijerph15102068
Li C, Hu S, Yu C. All-Cause and Cancer Mortality Trends in Macheng, China (1984–2013): An Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health. 2018; 15(10):2068. https://doi.org/10.3390/ijerph15102068
Chicago/Turabian StyleLi, Chunhui, Songbo Hu, and Chuanhua Yu. 2018. "All-Cause and Cancer Mortality Trends in Macheng, China (1984–2013): An Age-Period-Cohort Analysis" International Journal of Environmental Research and Public Health 15, no. 10: 2068. https://doi.org/10.3390/ijerph15102068
APA StyleLi, C., Hu, S., & Yu, C. (2018). All-Cause and Cancer Mortality Trends in Macheng, China (1984–2013): An Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health, 15(10), 2068. https://doi.org/10.3390/ijerph15102068