
Soil Lead and Children’s Blood Lead Disparities in Pre- and Post-Hurricane Katrina New Orleans (USA)



Abstract
:1. Introduction
2. Materials and Methods
3. Results
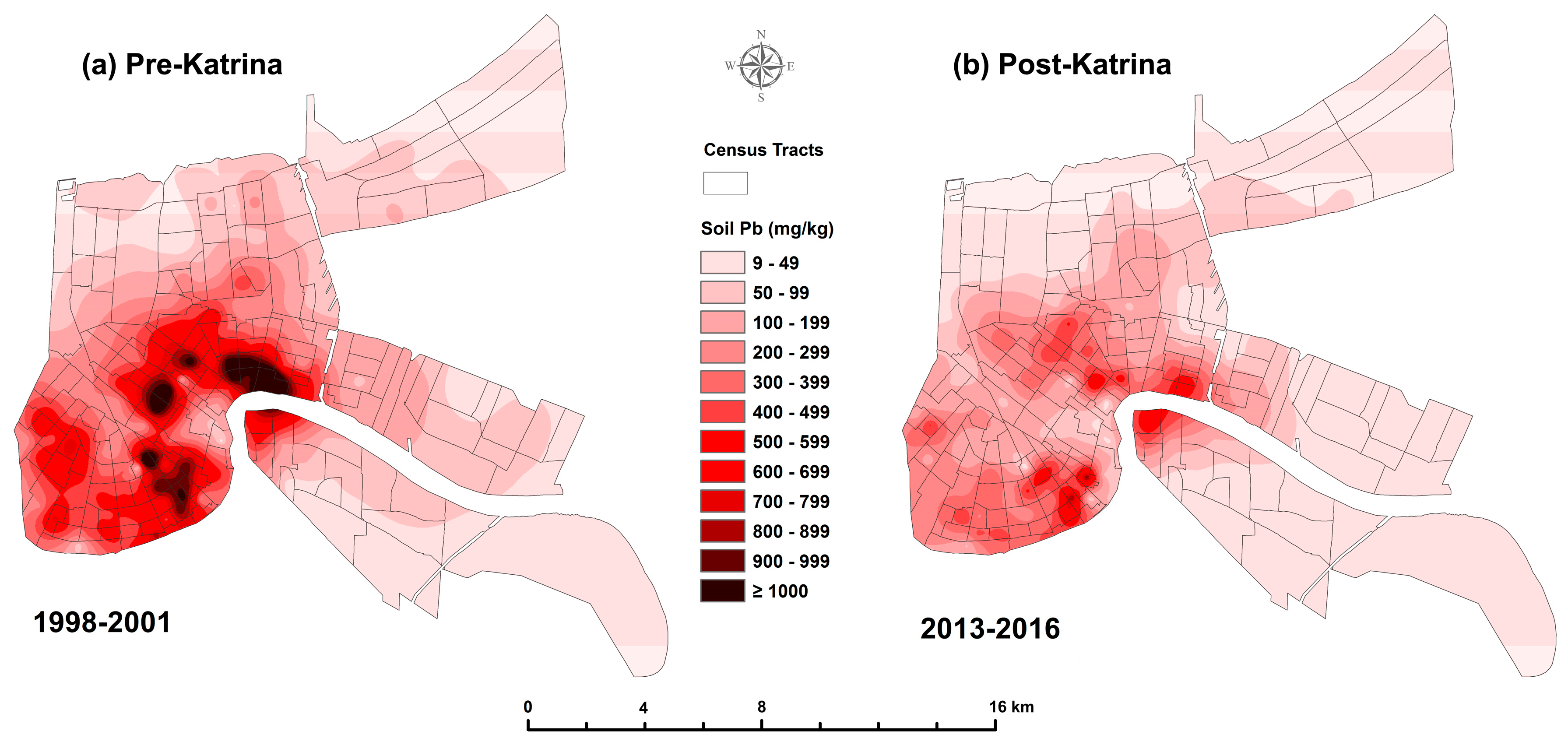
3.1. Change in Soil Lead
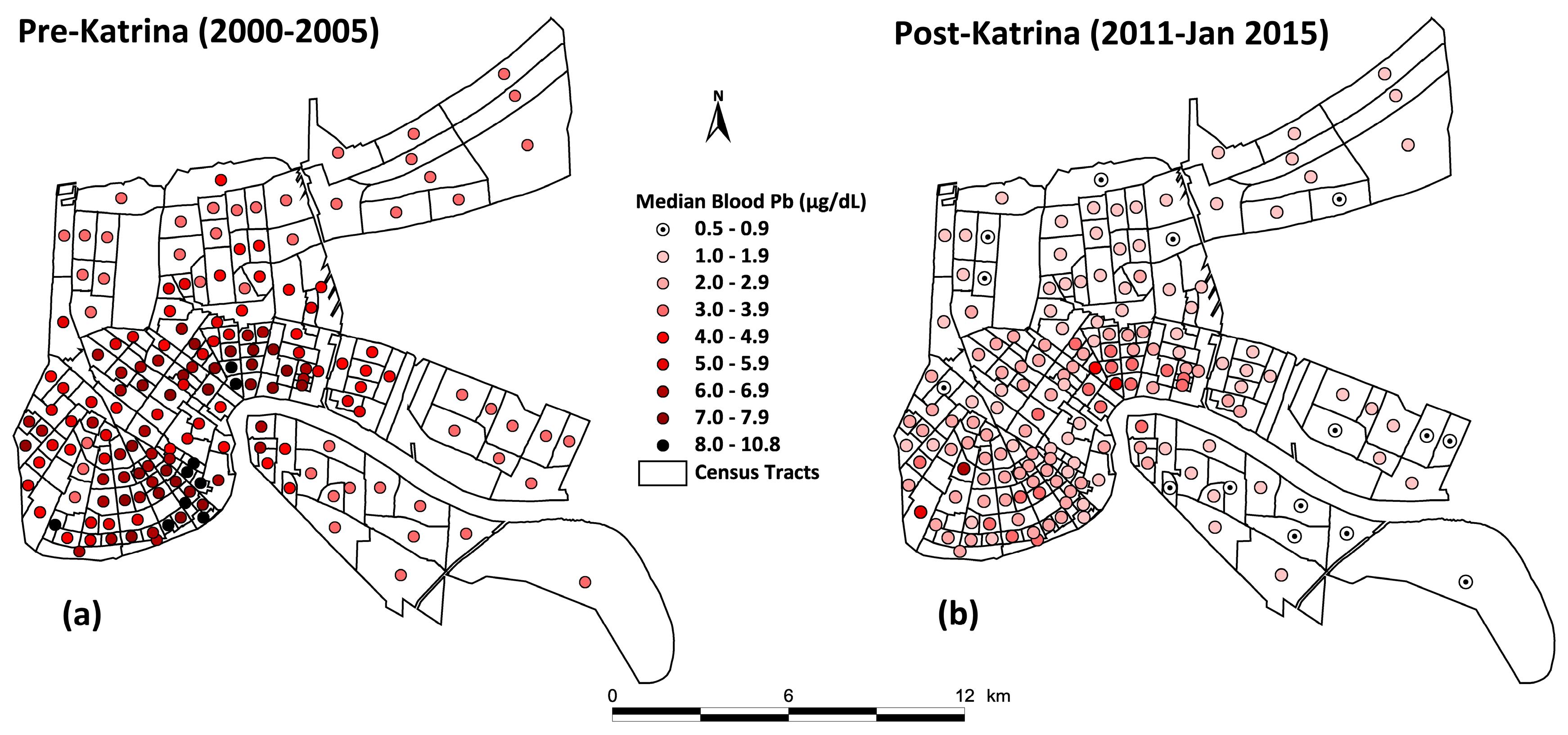
3.2. Change in Children’s Blood Lead
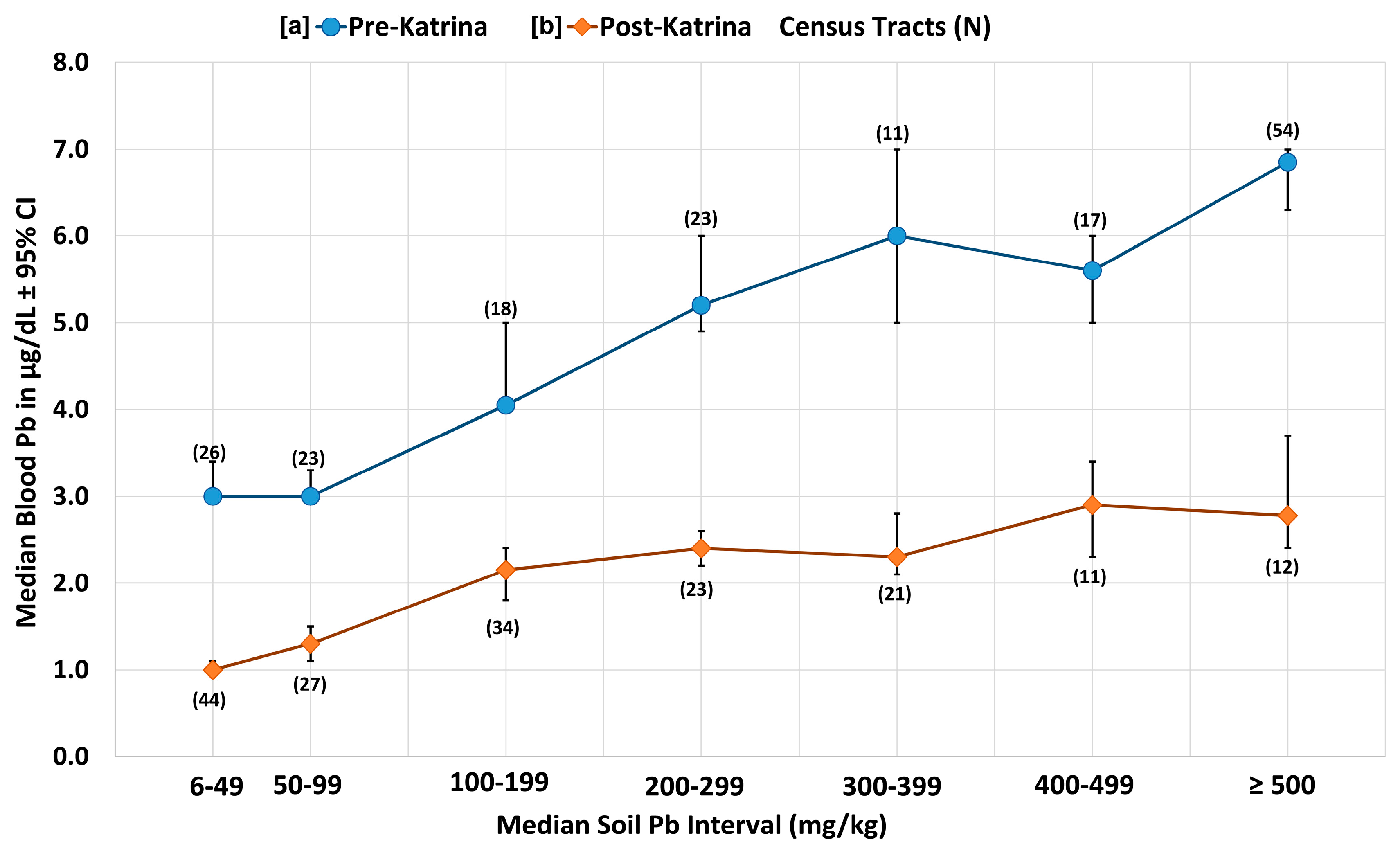
3.3. Graph of the Disparities of Pre- and Post-Katrina Soil Lead and Blood Lead in New Orleans
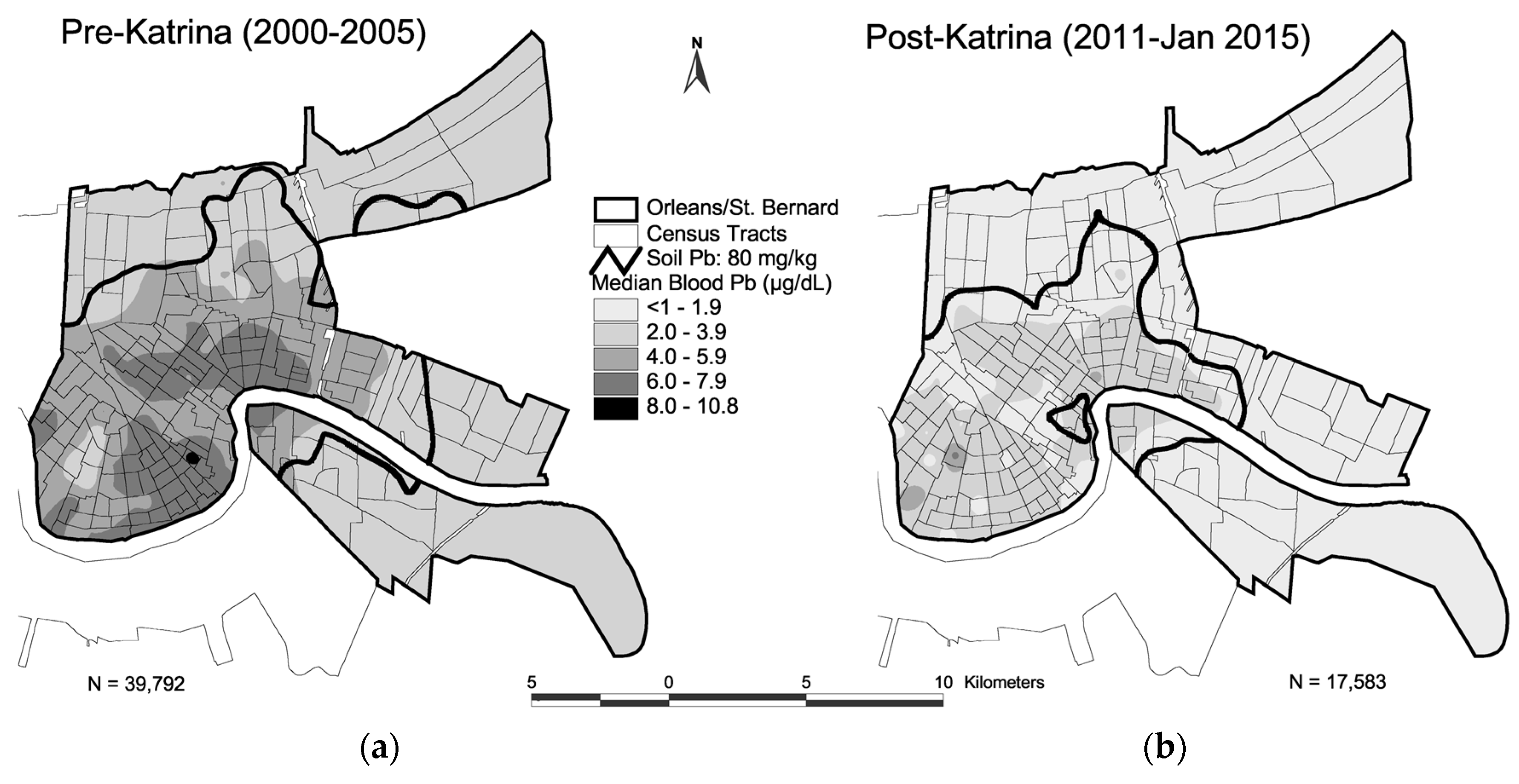
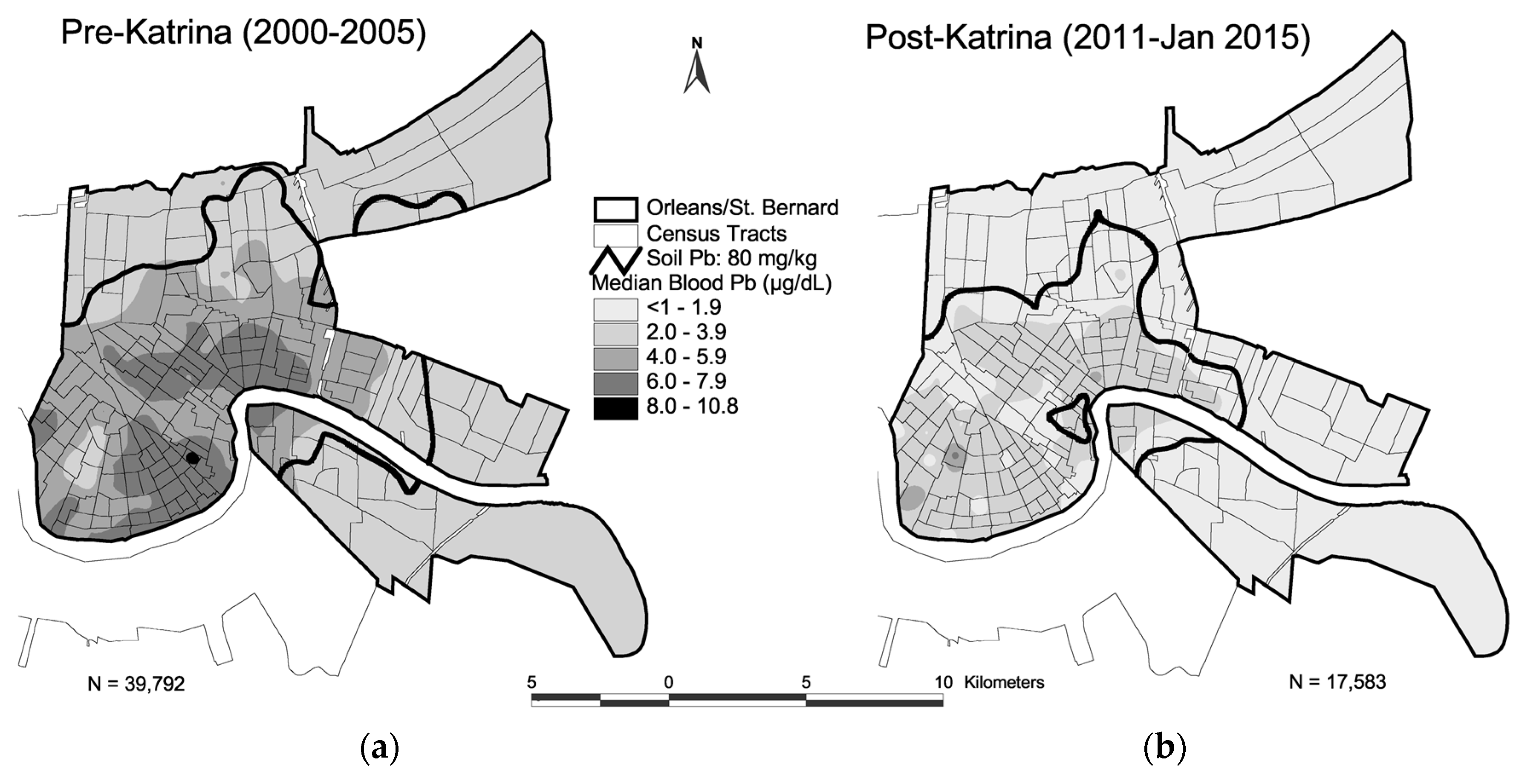
3.4. Map of Pre- and Post-Katrina Changes of Soil Lead and Blood Lead
4. Discussion
4.1. National Health and Nutrition Evaluation Survey (NHANES) vs. New Orleans Blood Lead Trends
4.2. Inputs of Lead and Other Toxic Substances into the Environment
4.3. Soil Lead Content vs. Lead Loading, Environmental Signaling, and Lead Exposure
4.4. Lessons from Hurricane Katrina and the New Orleans Soil Environment
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A
References
- Wolman, A. The metabolism of cities. Sci. Am. 1965, 213, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.P. The exposome: from concept to utility. Int. J. Epidemiol. 2012, 41, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C. The Protean Toxicities of Lead: New Chapters in a Familiar Story. Int. J. Environ. Res. Public Health 2011, 8, 2593–2628. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C. Childhood lead exposure and adult outcomes. JAMA 2017, 317, 1219–1220. [Google Scholar] [CrossRef] [PubMed]
- Juarez, P.D.; Matthews-Juarez, P.; Hood, D.B.; Im, W.; Levine, R.S.; Kilbourne, B.J.; Langston, M.A.; Al-Hamdan, M.Z.; Crosson, W.L.; Estes, M.G.; et al. The Public Health Exposome: A Population-Based, Exposure Science Approach to Health Disparities Research. Int. J. Environ. Res. Public Health 2014, 11, 12866–12895. [Google Scholar] [CrossRef] [PubMed]
- White, B.M.; Bonilha, H.S.; Ellis, C., Jr. Racial/ethnic differences in childhood blood lead levels among children <72 months of age in the United States: A systematic review of the literature. J. Racial Ethn. Health Disparities 2016, 3, 145–153. [Google Scholar]
- Needleman, H.L.; McFarland, C.; Ness, R.B.; Fienberg, S.E.; Tobin, M.J. Bone lead levels in adjudicated delinquents. A case control study. Neurotoxicol. Teratol. 2003, 24, 711–717. [Google Scholar] [CrossRef]
- Mielke, H.W.; Zahran, S. The urban rise and fall of air lead (Pb) and the latent surge and retreat of societal violence. Environ. Int. 2012, 43, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. CDC Response to Advisory Committee on Childhood Lead Poisoning Prevention Recommendations in “Low Level Lead Exposure Harms Children: A Renewed Call for Primary Prevention”. U.S. Department of Health and Human Services: Atlanta, GA, USA. Available online: http://www.cdc.gov/nceh/lead/acclpp/cdc_response_lead_exposure_recs.pdf (accessed on 12 December 2016).
- Desmurget, M.; Richard, N.; Harquel, S.; Baraduc, P.; Szathmari, A.; Mottolese, C.; Sirigu, A. Neural representations of ethologically relevant hand/mouth synergies in the human Precentral gyrus. Proc. Natl. Acad. Sci. USA 2014, 111, 5718–5722. [Google Scholar] [CrossRef] [PubMed]
- Bruening, K.; Kemp, F.W.; Simone, N.; Holding, Y.; Louria, D.B.; Bogden, J.D. Dietary calcium intakes of urban children at risk of lead poisoning. Environ. Health Perspect. 1999, 107, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Nussbaumer-Streit, B.; Yeoh, B.; Griebler, U.; Pfadenhauer, L.M.; Busert, L.K.; Lhachimi, S.K.; Lohner, S.; Gartlehner, G. Household interventions for preventing domestic lead exposure in children. Cochrane Database Syst. Rev. 2016, 16, CD006047. [Google Scholar]
- Kennedy, C.; Lordo, R.; Sucosky, M.S.; Boehm, R.; Brown, M.J. Evaluating the effectiveness of state specific lead-based paint hazard risk reduction laws in preventing recurring incidences of lead poisoning in children. Int. J. Hyg. Environ. Health 2016, 219, 110–117. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Exposure Science in the 21st Century: A Vision and a Strategy; National Research Council: Washington, DC, USA, 2012. [Google Scholar]
- Mielke, H.W.; Gonzales, C.R.; Powell, E.T.; Mielke, P.W., Jr. Spatiotemporal dynamic transformations of soil lead and children’s blood lead ten years after Hurricane Katrina: New grounds for primary prevention. Environ. Int. 2016. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Gonzales, C.R.; Powell, E.T.; Mielke, P.W., Jr. Spatiotemporal exposome dynamics of soil lead and children’s blood lead pre- and ten years post-Hurricane Katrina: Lead and other metals on public and private properties in the city of New Orleans, Louisiana, U.S.A. Environ. Res. 2017, 155, 208–218. [Google Scholar] [CrossRef] [PubMed]
- U.S. Bureau of the Census. Table 32: Selected Structural Characteristics of Housing Units: 1990; and Summary Tape File 3A. In Tracts and Block Numbering Areas. New Orleans, LA MSA; U.S. Bureau of the Census: Suitland, MD, USA, 1993. [Google Scholar]
- Mielke, H.W.; Gonzales, C.; Powell, E.; Mielke, P.W., Jr. Changes of multiple metal accumulation (MMA) in New Orleans soil: Preliminary evaluation of differences between Survey I (1992) and Survey II (2000). Int. J. Environ. Res. Public Health 2005, 2, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Dugas, D.; Mielke, P.W., Jr.; Smith, K.S.; Smith, S.L.; Gonzales, C.R. Associations between Soil Lead and Childhood Blood Lead in Urban New Orleans and Rural Lafourche Parish of Louisiana. Environ. Health Perspect. 1997, 105, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Final Report: Revised California Human Health Screening Levels for Lead and Beryllium. 17 September 2009. Available online: https://oehha.ca.gov/risk/soils091709 (accessed on 5 April 2017).
- Mielke, P.W., Jr.; Berry, K.J. Permutation Methods: A Distance Function Approach, 2nd ed.; Springer: New York, NY, USA, 2007; p. 439. [Google Scholar]
- Surfer® 8, Golden Software, Inc. Available online: http://www.goldensoftware.com/products/surfer (accessed on 13 December 2016).
- Patel, C.J.; Manra, A.K. Development of exposome correlation globes to map out environment-wide associations. Pac. Symp. Biocomput. 2015, 20, 231–242. [Google Scholar]
- U.S. DHHS (Department of Health and Human Services). National Toxicology Program. Monograph on Health Effects of Low-Level Lead. 2012. Available online: http://ntp.niehs.nih.gov/go/36443 (accessed on 5 April 2017).
- Campanella, R.; Mielke, H.W. Human geography of New Orleans’ urban soil lead contaminated geochemical setting. Environ. Geochem. Health 2008, 30, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Henderson, Y. Sees Deadly gas a peril in streets. New York Times (1923-Current File): ProQuest Historical Newspapers. The New York Times, 22 April 1925; 25. [Google Scholar]
- Datko-Williams, L.; Wilkie, A.; Richmond-Bryant, J. Analysis of U.S. soil lead (Pb) studies from 1970 to 2012. Sci. Total Environ. 2014, 468–469, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Gonzales, C.R.; Mielke, P.W., Jr. The continuing impact of lead dust on children’s blood lead: Comparison of public and private properties in New Orleans. Environ. Res. 2011, 111, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Laidlaw, M.A.S.; Gonzales, C.R. Estimation of leaded (Pb) gasoline’s continuing material and health impacts on 90 U.S. urbanized areas. Environ. Int. 2011, 37, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Gonzales, C.R.; Smith, M.K.; Mielke, P.W. Quantities and associations of lead, zinc, cadmium, manganese, chromium, nickel, vanadium, and copper in fresh Mississippi delta alluvium and New Orleans alluvial soils. Sci. Total Environ. 2000, 246, 249–259. [Google Scholar] [CrossRef]
- Mielke, H.W.; Wang, G.; Gonzales, C.R.; Powell, E.T.; Le, B.; Quach, V.N. PAHs and metals in the soils of inner-city and suburban New Orleans, LA, USA. Environ. Toxicol. Pharmacol. 2004, 18, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Powell, E.T.; Gonzales, C.R.; Mielke, P.W., Jr. Potential lead on play surfaces: Evaluation of the “PLOPS” sampler as a new tool for primary lead prevention. Environ. Res. 2007, 103, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Annest, J.L.; Pirkle, J.L.; Makuc, D.; Neese, J.W.; Bayse, D.D.; Kovar, M.G. Chronological trend in blood lead levels between 1976 and 1980. N. Engl. J. Med. 1983, 308, 1373–1377. [Google Scholar] [CrossRef] [PubMed]
- Laidlaw, M.A.S.; Zahran, S.; Mielke, H.W.; Taylor, M.P.; Filippelli, G.M. Re-suspension of lead contaminated urban soil as a dominant source of atmospheric lead in Birmingham, Chicago, Detroit and Pittsburgh, USA. Atmos. Environ. 2012, 49, 302–310. [Google Scholar] [CrossRef]
- Zahran, S.; Laidlaw, M.A.S.; McElmurry, S.P.; Filippelli, G.M.; Taylor, M. Linking source and effect: Resuspended soil lead, air lead, and children’s blood lead levels in Detroit, Michigan. Environ. Sci. Technol. 2013, 47, 2839–2845. [Google Scholar] [CrossRef] [PubMed]
- Filippelli, G.M.; Laidlaw, M.A.S. The Elephant in the Playground: Confronting lead-contaminated soils as an important source of lead burdens to urban populations. Perspect. Biol. Med. 2010, 53, 31–45. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Mielke, H.W.; Gonzales, C.R.; Powell, E.; Mielke, P.W. Environmental and health disparities in residential communities of New Orleans: The need for soil lead intervention to advance primary prevention. Environ. Int. 2013, 51, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Laidlaw, M.A.S.; Filippelli, G.M.; Brown, S.; Paz-Ferreiro, J.; Reichman, S.M.; Netherway, P.; Truskewycz, A.; Ball, A.S.; Mielke, H.W. Case studies and evidence-based approaches to addressing urban soil lead contamination. Appl. Geochem. 2017. [Google Scholar] [CrossRef]
- Mielke, H.W.; Covington, T.P.; Mielke, P.W.; Wolman, F.J.; Powell, E.T.; Gonzales, C.R. Soil intervention as a strategy for lead exposure prevention: The New Orleans lead-safe childcare playground project. Environ. Pollut. 2011, 159, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Gonzales, C.; Powell, E.; Mielke, P.W. Evolving from reactive to proactive medicine: Community lead (Pb) and clinical disparities in pre- and post-Katrina New Orleans. Int. J. Environ. Res. Public Health 2014, 11, 7482–7491. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, N.; Bølviken, B.; Smith, D.B.; Severson, R.C. Geochemical Landscapes of the Conterminous United States—New Map Presentations for 22 Elements. Professional Paper 1648; U.S. Geological Survey: Denver, CO, USA, 2001; p. 22.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Percentiles | Soil Lead (mg/kg) 172 CTs | Blood Lead (µg/dL) 172 CTs | ||
|---|---|---|---|---|
| Pre-Katrina | Post-Katrina | Pre-Katrina | Post-Katrina | |
| min | 11 | 10 | 3.0 | <1.0 |
| 5% | 26 | 16 | 3.0 | <1.0 |
| 10% | 41 | 24 | 3.0 | 1.0 |
| 25% | 85 | 44 | 3.4 | 1.2 |
| 50% | 289 | 143 | 5.0 | 1.9 |
| 75% | 559 | 307 | 6.5 | 2.5 |
| 90% | 806 | 419 | 7.4 | 3.0 |
| 95% | 1052 | 593 | 8.1 | 3.4 |
| max | 1789 | 1076 | 10.8 | 6.8 |
| N | 3238 | 3243 | 38,861 | 17,544 |
| p-value * | 1.12 × 10−21 | 6.95 × 10−37 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mielke, H.W.; Gonzales, C.R.; Powell, E.T. Soil Lead and Children’s Blood Lead Disparities in Pre- and Post-Hurricane Katrina New Orleans (USA). Int. J. Environ. Res. Public Health 2017, 14, 407. https://doi.org/10.3390/ijerph14040407
Mielke HW, Gonzales CR, Powell ET. Soil Lead and Children’s Blood Lead Disparities in Pre- and Post-Hurricane Katrina New Orleans (USA). International Journal of Environmental Research and Public Health. 2017; 14(4):407. https://doi.org/10.3390/ijerph14040407
Chicago/Turabian StyleMielke, Howard W., Christopher R. Gonzales, and Eric T. Powell. 2017. "Soil Lead and Children’s Blood Lead Disparities in Pre- and Post-Hurricane Katrina New Orleans (USA)" International Journal of Environmental Research and Public Health 14, no. 4: 407. https://doi.org/10.3390/ijerph14040407
APA StyleMielke, H. W., Gonzales, C. R., & Powell, E. T. (2017). Soil Lead and Children’s Blood Lead Disparities in Pre- and Post-Hurricane Katrina New Orleans (USA). International Journal of Environmental Research and Public Health, 14(4), 407. https://doi.org/10.3390/ijerph14040407