Prenatal Heavy Metal Exposure and Adverse Birth Outcomes in Myanmar: A Birth-Cohort Study

Abstract
1. Introduction
2. Methods
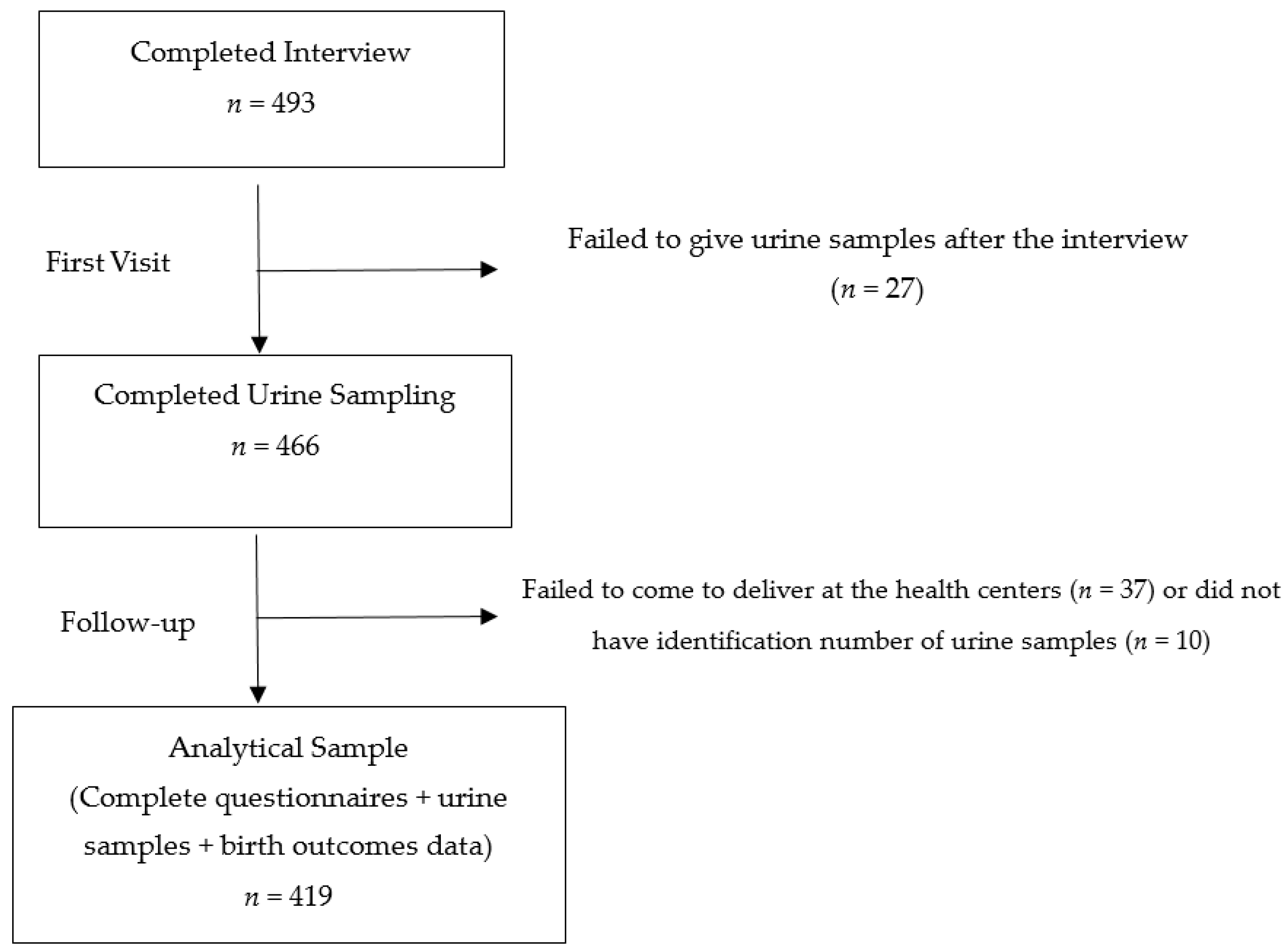
2.1. Study Design and Setting
2.2. Exposure Assessment
2.3. Measurement of Birth Outcomes and Other Covariates
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Vahter, M. Effects of arsenic on maternal and fetal health. Annu. Rev. Nutr. 2009, 29, 381–399. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Zhong, H.; Guo, Z.; Wu, Z.; Zhang, H.; Wang, C.; Zhou, Y.; Zuo, Z. Levels of heavy metals and trace elements in umbilical cord blood and the risk of adverse pregnancy outcomes: A population-based study. Biol. Trace Elem. Res. 2014, 160, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Quansah, R.; Armah, F.A.; Essumang, D.K.; Luginaah, I.; Clarke, E.; Marfoh, K.; Cobbina, S.J.; Nketiah-Amponsah, E.; Namujju, P.B.; Obiri, S.; et al. Association of arsenic with adverse pregnancy outcomes/infant mortality: A systematic review and meta-analysis. Environ. Health Perspect. 2015, 123, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Needham, L.L.; Grandjean, P.; Heinzow, B.; Jørgensen, P.J.; Nielsen, F.; Patterson, D.G.; Sjödin, A.; Turner, W.E.; Weihe, P. Partition of environmental chemicals between maternal and fetal blood and tissues. Environ. Sci. Technol. 2011, 45, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Caserta, D.; Graziano, A.; Lo Monte, G.; Bordi, G.; Moscarini, M. Heavy metals and placental fetal-maternal barrier: A mini-review on the major concerns. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 2198–2206. [Google Scholar] [PubMed]
- Chen, Z.; Myers, R.; Wei, T.; Bind, E.; Kassim, P.; Wang, G.; Ji, Y.; Hong, X.; Caruso, D.; Bartell, T.; et al. Placental transfer and concentrations of cadmium, mercury, lead, and selenium in mothers, newborns, and young children. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, I.; Shinwari, N.; Mashhour, A.; Rabah, A. Birth outcome measures and maternal exposure to heavy metals, (lead, cadmium and mercury) in Saudi Arabian population. Int. J. Hyg. Environ. Health 2014, 217, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Gundacker, C.; Hengstschläger, M. The role of the placenta in fetal exposure to heavy metals. Wien. Med. Wochenschr. 2012, 162, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Stasenko, S.; Bradford, E.M.; Piasek, M.; Henson, M.C.; Varnai, V.M.; Jurasović, J.; Kusec, V. Metals in human placenta: Focus on the effects of cadmium on steroid hormones and leptin. J. Appl. Toxicol. 2010, 30, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Potula, V.; Kaye, W. Report from the CDC. Is lead exposure a risk factor for bone loss? J. Womens Health 2005, 14, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Vahter, M.E. Interactions between arsenic-induced toxicity and nutrition in early life. J. Nutr. 2007, 137, 2798–2804. [Google Scholar] [PubMed]
- Sun, H.; Chen, W.; Wang, D.; Jin, Y.; Chen, X.; Xu, Y. The effects of prenatal exposure to low-level cadmium, lead and selenium on birth outcomes. Chemosphere 2014, 108, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Shirai, S.; Suzuki, Y.; Yoshinaga, J.; Mizumoto, Y. Maternal exposure to low-level heavy metals during pregnancy and birth size. J. Environ. Sci. Health A Toxic Hazard. Subst. Environ. Eng. 2010, 45, 1468–1474. [Google Scholar] [CrossRef] [PubMed]
- Laine, J.E.; Bailey, K.A.; Rubio-Andrade, M.; Olshan, A.F.; Smeester, L.; Drobná, Z.; Herring, A.H.; Stýblo, M.; García-Vargas, G.G.; Fry, R.C. Maternal arsenic exposure, arsenic methylation efficiency, and birth outcomes in the Biomarkers of Exposure to ARsenic (BEAR) pregnancy cohort in Mexico. Environ. Health Perspect. 2015, 123, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Fitzgerald, E.F.; Gelberg, K.H.; Lin, S.; Druschel, C.M. Maternal low-level lead exposure and fetal growth. Environ. Health Perspect. 2010, 118, 1471–1475. [Google Scholar] [CrossRef] [PubMed]
- Kippler, M.; Wagatsuma, Y.; Rahman, A.; Nermell, B.; Persson, L.; Raqib, R.; Vahter, M. Environmental exposure to arsenic and cadmium during pregnancy and fetal size: A longitudinal study in rural Bangladesh. Reprod. Toxicol. 2012, 34, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Chang, C.C.; Tsai, S.S.; Chuang, H.Y.; Ho, C.K.; Wu, T.N. Arsenic in drinking water and adverse pregnancy outcome in an arseniasis-endemic area in northeastern Taiwan. Environ. Res. 2003, 91, 29–34. [Google Scholar] [CrossRef]
- Yang, J.; Huo, W.; Zhang, B.; Zheng, T.; Li, Y.; Pan, X.; Liu, W.; Chang, H.; Jiang, M.; Zhou, A.; et al. Maternal urinary cadmium concentrations in relation to preterm birth in the Healthy Baby Cohort Study in China. Environ. Int. 2016, 94, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Xia, W.; Li, Y.; Bassig, B.A.; Zhou, A.; Wang, Y.; Li, Z.; Yao, Y.; Hu, J.; Du, X.; et al. Prenatal exposure to lead in relation to risk of preterm low birth weight: A matched case-control study in China. Reprod. Toxicol. 2015, 57, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Persson, L.; Nermell, B.; El Arifeen, S.; Ekström, E.C.; Smith, A.H.; Vahter, M. Arsenic exposure and risk of spontaneous abortion, stillbirth, and infant mortality. Epidemiology 2010, 21, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef]
- World Health Organization (WHO); United Nations Children’s Fund (UNICEF). Low Birth Weight: Country, Regional and Global Estimate; United Nations Children’s Fund (UNICEF): New York, NY, USA, 2004. [Google Scholar]
- Beck, S.; Wojdyla, D.; Say, L.; Betran, A.P.; Merialdi, M.; Requejo, J.H.; Rubens, C.; Menon, R.; Van Look, P.F. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull. World Health Organ. 2010, 88, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Lawn, J.E.; Wilczynska-Ketende, K.; Cousens, S.N. Estimating the causes of 4 million neonatal deaths in the year 2000. Int. J. Epidemiol. 2006, 35, 706–718. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Sports (MOHS); ICF International. Demographic and Health Survey 2015–2016: Key Indicators Report. In Myanmar Demographic and Health Survey (DHS); Ministry of Health and Sports (MOHS): Naypyidaw, Myanmar; The DHS Program ICF International: Rockville, MD, USA, 2016. [Google Scholar]
- Van Geen, A.; Win, K.H.; Zaw, T.; Naing, W.; Mey, J.L.; Mailloux, B. Confirmation of elevated arsenic levels in groundwater of Myanmar. Sci. Total Environ. 2014, 478, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Tun, T.N. Arsenic contamination of water sources in rural Myanmar. In Proceedings of the 29th WEDC International Conference towards the Millennium Development Goals, Abuja, Nigeria, 22–26 September 2003; pp. 219–221. [Google Scholar]
- Ministry of Health (MOH); The United Nations Children’s Fund (Unicef). An Analysis of Arsenic Content in Drinking Water Sources of Ayeyarwaddy Region; MOH: Naypyidaw, Myanmar, 2013.
- Bacquart, T.; Frisbie, S.; Mitchell, E.; Grigg, L.; Cole, C.; Small, C.; Sarkar, B. Multiple inorganic toxic substances contaminating the groundwater of Myingyan Township, Myanmar: Arsenic, manganese, fluoride, iron, and uranium. Sci. Total Environ. 2015, 517, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Brammer, H.; Ravenscroft, P. Arsenic in groundwater: A threat to sustainable agriculture in South and South-east Asia. Environ. Int. 2009, 35, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Soe Minn Htway, O.; Mya Aye, T.; Khin Tar Yar, M.; Mar Mar, M. Cardiovascular Risk in People with Chronic Exposure to Low Level of Arsenic Contamination in Drinking Water. Myanmar Health Sci. Res. J. 2014, 26, 159–165. [Google Scholar]
- New, M.S.; Oo, T.; Htut, T. Relationship between blood arsenic level, blood pressure and creatinine clearance in subjects living in Kyaungone Township, Ayeyawaddy Division. Myanmar Health Sci. Res. J. 2010, 22, 170–176. [Google Scholar]
- Ministry of Health and Sports (MOHS). Health in Myanmar 2014; Ministry of Health and Sports, The Republic of the Union of Myanmar: Naypyidaw, Myanmar, 2014.
- Huang, K.; Li, H.; Zhang, B.; Zheng, T.; Li, Y.; Zhou, A.; Du, X.; Pan, X.; Yang, J.; Wu, C.; et al. Prenatal cadmium exposure and preterm low birth weight in China. J. Expo. Sci. Environ. Epidemiol. 2016, 27, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Engström, K.; Vahter, M.; Broberg, K. Arsenic exposure through drinking water is associated with longer telomeres in peripheral blood. Chem. Res. Toxicol. 2012, 25, 2333–2339. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Roy, S.; Tong, L.; Argos, M.; Jasmine, F.; Rahaman, R.; Rakibuz-Zaman, M.; Parvez, F.; Ahmed, A.; Hore, S.K.; et al. Arsenic exposure, telomere length, and expression of telomere-related genes among Bangladeshi individuals. Environ. Res. 2015, 136, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Fillman, T.; Shimizu-Furusawa, H.; Ng, C.F.; Parajuli, R.P.; Watanabe, C. Association of cadmium and arsenic exposure with salivary telomere length in adolescents in Terai, Nepal. Environ. Res. 2016, 149, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, D.; Bhattacharjee, P.; Sau, T.J.; Das, J.K.; Sarma, N.; Bandyopadhyay, A.K.; Roy, S.S.; Giri, A.K. Arsenic exposure through drinking water leads to senescence and alteration of telomere length in humans: A case-control study in West Bengal, India. Mol. Carcinog. 2014, 54, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.E.; Valentiner, E.; Maxson, P.; Miranda, M.L.; Fry, R.C. Maternal cadmium levels during pregnancy associated with lower birth weight in infants in a North Carolina cohort. PLoS ONE 2014, 9, e109661. [Google Scholar] [CrossRef] [PubMed]
- Röllin, H.B.; Kootbodien, T.; Channa, K.; Odland, J. Prenatal Exposure to Cadmium, Placental Permeability and Birth Outcomes in Coastal Populations of South Africa. PLoS ONE 2015, 10, e0142455. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, V.; Woittiez, J. Trace elements in human clinical specimens: Evaluation of literature data to identify reference values. Clin. Chem. 1988, 34, 474–481. [Google Scholar] [PubMed]
- Moon, C.S.; Paik, J.M.; Choi, C.S.; Kim, D.H.; Ikeda, M. Lead and cadmium levels in daily foods, blood and urine in children and their mothers in Korea. Int. Arch. Occup. Environ. Health 2003, 76, 282–288. [Google Scholar] [PubMed]
- Shimbo, S.; Zhang, Z.W.; Watanabe, T.; Nakatsuka, H.; Matsuda-Inoguchi, N.; Higashikawa, K.; Ikeda, M. Cadmium and lead contents in rice and other cereal products in Japan in 1998–2000. Sci. Total Environ. 2001, 281, 165–175. [Google Scholar] [CrossRef]
- Fu, J.; Zhou, Q.; Liu, J.; Liu, W.; Wang, T.; Zhang, Q.; Jiang, G. High levels of heavy metals in rice (Oryza sativa L.) from a typical E-waste recycling area in southeast China and its potential risk to human health. Chemosphere 2008, 71, 1269–1275. [Google Scholar] [CrossRef] [PubMed]
- Tsukahara, T.; Ezaki, T.; Moriguchi, J.; Furuki, K.; Shimbo, S.; Matsuda-Inoguchi, N.; Ikeda, M. Rice as the most influential source of cadmium intake among general Japanese population. Sci. Total Environ. 2003, 305, 41–51. [Google Scholar] [CrossRef]
- Rahman, A.; Vahter, M.; Smith, A.H.; Nermell, B.; Yunus, M.; El Arifeen, S.; Persson, L.A.; Ekström, E.C. Arsenic exposure during pregnancy and size at birth: A prospective cohort study in Bangladesh. Am. J. Epidemiol. 2009, 169, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Kippler, M.; Tofail, F.; Gardner, R.; Rahman, A.; Hamadani, J.D.; Bottai, M.; Vahter, M. Maternal cadmium exposure during pregnancy and size at birth: A prospective cohort study. Environ. Health Perspect. 2012, 120, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Murphy, V.E.; Smith, R.; Giles, W.B.; Clifton, V.L. Endocrine regulation of human fetal growth: The role of the mother, placenta, and fetus. Endocr. Rev. 2006, 27, 141–169. [Google Scholar] [CrossRef] [PubMed]
- Kippler, M.; Hoque, A.M.; Raqib, R.; Ohrvik, H.; Ekström, E.C.; Vahter, M. Accumulation of cadmium in human placenta interacts with the transport of micronutrients to the fetus. Toxicol. Lett. 2010, 192, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Iijima, K.; Otake, T.; Yoshinaga, J.; Ikegami, M.; Suzuki, E.; Naruse, H.; Yamanaka, T.; Shibuya, N.; Yasumizu, T.; Kato, N. Cadmium, lead, and selenium in cord blood and thyroid hormone status of newborns. Biol. Trace Elem. Res. 2007, 119, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Jaquet, D.; Leger, J.; Levy-Marchal, C.; Oury, J.F.; Czernichow, P. Ontogeny of leptin in human fetuses and newborns: Effect of intrauterine growth retardation on serum leptin concentrations. J. Clin. Endocrinol. Metab. 1998, 83, 1243–1246. [Google Scholar] [CrossRef] [PubMed]
- Chertok, R.J.; Kullgren, B.; Burbank, D. The effects of CdCl2 on the maternal-to-fetal clearance of 67Cu and placental blood flow. Proc. Soc. Exp. Biol. Med. 1984, 176, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Wier, P.J.; Miller, R.K.; Maulik, D.; DiSant’Agnese, P.A. Toxicity of cadmium in the perfused human placenta. Toxicol. Appl. Pharmacol. 1990, 105, 156–171. [Google Scholar] [CrossRef]
- Thomas, S.; Arbuckle, T.E.; Fisher, M.; Fraser, W.D.; Ettinger, A.; King, W. Metals exposure and risk of small-for-gestational age birth in a Canadian birth cohort: The MIREC study. Environ. Res. 2015, 140, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Cantonwine, D.; Hu, H.; Sánchez, B.N.; Lamadrid-Figueroa, H.; Smith, D.; Ettinger, A.S.; Mercado-García, A.; Hernández-Avila, M.; Wright, R.O.; Téllez-Rojo, M.M. Critical windows of fetal lead exposure: Adverse impacts on length of gestation and risk of premature delivery. J. Occup. Environ. Med. 2010, 52, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Nishijo, M.; Nakagawa, H.; Honda, R.; Tanebe, K.; Saito, S.; Teranishi, H.; Tawara, K. Effects of maternal exposure to cadmium on pregnancy outcome and breast milk. Occup. Environ. Med. 2002, 59, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Fagher, U.; Laudanski, T.; Schütz, A.; Sipowicz, M.; Akerlund, M. The relationship between cadmium and lead burdens and preterm labor. Int. J. Gynaecol. Obstet. 1993, 40, 109–114. [Google Scholar] [CrossRef]
- Chen, P.C.; Pan, I.J.; Wang, J.D. Parental exposure to lead and small for gestational age births. Am. J. Ind. Med. 2006, 49, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Jaishankar, M.; Tseten, T.; Anbalagan, N.; Mathew, B.B.; Beeregowda, K.N. Toxicity, mechanism and health effects of some heavy metals. Interdiscip. Toxicol. 2014, 7, 60–72. [Google Scholar]
- Godfrey, K.; Robinson, S.; Barker, D.J.; Osmond, C.; Cox, V. Maternal nutrition in early and late pregnancy in relation to placental and fetal growth. BMJ 1996, 312, 410–414. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | n | % | Mean | SD |
|---|---|---|---|---|
| Age (years) | 419 | 27.9 | 6.6 | |
| Religion | ||||
| Buddhist | 376 | 89.7 | ||
| Christian | 41 | 9.8 | ||
| Others | 2 | 0.5 | ||
| Ethnicity | ||||
| Bamar | 311 | 74.2 | ||
| National ethnic groups † | 106 | 25.3 | ||
| Others | 2 | 0.5 | ||
| Education | ||||
| Illiterate | 7 | 1.7 | ||
| Able to read and write | 66 | 15.8 | ||
| Primary school completed | 193 | 46.1 | ||
| Middle school completed | 81 | 19.3 | ||
| High school completed | 44 | 10.5 | ||
| Graduate and above | 28 | 6.9 | ||
| Occupation | ||||
| Unemployed or housewives | 176 | 41.9 | ||
| Farmers | 152 | 36.3 | ||
| Private Sectors | 8 | 1.9 | ||
| Government officers | 14 | 3.3 | ||
| Own business | 32 | 7.6 | ||
| Others | 37 | 8.8 | ||
| Hospitals | ||||
| Kyaungone | 153 | 36.5 | ||
| Kyonpyaw | 139 | 33.2 | ||
| Ahtaung | 127 | 30.3 | ||
| Monthly household income # (USD) | 296 | 124.2 | 55.7 | |
| Smoking Status | ||||
| Not at all | 210 | 50.1 | ||
| Have or ever been or passively exposed | 209 | 49.9 | ||
| Characteristics | n | % | Mean | SD |
|---|---|---|---|---|
| Gestational age (weeks) | 419 | 38.0 | 2.4 | |
| Primigravida | ||||
| No | 181 | 43.2 | ||
| Yes | 238 | 56.8 | ||
| Antenatal visits | ||||
| Less than four times | 136 | 32.5 | ||
| Four or more than four times | 283 | 67.5 | ||
| Gestational week of first antenatal visit | 419 | 15.6 | 6.1 | |
| Mode of delivery | ||||
| Normal spontaneous delivery | 188 | 44.9 | ||
| Assisted delivery γ | 7 | 1.7 | ||
| Cesarean delivery | 224 | 53.5 | ||
| Baby’s sex | ||||
| Male | 238 | 56.8 | ||
| Female | 181 | 43.2 | ||
| Birth weight (g) | 419 | 3171.7 | 493.0 | |
| Birth outcomes | ||||
| Normal alive | 329 | 78.5 | ||
| Still-birth | 2 | 0.5 | ||
| Preterm θ | 80 | 19.1 | ||
| Congenital abnormality | 2 | 0.5 | ||
| Low birth weight † | 26 | 6.2 | ||
| Adjusted Urinary Heavy Metal Concentration (μg/g Creatinine) | Median | IQR |
|---|---|---|
| Arsenic | 74 | (45–127) |
| Cadmium | 0.86 | (0.50–1.40) |
| Selenium | 23 | (18–30) |
| Lead | 1.8 | (1.0–3.3) |
| Adjusted Urinary Heavy Metal Concentration (μg/g Creatinine) | Preterm Delivery θ | Low Birth Weight † | Preterm and Low Birth Weight | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 80) | No (n = 339) | p-Value | Yes (n = 26) | No (n = 393) | p-Value | Yes (n = 18) | No (n = 401) | p-Value | |
| Arsenic | 73.2 | 74.2 | 1.000 | 89.0 | 73.8 | 0.500 | 84.2 | 73.9 | 0.490 |
| Cadmium | 0.8 | 0.8 | 0.743 | 1.4 | 0.8 | 0.020 | 1.4 | 0.8 | 0.014 |
| Selenium | 22.4 | 22.7 | 0.940 | 20.6 | 22.7 | 0.998 | 19.3 | 22.7 | 0.324 |
| Lead | 1.7 | 1.8 | 0.729 | 1.5 | 1.8 | 0.117 | 1.5 | 1.8 | 0.236 |
| Characteristics | Crude OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|
| Maternal age (years) | 0.99 (0.93–1.05) | 1.04 (0.96–1.11) |
| Maternal education | 0.67 (0.45–1.01) | 0.72 (0.46–1.13) |
| Gestational age (weeks) | 0.79 (0.69–0.90) *** | 0.83 (0.72–0.95) ** |
| Primigravida (ref: non-primigravida) | 2.16 (0.89–5.25) * | 4.23 (1.31–13.65) * |
| Antenatal visit ≥4 times (ref: <4 times) | 0.54 (0.24–1.20) | 0.55 (0.22–1.36) |
| Cesarean section or assisted delivery (ref: normal vaginal delivery) | 0.68 (0.31–1.51) | 0.67 (0.28–1.63) |
| Baby’s sex (ref: male) | 1.58 (0.71–3.50) | 1.60 (0.67–3.85) |
| Have or ever been or passively exposed to smoking (ref: no exposure) | 1.01 (0.42–2.22) | 0.76 (0.32–1.82) |
| Arsenic concentration (μg/g creatinine) | 1.00 (0.99–1.00) | 0.99 (0.99–1.00) |
| Cadmium concentration (μg/g creatinine) | 1.01 (1.02–1.19) * | 1.10 (1.01–1.21) * |
| Selenium concentration (μg/g creatinine) | 1.02 (0.99–1.04) | 1.02 (0.99–1.06) |
| Lead concentration (μg/g creatinine) | 0.85 (0.67–1.08) | 0.76 (0.57–1.03) |
| Characteristics | Crude OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|
| Maternal age (years) | 0.99 (0.96–1.04) | 1.02 (0.97–1.07) |
| Maternal education | 0.88 (0.70–1.10) | 0.92 (0.72–1.19) |
| Birth weight (grams) | 1.00 (0.997–0.999) *** | 0.52 (0.44–0.62) *** |
| Primigravida (ref: non-primigravida) | 1.34 (0.81–2.21) | 1.30 (0.66–2.57) |
| Antenatal visit ≥4 times (ref: <4 times) | 1.24 (0.73–2.11) | 1.59 (0.88–2.89) |
| Cesarean section or assisted delivery (ref: normal vaginal delivery) | 0.41 (0.25–0.68) ** | 0.40 (0.23–0.70) * |
| Baby’s sex (ref: male) | 1.24 (0.76–2.02) | 1.17 (0.68–2.00) |
| Have or ever been or passively exposed to smoking (ref: no exposure) | 1.56 (0.95–2.55) | 1.56 (0.91–2.69) |
| Arsenic concentration (μg/g creatinine) | 1.00 (0.99–1.00) | 1.00 (0.99–1.00) |
| Cadmium concentration (μg/g creatinine) | 1.06 (0.98–1.14) | 1.05 (0.97–1.13) |
| Selenium concentration (μg/g creatinine) | 0.99 (0.98–1.02) | 0.99 (0.96–1.01) |
| Lead concentration (μg/g creatinine) | 0.96 (0.87–1.05) | 0.98 (0.89–1.07) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wai, K.M.; Mar, O.; Kosaka, S.; Umemura, M.; Watanabe, C. Prenatal Heavy Metal Exposure and Adverse Birth Outcomes in Myanmar: A Birth-Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1339. https://doi.org/10.3390/ijerph14111339
Wai KM, Mar O, Kosaka S, Umemura M, Watanabe C. Prenatal Heavy Metal Exposure and Adverse Birth Outcomes in Myanmar: A Birth-Cohort Study. International Journal of Environmental Research and Public Health. 2017; 14(11):1339. https://doi.org/10.3390/ijerph14111339
Chicago/Turabian StyleWai, Kyi Mar, Ohn Mar, Satoko Kosaka, Mitsutoshi Umemura, and Chiho Watanabe. 2017. "Prenatal Heavy Metal Exposure and Adverse Birth Outcomes in Myanmar: A Birth-Cohort Study" International Journal of Environmental Research and Public Health 14, no. 11: 1339. https://doi.org/10.3390/ijerph14111339
APA StyleWai, K. M., Mar, O., Kosaka, S., Umemura, M., & Watanabe, C. (2017). Prenatal Heavy Metal Exposure and Adverse Birth Outcomes in Myanmar: A Birth-Cohort Study. International Journal of Environmental Research and Public Health, 14(11), 1339. https://doi.org/10.3390/ijerph14111339