
Fairness and Eligibility to Long-Term Care: An Analysis of the Factors Driving Inequality and Inequity in the Use of Home Care for Older Europeans


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Statistics
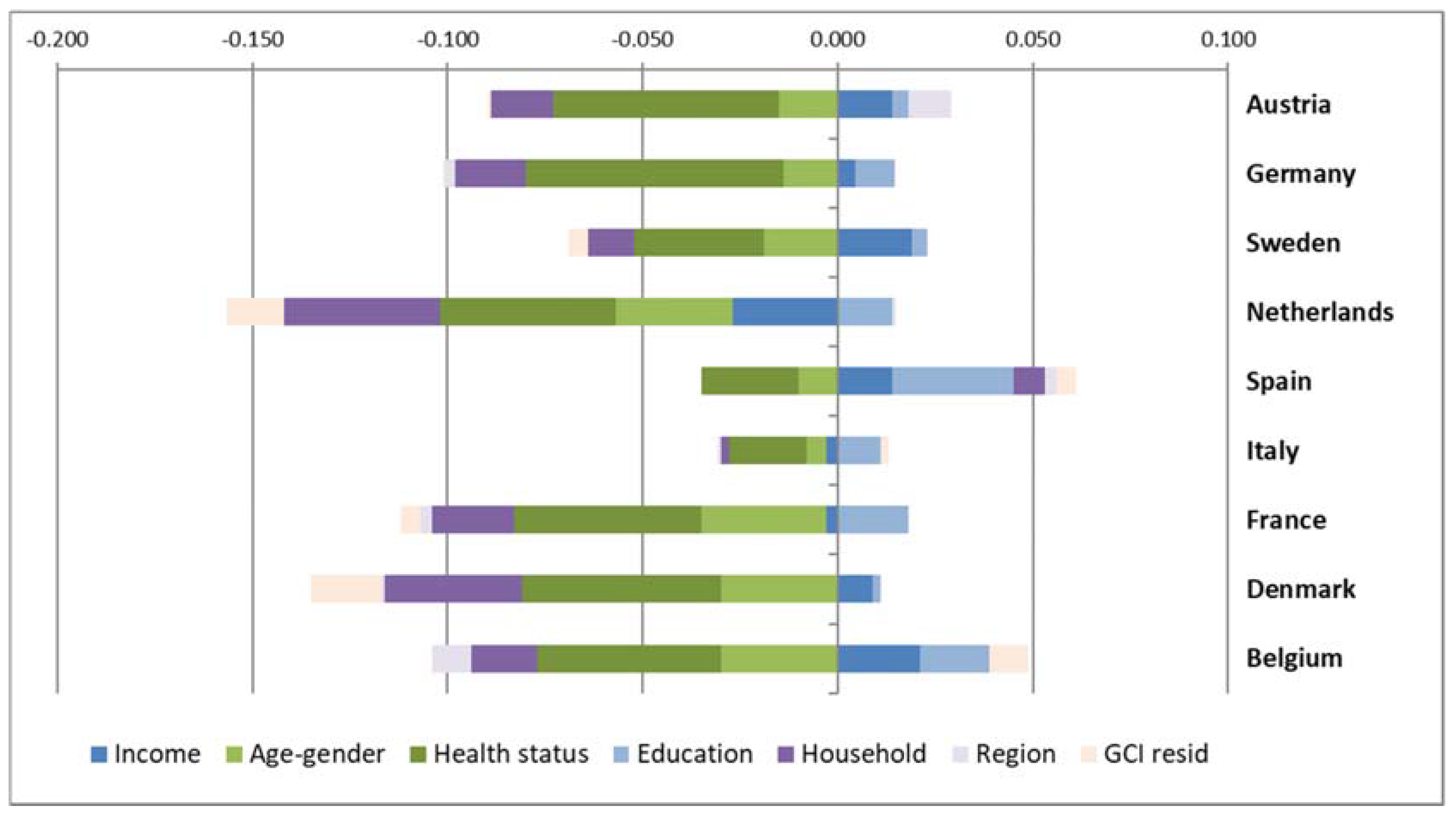
3.2. Analysis of Inequality in Access to Home Care
3.3. Inequity Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Colombo, F.; Llena-Nozal, A.; Mercier, J.; Tjadens, F. Help Wanted? Providing and Paying for Long-Term Care; OECD Publishing: Paris, France, 2011. [Google Scholar]
- Bakx, P.; de Meijer, C.; Schut, F.T.; van Doorslaer, E. Going Formal or Informal, Who Cares? The Influence of Public Long-term Care Insurance. Health Econ. 2015, 24, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Albertini, M.; Pavolini, E. Unequal Inequalities: The Stratification of the Use of Formal Care Among Older Europeans. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2015, 72, 510–521. [Google Scholar] [CrossRef] [PubMed]
- Van Doorslaer, E.; Koolman, X.; Jones, A.M. Explaining income-related inequalities in doctor utilisation in Europe. Health Econ. 2004, 13, 629–647. [Google Scholar] [CrossRef] [PubMed]
- Bago d’Uva, T.; Jones, A.M.; van Doorslaer, E. Measurement of horizontal inequity in health care utilisation using European panel data. J. Health Econ. 2009, 28, 280–289. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Health Inequalities in the EU—Final Report of a Consortium; Consortium lead: Sir Michael Marmot; European Commission, DG Health and Consumers: Brussels, Belgium, 2013. [Google Scholar]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bambra, C. Cash Versus Services: “Worlds of Welfare” and the Decommodification of Cash Benefits and Health Care Services. J. Soc. Policy 2005, 34, 195–213. [Google Scholar] [CrossRef]
- Jensen, C. Worlds of welfare services and transfers. J. Eur. Soc. Policy 2008, 18, 151–162. [Google Scholar] [CrossRef]
- The Organisation for Economic Co-operation and Development (OECD); World Health Organization (WHO). Poverty and Health—DAC Guidelines and Reference Series; OECD Publishing: Paris, France, 2003. [Google Scholar]
- Paraponaris, A.; Bérengè, D.; Verger, P. Formal and informal care for disabled elderly living in the community: An appraisal of French care composition and costs. Eur. J. Health Econ. 2011. [Google Scholar] [CrossRef] [PubMed]
- Geerlings, S.W.; Pot, A.M.; Twisk, J.W.R.; Deeg, D. Predicting transitions in the use of informal and professional care by older adults. Ageing Soc. 2005, 25, 111–130. [Google Scholar] [CrossRef] [Green Version]
- Hoeck, S.; François, G.; Geerts, J.; Van der Heyden, J.; Vandewoude, M.; Van Hal, G. Health-Care and Home-Care Utilization among Frail Elderly Persons in Belgium Health-care and home-care utilization among frail elderly persons in Belgium. Eur. J. Public Health 2011, 22, 671–676. [Google Scholar] [CrossRef] [PubMed]
- García-Gómez, P.; Hernández-Quevedo, C.; Jiménez-Rubio, D.; Oliva-Moreno, J. Inequity in long-term care use and unmet need: Two sides of the same coin. J. Health Econ. 2015, 39, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, M. Use of informal and formal care among community dwelling dependent elderly in Spain. Eur. J. Public Health 2013, 24, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Larsson, K.; Silverstein, M. The effects of marital and parental status on informal support and service utilization: A study of older Swedes living alone. J. Aging Stud. 2004, 18, 231–244. [Google Scholar] [CrossRef]
- Meinow, B.; Kåreholt, I.; Lagergren, M. According to need? Predicting the amount of municipal home help allocated to elderly recipients in an urban area of Sweden. Health Soc. Care Community 2005, 13, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.E. Analysing the importance of older people’s resources for the use of home care in a cash-for-care scheme: Evidence from Vienna. Health Soc. Care Community 2017, 25, 514–526. [Google Scholar] [CrossRef] [PubMed]
- Motel-Klingebiel, A.; Tesch-Roemer, C.; Von Kondratowitz, H.-J. Welfare states do not crowd out the family: Evidence for mixed responsibility from comparative analyses. Ageing Soc. 2005, 25, 863. [Google Scholar] [CrossRef]
- Van Broese Groenou, M.; Glaser, K.; Tomassini, C.; Jacobs, T. Socio-economic status differences in older people’s use of informal and formal help: A comparison of four European countries. Ageing Soc. 2006, 26, 745. [Google Scholar] [CrossRef]
- Blinkert, B.; Klie, T. Der Einfluss von Bedarf und Chancen auf Pflegezeiten in haeuslichen Pflegearrangements. Z. Gerontol. Geriatr. 2006, 39, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.E. Older Persons’ Views on Using Cash-for-Care Allowances at the Crossroads of Gender, Socio-economic Status and Care Needs in Vienna. Soc. Policy Adm. 2017. [Google Scholar] [CrossRef]
- Auslander, G.K.; Litwin, H. Social support networks and formal help seeking: Differences between applicants to social services and a nonapplicant sample. J. Gerontol. 1990, 45, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Lamura, G.; Mnich, E.; Nolan, M.; Wojszel, B.; Krevers, B.; Mestheneos, L.; Döhner, H.; EUROFAMCARE Group. Family carers’ experiences using support services in Europe: Empirical evidence from the EUROFAMCARE study. Gerontologist 2008, 48, 752–771. [Google Scholar] [CrossRef] [PubMed]
- Weyers, S.; Dragano, N.; Möbus, S.; Beck, E.M.; Stang, A.; Möhlenkamp, S.; Jöckel, K.H.; Erbel, R.; Sieqrist, J. Low socio-economic position is associated with poor social networks and social support: Results from the Heinz Nixdorf Recall Study. Int. J. Equity Health 2008, 7. [Google Scholar] [CrossRef] [PubMed]
- Gray, A. The social capital of older people. Ageing Soc. 2009, 29, 5–31. [Google Scholar] [CrossRef]
- Van Broese Groenou, M.; van Tilburg, T. Network size and support in old age: Differentials by socio-economic status in childhood and adulthood. Ageing Soc. 2003, 23, 625–645. [Google Scholar] [CrossRef]
- Da Roit, B. Changing Intergenerational Solidarities within Families in a Mediterranean Welfare State. Curr. Sociol. 2007, 55, 251–269. [Google Scholar] [CrossRef]
- Sarasa, S.; Bilingsley, S. Personal and household care giving from adult children to parents and social stratification. In Families, Ageing and Social Policy; Saraceno, C., Ed.; Edward Elgar: Cheltenham, UK, 2008; pp. 123–146. [Google Scholar]
- Fernandez, J.L.; Forder, J.E. Local variability in long-term care services: Local autonomy, exogenous influences and policy spillovers. Health Econ. 2015, 24 (Suppl. 1), 146–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demaerschalk, M.F.; Boer, L.E.; Vanden, B.L.E.; Bronselaer, J.L.; Molenberghs, G. The influence of municipal characteristics on the use of informal home care and home care services by the elderly Flemish. Eur. J. Public Health 2012, 23, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Lagergren, M.; Fagerström, C.; Sjölund, B.M.; Berglund, J.; Fratiglioni, L.; Nordell, E.; von Staruss, E.; Wimo, A.; Elmståhl, S. Horizontal and vertical targeting: A population-based comparison of public eldercare services in urban and rural areas of Sweden. Aging Clin. Exp. Res. 2016, 28, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Pulkki, J.; Jylha, M.; Forma, L.; Aaltonen, M.; Raitanen, J.; Rissanen, P. Long-term care use among old people in their last 2 years of life: Variations across Finland. Health Soc. Care Community 2016, 24, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Duell, D.; Koolman, X.; Portrait, F. Practice variation in the Dutch long-term care and the role of supply—Sensitive care: Is access to the Dutch long-term care equitable? Health Econ. 2017, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fleurbaey, M.; Schokkaert, E. Unfair inequalities in health and health care. J. Health Econ. 2009, 28, 73–90. [Google Scholar] [CrossRef] [PubMed]
- Cohen, G.A. On the Currency of Egalitarian Justice. Ethics 1989, 99, 906–944. [Google Scholar] [CrossRef]
- Dannefer, D. Cumulative Advantage/Disadvantage and the Life Course: Cross-Fertilizing Age and Social Science Theory. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, S327–S337. [Google Scholar] [CrossRef]
- Ferraro, K.F.; Shippee, T.P. Aging and Cumulative Inequality: How Does Inequality Get Under the Skin? Gerontologist 2004, 49, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Hammar, T.; Rissanen, P.; Perälä, M.-L. Home-care clients’ need for help, and use and costs of services. Eur. J. Ageing 2008, 5, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.; Paci, P.; van Doorslaer, E. On the measurement of inequalities in health. Soc. Sci. Med. 1991, 33, 545–557. [Google Scholar] [CrossRef]
- Wagstaff, A.; van Doorslaer, E. Measuring and testing for inequity in the delivery of health care. J. Hum. Resour. 2000, 35, 716–733. [Google Scholar] [CrossRef]
- Erreygers, G. Correcting the Concentration Index. J. Health Econ. 2009, 28, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.; van Doorslaer, E.; Watanabe, N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J. Econom. 2003, 112, 207–223. [Google Scholar] [CrossRef]
- O’Donnell, O.; van Doorslaer, E.; Wagstaff, A.; Lindelow, M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation; The World Bank: Washington, DC, USA, 2008. [Google Scholar]
- Van de Poel, E.; van Doorslaer, E.; O’Donnell, O. Measurement of inequity in health care with heterogeneous response of use to need. J. Health Econ. 2012, 31, 676–689. [Google Scholar] [CrossRef] [PubMed]
- Börsch-Supan, A.; Jürges, H. The Survey of Health, Aging, and Retirement in Europe: Methodology; Mannheim Research Institute for the Economics of Aging: Mannheim, Germany, 2005. [Google Scholar]
- SHARE Wave 5: Innovations & Methodology; Malter, F.; Börsch-Supan, A. (Eds.) MEA, Max Planck Institute for Social Law and Social Policy: Munich, Germany, 2015. [Google Scholar]
- De Luca, G.; Celidoni, M.; Trevisan, E. Item non response and imputation strategies in SHARE Wave 5. In SHARE Wave 5: Innovations & Methodology; Malter, F., Börsch-Supan, A., Eds.; MEA, Max Planck Institute for Social Law and Social Policy: Munich, Germany, 2015. [Google Scholar]
- The Organisation for Economic Co-operation and Development (OECD). Fostering Innovation to Address Social Challenges—Workshop Proceedings; OECD Publishing: Paris, France, 2011; pp. 1–99. [Google Scholar]
- Bonsang, E. Does informal care from children to their elderly parents substitute for formal care in Europe? J. Health Econ. 2009, 28, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Bolin, K.; Lindgren, B.; Lundborg, P. Informal and formal care among single-living elderly in Europe. Health Econ. 2008, 17, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Genet, N.; Boerma, W.; Kroneman, M.; Hutchinson, A.; Saltman, R.B. Home Care across Europe; European Observatory on Health Systems and Policies: Utrecht, The Netherlands, 2013. [Google Scholar]
- Sadana, R.; Blas, E.; Budhwani, S.; Koller, T.; Paraje, G. Healthy Ageing: Raising Awareness of Inequalities, Determinants, and What Could Be Done to Improve Health Equity. Gerontologist 2016, 56, 178–193. [Google Scholar] [CrossRef] [PubMed]
- Read, S.; Grundy, E.; Foverskov, E. Socio-economic position and subjective health and well-being among older people in Europe: A systematic narrative review. Aging Ment. Health 2017, 20, 529–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Houtven, C.H.; Norton, E.C. Informal care and health care use of older adults. J. Health Econ. 2004, 23, 1159–1180. [Google Scholar] [CrossRef] [PubMed]
- Bremer, P.; Challis, D.; Hallberg, I.R.; Leino-Kilpi, H.; Saks, K.; Vellas, B.; Zwakhalen, S.M.G.; Sauerland, D. RightTimePlaceCare Consortium. Informal and formal care: Substitutes or complements in care for people with dementia? Empirical evidence for 8 European countries. Health Policy 2017, 121, 613–622. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| AT | DE | SE | NL | ES | IT | FR | DK | BE | |
|---|---|---|---|---|---|---|---|---|---|
| Age (in years), 60+ | 70.99 | 70.40 | 71.13 | 70.28 | 72.90 | 71.41 | 71.74 | 70.63 | 71.25 |
| (7.70) | (7.62) | (7.73) | (7.64) | (8.83) | (7.72) | (8.67) | (7.96) | (8.34) | |
| Female (%) | 56.63 | 50.34 | 51.85 | 52.67 | 52.66 | 52.39 | 56.38 | 52.14 | 53.58 |
| (49.56) | (50.00) | (49.97) | (49.93) | (49.93) | (49.94) | (49.60) | (49.96) | (49.88) | |
| Less than good self-rated health (%) | 35.33 | 44.40 | 26.11 | 31.38 | 48.89 | 49.78 | 41.23 | 24.55 | 30.45 |
| (47.81) | (49.69) | (43.93) | (46.41) | (49.99) | (50.00) | (49.23) | (43.05) | (46.02) | |
| Has moderate ADL limitations (%) | 7.91 | 8.17 | 6.50 | 5.75 | 7.87 | 9.63 | 11.10 | 7.43 | 13.85 |
| (26.9) | (27.40) | (24.66) | (23.29) | (26.93) | (29.51) | (31.42) | (26.23) | (34.55) | |
| Has severe ADL limitations (%) | 3.95 | 3.84 | 1.74 | 1.48 | 7.56 | 5.77 | 3.39 | 2.07 | 3.99 |
| (19.50) | (19.22) | (13.05) | (12.11) | (26.44) | (23.33) | (18.11) | (14.24) | (19.58) | |
| Number. of chronic illnesses | 1.91 | 2.25 | 1.97 | 1.83 | 2.24 | 2.04 | 2.01 | 2.05 | 2.09 |
| (1.17) | (1.34) | (1.20) | (1.15) | (1.31) | (1.27) | (1.20) | (1.23) | (1.25) | |
| Has long-term illness (%) | 50.87 | 62.82 | 53.07 | 51.64 | 53.30 | 46.54 | 49.80 | 52.39 | 49.83 |
| (50.00) | (48.34) | (49.91) | (49.98) | (49.89) | (49.89) | (50.00) | (49.95) | (50.00) | |
| Has poor mental health status (%) | 19.64 | 23.04 | 17.99 | 16.35 | 33.39 | 37.88 | 34.93 | 16.24 | 27.95 |
| (39.73) | (42.11) | (38.41) | (36.98) | (47.16) | (48.51) | (47.68) | (36.89) | (44.88) | |
| Has cognitive impairment (%) | 2.93 | 1.61 | 1.35 | 1.15 | 4.65 | 2.47 | 1.31 | 0.69 | 1.98 |
| (16.86) | (12.57) | (11.56) | (10.66) | (21.05) | (15.51) | (11.39) | (8.28) | (13.94) | |
| Is frail (%) | 34.20 | 28.52 | 33.48 | 32.87 | 40.66 | 34.19 | 49.54 | 29.19 | 43.94 |
| (47.44) | (45.15) | (47.19) | (46.98) | (49.13) | (47.44) | (50.00) | (45.47) | (49.64) | |
| Completed secondary education (%) | 60.43 | 69.16 | 46.05 | 61.71 | 24.67 | 38.20 | 39.43 | 48.27 | 48.84 |
| (48.90) | (46.18) | (49.85) | (48.61) | (43.11) | (48.59) | (48.88) | (49.98) | (49.99) | |
| Completed tertiary education (%) | 25.25 | 28.98 | 27.85 | 25.66 | 8.15 | 6.82 | 19.18 | 37.66 | 30.17 |
| (43.45) | (45.37) | (44.83) | (43.68) | (27.37) | (25.21) | (39.37) | (48.46) | (45.91) | |
| Lives in a town (%) | 20.91 | 34.54 | 52.73 | 42.98 | 69.51 | 42.01 | 35.64 | 48.62 | 47.64 |
| (40.67) | (47.56) | (49.93) | (49.51) | (46.04) | (49.37) | (47.90) | (49.99) | (49.95) | |
| Lives in rural area (%) | 44.94 | 41.98 | 17.70 | 22.26 | 6.64 | 37.76 | 47.17 | 22.83 | 27.28 |
| (49.75) | (49.35) | (38.17) | (41.60) | (24.90) | (48.48) | (49.93) | (41.98) | (44.55) | |
| Number of household members | 1.88 | 1.91 | 1.81 | 1.85 | 2.22 | 2.23 | 1.80 | 1.78 | 1.85 |
| (0.88) | (0.59) | (0.53) | (0.54) | (0.91) | (0.95) | (0.68) | (0.55) | (0.70) | |
| Number of children | 2.16 | 2.02 | 2.35 | 2.39 | 2.42 | 2.06 | 2.29 | 2.30 | 2.22 |
| (1.46) | (1.29) | (1.31) | (1.38) | (1.52) | (1.34) | (1.48) | (1.26) | (1.49) | |
| Is married (%) | 63.36 | 75.92 | 73.37 | 78.06 | 77.74 | 76.78 | 63.26 | 70.00 | 68.39 |
| (48.19) | (42.76) | (44.21) | (41.38) | (41.60) | (42.23) | (48.21) | (45.83) | (46.50) | |
| Use home care (%) | 13.42 | 11.74 | 7.72 | 14.69 | 11.95 | 8.38 | 17.13 | 11.45 | 23.02 |
| (34.09) | (32.19) | (26.70) | (35.41) | (32.44) | (27.73) | (37.68) | (31.85) | (42.10) | |
| Gini coefficient for household income | 0.285 | 0.326 | 0.280 | 0.302 | 0.338 | 0.420 | 0.456 | 0.275 | 0.446 |
| (0.003) | (0.003) | (0.002) | (0.007) | (0.003) | (0.012) | (0.057) | (0.003) | (0.008) | |
| N | 3212 | 3671 | 3691 | 2954 | 4905 | 3445 | 3269 | 2610 | 3632 |
| AT | DE | SE | NL | ES | IT | FR | DK | BE | |
|---|---|---|---|---|---|---|---|---|---|
| Concentration Index (CI) | −0.078 *** | −0.088 *** | −0.080 *** | −0.161 *** | 0.027 | −0.009 | −0.105 *** | −0.186 *** | −0.046 ** |
| (0.018) | (0.017) | (0.014) | (0.018) | (0.017) | (0.014) | (0.017) | (0.017) | (0.018) |
| Self-Rated Health | Moderate Limitations | Severe Limitations | Chronic Conditions | Long-Term Illness | Mental Health | Cognitive Impairment | Frailty | |||||||||
| Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | |
| Austria | 0.121 | −0.179 | 0.101 | −0.157 | 0.139 | −0.247 | 0.254 | −0.025 | 0.050 | −0.053 | 0.035 | −0.148 | 0.018 | −0.194 | 0.069 | −0.132 |
| Germany | 0.121 | −0.146 | 0.108 | −0.182 | 0.204 | −0.187 | 0.165 | −0.055 | 0.090 | −0.059 | 0.056 | −0.149 | 0.008 | −0.242 | 0.102 | −0.113 |
| Sweden | 0.098 | −0.198 | 0.058 | −0.231 | 0.058 | −0.298 | 0.086 | −0.059 | 0.177 | −0.067 | 0.019 | −0.174 | 0.024 | −0.165 | 0.112 | −0.145 |
| Netherlands | 0.117 | −0.135 | 0.087 | −0.166 | 0.042 | −0.232 | 0.133 | −0.048 | 0.090 | −0.032 | −0.006 | −0.148 | 0.006 | −0.295 | 0.107 | −0.115 |
| Spain | 0.118 | −0.096 | 0.040 | −0.052 | 0.134 | −0.197 | 0.157 | −0.029 | 0.093 | −0.037 | 0.041 | −0.133 | 0.002 | −0.083 | 0.018 | −0.1 |
| Italy | 0.097 | −0.084 | 0.033 | −0.151 | 0.068 | −0.118 | −0.008 | −0.042 | 0.034 | −0.051 | 0.050 | −0.106 | 0.021 | −0.155 | 0.200 | −0.112 |
| France | 0.150 | −0.139 | 0.063 | −0.130 | 0.069 | −0.209 | 0.054 | −0.032 | 0.149 | −0.066 | 0.035 | −0.091 | 0.011 | −0.063 | 0.145 | −0.07 |
| Denmark | 0.089 | −0.226 | 0.058 | −0.164 | 0.071 | −0.401 | 0.100 | −0.073 | 0.104 | −0.080 | 0.010 | −0.136 | 0.005 | −0.355 | 0.123 | −0.18 |
| Belgium | 0.114 | −0.113 | 0.082 | −0.074 | 0.066 | −0.225 | 0.115 | −0.027 | 0.084 | −0.040 | 0.010 | −0.055 | 0.002 | −0.086 | 0.094 | −0.091 |
| Income | Household Size | No. of Children | Married | Urban | Rural | Secondary Education | Tertiary Education | |||||||||
| Elast. | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | Elast. | CI | ||
| Austria | 0.732 | −0.107 | −0.005 | 0.016 | −0.063 | −0.209 | 0.132 | −0.011 | 0.047 | −0.162 | −0.121 | −0.014 | −0.019 | 0.018 | 0.315 | |
| Germany | 0.241 | −0.150 | 0.042 | −0.046 | −0.038 | −0.210 | 0.124 | −0.005 | 0.024 | 0.066 | −0.040 | −0.214 | −0.082 | 0.000 | 0.251 | |
| Sweden | 1.621 | −0.346 | 0.069 | −0.063 | 0.024 | −0.044 | 0.169 | −0.013 | −0.047 | 0.017 | −0.015 | −0.016 | 0.006 | 0.047 | 0.261 | |
| Netherlands | −1.072 | −1.038 | 0.046 | −0.038 | −0.019 | −0.071 | 0.121 | −0.002 | 0.044 | −0.046 | −0.013 | −0.071 | −0.048 | 0.046 | 0.331 | |
| Spain | 0.576 | −0.461 | −0.037 | −0.124 | −0.046 | −0.080 | 0.058 | −0.015 | −0.052 | −0.022 | −0.058 | 0.089 | 0.148 | 0.109 | 0.523 | |
| Italy | −0.076 | −0.173 | −0.015 | −0.103 | −0.059 | −0.180 | 0.072 | −0.090 | 0.045 | −0.083 | −0.076 | 0.073 | 0.142 | 0.042 | 0.474 | |
| France | −0.090 | −0.307 | 0.022 | 0.080 | −0.018 | −0.192 | 0.111 | 0.029 | −0.019 | 0.015 | −0.063 | 0.058 | 0.076 | 0.047 | 0.443 | |
| Denmark | 0.591 | −0.734 | 0.065 | −0.135 | −0.005 | −0.140 | 0.145 | 0.064 | −0.040 | 0.031 | −0.009 | 0.009 | −0.053 | 0.018 | 0.243 | |
| Belgium | 0.506 | −0.214 | 0.030 | 0.052 | −0.015 | −0.142 | 0.080 | 0.066 | −0.001 | 0.041 | −0.066 | 0.056 | −0.039 | 0.088 | 0.243 | |
| Household Structures as Non-Need Factors | Household Structures as Need Factors | |||
|---|---|---|---|---|
| Country | HI | Std. Error | HI | Std. Error |
| Austria | 0.005 | 0.014 | 0.026 * | 0.014 |
| Germany | −0.005 | 0.013 | 0.012 | 0.013 |
| Sweden | −0.012 | 0.012 | 0.007 | 0.012 |
| Netherlands | −0.040 * | 0.016 | 0.007 | 0.015 |
| Spain | 0.067 *** | 0.015 | 0.063 *** | 0.015 |
| Italy | 0.024 | 0.013 | 0.028 ** | 0.013 |
| France | 0.008 | 0.014 | 0.030 ** | 0.014 |
| Denmark | −0.063 *** | 0.014 | −0.008 | 0.013 |
| Belgium | 0.020 | 0.016 | 0.037 ** | 0.016 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilinca, S.; Rodrigues, R.; Schmidt, A.E. Fairness and Eligibility to Long-Term Care: An Analysis of the Factors Driving Inequality and Inequity in the Use of Home Care for Older Europeans. Int. J. Environ. Res. Public Health 2017, 14, 1224. https://doi.org/10.3390/ijerph14101224
Ilinca S, Rodrigues R, Schmidt AE. Fairness and Eligibility to Long-Term Care: An Analysis of the Factors Driving Inequality and Inequity in the Use of Home Care for Older Europeans. International Journal of Environmental Research and Public Health. 2017; 14(10):1224. https://doi.org/10.3390/ijerph14101224
Chicago/Turabian StyleIlinca, Stefania, Ricardo Rodrigues, and Andrea E. Schmidt. 2017. "Fairness and Eligibility to Long-Term Care: An Analysis of the Factors Driving Inequality and Inequity in the Use of Home Care for Older Europeans" International Journal of Environmental Research and Public Health 14, no. 10: 1224. https://doi.org/10.3390/ijerph14101224