
Temporal Trends of Suicide Mortality in Mainland China: Results from the Age-Period-Cohort Framework

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
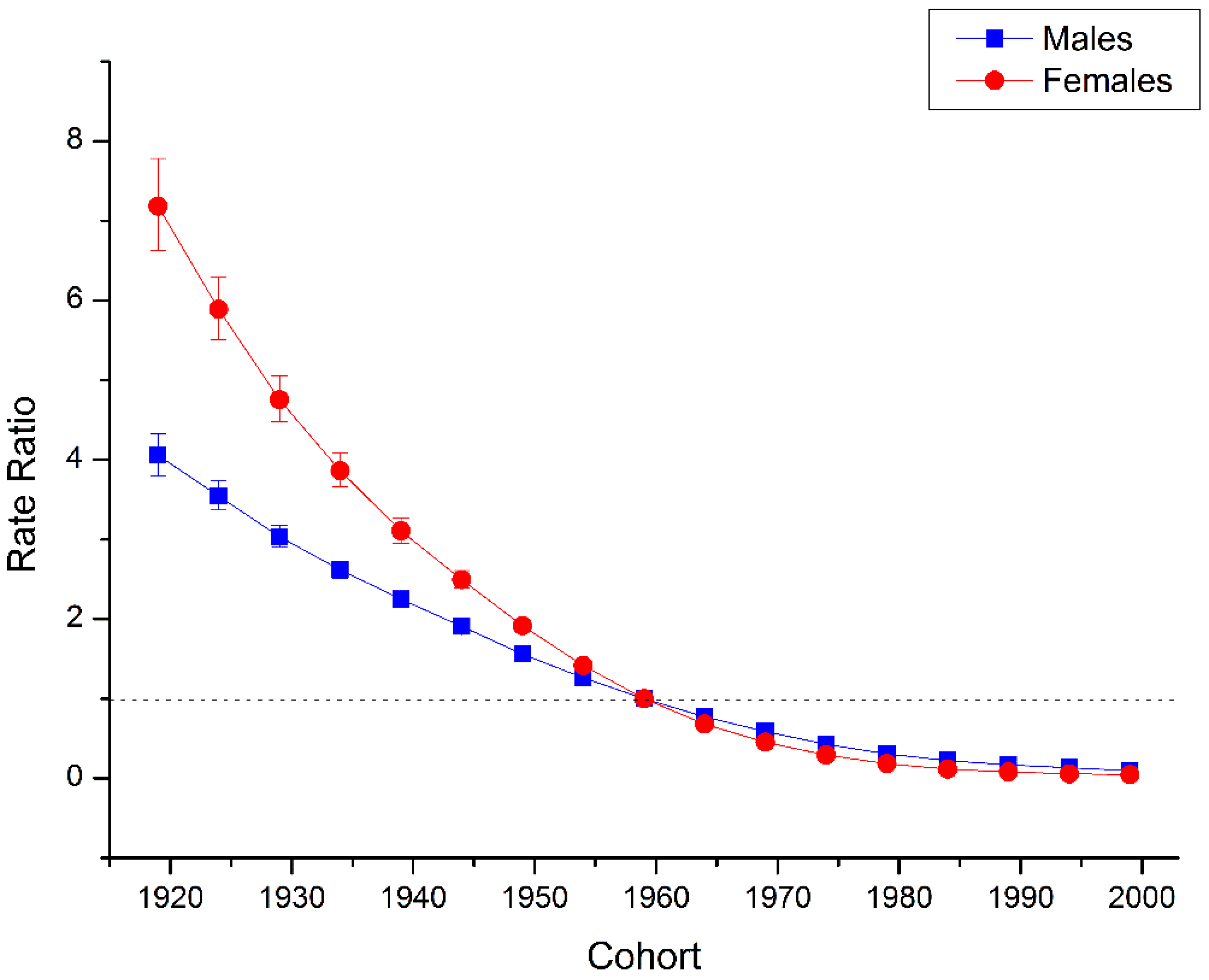
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| GBD 2013 | The Global Burden of Disease Study 2013 |
| ASMR | age-standardized mortality rate |
| APC analysis | age-period-cohort analysis |
References
- World Health Organization. Public Health Action for the Prevention of Suicide: A Framework; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Hu, G.; Wilcox, H.L. Mid-life suicide: An increasing problem in U.S. Whites, 1999–2005. Am. J. Prev. Med. 2008, 35, 589–593. [Google Scholar] [CrossRef] [PubMed]
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- World Health Organization. Global Health Observatory (GHO) Data; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Phillips, M.R.; Li, X.; Zhang, Y. Suicide rates in China, 1995–1999. Lancet 2002, 359, 835–840. [Google Scholar] [CrossRef]
- Lester, D. Suicide in Mainland China by sex, urban/rural location, and age: Preliminary data. Percept. Mot. Skills 1990, 71, 1090. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Qu, G.; Peng, Z.; Peng, T. The sex ratio of suicide rates in China. Crisis 1994, 15, 44–48. [Google Scholar] [PubMed]
- Pritchard, C. Suicide in the people’s republic of China categorized by age and gender: Evidence of the influence of culture on suicide. Acta Psychiatr. Scand. 1996, 93, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Pearson, V.; Lee, S. Suicide in China. Br. J. Psychiatry 1997, 170, 387. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.R.; Liu, H.; Zhang, Y. Suicide and social change in China. Cult. Med. Psychiatry 1999, 23, 25–50. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Kleinman, A.; Becker, A.E. Suicide in contemporary China: A review of China’s distinctive suicide demographics in their sociocultural context. Harv. Rev. Psychiatry 2001, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Qin, P.; Mortensen, P.B. Specific characteristics of suicide in China. Acta Psychiatr. Scand. 2001, 103, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Bertolote, J.M.; Fleischmann, A. Suicide rates in China. Lancet 2002, 359, 2274; author reply 2274–2275. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Suicide and attempted suicide—China, 1990–2002. MMWR Morb. Mortal Wkly. Rep. 2004, 53, 481–484. [Google Scholar]
- Yang, G.H.; Phillips, M.R.; Zhou, M.G.; Wang, L.J.; Zhang, Y.P.; Xu, D. Understanding the unique characteristics of suicide in China: National psychological autopsy study. Biomed. Environ. Sci. 2005, 18, 379–389. [Google Scholar] [PubMed]
- Yip, P.S.; Liu, K.Y.; Hu, J.; Song, X.M. Suicide rates in China during a decade of rapid social changes. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Law, S.; Liu, P. Suicide in China: Unique demographic patterns and relationship to depressive disorder. Curr. Psychiatry Rep. 2008, 10, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ma, J.; Jia, C.; Sun, J.; Guo, X.; Xu, A.; Li, W. Economic growth and suicide rate changes: A case in China from 1982 to 2005. Eur. Psychiatry 2010, 25, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Guo, X.; Ma, J.; Zhang, J.; Jia, C.; Xu, A. Seasonality of suicide in Shandong China, 1991–2009: Associations with gender, age, area and methods of suicide. J. Affect. Disord. 2011, 135, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.W.; Chan, C.L.; Yip, P.S. Suicide rates in China from 2002 to 2011: An update. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 929–941. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Sun, L.; Liu, Y.; Zhang, J. The change in suicide rates between 2002 and 2011 in China. Suicide Life Threat. Behav. 2014, 44, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Wang, H.; Zhu, J.; Chen, W.; Wang, L.; Liu, S.; Li, Y.; Wang, L.; Liu, Y.; Yin, P. Cause-specific mortality for 240 causes in China during 1990–2013: A systematic subnational analysis for the global burden of disease study 2013. Lancet 2015, 387, 251–272. [Google Scholar] [CrossRef]
- Anderson, R.N.; Miniño, A.M.; Hoyert, D.L.; Rosenberg, H.M. Comparability of cause of death between ICD-9 and ICD-10: Preliminary estimates. Nat. Vital Stat. Rep. 2001, 49, 1–32. [Google Scholar]
- Yang, Y.; Land, K.C. Age-Period-Cohort Analysis: New Models, Methods, and Empirical Applications; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Holford, T. Age-period-cohort analysis. In Wiley StatsRef: Statistics Reference Online; Wiley Online Library: Hoboken, NJ, USA, 2005; pp. 1–25. [Google Scholar]
- Glenn, N.D. Cohort Analysis; Sage: New York, NY, USA, 2005; Volume 5. [Google Scholar]
- Bell, A.; Jones, K. Another “futile quest”? A simulation study of yang and land’s hierarchical age-period-cohort model. Demogr. Res. 2014, 30, 333–360. [Google Scholar] [CrossRef]
- Bell, A.; Jones, K. The impossibility of separating age, period and cohort effects. Soc. Sci. Med. 2013, 93, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.; Jones, K. Age, period and cohort processes in longitudinal and life course analysis: A multilevel perspective. In A Life Course Perspective on Health Trajectories and Transitions; Springer International Publishing: Cham, Switzerland, 2015; pp. 197–213. [Google Scholar]
- Holford, T.R. The estimation of age, period and cohort effects for vital rates. Biometrics 1983, 39, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.; Gandini, S.; Boyle, P. Age-period-cohort models: A comparative study of available methodologies. J. Clin. Epidemiol. 1999, 52, 569–583. [Google Scholar] [CrossRef]
- Mbulaiteye, S.M.; Anderson, W.F.; Ferlay, J.; Bhatia, K.; Chang, C.; Rosenberg, P.S.; Devesa, S.S.; Parkin, D.M. Pediatric, elderly, and emerging adult-onset peaks in burkitt’s lymphoma incidence diagnosed in four continents, excluding Africa. Am. J. Hematol. 2012, 87, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.F.; Rosenberg, P.S.; Menashe, I.; Mitani, A.; Pfeiffer, R.M. Age-related crossover in breast cancer incidence rates between black and white ethnic groups. J. Nat. Cancer Inst. 2008, 100, 1804–1814. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.P.; Anderson, W.F.; Rosenberg, P.S.; Trabert, B.; Gierach, G.L.; Wentzensen, N.; Cronin, K.A.; Sherman, M.E. Ovarian cancer incidence trends in relation to changing patterns of menopausal hormone therapy use in the United States. J. Clin. Oncol. 2013, 31, 2146–2151. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Ma, J.; Rosenberg, P.S.; Siegel, R.; Anderson, W.F. Increasing lung cancer death rates among young women in southern and midwestern states. J. Clin. Oncol. 2012, 30, 2739–2744. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.S.; Check, D.P.; Anderson, W.F. A web tool for Age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2296–2302. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.A. A changing epidemiology of suicide? The influence of birth cohorts on suicide rates in the United States. Soc. Sci. Med. 2014, 114, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Ajdacic-Gross, D.P.V.; Bopp, M.; Gostynski, M.; Lauber, C.; Gutzwiller, F.; Rössler, W. Age-period-cohort analysis of Swiss suicide data, 1881–2000. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Allebeck, P.; Brandt, L.; Nordstrom, P.; Åsgård, U. Are suicide trends among the young reversing? Age, period and cohort analyses of suicide rates in Sweden. Acta Psychiatr. Scand. 1996, 93, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Surtees, P.G.; Duffy, J. Suicide in England and Wales 1946–1985: An age-period-cohort analysis. Acta Psychiatr. Scand. 1989, 79, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Odagiri, Y.; Uchida, H.; Nakano, M. Gender differences in age, period, and birth-cohort effect on suicide mortality rate in Japan 1985–2006. Asia-Pac. J. Public Health 2011, 23, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Jee, Y.H.; Jung, K.J. Age-period-cohort analysis of the suicide rate in Korea. J. Affect. Disord. 2016, 194, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Chung, R.Y.; Yip, B.H.; Chan, S.S.; Wong, S. Cohort effects of suicide mortality are sex specific in the rapidly developed Hong Kong Chinese population, 1976–2010. Depression Anxiety 2015, 33, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Joe, S. Explaining changes in the patterns of black suicide in the United States from 1981 to 2002: An age, cohort, and period analysis. J. Black Psychol. 2006, 32, 262–284. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yu, C.; Wang, J.; Bao, J.; Gao, X.; Xiang, H. Age-period-cohort analysis of suicide mortality by gender among white and black Americans, 1983–2012. Int. J. Equity Health 2016, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, N.; Tu, X.M.; Xiao, S.; Jia, C. Risk factors for rural young suicide in China: A case-control study. J. Affect. Disord. 2011, 129, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.L.; Zhong, B.L.; Xiang, Y.T.; Ungvari, G.S.; Lai, K.Y.; Chiu, H.F.; Caine, E.D. Prevalence of suicidal ideation and suicide attempts in the general population of China: A meta-analysis. Int. J. Psychiatry Med. 2015, 49, 296–308. [Google Scholar] [CrossRef] [PubMed]
- Stack, S. Social correlates of suicide by age. In Life Span Perspectives of Suicide; Springer U.S.: New York, NY, USA, 1991; pp. 187–213. [Google Scholar]
- Hawton, K.; Haw, C. Economic recession and suicide. BMJ 2013, 347. [Google Scholar] [CrossRef] [PubMed]
- Reeves, A.; Stuckler, D.; McKee, M.; Gunnell, D.; Chang, S.-S.; Basu, S. Increase in state suicide rates in the USA during economic recession. Lancet 2012, 380, 1813–1814. [Google Scholar] [CrossRef]
- Sun, J.; Guo, X.; Zhang, J.; Jia, C.; Xu, A. Suicide rates in Shandong, China, 1991–2010: Rapid decrease in rural rates and steady increase in male-female ratio. J. Affect. Disord. 2013, 146, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Song, J.; Lin, T.; Dixon, J.; Zhang, G.; Ye, H. Urbanization and health in China, thinking at the national, local and individual levels. Environ. Health 2016, 15, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.H.; Yang, H.F. The management and control status of banned/restricted pesticides in China. Mod. Prev. Med. 2013, 40, 2198–2202. [Google Scholar]
- He, Z.X.; Lester, D. Methods for suicide in Mainland China. Death Stud. 1998, 22, 571–579. [Google Scholar] [PubMed]
- Wu, K.C.; Chen, Y.Y.; Yip, P.S. Suicide methods in Asia: Implications in suicide prevention. Int. J. Environ. Res. Public Health 2012, 9, 1135–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Jiang, C.; Jia, S.; Wieczorek, W.F. An overview of suicide research in China. Arch. Suicide Res. 2002, 6, 167–184. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Lopez, A.D.; Murray, C.J.L.; Lozano, R. A comparison of maternal mortality estimates from GBD 2013 and WHO. Lancet 2014, 384, 2209–2210. [Google Scholar] [CrossRef]
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C.; Abera, S.F.; Abraham, J.P.; Adofo, K.; Alsharif, U. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Inj. Prev. 2016, 22, 3–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J.L.; Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J.L. The Global Burden of Disease and Risk Factors; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2006. [Google Scholar]
- Salmerón, D.; Cirera, L.; Ballesta, M.; Navarro-Mateu, F. Time trends and geographical variations in mortality due to suicide and causes of undetermined intent in Spain, 1991–2008. J. Public Health 2013, 35, 237–245. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Null Hypothesis | Males | Females | ||
|---|---|---|---|---|
| Chi-Square | p-Value | Chi-Square | p-Value | |
| Net Drift = 0 | 9386.6 | <0.01 | 11,294 | <0.01 |
| All Period RR = 1 | 9390.7 | <0.01 | 11,513 | <0.01 |
| All Cohort RR = 1 | 10,298 | <0.01 | 12,444 | <0.01 |
| All Local Drifts = Net Drift | 721.41 | <0.01 | 930.6 | <0.01 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.; Wang, J.; Bao, J.; Gao, X.; Yu, C.; Xiang, H. Temporal Trends of Suicide Mortality in Mainland China: Results from the Age-Period-Cohort Framework. Int. J. Environ. Res. Public Health 2016, 13, 784. https://doi.org/10.3390/ijerph13080784
Wang Z, Wang J, Bao J, Gao X, Yu C, Xiang H. Temporal Trends of Suicide Mortality in Mainland China: Results from the Age-Period-Cohort Framework. International Journal of Environmental Research and Public Health. 2016; 13(8):784. https://doi.org/10.3390/ijerph13080784
Chicago/Turabian StyleWang, Zhenkun, Jinyao Wang, Junzhe Bao, Xudong Gao, Chuanhua Yu, and Huiyun Xiang. 2016. "Temporal Trends of Suicide Mortality in Mainland China: Results from the Age-Period-Cohort Framework" International Journal of Environmental Research and Public Health 13, no. 8: 784. https://doi.org/10.3390/ijerph13080784