
Prevalence and Risk Factors of Heart Failure with Preserved Ejection Fraction: A Population-Based Study in Northeast China

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection and Definitions
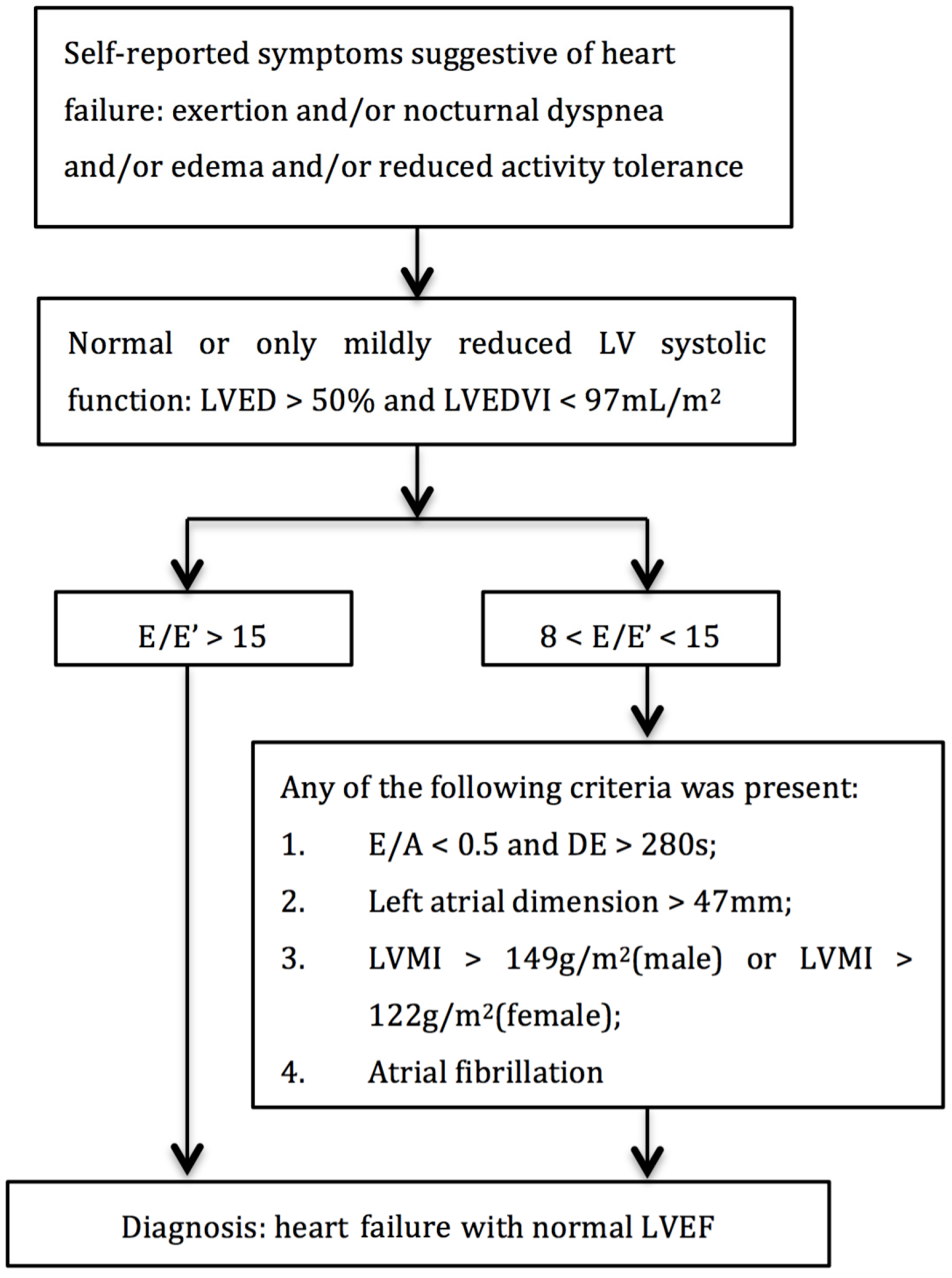
2.3. Echocardiography Measurements
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Study Population
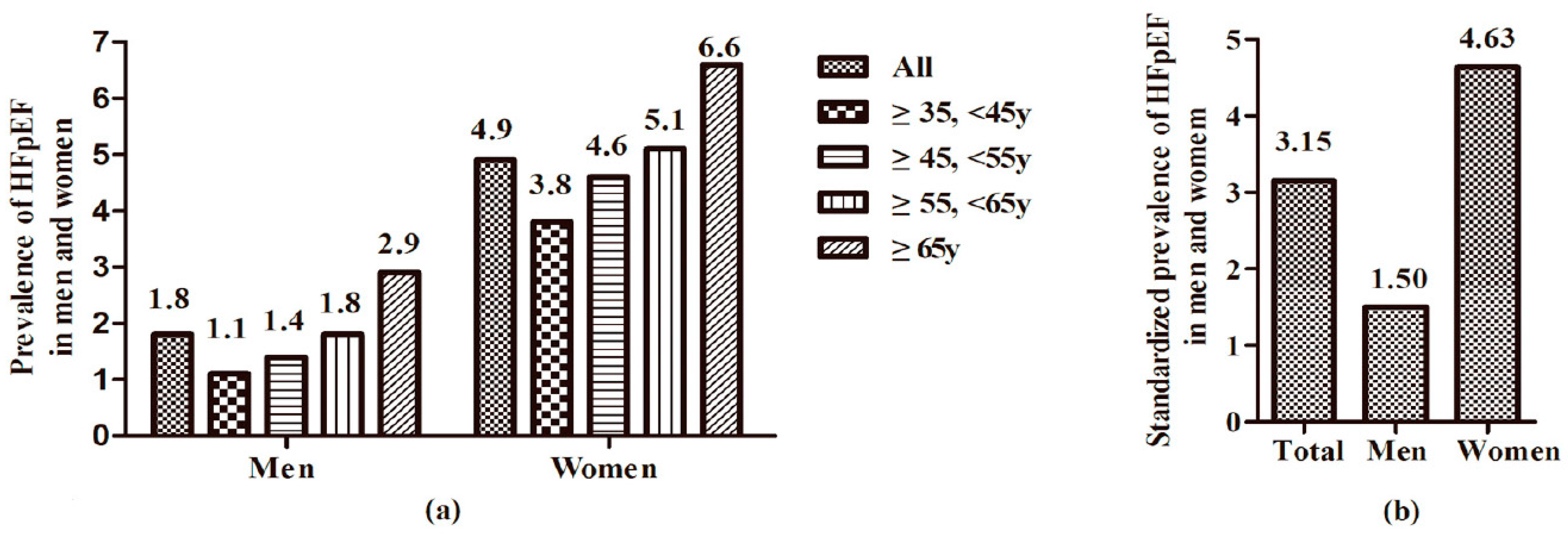
3.2. Prevalence of HFpEF by Age and Sex
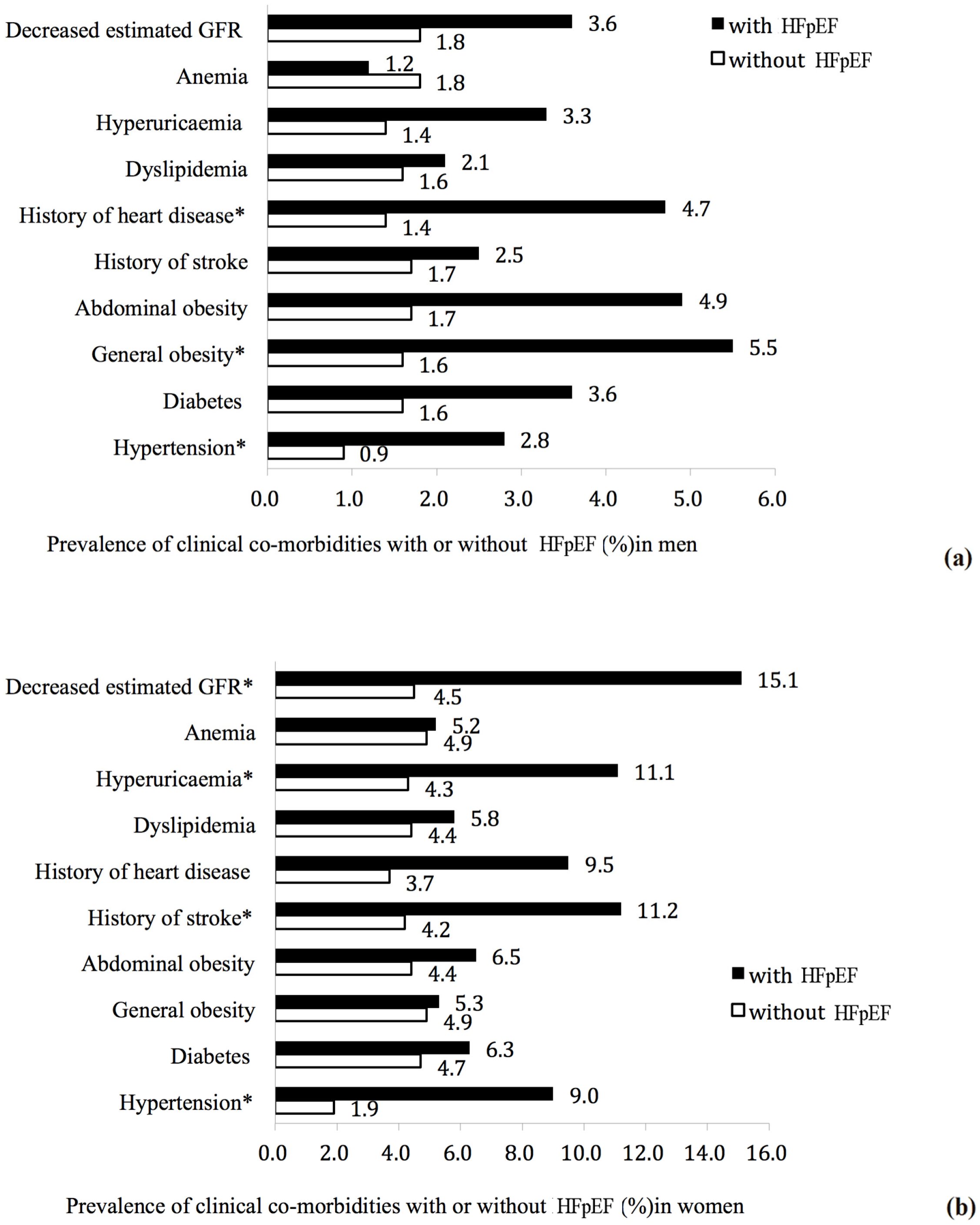
3.3. Prevalence of Clinical Co-Morbidities by Presence of HFpEF
3.4. Factors Associated with HFpEF
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Schocken, D.D.; Benjamin, E.J.; Fonarow, G.C.; Krumholz, H.M.; Levy, D.; Mensah, G.A.; Narula, J.; Shor, E.S.; Young, J.B.; Hong, Y.; et al. Prevention of heart failure: A scientific statement from the american heart association councils on epidemiology and prevention, clinical cardiology, cardiovascular nursing, and high blood pressure research; quality of care and outcomes research interdisciplinary working group; and functional genomics and translational biology interdisciplinary working group. Circulation 2008, 117, 2544–2565. [Google Scholar] [PubMed]
- Levy, D.; Kenchaiah, S.; Larson, M.G.; Benjamin, E.J.; Kupka, M.J.; Ho, K.K.; Murabito, J.M.; Vasan, R.S. Long-term trends in the incidence of and survival with heart failure. N. Engl. J. Med. 2002, 347, 1397–1402. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, F.P.; de Boer, R.A.; van der Harst, P.; Voors, A.A.; Gansevoort, R.T.; Bakker, S.J.; Hillege, H.L.; van Veldhuisen, D.J.; van Gilst, W.H. Incidence and epidemiology of new onset heart failure with preserved vs. reduced ejection fraction in a community-based cohort: 11-year follow-up of PREVEND. Eur. Heart J. 2013, 34, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Lenzen, M.J.; Scholte op Reimer, W.J.; Boersma, E.; Vantrimpont, P.J.; Follath, F.; Swedberg, K.; Cleland, J.; Komajda, M. Differences between patients with a preserved and a depressed left ventricular function: A report from the euroheart failure survey. Eur. Heart J. 2004, 25, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Stough, W.G.; Abraham, W.T.; Albert, N.M.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B.; et al. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: A report from the OPTIMIZE-HF registry. J. Am. Coll. Cardiol. 2007, 50, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, T.; Lesman-Leegte, I.; van Veldhuisen, D.J.; Sanderman, R.; Jaarsma, T. Quality of life is impaired similarly in heart failure patients with preserved and reduced ejection fraction. Eur. J. Heart Fail. 2011, 13, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.F.; Hammill, B.G.; O’Connor, C.M.; Schulman, K.A.; Curtis, L.H.; Fonarow, G.C. Clinical effectiveness of beta-blockers in heart failure: Findings from the optimize-hf (organized program to initiate lifesaving treatment in hospitalized patients with heart failure) registry. J. Am. Coll. Cardiol. 2009, 53, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Hogg, K.; Swedberg, K.; McMurray, J. Heart failure with preserved left ventricular systolic function; Epidemiology, clinical characteristics, and prognosis. J. Am. Coll. Cardiol. 2004, 43, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Owan, T.E.; Redfield, M.M. Epidemiology of diastolic heart failure. Prog. Cardiovasc. Dis. 2005, 47, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Benjamin, E.J.; Levy, D. Prevalence, clinical features and prognosis of diastolic heart failure: An epidemiologic perspective. J. Am. Coll. Cardiol. 1995, 26, 1565–1574. [Google Scholar] [CrossRef]
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J.; Roger, V.L.; Redfield, M.M. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B. Incidence and epidemiology of heart failure. Heart Fail. Rev. 2000, 5, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Cowie, M.R.; Wood, D.A.; Coats, A.J.; Thompson, S.G.; Poole-Wilson, P.A.; Suresh, V.; Sutton, G.C. Incidence and aetiology of heart failure; A population-based study. Eur. Heart J. 1999, 20, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.K.; Lee, L.C.; Liu, C.W.; Lim, S.L.; Shi, L.M.; Ong, H.Y.; Lim, Y.T.; Yeo, T.C. Framingham risk score inadequately predicts cardiac risk in young patients presenting with a first myocardial infarction. Ann. Acad. Med. Singap. 2010, 39, 163–167. [Google Scholar] [PubMed]
- Mureddu, G.F.; Agabiti, N.; Rizzello, V.; Forastiere, F.; Latini, R.; Cesaroni, G.; Masson, S.; Cacciatore, G.; Colivicchi, F.; Uguccioni, M.; et al. Prevalence of preclinical and clinical heart failure in the elderly. A population-based study in central Italy. Eur. J. Heart Fail. 2012, 14, 718–729. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A.; Philbin, E.F.; Spertus, J.A.; Kaatz, S.; Sandberg, K.R.; Weaver, W.D. Resource Utilization Among Congestive Heart Failure Study. Confirmation of a heart failure epidemic: Findings from the resource utilization among congestive heart failure (reach) study. J. Am. Coll. Cardiol. 2002, 39, 60–69. [Google Scholar] [CrossRef]
- Rodeheffer, R.J.; Jacobsen, S.J.; Gersh, B.J.; Kottke, T.E.; McCann, H.A.; Bailey, K.R.; Ballard, D.J. The incidence and prevalence of congestive heart failure in Rochester, Minnesota. Mayo Clin. Proc. 1993, 68, 1143–1150. [Google Scholar] [CrossRef]
- Hu, G.; Tuomilehto, J.; Silventoinen, K.; Barengo, N.; Jousilahti, P. Joint effects of physical activity, body mass index, waist circumference and waist-to-hip ratio with the risk of cardiovascular disease among middle-aged Finnish men and women. Eur. Heart J. 2004, 25, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Hypertension control. Report of a who expert committee. World Health Organ. Tech. Rep. Ser. 1996, 862, 1–83. [Google Scholar]
- World Health Organization. Department of Nutrition for Health and Development. Diet, Nutrition and the Prevention of Chronic Diseases; Report of a Joint WHO/FAO Expert Consultation; Geneva, 28 January–1 February 2002; World Health Organization: Geneva, Switzerland, 2003; p. 149. [Google Scholar]
- Expert Panel on Detection, Evaluation; Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar]
- World Health Organization; International Diabetes Federation. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia; Report of a WHO/IDF consultation; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Worldwide Prevalence of Anaemia 1993–2005: Who Global Database on Anaemia; World Health Organization: Geneva, Switzerland, 2008; p. 40. [Google Scholar]
- Zhang, L.; Wang, F.; Wang, L.; Wang, W.; Liu, B.; Liu, J.; Chen, M.; He, Q.; Liao, Y.; Yu, X.; et al. Prevalence of chronic kidney disease in China: A cross-sectional survey. Lancet 2012, 379, 815–822. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Schiller, N.B.; Shah, P.M.; Crawford, M.; DeMaria, A.; Devereux, R.; Feigenbaum, H.; Gutgesell, H.; Reichek, N.; Sahn, D.; Schnittger, I.; et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. J. Am. Soc. Echocardiogr. 1989, 2, 358–367. [Google Scholar] [PubMed]
- Paulus, W.J.; Tschope, C.; Sanderson, J.E.; Rusconi, C.; Flachskampf, F.A.; Rademakers, F.E.; Marino, P.; Smiseth, O.A.; De Keulenaer, G.; Leite-Moreira, A.F.; et al. How to diagnose diastolic heart failure: A consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the heart failure and echocardiography associations of the European society of cardiology. Eur. Heart J. 2007, 28, 2539–2550. [Google Scholar] [CrossRef] [PubMed]
- China Heart Failure Symposium. A consensus statement on the diagnosis and treatment of heart failure with normal left in China. Chin. J. Med. 2010, 45, 63–67. [Google Scholar]
- The 2010 Population Census of China. Available online: http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm (accessed on 28 July 2016).
- Senni, M.; Tribouilloy, C.M.; Rodeheffer, R.J.; Jacobsen, S.J.; Evans, J.M.; Bailey, K.R.; Redfield, M.M. Congestive heart failure in the community: A study of all incident cases in Olmsted County, Minnesota, in 1991. Circulation 1998, 98, 2282–2289. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Weston, S.A.; Redfield, M.M.; Hellermann-Homan, J.P.; Killian, J.; Yawn, B.P.; Jacobsen, S.J. Trends in heart failure incidence and survival in a community-based population. JAMA 2004, 292, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Squara, P.; Denjean, D.; Estagnasie, P.; Brusset, A.; Dib, J.C.; Dubois, C. Noninvasive cardiac output monitoring (NICOM): A clinical validation. Intensive Care Med. 2007, 33, 1191–1194. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Larson, M.G.; Benjamin, E.J.; Evans, J.C.; Reiss, C.K.; Levy, D. Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: Prevalence and mortality in a population-based cohort. J. Am. Coll. Cardiol. 1999, 33, 1948–1955. [Google Scholar] [CrossRef]
- Hedberg, P.; Lonnberg, I.; Jonason, T.; Nilsson, G.; Pehrsson, K.; Ringqvist, I. Left ventricular systolic dysfunction in 75-year-old men and women; A population-based study. Eur. Heart J. 2001, 22, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Redfield, M.M.; Jacobsen, S.J.; Burnett, J.C., Jr.; Mahoney, D.W.; Bailey, K.R.; Rodeheffer, R.J. Burden of systolic and diastolic ventricular dysfunction in the community: Appreciating the scope of the heart failure epidemic. JAMA 2003, 289, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.; Hobbs, F.; Davis, R.; Kenkre, J.; Roalfe, A.K.; Hare, R.; Wosornu, D.; Lancashire, R.J. Prevalence of left-ventricular systolic dysfunction and heart failure in the echocardiographic heart of England screening study: A population based study. Lancet 2001, 358, 439–444. [Google Scholar] [CrossRef]
- Tiller, D.; Russ, M.; Greiser, K.H.; Nuding, S.; Ebelt, H.; Kluttig, A.; Kors, J.A.; Thiery, J.; Bruegel, M.; Haerting, J.; et al. Prevalence of symptomatic heart failure with reduced and with normal ejection fraction in an elderly general population—The CARLA Study. PLoS ONE 2013, 8, e59225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosterd, A.; Hoes, A.W.; de Bruyne, M.C.; Deckers, J.W.; Linker, D.T.; Hofman, A.; Grobbee, D.E. Prevalence of heart failure and left ventricular dysfunction in the general population; The Rotterdam Study. Eur. Heart J. 1999, 20, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, T.S.; Tulloch-Reid, M.K.; Younger, N.O.; Knight-Madden, J.M.; Samms-Vaughan, M.; Ashley, D.; Van den Broeck, J.; Wilks, R.J. Prevalence of the metabolic syndrome and its components in relation to socioeconomic status among Jamaican young adults: A cross-sectional study. BMC Public Health 2010, 10, 307. [Google Scholar] [CrossRef] [PubMed]
- Baghshomali, S.; Bushnell, C. Reducing stroke in women with risk factor management: Blood pressure and cholesterol. Women’s Health 2014, 10, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Tsuchihashi, M.; Takeshita, A. Mortality and readmission of hospitalized patients with congestive heart failure and preserved versus depressed systolic function. Am. J. Cardiol. 2001, 88, 530–533. [Google Scholar] [CrossRef]
- Lam, C.S.; Carson, P.E.; Anand, I.S.; Rector, T.S.; Kuskowski, M.; Komajda, M.; McKelvie, R.S.; McMurray, J.J.; Zile, M.R.; Massie, B.M.; et al. Sex differences in clinical characteristics and outcomes in elderly patients with heart failure and preserved ejection fraction: The Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial. Circ. Heart Fail. 2012, 5, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Kalsch, H.; Lehmann, N.; Mohlenkamp, S.; Neumann, T.; Slomiany, U.; Schmermund, A.; Stang, A.; Moebus, S.; Bauer, M.; Mann, K.; et al. Association of coronary artery calcium and congestive heart failure in the general population: Results of the Heinz Nixdorf Recall study. Clin. Res. Cardiol. 2010, 99, 175–182. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 2230) | Male (n = 1055) | Female (n = 1175) | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 56 ± 11 | 56 ± 11 | 55 ± 10 | 0.025 |
| Current smoking status | 818 (36.7) | 597 (56.6) | 221 (18.8) | <0.001 |
| Current drinking status | 440 (19.7) | 421 (39.9) | 19 (1.6) | <0.001 |
| Physical activity | 0.001 | |||
| Low | 509 (22.8) | 205 (19.4) | 304 (25.9) | |
| Moderate | 1540 (69.1) | 762 (72.2) | 778 (66.2) | |
| High | 181 (8.1) | 88 (8.3) | 93 (7.9) | |
| Family income (CNY/year) | 0.345 | |||
| ≤5000 | 427 (19.1) | 213 (20.2) | 214 (18.2) | |
| 5000–20,000 | 1196 (53.6) | 550 (52.1) | 646 (55.0) | |
| >20,000 | 607 (27.2) | 292 (27.7) | 315 (26.8) | |
| BMI (kg/m2) | 24.2 ± 3.6 | 24.1 ± 3.6 | 24.3 ± 3.7 | 0.207 |
| WC (cm) | 83.1 ± 9.7 | 84.1 ± 10.0 | 82.1 ± 9.4 | <0.001 |
| SBP (mm Hg) | 137.9 ± 23.0 | 139.7 ± 22.1 | 136.3 ± 23.7 | <0.001 |
| DBP (mm Hg) | 81.1 ± 11.6 | 82.6 ± 11.2 | 79.7 ± 11.8 | <0.001 |
| Laboratory variables | ||||
| TC (mmol/L) | 5.13 ± 1.06 | 5.05 ± 1.06 | 5.20 ± 1.05 | 0.001 |
| TG (mmol/L) | 1.78 ± 1.73 | 1.84 ± 2.00 | 1.73 ± 1.44 | 0.143 |
| LDL-C (mmol/L) | 2.67 ± 0.67 | 2.63 ± 0.64 | 2.71 ± 0.69 | 0.005 |
| HDL-C (mmol/L) | 1.32 ± 0.30 | 1.30 ± 0.33 | 1.33 ± 0.27 | 0.034 |
| FPG (mmol/L) | 5.95 ± 1.63 | 6.00 ± 1.64 | 5.91 ± 1.63 | 0.220 |
| Uric acid (μmol/L) | 315.4 ± 87.8 | 356.7 ± 88.0 | 278.3 ± 69.2 | <0.001 |
| Hemoglobin (g/L) | 136.5 ± 14.8 | 146.3 ± 12.7 | 127.8 ± 10.5 | <0.001 |
| Estimated GFR (mL/min/1.73 m2) | 87.5 ± 14.6 | 90.2 ± 13.8 | 85.1 ± 14.8 | <0.001 |
| Echocardiographic parameters | ||||
| LAD, cm | 3.4 ± 0.4 | 3.5 ± 0.4 | 3.3 ± 0.4 | <0.001 |
| LVEDV, mL | 104.3 ± 23.9 | 112.7 ± 22.4 | 96.7 ± 22.5 | <0.001 |
| LVESV, mL | 37.2 ± 10.2 | 39.6 ± 11.4 | 35.0 ± 8.6 | <0.001 |
| LVEF, % | 64.1 ± 6.8 | 64.9 ± 5.9 | 63.4 ± 7.4 | <0.001 |
| E/E′ | 9.1 ± 3.9 | 8.6 ± 3.7 | 9.5 ± 4.1 | <0.001 |
| E/A | 1.0 ± 0.6 | 1.0 ± 0.7 | 1.0 ± 0.4 | 0.252 |
| EDT, ms | 191.8 ± 37.7 | 191.1 ± 35.7 | 192.4 ± 39.4 | 0.337 |
| LVMI, g/m2 | 90.3 ± 57.5 | 95.3 ± 67.4 | 85.7 ± 46.5 | <0.001 |
| Co-morbidities | ||||
| Hypertension | 1001 (44.9) | 499 (47.3) | 502 (42.7) | 0.03 |
| Diabetes | 253 (11.3) | 110 (10.4) | 143 (12.2) | 0.195 |
| General obesity | 131 (5.9) | 55 (5.2) | 76 (6.5) | 0.208 |
| Abdominal obesity | 351 (15.7) | 41 (3.9) | 310 (26.4) | <0.001 |
| History of stroke | 244 (10.9) | 119 (11.3) | 125 (10.6) | 0.628 |
| History of heart disease | 370 (16.6) | 129 (12.2) | 241 (20.5) | <0.001 |
| Dyslipidemia | 856 (38.4) | 424 (40.2) | 432 (36.8) | 0.097 |
| Variable | Men | Women | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (year) | 1.016 | 0.966–1.070 | 0.536 | 0.973 | 0.939–1.008 | 0.128 |
| Current smoking status | 0.671 | 0.254–1.775 | 0.422 | 1.713 | 0.902–3.253 | 0.1 |
| Current drinking status | 1.455 | 0.549–3.854 | 0.45 | 2.007 | 0.420–9.592 | 0.383 |
| Physical activity | 1.156 | 0.492–2.716 | 0.74 | 0.916 | 0.562–1.493 | 0.725 |
| Dyslipidemia | 0.863 | 0.307–2.423 | 0.78 | 0.902 | 0.498–1.637 | 0.735 |
| Hyperuricaemia | 1.99 | 0.697–5.684 | 0.199 | 1.755 | 0.815–3.777 | 0.15 |
| Anemia | 0.673 | 0.080–5.694 | 0.716 | 1.234 | 0.583–2.613 | 0.583 |
| Decreased estimated GFR | 0.908 | 0.089–9.245 | 0.935 | 1.983 | 0.723–5.435 | 0.183 |
| Hypertension | 2.346 | 0.784–7.018 | 0.127 | 4.462 | 2.222–8.960 | <0.001 * |
| Diabetes | 1.799 | 0.543–5.958 | 0.337 | 0.759 | 0.340–1.695 | 0.501 |
| General obesity | 1.911 | 0.284–12.867 | 0.505 | 0.75 | 0.234–2.403 | 0.628 |
| Abdominal obesity | 1.076 | 0.119–9.719 | 0.948 | 1.152 | 0.611–2.170 | 0.662 |
| History of stroke | 1.12 | 0.297–4.220 | 0.868 | 1.913 | 0.951–3.845 | 0.069 |
| History of heart disease | 2.602 | 0.917–7.388 | 0.072 | 1.872 | 1.034–3.390 | 0.039 * |
| Income | 1.031 | 0.502–2.120 | 0.934 | 1.048 | 0.667–1.647 | 0.839 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, L.; Guo, X.; Chang, Y.; Yang, J.; Zhang, L.; Li, T.; Sun, Y. Prevalence and Risk Factors of Heart Failure with Preserved Ejection Fraction: A Population-Based Study in Northeast China. Int. J. Environ. Res. Public Health 2016, 13, 770. https://doi.org/10.3390/ijerph13080770
Guo L, Guo X, Chang Y, Yang J, Zhang L, Li T, Sun Y. Prevalence and Risk Factors of Heart Failure with Preserved Ejection Fraction: A Population-Based Study in Northeast China. International Journal of Environmental Research and Public Health. 2016; 13(8):770. https://doi.org/10.3390/ijerph13080770
Chicago/Turabian StyleGuo, Liang, Xiaofan Guo, Ye Chang, Jun Yang, Limin Zhang, Tan Li, and Yingxian Sun. 2016. "Prevalence and Risk Factors of Heart Failure with Preserved Ejection Fraction: A Population-Based Study in Northeast China" International Journal of Environmental Research and Public Health 13, no. 8: 770. https://doi.org/10.3390/ijerph13080770