
Olives and Bone: A Green Osteoporosis Prevention Option



Abstract
:1. Introduction
2. Bone Protecting Effects of Olives
3. Bone Protecting Effects of Olive Oil
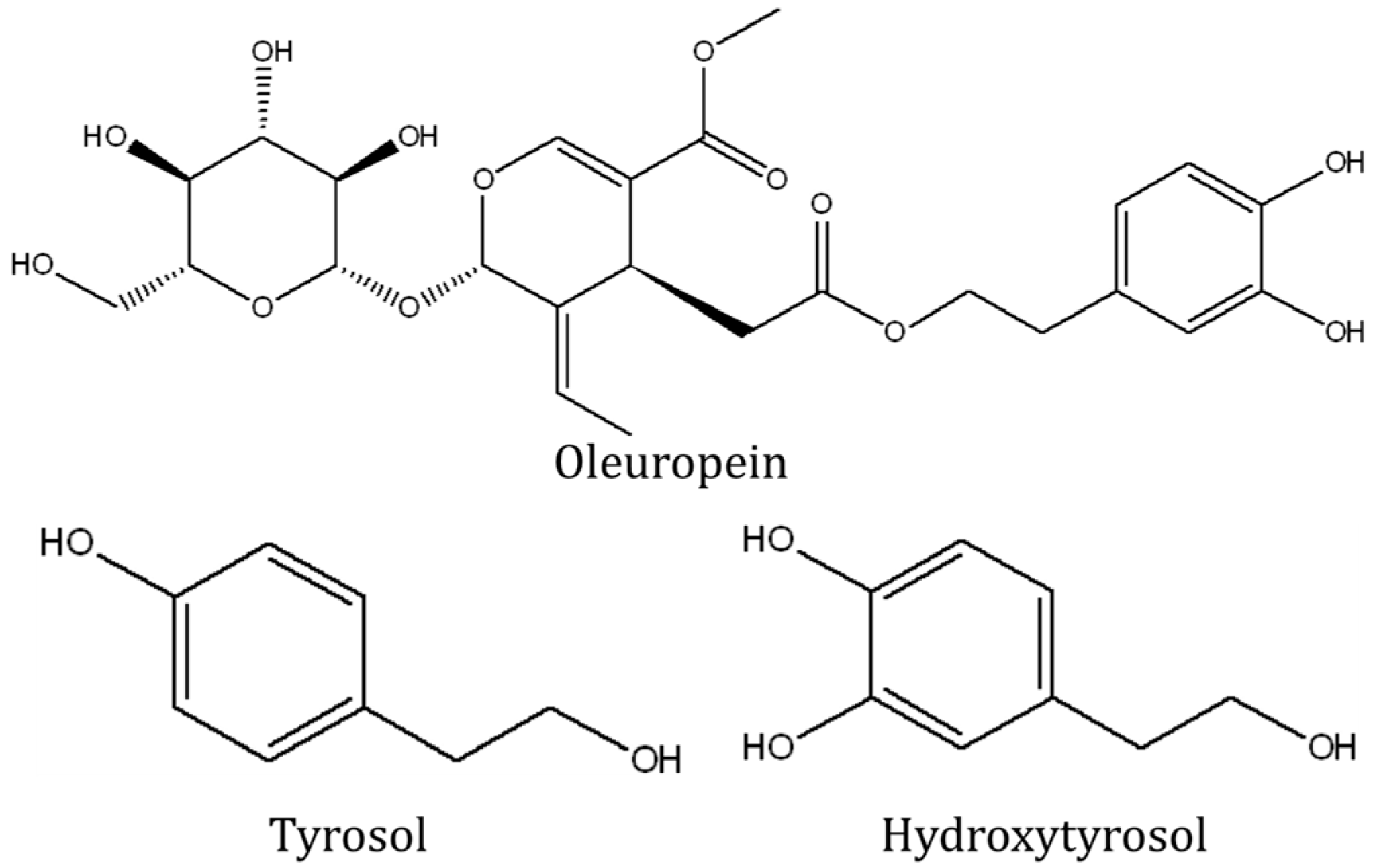
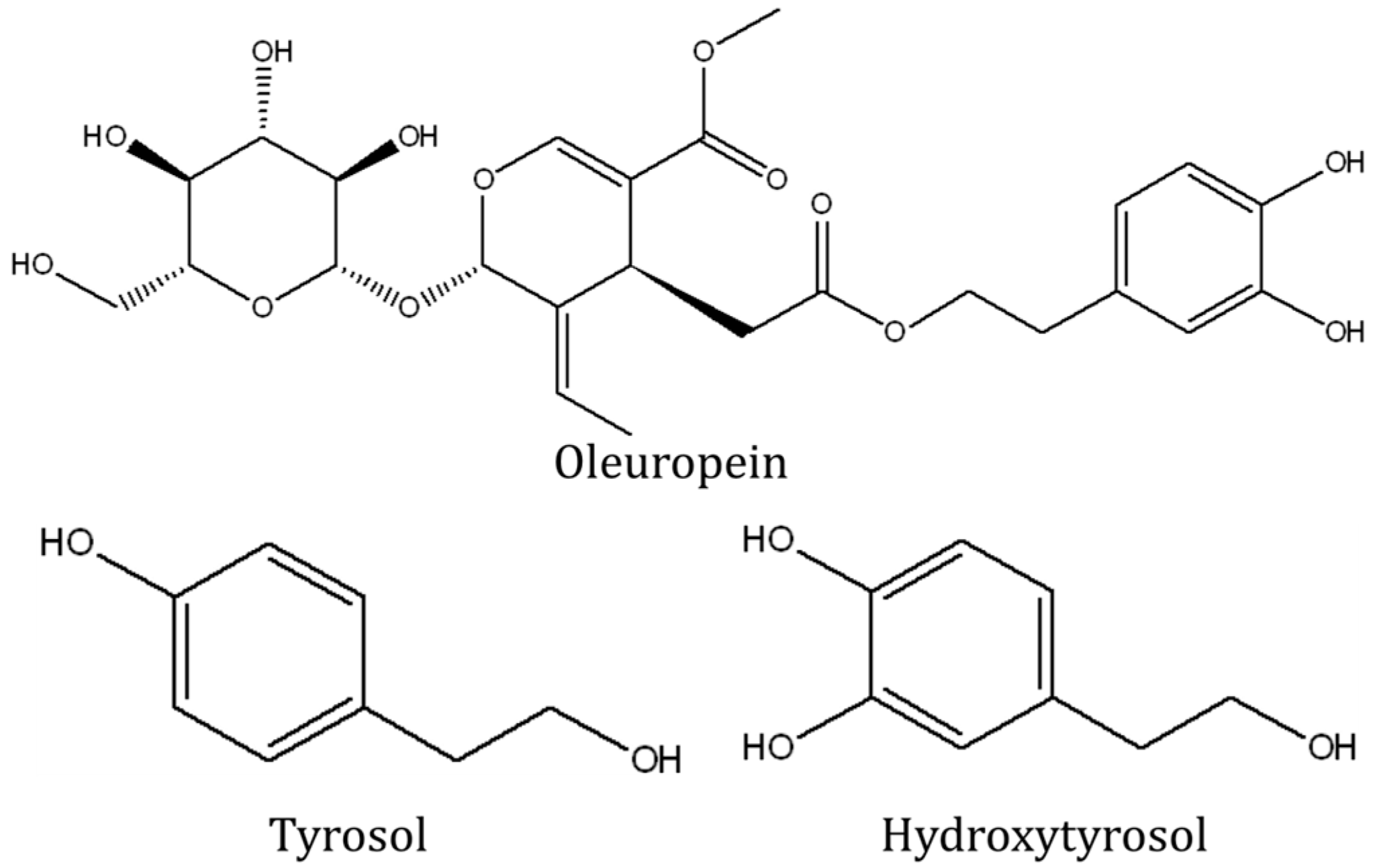
4. Bone-Protecting Effects of Olive Polyphenols
5. Studies of Olive Polyphenols on Bone Cells Using in Vitro Models
6. Human Studies on the Bone Protecting Effects of Olive Oil
7. Future Research Directions
8. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Edwards, M.H.; Dennison, E.M.; Aihie Sayer, A.; Fielding, R.; Cooper, C. Osteoporosis and sarcopenia in older age. Bone 2015, 80, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Gullberg, B.; Johnell, O.; Kanis, J.A. World-wide projections for hip fracture. Osteoporos. Int. 1997, 7, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; McDonald, J.M. Disorders of bone remodeling. Ann. Rev. Pathol. 2011, 6, 121–145. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C. From estrogen-centric to aging and oxidative stress: A revised perspective of the pathogenesis of osteoporosis. Endocr. Rev. 2010, 31, 266–300. [Google Scholar] [CrossRef] [PubMed]
- Ginaldi, L.; Di Benedetto, M.C.; De Martinis, M. Osteoporosis, inflammation and ageing. Immun. Ageing 2005, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Riggs, B.L.; Khosla, S.; Melton, L.J. Sex steroids and the construction and conservation of the adult skeleton. Endocr. Rev. 2002, 23, 279–302. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R. Proinflammatory cytokines and osteoporosis. Curr. Osteoporos. Rep. 2009, 7, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason, I.; Macpherson, A.; Mackintosh, C.; Buxton-Thomas, M.; Forgacs, I.; Moniz, C. Reduced bone density in patients with inflammatory bowel disease. Gut 1997, 40, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Blanchard, J.F.; Leslie, W.; Wajda, A.; Yu, B.N. The incidence of fracture among patients with inflammatory bowel disease. A population-based cohort study. Ann. Intern. Med. 2000, 133, 795–799. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.; Bok Kwak, H.; Woong Lee, S.; Mi Jin, H.; Kim, H.-M.; Kim, H.-H.; Hee Lee, Z. Reactive oxygen species mediate rank signaling in osteoclasts. Exp. Cell Res. 2004, 301, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Fatokun, A.A.; Stone, T.W.; Smith, R.A. Responses of differentiated MC3T3-E1 osteoblast-like cells to reactive oxygen species. Eur. J. Pharmacol. 2008, 587, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Sharma, T.; Islam, N.; Ahmad, J.; Akhtar, N.; Beg, M. Correlation between bone mineral density and oxidative stress in postmenopausal women. Indian J. Endocrinol. Metab. 2015, 19, 491–497. [Google Scholar] [PubMed]
- Cervellati, C.; Bonaccorsi, G.; Cremonini, E.; Bergamini, C.M.; Patella, A.; Castaldini, C.; Ferrazzini, S.; Capatti, A.; Picarelli, V.; Pansini, F.S.; et al. Bone mass density selectively correlates with serum markers of oxidative damage in post-menopausal women. Clin. Chem. Lab. Med. 2013, 51, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.Y.; Ima-Nirwana, S. The biological effects of tocotrienol on bone: A review on evidence from rodent models. Drug Des. Dev. Ther. 2015, 9, 2049–2061. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.-Y.; Mo, H.; Soelaiman, I.-N. A review of the possible mechanisms of action of tocotrienol—A potential antiosteoporotic agent. Curr. Drug Targets 2013, 14, 1533–1541. [Google Scholar] [CrossRef] [PubMed]
- Peddada, K.V.; Peddada, K.V.; Shukla, S.K.; Mishra, A.; Verma, V. Role of curcumin in common musculoskeletal disorders: A review of current laboratory, translational, and clinical data. Orthop. Surg. 2015, 7, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Mangano, K.M.; Sahni, S.; Kerstetter, J.E.; Kenny, A.M.; Hannan, M.T. Polyunsaturated fatty acids and their relation with bone and muscle health in adults. Curr. Osteoporos. Rep. 2013, 11, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Benetou, V.; Orfanos, P.; Pettersson-Kymmer, U.; Bergstrom, U.; Svensson, O.; Johansson, I.; Berrino, F.; Tumino, R.; Borch, K.B.; Lund, E.; et al. Mediterranean diet and incidence of hip fractures in a european cohort. Osteoporos. Int. 2013, 24, 1587–1598. [Google Scholar] [CrossRef] [PubMed]
- Seiquer, I.; Mesias, M.; Hoyos, A.M.; Galdo, G.; Navarro, M.P. A mediterranean dietary style improves calcium utilization in healthy male adolescents. J. Am. Coll. Nutr. 2008, 27, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Real, J.M.; Bulló, M.; Moreno-Navarrete, J.M.; Ricart, W.; Ros, E.; Estruch, R.; Salas-Salvadó, J. A mediterranean diet enriched with olive oil is associated with higher serum total osteocalcin levels in elderly men at high cardiovascular risk. J. Clin. Endocrinol. Metab. 2012, 97, 3792–3798. [Google Scholar] [CrossRef] [PubMed]
- Ostrowska, E.; Gabler, N.K.; Ridley, D.; Suster, D.; Eagling, D.R.; Dunshea, F.R. Extra-virgin and refined olive oils decrease plasma triglyceride, moderately affect lipoprotein oxidation susceptibility and increase bone density in growing pigs. J. Sci. Food Agric. 2006, 86, 1955–1963. [Google Scholar] [CrossRef]
- Rezq, A.A.; Labib, F.A.; Attia, A.E.M. Effect of some dietary oils and fats on serum lipid profile, calcium absorption and bone mineralization in mice. Pakistan J. Nutr. 2010, 9, 643–650. [Google Scholar] [CrossRef]
- Tuck, K.L.; Hayball, P.J. Major phenolic compounds in olive oil: Metabolism and health effects. J. Nutr. Biochem. 2002, 13, 636–644. [Google Scholar] [CrossRef]
- Efentakis, P.; Iliodromitis, E.K.; Mikros, E.; Papachristodoulou, A.; Dagres, N.; Skaltsounis, A.L.; Andreadou, I. Effects of the olive tree leaf constituents on myocardial oxidative damage and atherosclerosis. Planta Med. 2015, 81, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Puel, C.; Mardon, J.; Kati-Coulibaly, S.; Davicco, M.J.; Lebecque, P.; Obled, C.; Rock, E.; Horcajada, M.N.; Agalias, A.; Skaltsounis, L.A.; et al. Black lucques olives prevented bone loss caused by ovariectomy and talc granulomatosis in rats. Br. J. Nutr. 2007, 97, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Puel, C.; Quintin, A.; Agalias, A.; Mathey, J.; Obled, C.; Mazur, A.; Davicco, M.J.; Lebecque, P.; Skaltsounis, A.L.; Coxam, V. Olive oil and its main phenolic micronutrient (oleuropein) prevent inflammation-induced bone loss in the ovariectomised rat. Br. J. Nutr. 2004, 92, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Saleh, N.K.; Saleh, H.A. Olive oil effectively mitigates ovariectomy-induced osteoporosis in rats. BMC Complement. Altern. Med. 2011, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Huang, H.; Li, B.; Wu, D.; Wang, F.; Zheng, X.H.; Chen, Q.; Wu, B.; Fan, X. Olive oil in the prevention and treatment of osteoporosis after artificial menopause. Clin. Interv. Aging 2014, 9, 2087–2095. [Google Scholar] [CrossRef] [PubMed]
- Soler-Rivas, C.; Espín, J.C.; Wichers, H.J. Oleuropein and related compounds. J. Sci. Food Agric. 2000, 80, 1013–1023. [Google Scholar] [CrossRef]
- Puel, C.; Mardon, J.; Agalias, A.; Davicco, M.J.; Lebecque, P.; Mazur, A.; Horcajada, M.N.; Skaltsounis, A.L.; Coxam, V. Major phenolic compounds in olive oil modulate bone loss in an ovariectomy/inflammation experimental model. J. Agric. Food. Chem. 2008, 56, 9417–9422. [Google Scholar] [CrossRef] [PubMed]
- Puel, C.; Mathey, J.; Agalias, A.; Kati-coulibaly, S.; Mardon, J.; Obled, C.; Davicco, M.J.; Lebecque, P.; Horcajada, M.N.; Skaltsounis, A.L.; et al. Dose-response study of effect of oleuropein, an olive oil polyphenol, in an ovariectomy/inflammation experimental model of bone loss in the rat. Clin. Nutr. 2006, 25, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, K.; Goto, T.; Araki, M.; Miyazaki, H.; Hagiwara, H. Olive polyphenol hydroxytyrosol prevents bone loss. Eur. J. Pharmacol. 2011, 662, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Keiler, A.M.; Zierau, O.; Bernhardt, R.; Scharnweber, D.; Lemonakis, N.; Termetzi, A.; Skaltsounis, L.; Vollmer, G.; Halabalaki, M. Impact of a functionalized olive oil extract on the uterus and the bone in a model of postmenopausal osteoporosis. Eur. J. Nutr. 2014, 53, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- García-Martínez, O.; Mazzaglia, G.; Sánchez-Ortiz, A.; Ocaña-Peinado, F.M.; Rivas, A. Phenolic content of sicilian virgin olive oils and their effect on MG-63 human osteoblastic cell proliferation. Grasas Aceites 2014, 65, e032. [Google Scholar]
- Garcia-Martinez, O.; De Luna-Bertos, E.; Ramos-Torrecillas, J.; Ruiz, C.; Milia, E.; Lorenzo, M.L.; Jimenez, B.; Sanchez-Ortiz, A.; Rivas, A. Phenolic compounds in extra virgin olive oil stimulate human osteoblastic cell proliferation. PLoS ONE 2016, 11, e0150045. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Mora, R.; Casado-Diaz, A.; De Castro, M.D.; Quesada-Gomez, J.M. Oleuropein enhances osteoblastogenesis and inhibits adipogenesis: The effect on differentiation in stem cells derived from bone marrow. Osteoporos. Int. 2011, 22, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Mazzanti, L.; Battino, M.; Nanetti, L.; Raffaelli, F.; Alidori, A.; Sforza, G.; Carle, F.; Quagliarini, V.; Cester, N.; Vignini, A. Effect of 1-year dietary supplementation with vitaminized olive oil on markers of bone turnover and oxidative stress in healthy post-menopausal women. Endocrine 2015, 50, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Gundberg, C.M.; Lian, J.B.; Booth, S.L. Vitamin k-dependent carboxylation of osteocalcin: Friend or foe? Adv. Nutr. 2012, 3, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; LaCroix, A.Z.; Kooperberg, C.; Stefanick, M.L.; Jackson, R.D.; Beresford, S.A.; Howard, B.V.; Johnson, K.C.; et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the women’s health initiative randomized controlled trial. JAMA 2002, 288, 321–333. [Google Scholar] [PubMed]
- Kuiper, G.G.; Lemmen, J.G.; Carlsson, B.; Corton, J.C.; Safe, S.H.; van der Saag, P.T.; van der Burg, B.; Gustafsson, J.A. Interaction of estrogenic chemicals and phytoestrogens with estrogen receptor beta. Endocrinology 1998, 139, 4252–4263. [Google Scholar] [PubMed]
- Holt, G.; Smith, R.; Duncan, K.; Hutchison, J.D.; Gregori, A. Gender differences in epidemiology and outcome after hip fracture: Evidence from the scottish hip fracture audit. Bone Jt. J. 2008, 90-B, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Penrod, J.D.; Litke, A.; Hawkes, W.G.; Magaziner, J.; Doucette, J.T.; Koval, K.J.; Silberzweig, S.B.; Egol, K.A.; Siu, A.L. The association of race, gender, and comorbidity with mortality and function after hip fracture. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 867–872. [Google Scholar] [CrossRef]
- Lelovas, P.P.; Xanthos, T.T.; Thoma, S.E.; Lyritis, G.P.; Dontas, I.A. The laboratory rat as an animal model for osteoporosis research. Comp. Med. 2008, 58, 424–430. [Google Scholar] [PubMed]
- Turner, A.S. Animal models of osteoporosis—Necessity and limitations. Eur. Cells Mater. 2001, 1, 66–81. [Google Scholar]

{kind=link}
| No. | Reference | Treatment; Dose; Length | Method of Inducing Bone Loss | Bone Mineral Density | Histology/ Histomorphometry | Bone Turnover Marker | Bone Strength | Oxidative Stress | Inflammation |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Puel et al. 2007 [26] | Black Lucques olives; 6 g per day; 84 days | OVX or OVX + talc | ↑ (diaphyseal) | NA | ↔ | ↔ | ↔ | ↔ |
| 2 | Puel et al. 2004 [27] | Extra virgin olive oil; 50 g/kg diet; 80 days. Oleuropein; 0.15 g/kg diet; 80 days | OVX or OVX + talc | ↑ | NA | ↔ | ↑ | ↔ | ↓ (olive oil only) |
| 3 | Saleh and Saleh 2011 [28] | Olive oil; 1 mL/100 g diet; 12 weeks | OVX | ↑ bone thickness | NA | ↓ calcim and ALP activity | NA | ↓ | NA |
| 4 | Liu et al. 2014 [29] | Olive oil; 1 mL/100 g diet; 12 weeks | OVX | ↑ | NA | ↔ | NA | ↓ | NA |
| 5 | Puel et al. 2006 [32] | Oleuropein; 2.5–15 mg/kg; 100 days | OVX or OVX + talc | ↑ | NA | ↓ formation & resorption markers | ↔ | ↔ | NA |
| 6 | Puel et al. 2008 [31] | Tyrosol 0.017%, or hydroxytyrosol 0.017%, or olive mill wastewater 0.17%, or olive mill wastewater extract 0.08% or 0.0425%; 84 days. | OVX or OVX + talc | ↑ (all except OMWW) | NA | ↑ osteocalcin; ↔ DPD | ↔ | ↓ isoprostane; ↔ FRAP | ↓ granulocytes (OMWW 0.0425%); ↔ fibrinogen |
| 7 | Hagiwara et al. 2011 [33] | Hydroxytyrosol or tyrosol or oleuropein; 10 mg/kg; 28 days | OVX | ↑ trabecular; ↔ cortical | NA | NA | NA | NA | NA |
| 8 | Keiler et al. 2014 [34] | Olive oil phenolic extract; 800 mg/kg diet; 12 weeks | OVX | NA | ↔ | NA | NA | NA | NA |
| No. | Reference | Subjects and Treatment | Bone Mineral Density | Bone Turnover Markers | Antioxidants |
|---|---|---|---|---|---|
| 1 | Fernandez-Real et al. 2012 [21] | 127 community-dwelling men aged 55–80 years participated in the Prevencion con Dieta Mediterranea (PREDIMED) study with high cardivascular risk. They were divided into 3 groups: Mediterranean diet with virgin olive oil, Mediterranean diet with mixed nuts, low-fat diet. 2 years follow up. | NA | ↑ | NA |
| 2 | Liu et al. 2014 [29] | Patients aged 30–50 years who had undergone a hysterectomy. 10 took 50 mL olive oil daily and 10 took nothing. Follow up 1 year. | ↑ | ↑ | NA |
| 3 | Mazzanti et al. 2015 [15] | 60 Caucasian post-menopausal women aged 50–61 years attending health screening for osteoporosis in a hospital. They were randomly divided into two groups, 1 taking enriched extra virgin olive oil (vitamin K1 0.07 mg/100 mL, vitamin D3 50 µg/100 mL and vitamin B6 6.0 mg/100 mL) and another taking plain virgin olive oil for 1 year. | NA | ↑ | ↑ |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chin, K.-Y.; Ima-Nirwana, S. Olives and Bone: A Green Osteoporosis Prevention Option. Int. J. Environ. Res. Public Health 2016, 13, 755. https://doi.org/10.3390/ijerph13080755
Chin K-Y, Ima-Nirwana S. Olives and Bone: A Green Osteoporosis Prevention Option. International Journal of Environmental Research and Public Health. 2016; 13(8):755. https://doi.org/10.3390/ijerph13080755
Chicago/Turabian StyleChin, Kok-Yong, and Soelaiman Ima-Nirwana. 2016. "Olives and Bone: A Green Osteoporosis Prevention Option" International Journal of Environmental Research and Public Health 13, no. 8: 755. https://doi.org/10.3390/ijerph13080755
APA StyleChin, K.-Y., & Ima-Nirwana, S. (2016). Olives and Bone: A Green Osteoporosis Prevention Option. International Journal of Environmental Research and Public Health, 13(8), 755. https://doi.org/10.3390/ijerph13080755