1. Introduction
Heavy metals are a common occurrence in the environment and have resulted in human exposure for the entire history of mankind. However, anthropogenic activities such as mining have resulted in elevated levels of these contaminants in the environment. By definition, any toxic metal may be called a heavy metal, irrespective of its atomic mass or density. The classification includes some metalloids, transition metals, basic metals, lanthanides and actinides and metals of groups III to V of the periodic table [
1]. Examples include As, Pb, Hg, Cd, Cr, Co, Ni, Cu, Zn, Se, Al, Cs, Mn, Mo, Sr, U, Be and Bi [
2].
Some metals are essential to life and play irreplaceable roles as sources of vitamins, and minerals in the functioning of body organs. All living organisms require varying amounts of metals, but become toxic at higher concentrations [
3]. Other metals have no useful role in the human physiology. Examples of such elements are arsenic, lead and mercury. They may be toxic even at low levels of exposure. Once absorbed by the body, heavy metals continue to accumulate in vital organs like the brain, liver, bones, and kidneys, for years or decades causing serious health consequences [
4]. Arsenic, lead and mercury are the first, second and third hazards on the priority list of heavy metal pollutants as designated by the United States Agency for Toxic Substances and Disease Registry [
5].
Arsenic, for instance, is regarded a human carcinogen from extremely low levels of exposure [
6]. Acute exposure to arsenic compounds may cause nausea, vomiting, abdominal pain, muscle cramps and diarrhoea [
7] while chronic exposure is associated with peripheral nerve damage causing diabetes [
8]. Pb on the other hand, is regarded as a human mutagen and probable carcinogen [
9]. It induces renal tumours, and also disturbs the normal functioning of kidneys, joints, reproductive and nervous systems [
10].
The acute ingestion of inorganic Hg potentially causes gastrointestinal disorders, diarrhoea, and haemorrhage [
8]. Repeated and prolonged exposure may seriously affect the kidneys, liver and skin. Cd is known to be toxic even at low concentrations and is also regarded as a probable carcinogen. Severe exposure to Cd may result in pulmonary effects such as bronchiolitis, emphysema, and alveolitis [
4]. Cd can also result in bone fracture, kidney dysfunction, hypertension and even cancer [
11]. Arthritis, diabetes, anaemia, cardiovascular disease, cirrhosis, reduced fertility, headaches and strokes are some of its odd long term effects.
Whereas chromium (III) is an essential element [
9], chromium (VI) compounds are known to be mutagenic and carcinogenic. Breathing high levels of chromium (VI) may cause asthma and shortness of breath. Long term exposure may cause damage to the liver and kidneys. Ni on the other hand is known to cause cancer, both oral and intestinal. It also causes depression, heart attacks, haemorrhages and kidney problems [
7]. Excessive intake of Zn and Cu may cause non-carcinogenic effects on human health, even though they are essential to human life [
12]. Cu surplus had been associated with liver damage while Zn may cause impairment of growth and reproduction [
13].
The Witwatersrand Gold Mining Basin is the world largest that covers an area of 1600 km
2. Mining activities have led to a legacy of some 400 km
2 of mine tailings [
14]. Gold mine tailings in the study area constitute a major source of heavy metal pollution to the environment. Major mechanisms through which heavy metals can be transported from mine tailings are the atmosphere, ground water sources and surface water body. Their accumulation in soil, air, water and edible parts of plants represents a direct pathway for their incorporation into the human food chain. In the study area, air pollution has been reported as a result of soil being blown by wind from mine tailings and the surroundings [
14]. Although no health risk studies have been carried out in the mining area, children of community members have often been reported sick due to chest pains, tuberculosis diarrhoea, cough and itchy skin [
15]. Liefferink [
16] also observed, on frequent occasions, children playing with soil and young mothers eating salt crusts from mine tailings. Although this has been the case, information about heavy metal contamination and their risks is lacking. Therefore, the study aimed to measure the concentration levels of heavy metals in soils from the study area, and to estimate the health risks on the residents. In this study, nine heavy metals, namely As, Pb, Hg, Cd, Cr, Co, Ni, Cu and Zn were included in the measurement.
2. Materials and Methods
2.1. Study Area
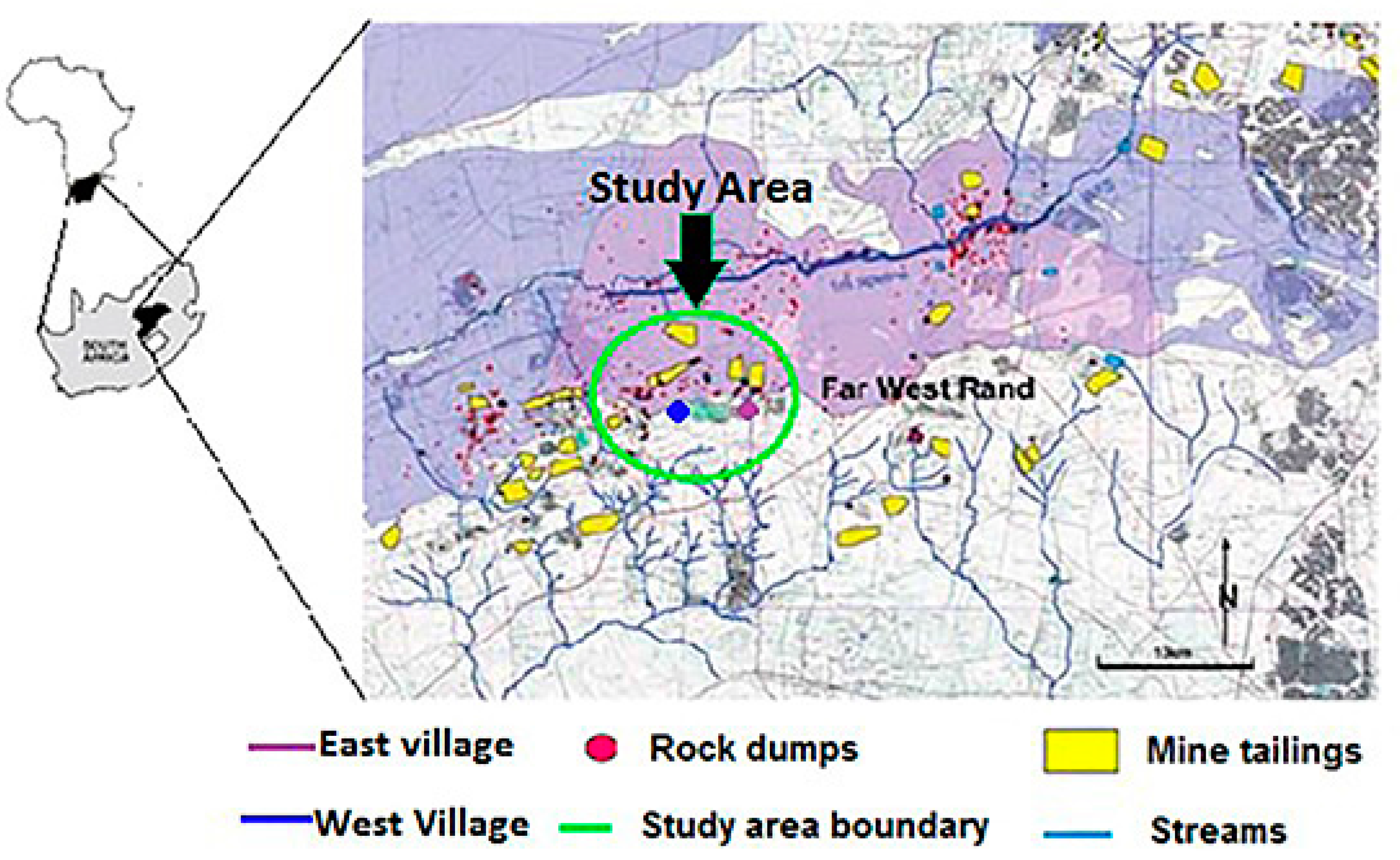
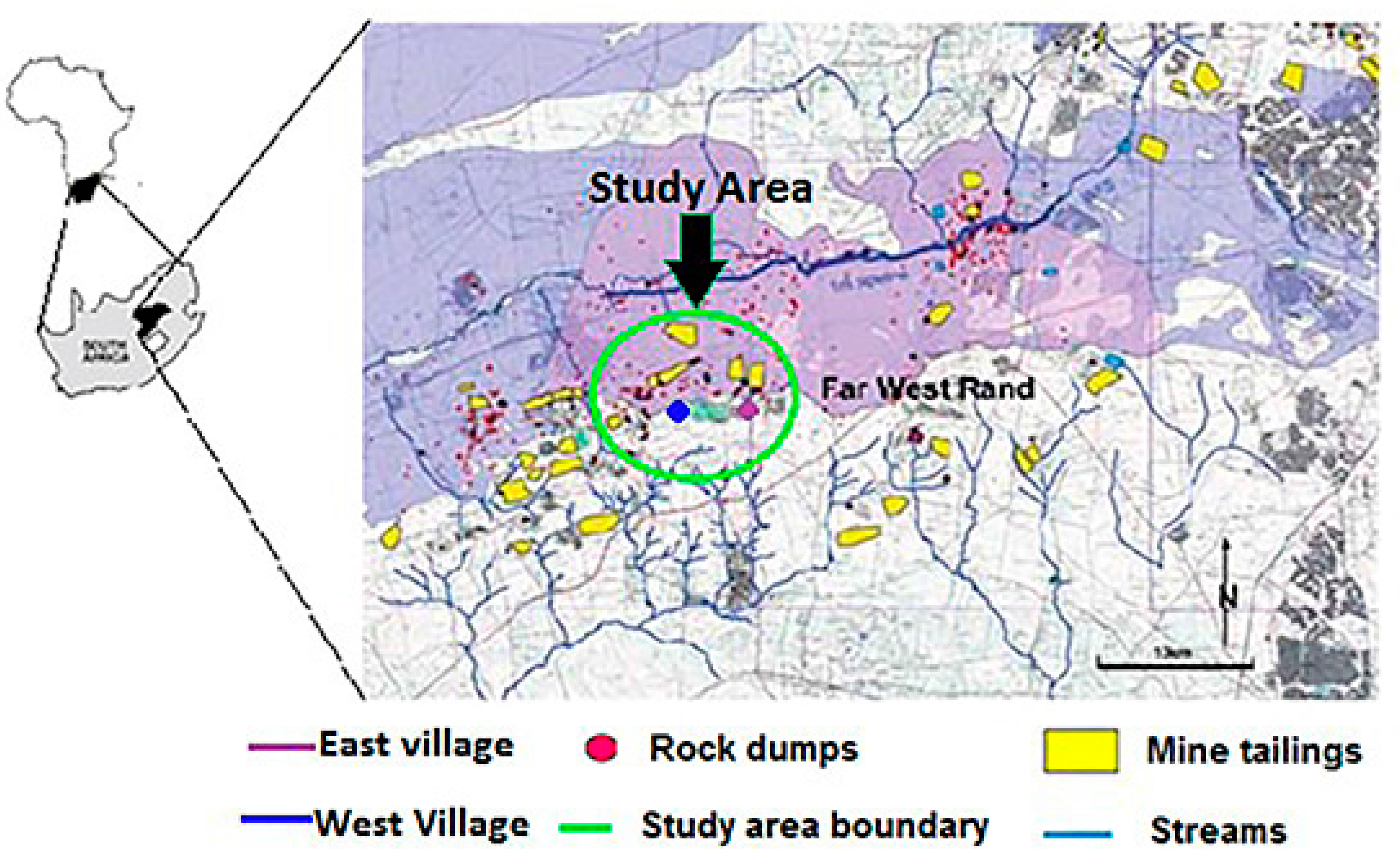
The study area is a gold mining area situated some 70 km west of Johannesburg in the Gauteng Province of South Africa. It lies between 26°18’ S–26°26’ S latitude and 27°23’ E–27°31’ E longitude. Gold exploration in the area dates back to 1898 and mining started from 1945 to date. Geographically the area, which is approximately 86 km
2 is located in the West Wits line (Far West Rand) Goldfield of the Witwatersrand Gold Mining Basin. The study area is densely populated with informal settlements residing close to gold mine tailings. The topography of the area is relatively flat and the vegetation is largely grassland. The climate is temperate, with temperatures averaging 24 °C in summer and 13 °C in winter. Annual rainfall is about 750 mm [
17].
Figure 1 shows the map of the study area.
2.2. Sampling and Sample Preparation
A total of 56 soil samples from five mine tailings and 17 from two mine villages representative of the gold mining area were collected with a steel auger at a depth of 5 cm. At each sampling location, five replicate samples were collected within a 2 m × 2 m grid, thoroughly mixed to obtain a homogenous sample, out of which 1 kg was packaged in polyethylene bags [
18]. All the collected samples were properly marked and identified by their sampling locations using a Global Positioning System (GPS) receiver. The collected soil samples were taken to the laboratory for further processing. A common problem in the analysis of samples for As and Hg is loss during sample preparation. As a precautionary measure, ashing was avoided. At the laboratory, the soil samples were first spread out on a plastic sheet and allowed to air dry for 2–3 days. The samples were then sieved through a 2 mm nylon mesh to obtain a homogenous sample matrix. Close attention was paid to every sample to avoid cross-contamination [
17].
2.3. Soil Sample Analysis
The soil samples were then analysed for heavy metal elements using Inductively Coupled Plasma-Mass Spectrometry (ICP-MS), model PerkinElmer NexION 300 ICP-MS (PerkinElmer, Waltham, MA, USA). Before ICP-MS was done, soil samples were first digested in a Multiwave 3000 microwave system. Digestion is done in order to dissolve the heavy metals from the soil samples. In this process, 1 g dry weight of each soil sample was accurately measured and mixed with 3 mL of nitric acid and 9 mL of hydrochloric acid in a rotor vessel. 1 mL of hydrogen peroxide also added to the mixture. The mixture was then digested at a temperature of 120 °C for about 25 min and then allowed to cool down for about 15 min. After this, the digested samples were transferred into 100 mL volumetric flasks with 2% HNO
3. Deionised water was then used to top up to this volume [
19]. The digested samples were then allowed to sediment overnight and there after filtered with No. 40 Whatman filter paper in readiness for ICP-MS.
The digested samples were then introduced into the ICP-MS, where the sample components were decomposed into their atomic constituents. TotalQuant method was used together with Perkin Elmer Pure Plus NexION Dual Detector Calibration Solution standard. This method has the advantage of high sensitivity (ng × L−1 range), wide linear dynamic detection range and specificity for the accurate detection and quantification of heavy metals. TotalQuant calibration was achieved using 200 µg/L of Al, Ba, Ce, Co, Cu, In, Li, Mg, Mn, Ni, Pb, Tb, U and Zn. The quality of the analytical data was guaranteed by implementing standard quality assurance procedures. Each sample was analysed in duplicates. After every 10 samples, a certified standard and a blank solution were run to check for contamination and drift. All the chemicals and reagents used were of certified analytical grade and procured from Merck (South Africa). The detection limits for As, Pb, Hg, Cd, Cr, Co, Ni, Cu and Zn were 0.015, 0.0003, 0.0003, 0.005, 0.0009, 0.001, 0.006, 0.004 and 0.04 µg/L, respectively. The heavy metal concentrations obtained from the ICP-MS analysis in mg/L were then converted into mg/kg.




{kind=link}
{kind=link}
{kind=link}