1. Introduction
The Fifth Report of the Intergovernmental Panel on Climate Change stated that the average global surface temperature increased linearly by 0.85 °C from 1880 to 2012 [
1]. Therefore, it is highly possible that the frequency and duration of heat waves will increase in the future. Heat-related diseases may affect the health of billions of people at risk, and will likely affect most populations in the coming decades [
2]. The adverse effects of elevated temperature on mortality have been widely reported. For example, in 2012, heat caused more fatalities than any other severe weather event worldwide [
3], and a study from USA reported that 8015 deaths were directly caused by heat waves from 1979 to 1999 [
4]. Other studies have reported that the 1995 heat wave in Chicago was alone responsible for over 800 deaths [
5], and that the heat wave in 2003 across Europe was associated with 22,000 to 35,000 additional deaths [
6]. Heat waves have been reported to introduce health risks in some areas in China. The 2003 heat wave in Shanghai was believed to be associated with high respiratory and cardiovascular mortality rates [
7]. Furthermore, extremely high temperature in Guangzhou was linked with an increase in the risk of death [
8]. Elderly, women, and individuals with pre-existing diseases are considered to be very vulnerable to heat-related illnesses in China [
9,
10]. Therefore, more attention should be paid to the health effects of heat and heat waves.
A “Knowledge, Attitude, and Practice” (KAP) study is performed in a specific population to collect data on what the population knows, believes, and does regarding a certain topic. The public’s attitude to risks, adaptation practices, and knowledge of heat waves are three of the most important factors for reducing the health impact of heat waves [
11,
12]. KAP studies on heat waves have been mostly performed in developed countries [
13,
14,
15], and relatively few studies have been performed in developing countries, especially in China. Yet, according to the Global Climate Risk Index 2014, China is vulnerable to extreme weather events [
16]. Therefore, it is important to understand the Chinese public’s KAP in order to reduce the negative effects of heat waves.
The public’s KAP can be influenced by several aspects, such as climate type, economic level, and public characteristics. Although KAP data are sensitive, the findings can be considered as local indicators that are only representative in a defined and limited area. KAP studies on heat waves have been performed in the south and west regions of China [
12,
17]. However, KAP studies on heat waves have not been performed in the east region. Heat waves have become increasingly common in Jinan City. From 1951 to 2005, 763 days had high temperatures (≥35 °C) [
18]. According to the 2011 Statistical Yearbook of Jinan City, the maximum daily temperature in summer has continuously increased in recent years, and the maximum temperature reached 41.4 °C in the summer of 2009 [
19]. Owing to the continuously high temperature in this region, it is necessary to perform a public survey to evaluate the health impact of heat waves so that the number of deaths from heat waves can be reduced. The results could contribute to the understanding of the public‘s KAP with regard to heat waves, which would in turn provide data to local health authorities and communities for future policy-making and implementation in terms of coping with heat waves and the corresponding adverse effects.
The present study aimed to obtain data in order to better understand the heat wave-related KAP of a population in Licheng District of Jinan City in the northeast region of China. We selected Licheng District as the study area because its demographic characteristics, climate type, and population lifestyle are representative of Jinan City [
19]. The results will be further evaluated so that they can be used to develop policies for coping with heat waves.
2. Methods
2.1. Study Area and Definition of Heat Waves
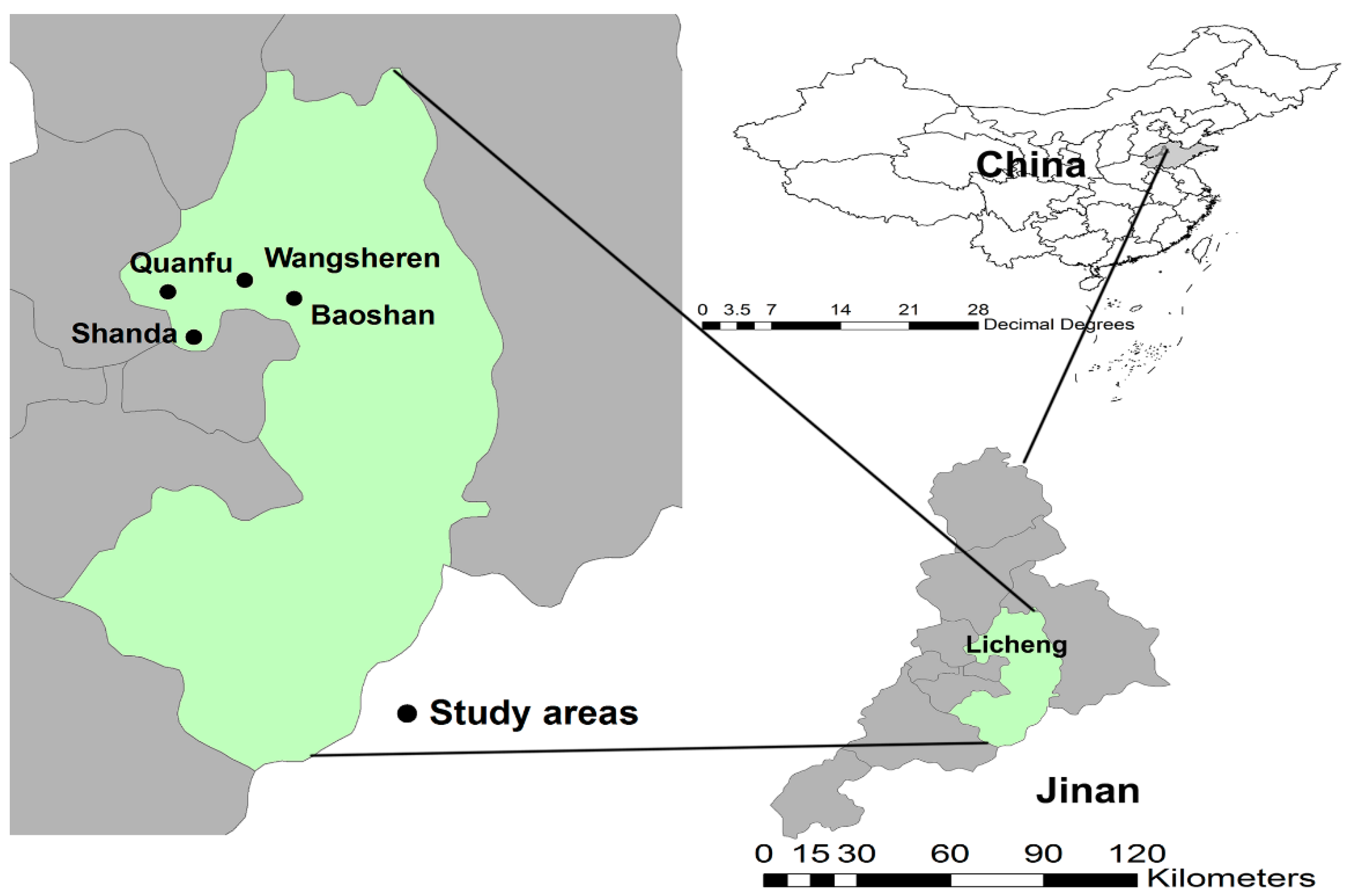
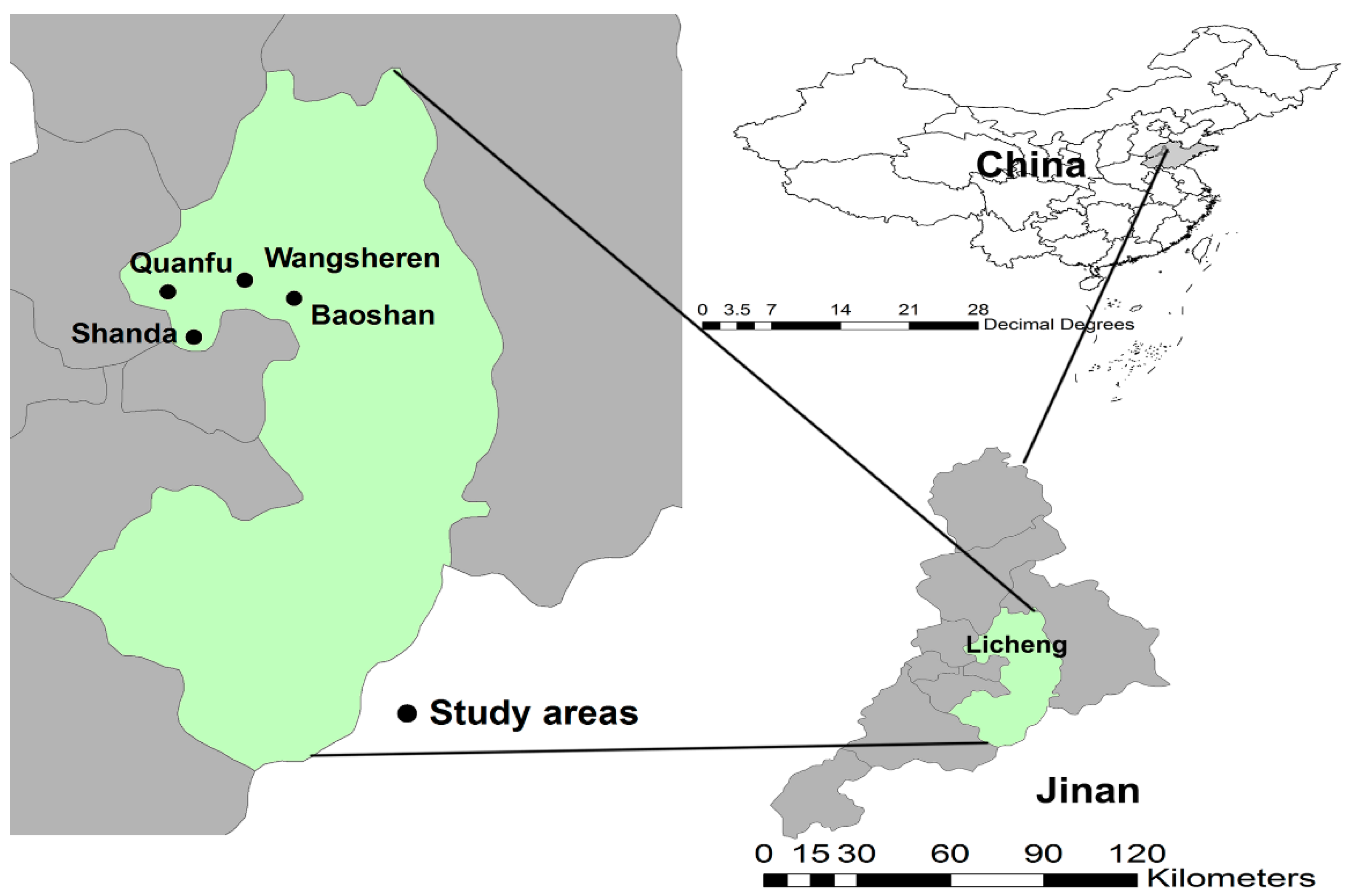
Licheng District is located in the southeast area of Jinan City (geographical coordinates, 36°40′ N and 117°03′ E,
Figure 1). The area of the district is 1298.57 km
2, with a mean elevation of 41 m and a total population of 1.12 million. At the end of 2010, the sex ratio was 99.6:100 (male:female). The climate of the district is characterized as sub-humid and warm, with obvious continental monsoon weather and four distinct seasons. The annual mean temperature, precipitation, and sunshine hours are 13.8 °C, 685 mm, and 5.1 h, respectively. Licheng District has 15 streets, with 47 community resident committees and 655 administrative villages. Individuals living in the communities mainly work in industries and related services, and those living in the villages mainly grow cash crops. Jinan City is called one of the four “ovens”. According to the Chinese Meteorological Administration, a “heat day” is defined as a day when the maximum temperature exceeds 35 °C, and a heat wave is a period of at least three consecutive “heat days” [
7]. This definition was adopted in the present study.
2.2. Study Participants
The multistage sampling method was utilized to select a representative sample in Licheng District. First, the district was divided into an urban area and a rural area according to the density of population and vegetation cover. Then, two streets were selected non-randomly from each area that had similar demographic characteristics and economic status. The four selected streets were Shanda, Quanfu, Baoshan, and Wangsheren (
Figure 1). Shanda and Quanfu were from the urban area, and Baoshan and Wangsheren were from the rural area. We further selected 600 households from each street randomly. Finally, individuals who were over 14 years old and had been living in the selected areas for at least 6 months were considered eligible for inclusion in the present study. One eligible participant was selected from each household using the Kish grid method.
2.3. Data Collection
A questionnaire was drafted after a review of the literature on heat waves and climate change [
13,
15,
17,
20,
21]. Experts were consulted during the development of each question and its response. The following five sections were present in the questionnaire: (1) section “A” (questions on demographic information, such as gender, age, education, and marital status); (2) section “B” (eight questions on knowledge about heat waves); (3) section “C” (one attitude-related question, i.e., whether measures were taken to prevent heatstroke if a high temperature warning had been provided); (4) section “D” (four questions on practices for preventing heat waves and previous experiences of heat-related diseases); and (5) section “E” (questions on economic and social factors, such as dwelling environment, cooling system, and neighborhood relationships).
From 12 to 18 July 2014, each participant was interviewed at home by a well-trained investigator using the structured questionnaire. Various actions were taken to ensure the quality of the questionnaire. First, all interviewers received systematic training for several days before the survey. Training provided the interviewers with an opportunity to become familiar with the survey objectives, content, and plan for implementation in the study. The training mainly included the following areas: survey purpose; roles and responsibilities; content and use of the questionnaires; survey forms and materials; appropriate interviewing techniques, including listening skills and probing techniques; and final pre-testing of the questionnaire. A small-scale pilot study was performed to assess the validity and reliability of the questionnaire. Moreover, the questionnaire and the research methods were thoroughly discussed within the research team. Feedback was carefully reviewed, and appropriate modifications were made to the questionnaire. Furthermore, four senior researchers were always present during questionnaire collection to monitor the process and examine the quality of the data collected.
2.4. Statistical Analysis
There were eight, one, and four questions regarding knowledge (K), attitude (A), and practice (P), respectively. For the K and P sections, the scores were assessed by assigning 1 point to each response of “Yes” and 0 point to response of “No.” For the A section, a 5-point scale was used as the marking scheme, corresponding to the five options of the questions (the options from “not at all” to “very much” were scored from 1 to 5). The score ranges for the K, A, and P sections were 0–8, 1–5, and 0–4, respectively. The total KAP score was the sum of the scores of the three components, and the score range was 1 to 17.
To identify the occurrence of a heat-related illness, which was the dependent variable in our study, every participant was asked if they felt discomfort due to high temperature and visited a doctor; if they showed self-medication behavior to cope with the heat; if they had been diagnosed with heatstroke by a clinical doctor; or if they had any symptoms of heatstroke during the heat wave period in a particular year. Those who responded “yes” to any of the above questions were considered to have experienced heat-related illnesses in this study.
Mean and standard deviation (SD) values were calculated for continuous variables, such as age and KAP score. Categorical variables were computed as a percentage of subjects with the perspective attribute. First, univariate analysis of variance was used to test the association of each demographic characteristic with the K, A, and P scores and the total score. Then, Pearson correlation analysis was performed to clarify the correlations among the K, A, and P scores. In the next stage, participants were divided into three groups according to the K score (<3, 3–5, and >5), two groups according to the A score (<3 and ≥3), and two groups according to the P score (<3 and ≥3). Unconditional logistic regression models (I and II) were used to assess the associations of the K, A, and P scores with heat-related illnesses. Model I assessed the main effects of the K, A, and P scores with heat-related illnesses, without confounding variables, whereas model II assessed the main effects of the K, A, and P scores with heat-related illnesses after adjusting for confounding variables. A product term (K × A, A × P, and K × P) of KAP was further added into the logistic models to test their interaction effects on heat illnesses. The new models were model III (without confounding variables) and model IV (with confounding variables). The interaction effects were analyzed in any two groups of K, A, and P using the low score group as a control. Adjusted confounding variables included sex, age, education level, marital status, occupation, monthly income, and Hukou with a registered permanent residence. All statistical analyses were performed using SPSS 21.0 (SPSS Inc., Chicago, IL, USA), and a p-value < 0.05 was considered statistically significant.
5. Discussion
Studies have found that heat waves or extremely high temperatures have negative effects on human health [
24,
25]. However, few studies have explored the public’s KAP with regard to heat waves. Studies on heat wave-related KAP in China may be greatly significant as China is severely affected by heat events; hence, the findings of such studies may essentially transform or modify political, economic, and social actions so that the effects and risks from global or regional heat wave events can be addressed [
12,
26].
To our knowledge, this is the first study in East China to investigate the public’s KAP with regard to heat waves. The majority of the participants had a high KAP score. However, some subgroups showed low KAP scores because of demographic factors, environmental differences, and different social ties.
In this survey, most participants stated that they would protect themselves on days when the temperature was high. However, this finding is different from the results of a study performed in America [
21] where only about half of the participants protected themselves when the temperature was high. Male participants, young participants, and participants living in rural areas had a low mean A score, although they are considered to be more vulnerable to the effects of heatstroke [
12]. These findings are similar to those of previous studies [
12,
27] that reported a relatively lower risk perception to heat waves among vulnerable populations. These findings may be partially explained by two factors. First, the majority of outdoor employees were young men who may be more willing to take risks and believe that they can handle heat [
21]. Second, rural populations usually have a low level of education and insufficient knowledge, and therefore, they are not aware of methods to protect themselves during high temperature days. Moreover, they do not consider themselves to be vulnerable to heat illnesses. There is an urgent need to take effective actions, such as implementation of education programs about heat waves, to increase awareness among such populations.
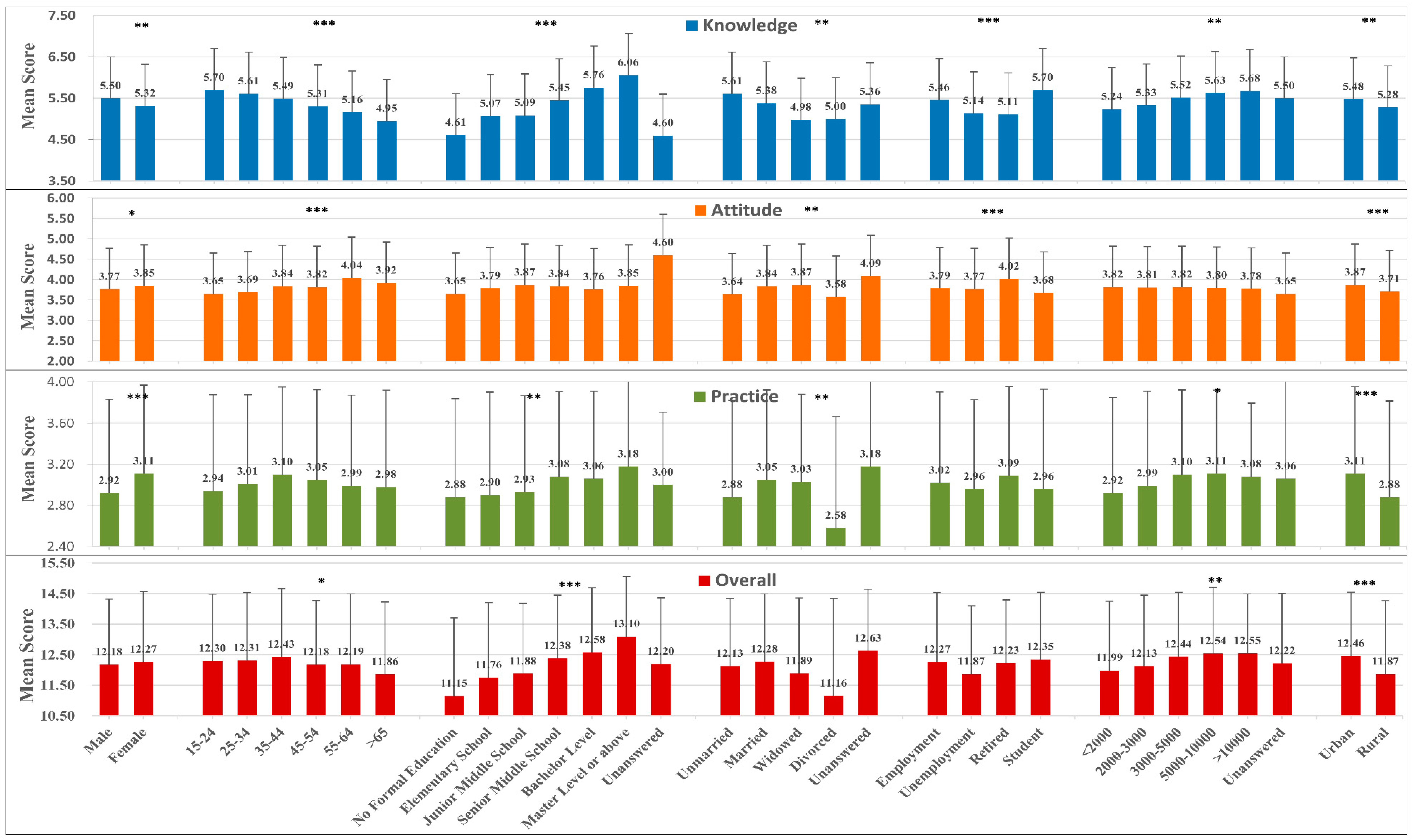
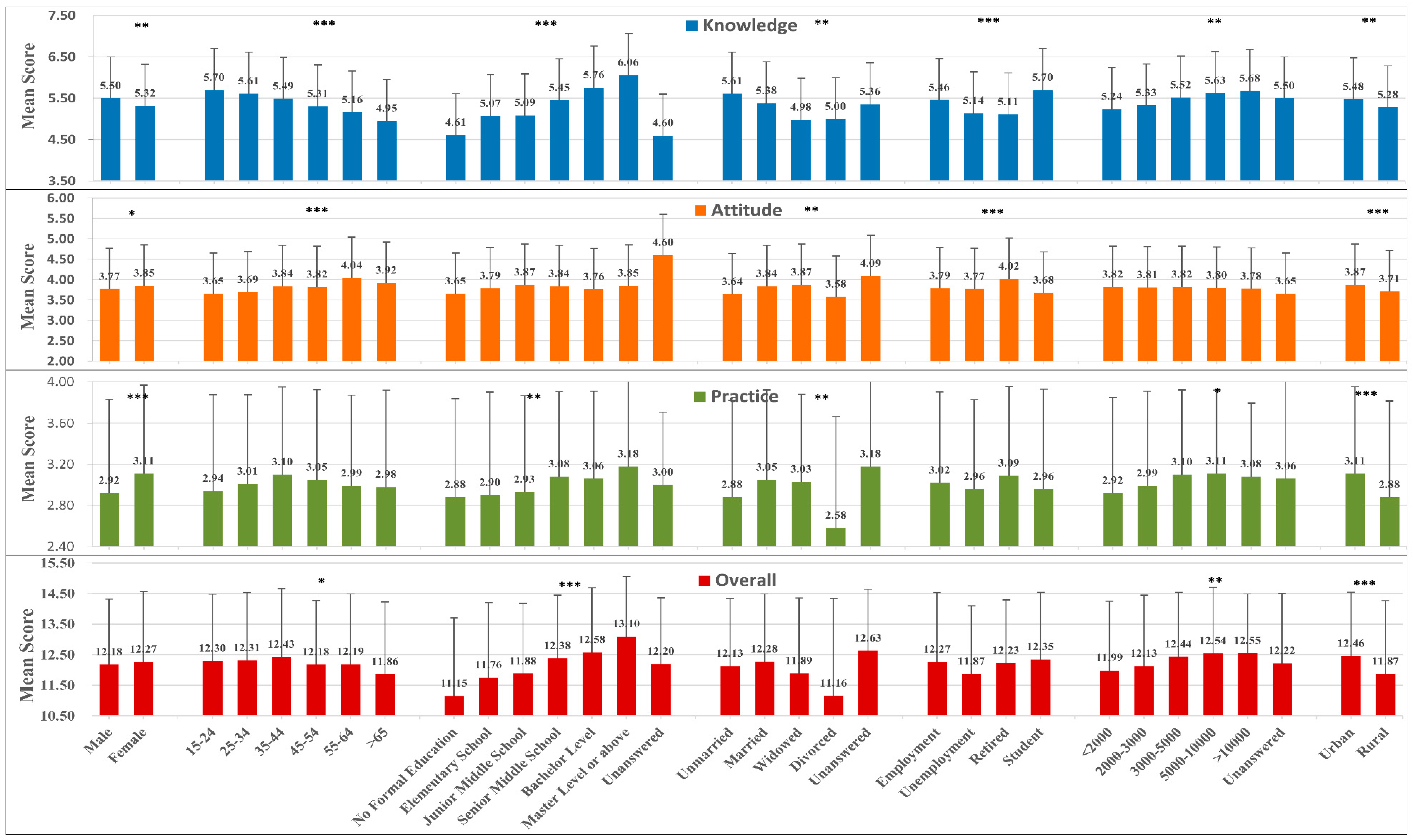
Knowledge is important to reduce the adverse impact of climate change. In the present study, all demographic characteristics of the participants were associated with the K score. Participants with high education levels had high mean K scores. Additionally, the K score was higher among young participants than among old participants, and this may be because young individuals can obtain information on heat waves through more channels. For example, young individuals may access information through educational programs on various media, such as television, radio, the internet, smart phones, and/or newspapers [
28]; whereas, old individuals obtain information mostly through traditional media as they may face challenges and may have to put in more effort when using new technologies, such as the internet and smart phones. Media channels, such as television and radio, should be used to provide information during a heat-wave period in order to reduce the mortality rate among elderly individuals. Government offices should realize that providing educational programs through various methods is very important. Certain age groups do not appear to have adequate ways to access heat wave-related knowledge; moreover, the entire population does not appear to be aware of certain important information. In our survey, the public’s awareness of the causes of the greenhouse effect and rational prescription drug use was rather low, with 26% and 42.2% of the participants providing accurate responses to those questions, respectively. This may be because knowledge regarding these factors is not as common as knowledge regarding the role of green plants in cooling. Hence, people are simply unaware of the importance of such knowledge. Furthermore, local governments may have insufficient resources or may not have taken adequate efforts to raise public awareness by promoting such information. Knowledge may be related to the level of economic development, as high economic status is often associated with high education levels. This could explain why populations in developed countries tend to be aware of the current situation of the global environment [
20,
21,
29]. Therefore, further efforts from individuals, local governments, and national institutions are needed to improve the KAP with regard to heat waves.
The majority of participants took preventive measures during heat waves. However, a considerable number of participants did not take any measures. Additionally, only 56.1% of the participants drank water when they were thirsty, and 11.4% of the participants arranged outdoor activities on days with high temperatures. Sheridan et al. found that only half of the participants drank more water than usual during the warmest parts of the day [
21], and this is consistent with our finding. Perspiration is required to lower body temperatures when the ambient temperature exceeds 34 °C. The best method to overcome excess loss of water is to drink sufficient water so that the perspiration cycle is appropriate. Many participants took personal measures only based on whether they felt thirsty owing to lack of knowledge on perspiration. It is important to determine the most appropriate intake of water, as Yong et al. found that people who had a history of excessive water intake had a high risk of hyponatremia during heat waves [
30]. Fluid intake guided by thirst levels and urination is considered by experts to be appropriate for heat wave protection. Our study also found that the P score was higher in female participants than in male participants. Differences in risk awareness between male and female individuals may explain this difference. Considering the general family-related roles and domestic responsibilities of women, they are more likely to care about the safety of their family members and friends [
28]; hence, they may pay more attention to the safety of their loved ones on days with extreme temperature or weather conditions. It has been shown that stressful events, such as heat-related events, have a greater effect in women than in men [
31]. Therefore, women are more likely to notice changes in the surrounding environment directly by recognizing changes in their own emotional or psychological status or indirectly by warnings from others who recognize their emotionally or psychological changes, and therefore, they can take preventive actions in time. In the present study, the P score was higher in urban populations than in rural populations, and the impact of the urban heat island (UHI) effect cannot be ignored. The UHI effect is a well-documented phenomenon wherein a thermal anomaly exists in urban areas when compared with proximate rural landscapes [
32,
33,
34]. It could cause higher temperatures in urban areas than in places that are less dense and have more vegetation cover, such as rural or suburban areas [
35]. The UHI effect has increased in Jinan City from 1970 to 2012 [
36]. Some studies have suggested that there is a significantly elevated risk of death on hot days in heat island areas [
37,
38,
39]. Therefore, the urban population should not only take protective measures, but also take measures to mitigate the UHI effect.
Pearson correlation analysis indicated that there is limited correlations between K and A scores, and weak correlations between A and P scores, which is consistent with the results of the interactive effect analysis in this study. This finding of a correlation between the A and P scores was consistent with the results of a study by Liu et al. performed in Guangdong, China [
12]. The authors reported that risk perception was positively correlated with adaptive behavior.
A series of multivariate logistic regression analyses were used to assess the main and interactive effects of KAP on heat-related illnesses. As explained earlier, a low K score may be associated with high health risks, and therefore, such individuals may experience severe heat-related illnesses. In addition, the results showed that the main effects of A and P had no significant differences with respect to heat illnesses, which contradicts the expected result. Generally, a positive attitude or perception to heat protection and preventive practice should reduce the adverse effects of high temperature [
12,
40]. In the questionnaire, there were few questions for assessing the A and P scores, which placed uneven weight on the total KAP score. The scores may not be sufficient and effective to identify a correlation of heat illnesses with the A or P score, as well as a relationship among the K, A, and P scores. Therefore, further studies with more questions for assessing the A and P scores are needed to explore their correlations with heat-related illnesses.
Stratified analysis was used to determine the interactive effects among the K, A, and P scores. Among the participants, those with high awareness and those who undertook adaptation practices had a low incidence of heat-related illnesses. Therefore, people who are aware of the importance of a preventive attitude and protective practice may have a low risk of heat-related illnesses. Another important finding is that participants with a high level of protective practice (≥3) but a negative attitude to heat protection (<3) during heat waves had the highest risk of heat illnesses, which is inconsistent with the widespread view that people with low protection awareness and limited adaptation behaviors are usually affected by heat illnesses. We further analyzed the demographic characteristics of this subgroup to determine the reasons for our finding (
Table 5). Most participants in this subgroup had a low income, were from rural areas, and had low education levels. Additionally, most of the participants took actions; however, they had a high prevalence rate of heat illnesses. Therefore, some other factors may have been present. These individuals may not have been able to afford cooling equipment, such as air conditioners, with their low income. Moreover, they may not know how to adapt to heat waves, as few education resources are available in rural areas. Furthermore, owing to the limited transportation resources in rural areas and/or in areas with individuals having a low economic status, the individuals in these areas may not be able to access places, such as shopping malls and natatoriums, which are mainly located in urban areas, to avoid heat in summer. Therefore, more attention should be paid to vulnerable sub-populations, and special adaptation strategies should be designed for such populations.
The present study has some limitations. First, this cross-sectional study only investigated regional KAP; thus, caution should be applied when generalizing the results to other cities or regions of the world. Second, because of the cross-sectional design of the study, a cause-effect relationship between KAP and heat-related illnesses could not be appropriately determined. To further explore the causal relationship between KAP and heat-related illnesses, we performed a quasi-experimental study on KAP in 2015, which is commonly used to measure behavior in communities before and after an intervention. Third, bias was not adequately addressed. For instance, although the interviewers were trained before the survey, there may have been some investigation bias during the interview process. Moreover, recall of previous experiences of heat illness may introduce bias. Furthermore, there may have been social desirability bias, as some participants may have provided answers that they believed were in the favor of the survey. Finally, the KAP approach cannot be used to explore perceptions and attitudes in depth. Despite these limitations, the findings of the present study are useful for policy implementation. In the future, relevant policy makers, such as emergency planners and health professionals, should pay close attention to the protection of the population, especially vulnerable groups. A series of measures can be implemented. First, a multi-level healthcare response network should be established to ensure that patients at the community level are identified and administered timely treatment. Second, the KAP level of community workers who provide special services to community residents should be enhanced. These workers can disseminate knowledge among residents through face-to-face communication. Finally, the government should use all available channels (newspapers, television, radio, the internet, telephone, etc.) to spread heat-related knowledge that will help prevent heat illnesses.



{kind=link}
{kind=link}