
Optimal Decision Model for Sustainable Hospital Building Renovation—A Case Study of a Vacant School Building Converting into a Community Public Hospital

Abstract
:1. Introduction
2. Overview of Hospital Renovation and Energy Use
3. Criteria for Sustainable Hospital Building Renovation Assessment and Rating Rules
3.1. Criteria for Sustainable Hospital Building Renovation
3.2. Assessment and Rating Rules
4. Methods
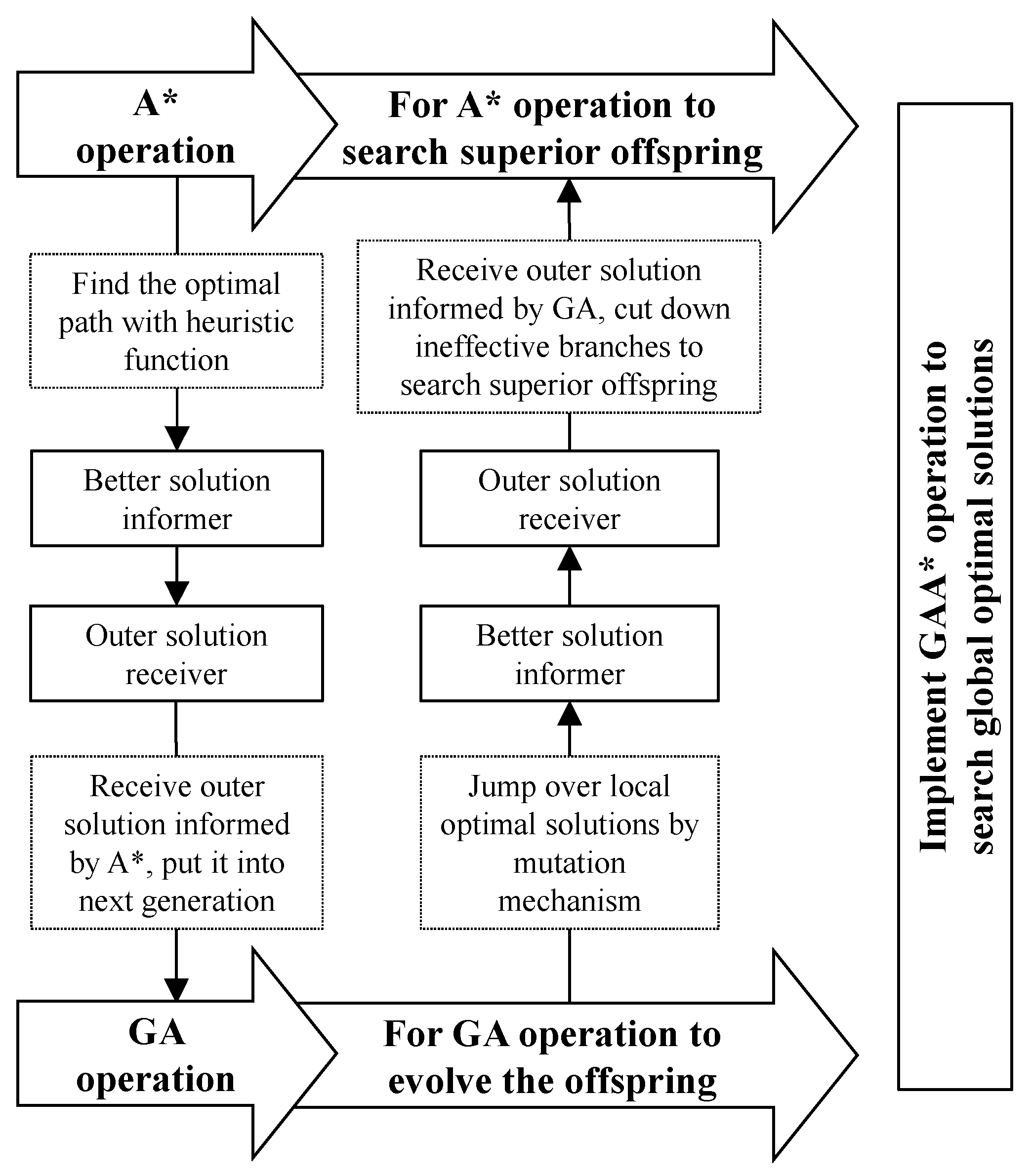
4.1. Genetic Algorithm and A* Search Algorithm
4.2. Hybrid Algorithm (GAA*) for Renovation Solution Optimization
5. Results
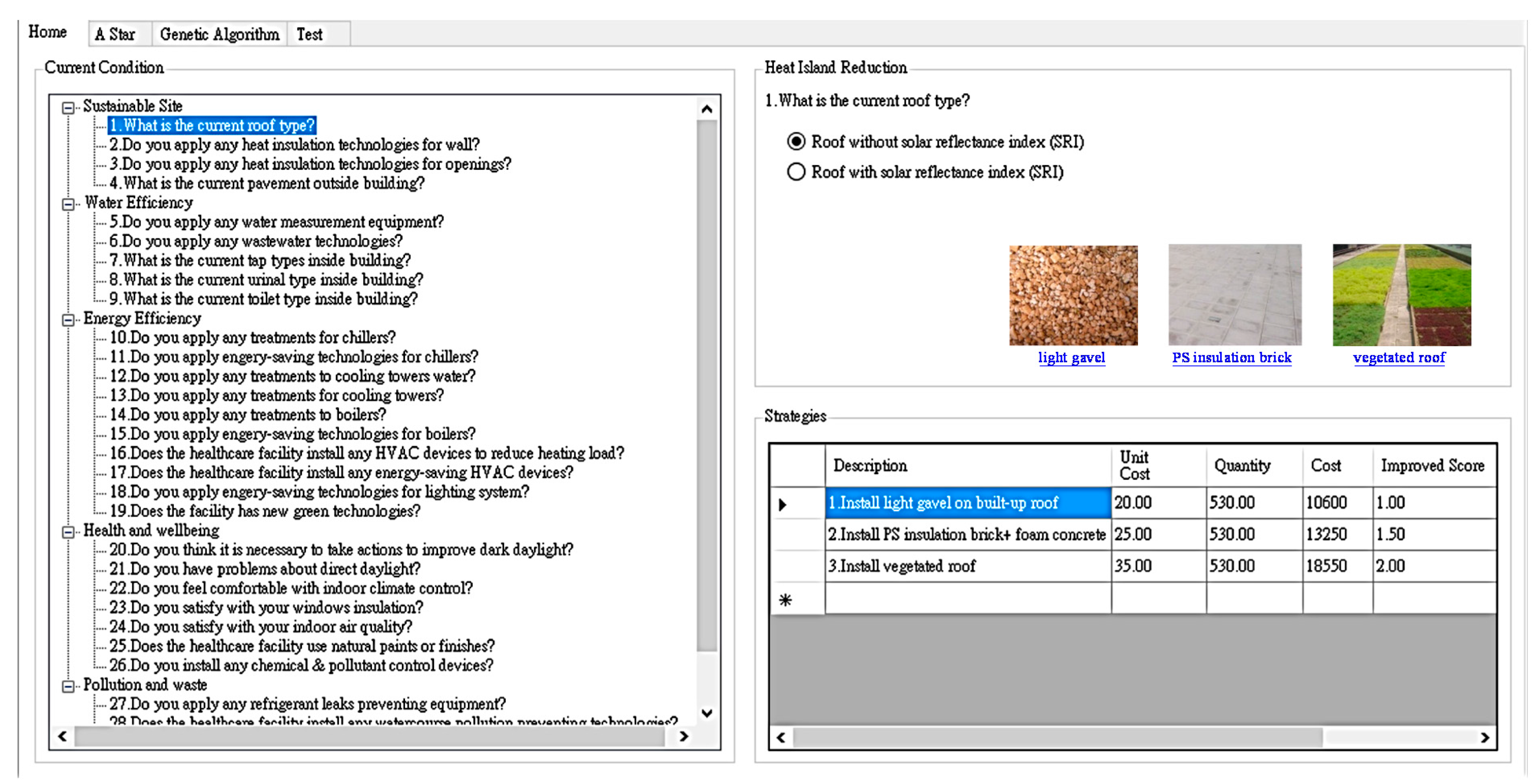
5.1. A Briefing on a Vacant School Building Converting to a Public Community Hospital
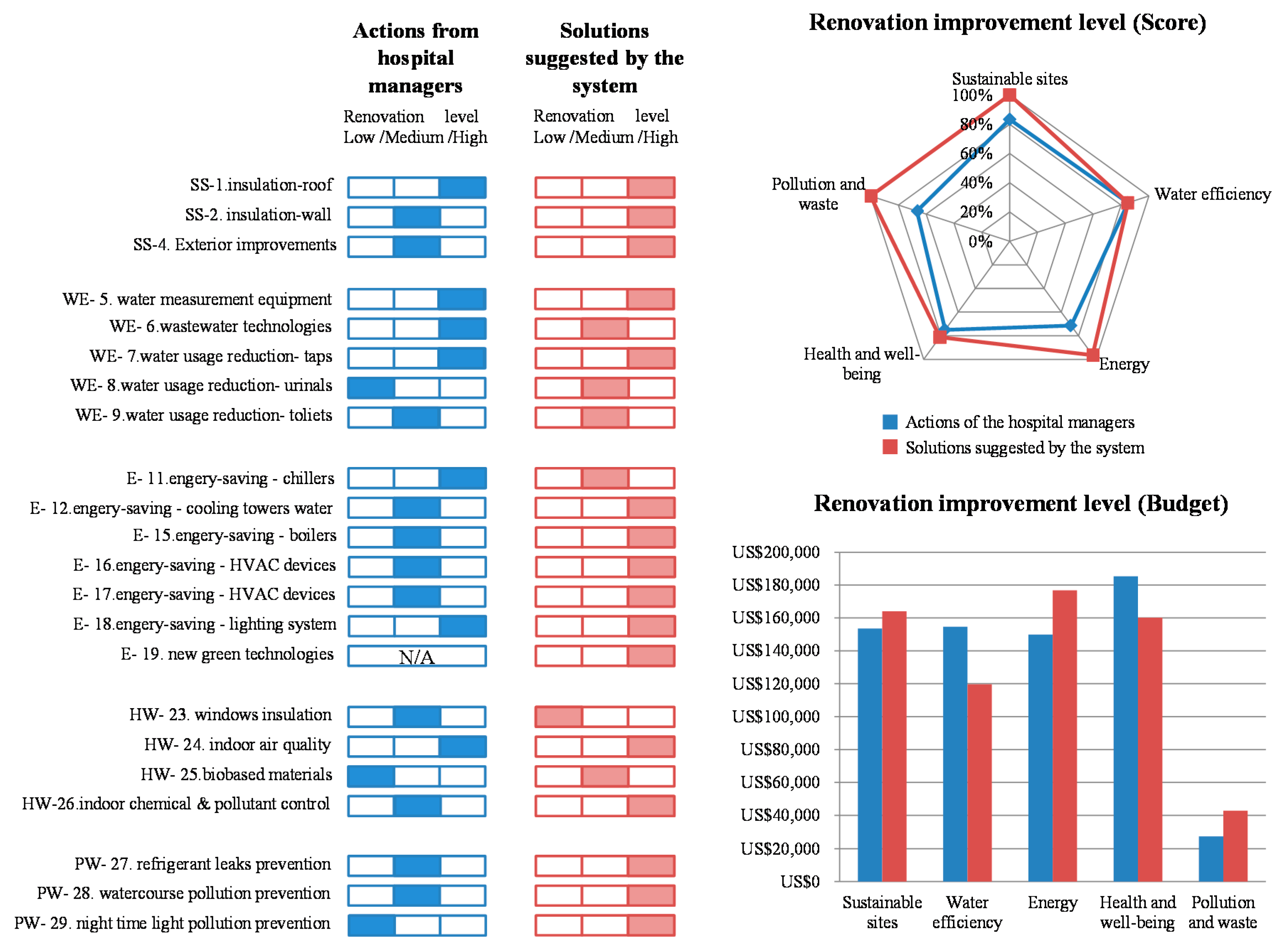
5.2. Comparison Result between the Simulated Project and the System
6. Conclusions and Suggestions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Otter, J.A.; Donskey, C.; Yezli, S.; Douthwaite, S.; Goldenberg, S.D.; Weber, D.J. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: The possible role of dry surface contamination. J. Hosp. Infect. 2015, 92, 235–250. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Jiang, C.; Donovan, C.; Wen, Y.; Wenjie, S. Middle East Respiratory Syndrome and Medical Students: Letter from China. Int. J. Environ. Res. Public Health 2015, 12, 13289–13294. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Summary of Probable SARS Cases with Onset of Illness from: 1 November 2002 to 31 July 2003. Available online: http://www.who.int/csr/sars/country/table2004_04_21/en/ (accessed on 21 April 2004).
- World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV)—Summary of Current Situation, Literature Update and Risk Assessment. Available online: http://apps.who.int/iris/bitstream/10665/179184/2/WHO_MERS_RA_15.1_eng.pdf?ua=1 (accessed on 25 February 2016).
- Mavalankar, D.; Abreub, E. Concepts and techniques for planning and implementing a program for renovation of an emergency obstetric care facility. Int. J. Gynecol. Obstet. 2002, 78, 263–273. [Google Scholar] [CrossRef]
- Ha, K.M. A lesson learned from the MERS outbreak in South Korea in 2015. J. Hosp. Infect. 2016, 92, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Assiri, A.; McGeer, A.; Perl, T.M.; Price, C.S.; Al Rabeeah, A.A.; Cummings, D.A.T.; Alabdullatif, Z.N.; Assad, M.; Almulhim, A.; Makhdoom, H.; et al. Hospital Outbreak of Middle East Respiratory Syndrome Coronavirus. N. Engl. J. Med. 2013, 369, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.C.C.; Chan, J.F.W.; To, K.K.W.; Yuen, K.Y. Clinical management and infection control of SARS: Lessons learned. Antivir. Res. 2013, 100, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, M.; Matilainen, P. Carbon Efficient Building Solutions. Sustainability 2010, 2, 844–858. [Google Scholar] [CrossRef]
- Pérez-Lombard, L.; Ortiz, J.; Pout, C. A review on buildings energy consumption information. Energy Build. 2008, 40, 394–398. [Google Scholar] [CrossRef]
- Setyowati, E.; Harani, A.R.; Falah, Y.N. Green Building Design Concepts of Healthcare Facilities on the Orthopedic Hospital in the Tropics. Proced.-Soc. Behav. Sci. 2013, 101, 189–199. [Google Scholar] [CrossRef]
- Mohareb, E.A.; Kennedy, C.A. Scenarios of technology adoption towards low-carbon cities. Energy Policy 2014, 66, 685–693. [Google Scholar] [CrossRef]
- Karol, E.; Brunner, J. Tools for Measuring Progress towards Sustainable Neighborhood Environments. Sustainability 2009, 1, 612–627. [Google Scholar] [CrossRef]
- Juan, Y.K.; Gao, P.; Wang, J. A hybrid decision support system for sustainable office building renovation and energy performance improvement. Energy Build. 2010, 42, 290–297. [Google Scholar] [CrossRef]
- Brandt, E.; Rasmussen, M.H. Assessment of building conditions. Energy Build. 2002, 34, 121–125. [Google Scholar] [CrossRef]
- Dascalaki, E.; Balaras, C.A. Xenios—A methodology for assessing refurbishment scenarios and the potential of application of RES and RUE in hotels. Energy Build. 2004, 36, 1091–1105. [Google Scholar] [CrossRef]
- Erhorn, H.; Mroz, T.; Mørck, O.; Schmidt, F.; Schoff, L.; Thomsen, K.E. The Energy Concept Adviser—A tool to improve energy efficiency in educational buildings. Energy Build. 2008, 40, 419–428. [Google Scholar] [CrossRef]
- Jaggs, M.; Palmer, J. Energy performance indoor environmental quality retrofit—A European diagnosis and decision making method for building refurbishment. Energy Build. 2000, 31, 97–101. [Google Scholar] [CrossRef]
- Jensen, P.A.; Maslesa, E. Value based building renovation—A tool for decision-making and evaluation. Build. Environ. 2015, 92, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Steskens, P.; Vanhellemont, Y.; Roels, S.; Van Den Bossche, N. A Decision Making Tool for the Energy Efficient Refurbishment of Residential Buildings. Energy Proced. 2015, 78, 997–1002. [Google Scholar] [CrossRef]
- Stockley, J.M.; Constantine, C.E.; Orr, K.E. The Association of Medical Microbiologists’ New Hospital Developments Project Group. Building new hospitals: A UK infection control perspective. J. Hosp. Infect. 2006, 62, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Bartley, J.M.; Olmsted, R.N.; Haas, J. Current views of health care design and construction: Practical implications for safer, cleaner environments. Am. J. Infect. Control 2010, 38, S1–S12. [Google Scholar] [CrossRef] [PubMed]
- Dettenkofer, M.; Ammo, A.; Astagneau, P.; Dancer, S.J.; Gastmeier, P.; Harbarth, S.; Humphreys, H.; Kern, W.V.; Lyytikäinen, O.; Sax, H.; et al. Infection control—A European research perspective for the next decade. J. Hosp. Infect. 2011, 77, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Qian, H.; Li, Y.; Seto, W.H.; Ching, P.; Ching, W.H.; Sun, H.Q. Natural ventilation for reducing airborne infection in hospitals. Build. Environ. 2010, 45, 559–565. [Google Scholar] [CrossRef]
- Mathur, P. Surveillance systems for health care associated infections. J. Patient Saf. Infect. Control 2015, 3, 4–11. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kwak, Y.G.; Yoo, H.; Lee, S.O.; Kim, H.B.; Han, S.H.; Choi, H.J.; Kim, Y.K.; Kim, S.R.; Kim, T.H.; et al. Trends in the incidence rate of device-associated infections in intensive care units after the establishment of the Korean Nosocomial Infections Surveillance System. J. Hosp. Infect. 2015, 91, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Manning, M.L.; Pogorzelska-Maziarz, M. Infection surveillance systems in primary health care: A literature review. Am. J. Infect. Control 2016, in press. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Fusco, F.M.; Schilling, S.; De Iaco, G.; Gottschalk, R.; Brodt, H.R.; Bannister, B.; Brouqui, P.; Thomson, G.; Puro, V.; et al. Infection control practices in facilities for highly infectious diseases across Europe. J. Hosp. Infect. 2012, 81, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Rani, N.A.A.; Baharum, M.R.; Akbar, A.R.N.; Nawawi, A.H. Perception of Maintenance Management Strategy on Healthcare Facilities. Proced.-Soc. Behav. Sci. 2015, 170, 272–281. [Google Scholar] [CrossRef]
- Yang, J.; Peng, H. Decision support to the application of intelligent building technologies. Renew. Energy 2001, 22, 67–77. [Google Scholar] [CrossRef]
- Zavadskas, E.K.; Bejder, E.; Kaklauskas, A. Raising the efficiency of the building lifetime with special emphasis on maintenance. Facilities 1998, 16, 334–340. [Google Scholar] [CrossRef]
- Burton, S.; Sala, M. Energy Efficient Office Refurbishment; Earthscan: London, UK, 2001. [Google Scholar]
- Energy Star of the U.S. Environmental Protection Agency (EPA). U.S. Energy Use Intensity by Property Type. Available online: https://portfoliomanager.energystar.gov/pdf/reference/US%20National%20Median%20Table.pdf (accessed on 29 January 2016).
- Ramesh, T.; Prakash, R.; Shukla, K.K. Life cycle energy analysis of buildings: An overview. Energy Build. 2010, 42, 1592–1600. [Google Scholar] [CrossRef]
- Juan, Y.K.; Kim, J.H.; Roper, K.; Castro-Lacouture, D. GA-based decision support system for housing condition assessment and refurbishment strategies. Autom. Constr. 2009, 18, 394–401. [Google Scholar] [CrossRef]
- Xu, J.; Kim, J.H.; Hong, H.; Koo, J. A systematic approach for energy efficient building design factors optimization. Energy Build. 2015, 89, 87–96. [Google Scholar] [CrossRef]
- Schwartz, Y.; Raslan, R. Variations in results of building energy simulation tools, and their impact on BREEAM and LEED ratings: A case study. Energy Build. 2013, 62, 350–359. [Google Scholar] [CrossRef]
- U.S. Green Building Council—LEED 2009 for Health Care. Available online: http://www.usgbc.org/resources/leed-2009-health-care-current-version (accessed on 4 May 2015).
- GGHC (Green Guide for Health Care). Available online: http://www.gghc.org/about.objectives.php (accessed on 19 April 2015).
- BREEAM UK New Construction 2014 Technical Manual. Available online: http://www.breeam.org/BREEAMUK2014SchemeDocument/ (accessed on 6 May 2015).
- Gowri, K. Green building rating systems: An overview. ASHRAE J. 2004, 46, 56–59. [Google Scholar]
- Lee, W.L.; Burnett, J. Benchmarking energy use assessment of HK-BEAM, BREEAM and LEED. Build. Environ. 2008, 43, 1882–1891. [Google Scholar] [CrossRef]
- Javadi, A.A.; Farmani, R.; Tan, T.P. A hybrid intelligent genetic algorithm. Adv. Eng. Inform. 2005, 19, 255–262. [Google Scholar] [CrossRef]
- Li, H.; Love, P.E.D.; Ogunlana, S. Genetic algorithm compared to nonlinear optimization for labour and equipment assignment. Build. Res. Inf. 1998, 26, 322–329. [Google Scholar] [CrossRef]
- Lee, C.K.; Kim, S.K. GA-based algorithm for selecting optimal repair and rehabilitation methods for reinforced concrete (RC) bridge decks. Autom. Constr. 2007, 16, 153–164. [Google Scholar] [CrossRef]
- Preechakul, C.; Kheawhom, S. Modified genetic algorithm with sampling techniques for chemical engineering optimization. J. Ind. Eng. Chem. 2009, 15, 110–118. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, X.P.; Wang, Q. Hybrid genetic algorithm for permutation flowshop scheduling problems with total flowtime minimization. Eur. J. Oper. Res. 2009, 196, 869–876. [Google Scholar] [CrossRef]
- Dechter, R.; Pearl, J. Generalized best-first search strategies and the optimality of A*. J. Assoc. Comput. Mach. 1985, 32, 505–536. [Google Scholar] [CrossRef]
- Russell, S.; Norvig, P. Artificial Intelligence: A Modern Approach; Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Yung, E.H.; Chan, E.H. Implementation challenges to the adaptive reuse of heritage buildings: Towards the goals of sustainable, low carbon cities. Habitat Int. 2012, 36, 352–361. [Google Scholar] [CrossRef]
- Munarim, U.; Ghisi, E. Environmental feasibility of heritage buildings rehabilitation. Renew. Sustain. Energy Rev. 2016, 58, 235–249. [Google Scholar] [CrossRef]
- Highfield, D.; Gorse, C. Refurbishment and Upgrading of Buildings; Taylor & Francis: London, UK, 2009. [Google Scholar]
- Langston, C.; Yung, E.H.K.; Chan, E.H.W. The application of ARP modelling to adaptive reuse projects in Hong Kong. Habitat Int. 2013, 40, 233–243. [Google Scholar]
- Su, C.J.; Chiang, C.Y. IAServ: An Intelligent Home Care Web Services Platform in a Cloud for Aging-in-Place. Int. J. Environ. Res. Public Health 2013, 10, 6106–6130. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.H.; Yu, J.U.; Huang, C.H. Theoretical System Dynamics Modeling for Taiwan Pediatric Workforce in an Era of National Health Insurance and Low Birth Rates. Pediatr. Neonatol. 2013, 54, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education R.O.C. 2013; Prediction Report of Student Numbers for Public School Education 2013–2128. (In Chinese). Available online: https://stats.moe.gov.tw/files/analysis/102basicstudent.pdf (accessed on 21 November 2013). [Google Scholar]
- Sukkird, V.; Shirahada, K. Technology challenges to healthcare service innovation in aging Asia: Case of value co-creation in emergency medical support system. Technol. Soc. 2015, 43, 122–128. [Google Scholar] [CrossRef]
- Srichuae, S.; Nitivattananon, V.; Perera, R. Aging society in Bangkok and the factors affecting mobility of elderly in urban public spaces and transportation facilities. IATSS Res. 2015, in press. [Google Scholar] [CrossRef]
- Fang, F.E.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.; Zhu, X.; Preedy, V.; Lu, H.; Bohr, V.A.; et al. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.P.; Choi, Y.J.; Moon, G.J.; Byun, N.H.; Choi, S.P. Reusing Vacant Public Buildings for Social Integration—Focusing on the Conversion of Dong-Offices and Primary Schools into “Housing-Mixed Public Facilities”. J. Korean Hous. Assoc. 2010, 21, 1–11. [Google Scholar] [CrossRef]
- Yu, H.J. Study on the Vacant Classrooms Use for Elementary School and Junior High School as the Decline of Natality (in Chinese); Architecture and Building Research Institute, Ministry of the Interior: Taipei, Taiwan, 2006.
- Lin, Z.; Yu, Z.; Zhang, L. Performance outcomes of balanced scorecard application in hospital administration in China. China Econ. Rev. 2014, 30, 1–15. [Google Scholar] [CrossRef]
- Zimring, C.; Joseph, A.; Nicoll, G.L.; Tsepas, S. Influences of building design and site design on physical activity. Am. J. Prev. Med. 2005, 28, 186–193. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sustainable Hospital Building Renovation Criteria | LEED for Healthcare | BREEAM (Healthcare) | GGHC |
|---|---|---|---|
| Regional priority | Management | Transportation operations | |
| Transport | |||
| Sustainable sites | Sustainable sites | Land use and ecology | Environmental service |
| Water efficiency | Water efficiency | Water | Water efficiency |
| Energy | Energy and atmosphere | Energy | Energy and atmosphere |
| Health and well-being | Indoor environmental quality | Materials | Materials and resources |
| Materials and resources | Health and wellbeing | Chemical management | |
| Pollution and waste | Waste | Waste management | |
| Pollution | |||
| Innovation | Innovation | Innovation |
| Criteria | Sub-Criteria | Assessment Items |
|---|---|---|
| Sustainable sites | Heat island reduction | Building roof, wall and opening |
| Exterior improvement | Paving type | |
| Water efficiency | Water performance measurement | Water measurement equipment |
| Wastewater technologies | Water technologies | |
| Water use reduction | Current urinal and toilet type | |
| Energy | HVAC system | Energy-saving technologies and treatments for chillers, cooling towers, boilers and HVAC devices. Energy- reducing heating load technologies for HVAC devices. |
| Lighting system | Lighting systems technologies | |
| Innovative technologies | New green technologies | |
| Health and well-being | Daylight | Daylight control |
| Occupant comfort | Climate control, windows insulation, indoor air quality | |
| Indoor chemical and pollution control | Chemical and pollution control devices | |
| Pollution and waste | Pollution | Preventing technologies or devices for refrigerant, water course and night time light pollution. |
| Waste | Waste storage management |
| Criteria | Current Condition | Assessment Description | Assessment Score (before Renovation) | Improved Score (after Renovation) | |
|---|---|---|---|---|---|
| Water Efficiency—Water use reduction | 7. What are the current tap types inside facility? | Yes (satisfy current conditions) | 1 | 0 | |
| No (need to take renovation actions) | 0 | 1–2 | |||
| Renovation strategies | Renovation level | Cost (per unit) | Improved score | ||
| 1. Tap with water-efficiency | Low level solutions for renovation | 100 per each | 1 | ||
| 2. Tap with automatic sensor | Medium level solutions for renovation | 140 per each | 1.5 | ||
| 3. Install “1” + “2” | High level solutions for renovation | 200 per each | 2 | ||
| Criteria | Current Condition | Assessment Scores |
|---|---|---|
| Sustainable site | ||
| Heat Island Reduction—roof | 1. Current building roof materials is not with solar reflectance index (SRI) | 0 |
| Heat Island Reduction—wall | 2. No heat insulation technologies for walls | 0 |
| Heat Island Reduction—opening | 3. Heat insulation technologies for openings are totally adopted | 1 |
| Exterior improvements | 4. Current pavement outside building is not eco- pavement | 0 |
| Water efficiency | ||
| Water performance measurement | 5. Water measurement equipment is not adopted | 0 |
| Wastewater technologies | 6. No wastewater technologies | 0 |
| Water use reduction | 7. Efficient tap type is not totally adopted | 0 |
| 8. Efficient with less water urinal type is not totally adopted | 0 | |
| 9. Efficient toilet type is not totally adopted | 0 | |
| Energy | ||
| HVAC system | 10. Treatment for chillers is adopted | 1 |
| 11. No energy-saving technologies for chillers | 0 | |
| 12. Cooling towers water treatment is not adopted | 0 | |
| 13. Treatment for cooling towers is adopted | 1 | |
| 14. Treatment for boilers is adopted | 1 | |
| 15. No energy-saving technologies for boilers | 0 | |
| 16. HVAC devices used to reduce heating load are not installed | 0 | |
| 17. No energy-saving technologies for HVAC devices | 0 | |
| Lighting system | 18. Energy-saving technologies for lighting system is not adopted | 0 |
| Innovative technology | 19. No new green technologies in the building | 0 |
| Health and wellbeing | ||
| Daylight | 20. Not necessary to improve daylight piping to interior | 1 |
| 21. No direct daylight | 1 | |
| Occupant comfort | 22. Indoor climate control is fine | 1 |
| 23. Window insulation is required | 0 | |
| 24. Improving IAQ (indoor air quality) is required | 0 | |
| Biobased materials | 25. No natural paints or finishes | 0 |
| Indoor chemical & pollutant control | 26. Indoor chemical & pollutant control devices are not totally installed | 0 |
| Pollution and waste | ||
| Pollution | 27. No refrigerant leak preventing equipment | 0 |
| 28. No watercourse pollution preventing technologies | 0 | |
| 29. Night time light pollution preventing technologies are not totally adopted | 0 | |
| Waste | 30. Good management for recyclable waste storage is adopted | 1 |
| Total assessment score | 8 | |
| Criteria | Improved Items | Actions from Hospital Building Managers (M) | Actions from the System (S) | Improved Scores (M/S) |
|---|---|---|---|---|
| Sustainable site | ||||
| Heat Island Reduction—roof | 1. Building roof type | Install vegetated roof | Install vegetated roof | 2/2 |
| Heat Island Reduction—wall | 2. Wall insulation technologies | Install heat insulation coating | Install heat insulation board | 1.5/2 |
| Exterior improvements | 4. Eco-pavement | Install Porous unit paving | Install Turf blocks | 1.5/2 |
| Water efficiency | ||||
| Water performance measurement | 5. Water measurement equipment | Install water meters + automatic leak detectors | Install water meters + automatic leak detectors | 2/2 |
| Wastewater technologies | 6. Wastewater technologies | Install rainwater capture system + graywater recycling system + wastewater treatment system | Install rainwater capture system + wastewater treatment system | 2/1.5 |
| Water use reduction | 7. Efficient tap type | Tap with water-efficiency and automatic sensor | Tap with water-efficiency and automatic sensor | 2/2 |
| 8. Efficient with less water urinal type | Install waterless urinal | Install water-free urinal | 1/1.5 | |
| 9. Efficient toilet type | Install vacuum toilet system | Install vacuum toilet system | 1.5/1.5 | |
| Energy | ||||
| HVAC system | 11. Energy-saving technologies for chillers | Install Variable Water Volume System + Variable Air Volume System + Chiller amount controlling + use of ice tanks + Heat recovery chiller system | Install Variable Water Volume System + Variable Air Volume System + Chiller amount controlling + use of ice tanks | 2/1.5 |
| 12. Cooling towers water treatment | Medicament treatment | Ozone treatment | 1.5/2 | |
| 15. Energy-saving technologies for boilers | Install CO2 sensors + Warm-keeping of pipes + air preheater + Cool-condensed water recycling | Install CO2 sensors + Warm-keeping of pipes + air preheater + Cool-condensed water recycling + waste heat recovery | 1.5/2 | |
| 16. Energy-reducing heating load technologies for HVAC devices | Install CO2 sensors + Outside Air Economizer | Install CO2 sensors + Outside Air Economizer + Heat recovery chiller system | 1.5/2 | |
| 17. Energy-saving technologies for HVAC devices | Ductwork insulation and sealing + Variable Water Volume System + Variable Air Volume System + Variable Refrigerant Volume System + Cooling water recycling | Ductwork insulation and sealing + Variable Water Volume System + Variable Air Volume System + Variable Refrigerant Volume System + Cooling water recycling + Thermal storage system | 1.5/2 | |
| Lighting system | 18. Energy-saving technologies for lighting system | High performance lamps and electronic ballasts + Illumination meters and illumination rationalization + Manual-on, automatic-off sensors | High performance lamps and electronic ballasts + Illumination meters and illumination rationalization + Manual-on, automatic-off sensors | 2/2 |
| Innovative technology | 19. New green technologies | N/A | Building energy management system | 0/2 |
| Health and wellbeing | ||||
| Occupant comfort | 23. Windows’ insulation | Install double-glazed with low-e coatings | Install solar-control window film | 1.5/1 |
| 24. Improving IAQ (indoor air quality) | Temperature auto-regulator + Air filter maintenance | Temperature auto-regulator + Air filter maintenance | 2/2 | |
| Biobased materials | 25. Natural paints or finishes | Natural paints and adhesive | Apply low-odor finishes | 1/1.5 |
| Indoor chemical & pollutant control | 26. Indoor chemical & pollutant control devices | Utilize entryway systems + Isolated exhaust system for pollutant areas | Install and maintain air filtration media + Utilize entryway systems + Isolated exhaust system for pollutant areas | 1.5/2 |
| Pollution and waste | ||||
| Pollution | 27. Refrigerant leak preventing equipment | Install refrigerant leak detection meters | Ductwork sealing and install refrigerant leak detection meters | 1.5/2 |
| 28. Watercourse pollution preventing technologies | Install leaks detectors + Oil separators maintenance | Install leaks detectors + Oil separators maintenance + Shut-off valves fitted to the site drainage system | 1.5/2 | |
| 29. Night time light pollution preventing technologies | Automatic-off timers for external lighting 23:00–07:00 (except for safety and security lighting) | Automatic-off timers for external lighting 23:00–07:00 (except for safety and security lighting) + Ultrared rays automatic-on for stairway and hallway at night | 1/2 | |
| Total assessment score | 33.5/44 | 40.5/44 | 33.5/40.5 | |
| Budget (US$) | 671,166 | 663,686 | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juan, Y.-K.; Cheng, Y.-C.; Perng, Y.-H.; Castro-Lacouture, D. Optimal Decision Model for Sustainable Hospital Building Renovation—A Case Study of a Vacant School Building Converting into a Community Public Hospital. Int. J. Environ. Res. Public Health 2016, 13, 630. https://doi.org/10.3390/ijerph13070630
Juan Y-K, Cheng Y-C, Perng Y-H, Castro-Lacouture D. Optimal Decision Model for Sustainable Hospital Building Renovation—A Case Study of a Vacant School Building Converting into a Community Public Hospital. International Journal of Environmental Research and Public Health. 2016; 13(7):630. https://doi.org/10.3390/ijerph13070630
Chicago/Turabian StyleJuan, Yi-Kai, Yu-Ching Cheng, Yeng-Horng Perng, and Daniel Castro-Lacouture. 2016. "Optimal Decision Model for Sustainable Hospital Building Renovation—A Case Study of a Vacant School Building Converting into a Community Public Hospital" International Journal of Environmental Research and Public Health 13, no. 7: 630. https://doi.org/10.3390/ijerph13070630