
Factors Affecting Parent’s Perception on Air Quality—From the Individual to the Community Level

 ,
,
Abstract
:
1. Introduction
2. Methods
2.1. Study Subjects
2.2. Perceived Air Quality and Scientifically-Monitored Air Quality
2.3. Quality Control
2.4. Data Analysis
2.5. Ethical Issues
3. Results
3.1. General Information of Subjects
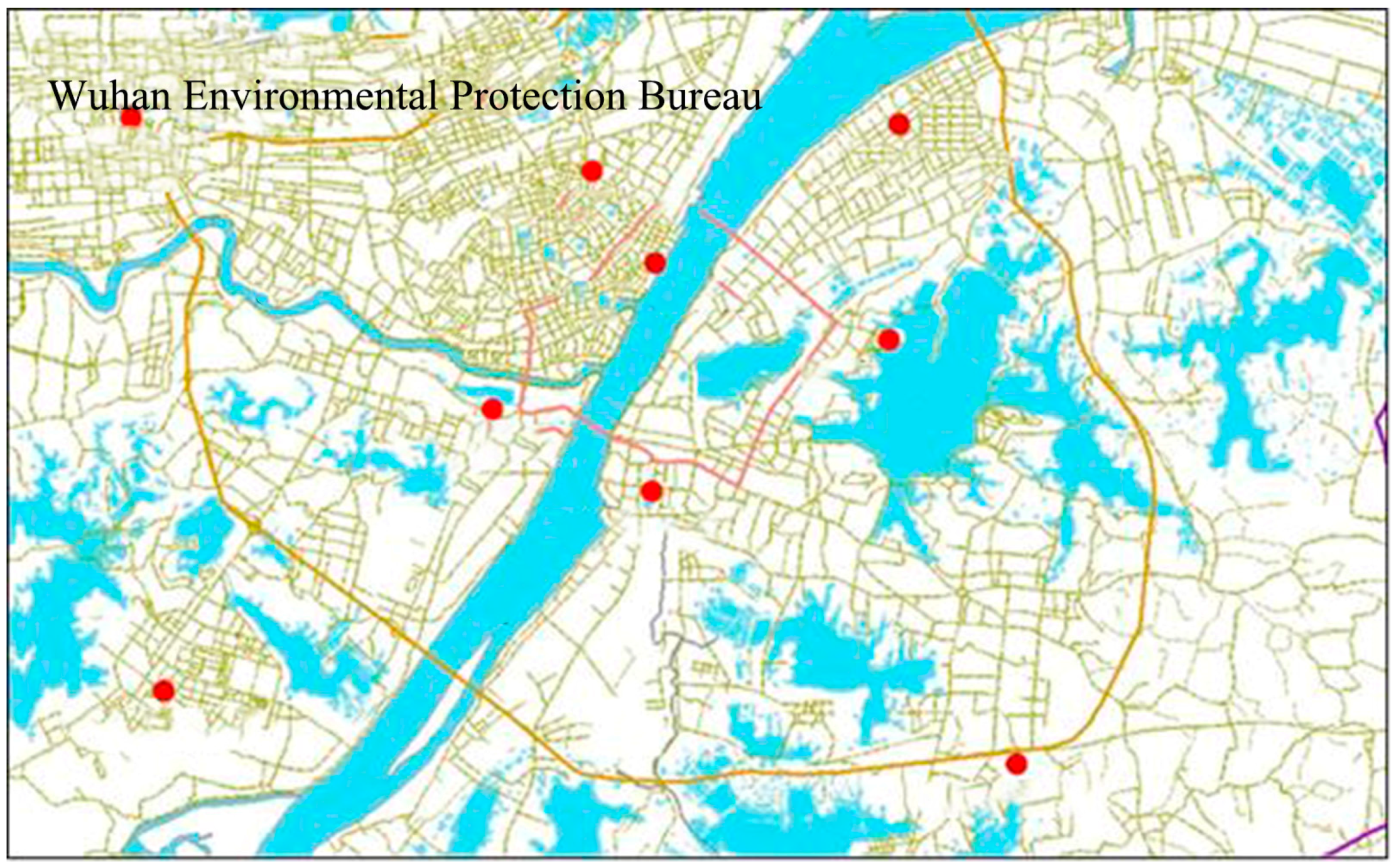
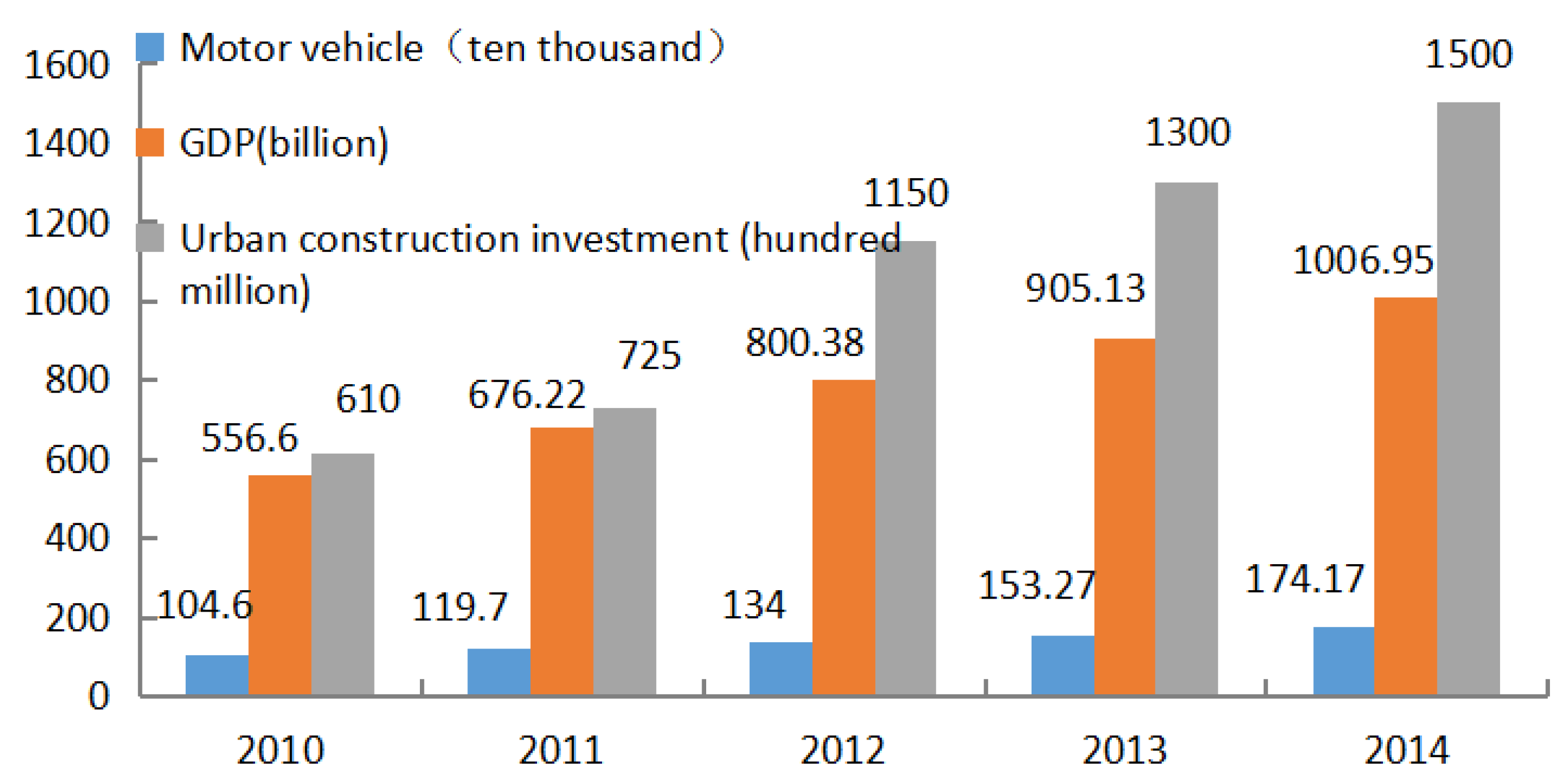
3.2. Analysis of Scientific Measurements of Air Quality in Wuhan
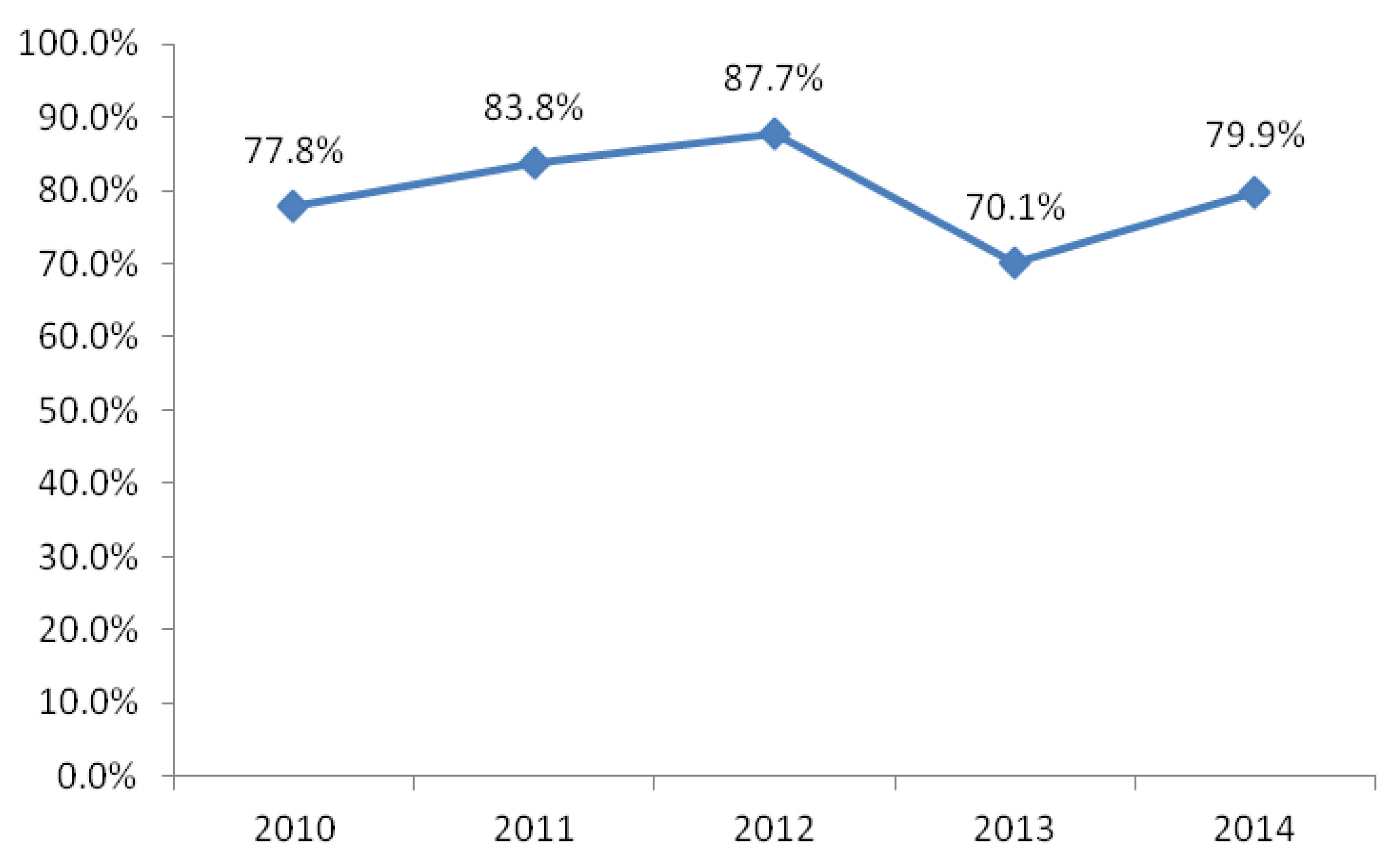
3.2.1. Annual Excellent Rate of Air Quality
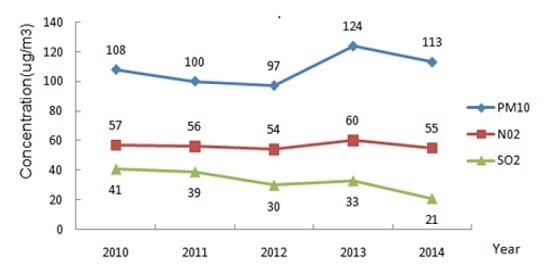
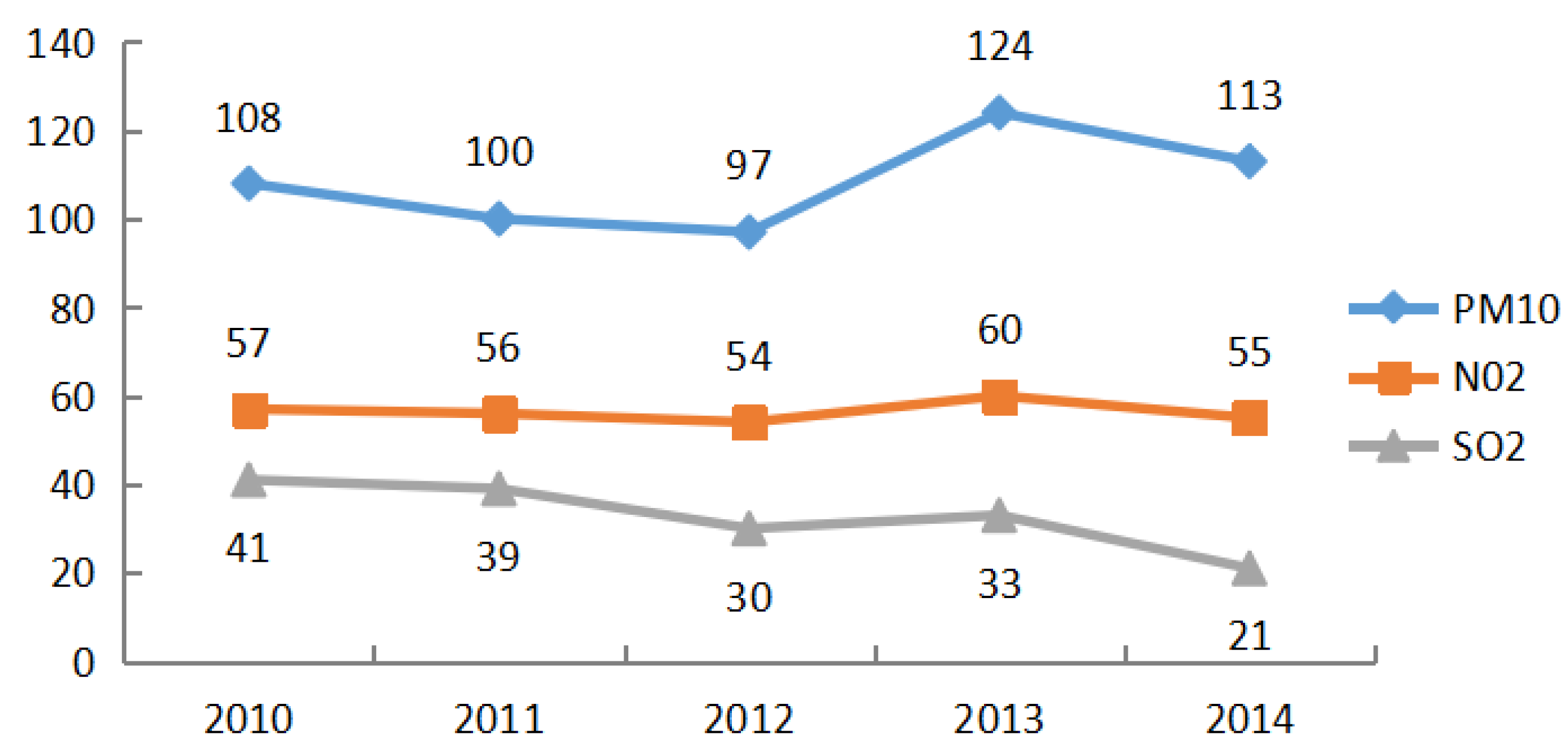
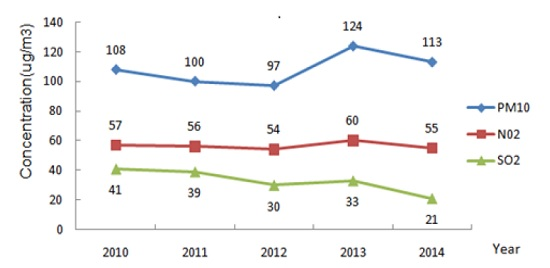
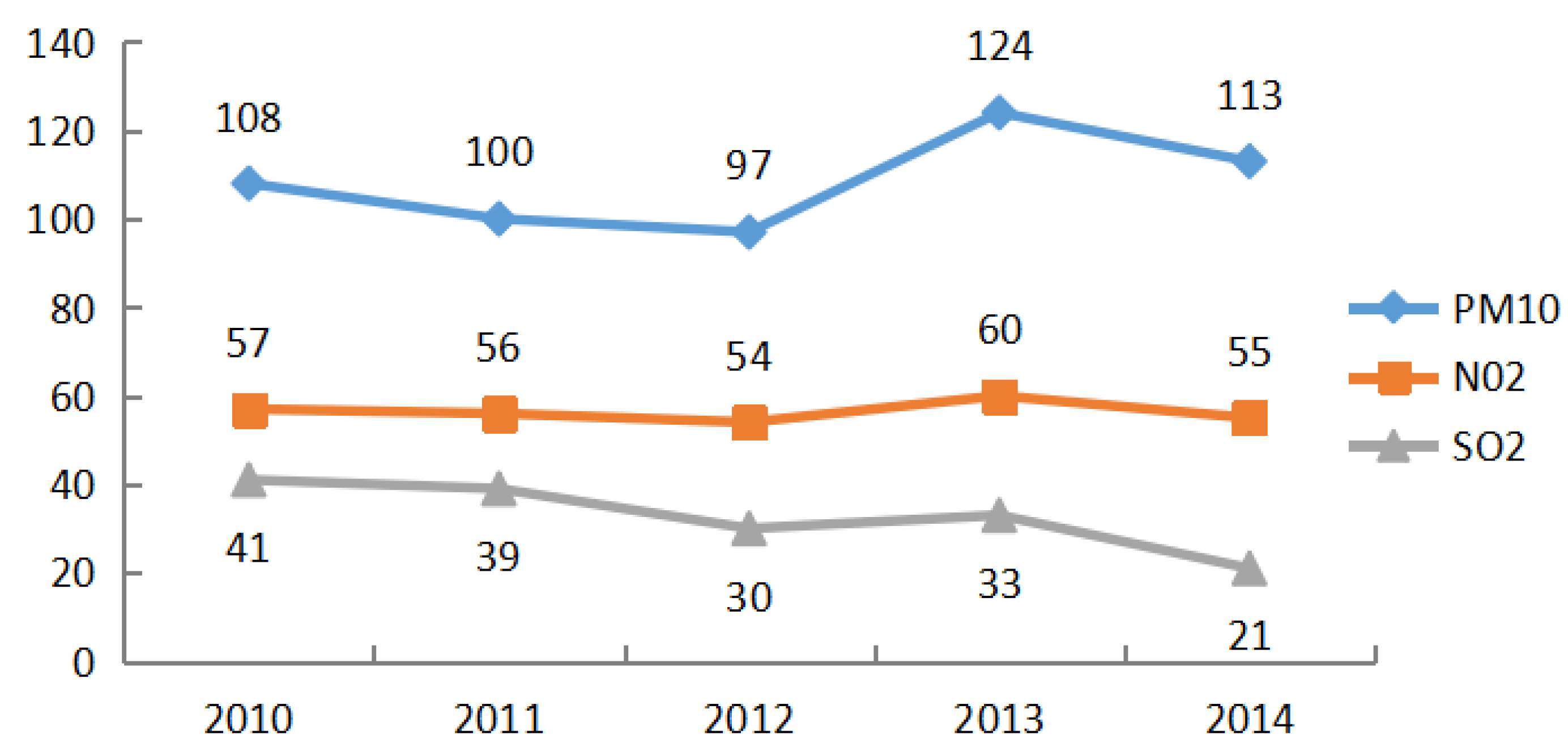
3.2.2. Variations of Average Air Pollutant Concentrations
3.2.3. Analysis of Parents’ Perception of Air Quality
3.3. The Effect of Community-Level Factors on Air Quality Perception
4. Discussion
5. Conclusions
Limitations of Our Research
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wang, G.C.; Wang, P.C. PM2.5 Pollution in China and its harmfulness to human health. Sci. Technol. Rev. 2014, 32, 72–78. [Google Scholar]
- Trasande, L.; Thurston, G.D. The role of air pollution in asthma and other pediatric morbidities. J. Allergy Clin. Immunol. 2005, 115, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Goldberg, M.S.; Villeneuve, P.J. A systematic review of the relation between long-term exposure to ambient air pollution and chronic diseases. Rev. Environ. Health 2008, 23, 243–297. [Google Scholar] [PubMed]
- Sigmund, E.; De Ste Croix, M.; Miklánková, L.; Frömel, K. Physical activity patterns of children in comparison to teenagers and young adults. Eur. J. Public Health 2007, 17, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Moya, J.; Bearer, C.F.; Etzel, R.A. Children’s behavior and physiology and how it affects exposure to environmental contaminants. Pediatrics 2004, 113, 996–1006. [Google Scholar] [PubMed]
- Esposito, S.; Tenconi, R.; Lelii, M.; Preti, V.; Nazzari, E.; Consolo, S.; Patria, M.F. Possible molecular mechanisms linking air pollution and asthma in children. BMC Pulm. Med. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Martinez, R.; Perez-Padilla, R.; Olaiz-Fernandez, G.; Mendoza-Alvarado, L.; Moreno-Macias, H.; Fortoul, T.; McDonnell, W.; Loomis, D.; Romieu, I. Lung function growth in children with long-term exposure to air pollutants in Mexico City. Am. J. Respir. Crit. Care Med. 2007, 176, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Schultz, E.S.; Gruzieva, O.; Bellander, T.; Bottai, M.; Hallberg, J.; Kull, I.; Svartengren, M.; Melén, E.; Pershagen, G. Traffic-related air pollution and lung function in children at 8 years of age: A birth cohort study. Am. J. Respir. Crit. Care Med. 2012, 186, 1286–1291. [Google Scholar] [CrossRef] [PubMed]
- Stenlund, T.; Garvill, J.; Nordin, S.; Andersson, K.; Liden, E. Annoyance and health symptoms and their influencing factors: A population-based air pollution intervention study. Public Health 2009, 123, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; He, G.; Liu, Y.; Yin, P.; Li, Y.; Kan, H.; Fan, M.; Xue, A.; Fan, M. The associations between ambient air pollution and adult respiratory mortality in 32 major Chinese cities, 2006–2010. Environ. Res. 2015, 137, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Piro, F.N.; Madsen, C.; Nafstad, P.; Naess, Q.; Claussen, B. A comparison of self- reported air pollution problems and GIS-modeled levels of air pollution in people with and without chronic diseases. Environ Health 2008, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yen, I.H.; Yelin, E.H.; Katz, P.; Eisner, M.D.; Blanc, P.D. Perceived neighborhood problems and quality of life, physical functioning, and depressive symptoms among adults with asthma. Am. J. Public Health 2006, 96, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Jacquemin, B.; Sunyer, J.; Forsberg, B.; Götschi, T.; Bayer-Oglesby, L.; Ackermann-Liebrich, U.; de Marco, R.; Heinrich, J.; Jarvis, D.; Torén, K.; et al. Annoyance due to air pollution in Europe. Int. J. Epidemiol. 2007, 36, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Atari, D.O.; Luqinaah, I.N.; Fung, K. The relationship between odour annoyance scores and modelled ambient air pollution in Sarnia, “Chemical Valley”, Ontario. Environ. Res. Public Health 2009, 6, 2655–2675. [Google Scholar] [CrossRef] [PubMed]
- Oglesby, L.; Künzli, N.; Monn, C.; Schindler, C.; Ackermann-Liebrich, U.; Leuenberger, P. Validity of annoyance scores for estimation of long term air pollution exposure in epidemiologic studies: The Swiss Study on Air Pollution and Lung Diseases in Adults (SAPALDIA). Am. J. Epidemiol. 2000, 152, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Howel, D.; Moffatt, S.; Bush, J.; Dunn, C.E.; Prince, H. Public views on the links between air pollution and health in Northeast England. Environ. Res. 2003, 91, 163–171. [Google Scholar] [CrossRef]
- Brody, S.D.; Peck, B.M.; Highfield, W.E. Examining localized patterns of air quality perception in Texas: A spatial and statistical analysis. Risk Anal. 2004, 6, 1561–1574. [Google Scholar] [CrossRef] [PubMed]
- Kohlhuber, M.; Mielck, A.; Weiland, S.K.; Bolte, G. Social inequality in perceived environmental exposures in relation to housing conditions in Germany. Environ. Res. 2006, 101, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.G. China’s Survey Report on Haze in 2013; New Media and Society; Shanghai Jiao Tong University: Shanghai, China, 2013; pp. 156–175. [Google Scholar]
- Omanga, E.; Ulmer, L.; Berhane, Z.; Gatari, M. Industrial air pollution in rural Kenya: Community awareness, risk perception and associations between risk variables. BMC Public Health 2014, 14, 377. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.G.; Ying, Q.; Hu, J.L.; Zhang, H.L. Spatial and temporal variations of six criteria air pollutants in 31 provincial capital cities in China during 2013–2014. Environ. Int. 2014, 73, 413–422. [Google Scholar] [CrossRef] [PubMed]
- He, Q.Q. Effects of ambient air pollution on lung function growth in Chinese schoolchildren. Respir. Med. 2010, 104, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z. Effects of air pollution on children’s respiratory health in three Chinese cities. Arch. Environ. Health Int. J. 2000, 55, 126–133. [Google Scholar] [CrossRef] [PubMed]
- The Official Website of Wuhan Environmental Protection Bureau. Available online: http://www.whepb.gov.cn (accessed on 9 May 2016).
- More Than Half All Day Last Year in Wuhan Polluted, Endogenous Contaminants in Air Is Main Cause. 2013. Available online: http://news.xinhuanet.com/overseas/2014–01/20/c_126033740.htm (accessed on 9 May 2016).
- Floating Population of Wuhan Is Nearly 3 Million. 2013. Available online: http://www.chinadaily.com.cn/hqgj/jryw/2013-09-26/content_10198536.html (accessed on 9 May 2016).
- Zhang, R.H.; Li, Q.; Zhang, R.N. Meteorological conditions for the persistent severe fog and haze event over eastern China in January 2013. Sci. China Earth Sci. 2014, 44, 26–35. [Google Scholar]
- Kim, M.; Yi, O.; Kim, H. The role of differences in individual and community attributes in perceived air quality. Sci. Total Environ. 2012, 425, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zou, H. Regional inequality in contemporary China. Ann. Econ. Financ. 2012, 13, 119–143. [Google Scholar]
- Yao, C.R.; Wu, F.; Li, J.M. Review of fertility desire investigation among rural and urban residents from 2000 to 2008. Popul. J. 2010, 35, 17–22. [Google Scholar]
- Egondi, T.; Kyobutungi, C.; Ng, N.; Muindi, K.; Oti, S.; van de Vijver, S.; Ettarh, R.; Rocklöv, J. Community perceptions of air pollution and related health risks in Nairobi Slums. Int. J. Environ. Res. Public Health 2013, 10, 4851–4868. [Google Scholar] [CrossRef] [PubMed]
- Badland, H.M.; Duncan, M.J. Perceptions of air pollution during the work-related commute by adults in Queensland, Australia. Atmos. Environ. 2009, 43, 5791–5795. [Google Scholar] [CrossRef]
- Esposito, S.; Galeone, C.; Lelii, M.; Longhi, B.; Ascolese, B.; Senatore, L.; Prada, E.; Montinaro, V.; Malerba, S.; Patria, M.F.; et al. Impact of air pollution on respiratory diseases in children with recurrent wheezing or asthma. BMC Pulm. Med. 2014, 130, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Pattenden, S.; Willers, S.; Antova, T.; Fabianova, E.; Braun-Fahrländer, C.; Forastiere, F.; Gehring, U.; Luttmann-Gibson, H.; Grize, L.; et al. PM10, and children’s respiratory symptoms and lung function in the PATY study. Eur. Respir. J. 2012, 40, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Yazdanparast, T.; Seyedmehdi, S.M.; Khalilzadeh, S.; Salehpour, S.; Boloursaz, M.R.; Baghaie, N.; Hassanzad, M.; Velayati, A.A. Knowledge and practice of asthmatic children’s parents about daily air quality. Tanaffos 2013, 12, 23–28. [Google Scholar] [PubMed]
- Zhu, Z.C.; Kong, L.L.; Xia, K. Analysis of PM10 source in Wuhan and its countermeasures. Environ. Sci. Technol. 2009, 2, 64–67. [Google Scholar]
- Wakefield, S.E.; Elliott, S.J.; Cole, D.C.; Eyles, J.D. Environmental risk and (re)action: Air quality, health, and civic involvement in an urban industrial neighbor-hood. Health Place 2001, 7, 163–177. [Google Scholar] [CrossRef]
- Ji, L.L.; Chen, C.K.; Wang, N.N. Comparison and analysis on characteristics and causes of PM2.5 pollution in six typical central cities of China. J. Catastrophol. 2014, 29, 230–234. [Google Scholar]
- Wu, D. Systematic review about haze weather in China nearly a decade. Acta Sci. Circumst. 2012, 32, 257–269. [Google Scholar]
- Leung, Y.K.; Wu, M.C.; Yeung, K.K. A study on the relationship among visibility, atmospheric suspended particulate concentration and meteorological conditions in Hong Kong. Acta Meteorol. Sin. 2008, 66, 461–469. [Google Scholar]
- Zhang, Q.; Quan, J.; Tie, X.; Li, X.; Liu, Q.; Gao, Y.; Zhao, D. Effects of meteorology and secondary particle formation on visibility during heavy haze events in Beijing, China. Sci. Total Environ. 2015, 502, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Song, G.J.; Guo, M.Y.; Yin, G.B. Urban air quality management satisfaction evaluation method and case study. Environ. Pollut. Control 2011, 33, 81–86. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Community (n = 453) | Hospital (n = 412) | p-Value | ||
|---|---|---|---|---|---|
| N | Percentage | N | Percentage | ||
| Gender | |||||
| Male | 181 | 40.0 | 187 | 45.4 | 0.11 |
| Female | 272 | 60.0 | 225 | 54.6 | |
| Age Group (years) | |||||
| 18–29 | 20 | 4.4 | 160 | 38.8 | <0.01 |
| 30–39 | 263 | 58.1 | 188 | 45.6 | |
| 40 and above | 170 | 37.5 | 64 | 15.5 | |
| Residency Status | |||||
| Rural | 52 | 11.5 | 229 | 55.6 | <0.01 |
| Urban | 401 | 88.5 | 183 | 44.4 | |
| Education Level | |||||
| Elementary school | 28 | 6.2 | 35 | 8.5 | <0.01 |
| Secondary school | 85 | 18.8 | 263 | 63.8 | |
| College and above | 340 | 75.1 | 114 | 27.7 | |
| Annual Family Income (Yuan) | |||||
| <50,000 | 80 | 20.4 | 206 | 50.0 | <0.01 |
| 50,000–15,000 | 251 | 64.0 | 189 | 45.9 | |
| >15,000 | 61 | 15.6 | 17 | 4.1 | |
| Health Condition of Child | |||||
| Good | 348 | 76.8 | 166 | 40.3 | <0.01 |
| Moderate | 97 | 21.4 | 174 | 42.2 | |
| Poor | 8 | 1.8 | 72 | 17.5 | |
| Degree of Concern of Air Quality | |||||
| Rather concerned | 17 | 3.7 | 16 | 3.9 | <0.05 |
| Concerned | 153 | 33.8 | 174 | 42.2 | |
| Highly concerned | 283 | 62.5 | 222 | 53.9 | |
| Item | Total N (%) | Air Quality Perception | Crude OR (95% CI) | Adjusted OR (95% CI) | |
|---|---|---|---|---|---|
| Better (N/%) | Worse (N/%) | ||||
| 69 (15.7) | 371 (84.3) | ||||
| Gender | |||||
| Male | 178 (40.4) | 31 (44.9) | 147 (39.6) | Ref. | Ref. |
| Female | 262 (59.6) | 38 (55.1) | 224 (60.4) | 1.243 (0.741, 2.087) | 0.947 (0.539, 1.666) |
| Age Group (years) | |||||
| 18–29 | 16 (3.6) | 2 (2.9) | 14 (3.8) | Ref. | Ref. |
| 30–39 | 256 (58.2) | 32 (46.4) | 224 (60.4) | 1.000 (0.217, 4.605) | 1.384 (0.280, 6.834) |
| 40 and above | 168 (38.2) | 35 (50.7) | 133 (35.8) | 0.543 (0.118, 2.501) | 0.785 (0.158, 3.889) |
| Residential Status | |||||
| Rural | 52 (11.8) | 9 (13.0) | 43 (11.6) | Ref. | Ref. |
| Urban | 388 (88.2) | 60 (87.0) | 328 (88.4) | 1.144 (0.530, 2.470) | 1.007 (0.529, 1.918) |
| Education Level | |||||
| Elementary school | 28 (6.4) | 11 (15.9) | 17 (4.6) | Ref. | Ref. |
| Secondary school | 83 (18.9) | 12 (17.4) | 71 (19.1) | 3.828 (1.445, 10.144) | 4.164 (1.491, 11.628) ** |
| College and above | 329 (74.8) | 46 (66.7) | 283 (76.3) | 3.981 (1.753, 9.038) ** | 4.034 (1.610, 10.110) ** |
| Child Health Condition | |||||
| Good | 336 (76.4) | 51 (73.9) | 285 (76.8) | Ref. | Ref. |
| Moderate | 96 (21.8) | 16 (23.2) | 80 (21.6) | 0.895 (0.484, 1.653) | 0.956 (0.503, 1.814) |
| Poor | 8 (1.8) | 2 (2.9) | 6 (1.6) | 0.537 (0.105, 2.734) | 0.570 (0.106, 3.053) |
| Annual Family Income (Yuan) | |||||
| <50,000 | 79 (18.0) | 15 (21.7) | 64 (17.3) | Ref. | Ref. |
| 50,000–150,000 | 242 (55.0) | 39 (56.5) | 203 (54.7) | 1.220 (0.632, 2.357) | 1.207 (0.609, 2.393) |
| >150,000 | 61 (13.9) | 7 (10.1) | 54 (14.5) | 1.808 (0.687, 4.758 ) | 1.523 (0.557, 4.162) |
| Unknown | 58 (13.1) | 8 (11.6) | 50 (13.5) | 1.465 (0.575, 3.729 ) | 1.759 (0.642, 4.817) |
| Degree of Concern of Air Quality | |||||
| Rather concerned | 16 (3.6) | 2 (2.9) | 14 (3.8) | Ref. | Ref. |
| Concerned | 146 (33.2) | 31 (44.9) | 115 (31.0) | 0.530 (0.114, 2.457) | 0.481 (0.098, 2.352) |
| Highly concerned | 278 (63.2) | 36 (52.2) | 242 (65.2) | 0.960 (0.210, 4.401) | 0.838 (0.172, 4.076) |
| Item | Total N (%) | Air Quality Perception | Crude OR (95% CI) | Adjusted OR (95% CI) | |
|---|---|---|---|---|---|
| Better (N/%) | Worse (N/%) | ||||
| 77 (25.8) | 222 (74.2) | ||||
| Gender | |||||
| Male | 133 (44.5) | 36 (46.8) | 97 (43.7) | Ref. | Ref. |
| Female | 166 (55.5) | 41 (53.2) | 125 (56.3) | 1.132 (0.672, 1.904) | 1.230 (0.685, 2.208) |
| Age Group (years) | |||||
| 18–29 | 109 (36.5) | 39 (50.6) | 70 (31.5) | Ref. | Ref. |
| 30–39 | 142 (47.5) | 31 (40.3) | 111 (50.0) | 1.995 (1.141, 3.487) * | 1.922 (1.024, 3.605) * |
| 40 and above | 48 (16.0) | 7 (9.1) | 41 (18.5) | 3.263 (1.337, 7.963) ** | 3.252 (1.170, 9.040) * |
| Residency Status | |||||
| Rural | 144 (48.2) | 47 (61.0) | 97 (43.7) | Ref. | Ref. |
| Urban | 155 (51.8) | 30 (39.0) | 125 (56.3) | 2.019 (1.189, 3.427) ** | 1.007 (0.529, 1.918) |
| Education Level | |||||
| Elementary school | 21 (7.0) | 10 (13.0) | 11 (5.0) | Ref. | Ref. |
| Secondary school | 180 (60.2) | 57 (74.0) | 123 (55.4) | 1.962 (0.788, 4.884) | 1.879 (0.678, 5.210) |
| College and above | 98 (32.8) | 10 (13.0) | 88 (39.6) | 7.997 (2.722, 23.489) ** | 7.598 (2.244, 25.732) ** |
| Child Health Condition | |||||
| Good | 117 (39.1) | 42 (54.5) | 75 (33.8) | Ref. | Ref. |
| Moderate | 130 (43.5) | 31 (40.3) | 99 (44.6) | 1.788 (1.029, 3.108) * | 1.779 (0.978, 3.237) |
| Poor | 52 (17.4) | 4 (5.2) | 48 (21.6) | 6.720 (2.265, 19.941) ** | 6.864 (2.212, 21.302) ** |
| Annual Family Income (Yuan) | |||||
| <50,000 | 134 (44.8) | 42 (54.5) | 92 (41.4) | Ref. | Ref. |
| 50,000–150,000 | 150 (50.2) | 33 (42.9) | 117 (52.7) | 1.619 (0.951, 2.754) | 1.180 (0.655, 2.127) |
| >150,000 | 15 (5.0) | 2 (2.6) | 13 (5.9) | 2.967 (0.641, 13.742) | 1.699 (0.334, 8.645) |
| Degree of Concern of Air Quality | |||||
| Rather concerned | 10 (3.3) | 4 (5.2) | 6 (2.7) | Ref. | Ref. |
| Concerned | 113 (37.8) | 29 (37.7) | 84 (37.8) | 1.932 (0.509, 7.333) | 1.071 (0.254, 4.517) |
| Highly concerned | 176 (58.9) | 44 (57.1) | 132 (59.5) | 2.001 (0.540, 7.420) | 0.956 (0.233, 3.921) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Liu, F.; Lu, Y.; Mao, Z.; Lu, H.; Wu, Y.; Chu, Y.; Yu, L.; Liu, Y.; Ren, M.; et al. Factors Affecting Parent’s Perception on Air Quality—From the Individual to the Community Level. Int. J. Environ. Res. Public Health 2016, 13, 493. https://doi.org/10.3390/ijerph13050493
Guo Y, Liu F, Lu Y, Mao Z, Lu H, Wu Y, Chu Y, Yu L, Liu Y, Ren M, et al. Factors Affecting Parent’s Perception on Air Quality—From the Individual to the Community Level. International Journal of Environmental Research and Public Health. 2016; 13(5):493. https://doi.org/10.3390/ijerph13050493
Chicago/Turabian StyleGuo, Yulin, Fengfeng Liu, Yuanan Lu, Zongfu Mao, Hanson Lu, Yanyan Wu, Yuanyuan Chu, Lichen Yu, Yisi Liu, Meng Ren, and et al. 2016. "Factors Affecting Parent’s Perception on Air Quality—From the Individual to the Community Level" International Journal of Environmental Research and Public Health 13, no. 5: 493. https://doi.org/10.3390/ijerph13050493