
A Primrose Path? Moderating Effects of Age and Gender in the Association between Green Space and Mental Health


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
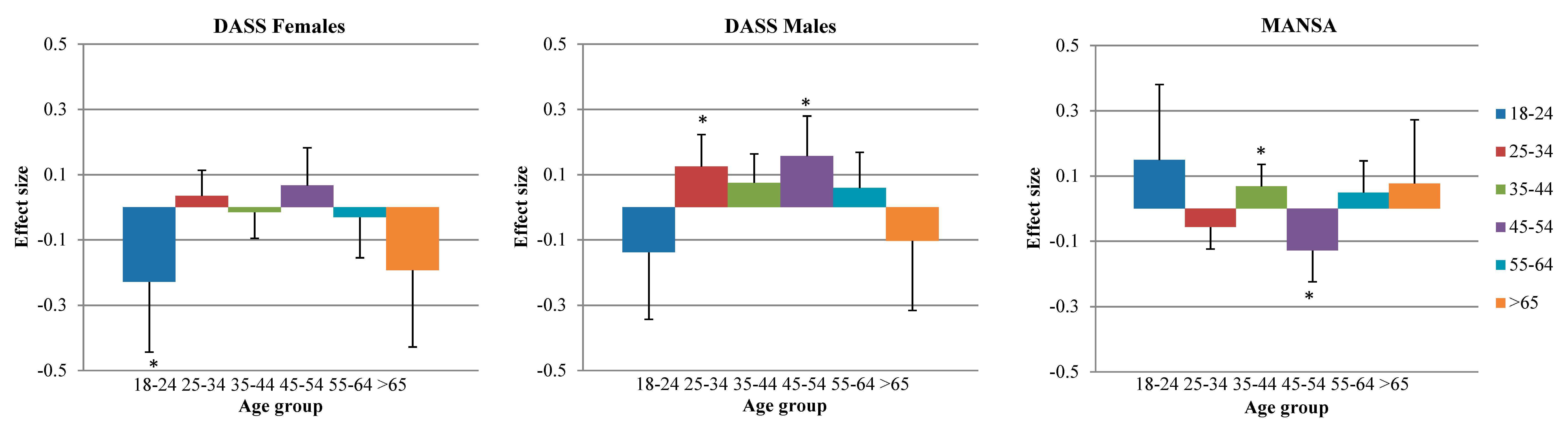
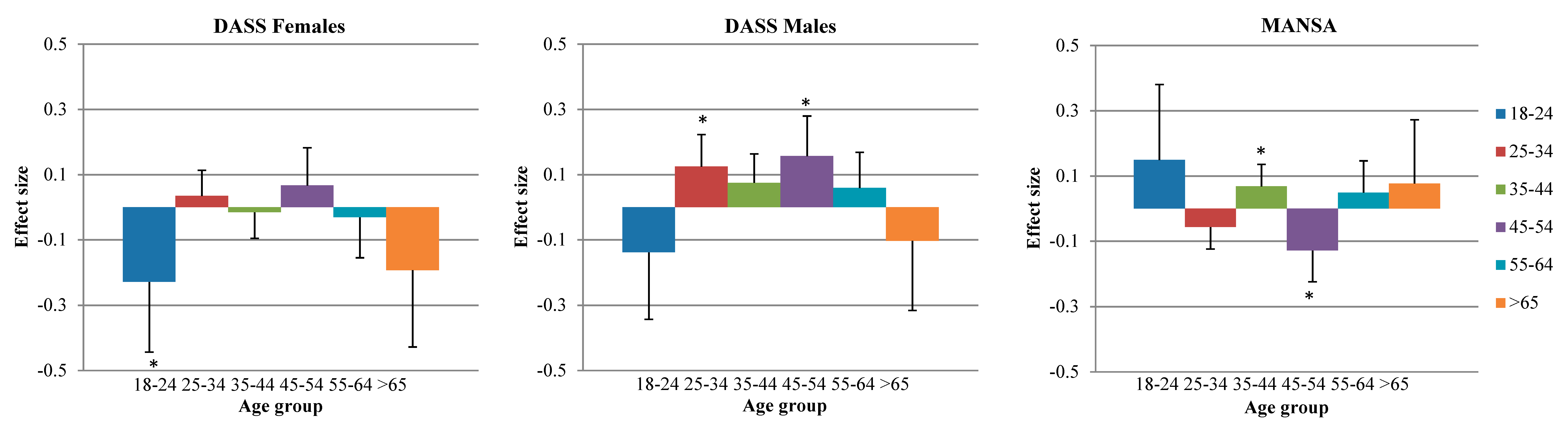
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bowler, D.E.; Buyung-Ali, L.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Triguero-Mas, M.; Dadvand, P.; Cirach, M.; Martínez, D.; Medina, A.; Mompart, A.; Basagaña, X.; Gražulevičienė, R.; Nieuwenhuijsen, M.J. Natural outdoor environments and mental and physical health: Relationships and mechanisms. Environ. Int. 2015, 77, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Triguero-Mas, M.; Martí-nez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, J.M. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, A.E.; Van den Berg, M.M.H.E. Health benefits of plants and green space: Establishing the evidence base. Acta Hort. 2015, 1093, 19–30. [Google Scholar] [CrossRef]
- Groenewegen, P.P.; van den Berg, A.E.; Maas, J.; Verheij, R.A.; de Vries, S. Is a green residential environment better for health? If so, why? Ann. Assoc. Am. Geogr. 2012, 102, 996–1003. [Google Scholar] [CrossRef]
- Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207. [Google Scholar]
- Lee, A.C.K.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; Verheij, R.; Groenewegen, P.; Spreeuwenberg, P. Natural environments—Healthy environments? An exploratory analysis of the relationship between greenspace and health. Environ. Plann. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.; Groenewegen, P.; de Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Mitchell, R.; Hartig, T. The association between green space and mental health varies across the lifecourse. A longitudinal study. J. Epidemiol. Community Health 2014, 68, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Reklaitiene, R.; Grazuleviciene, R.; Dedele, A.; Virviciute, D.; Vensloviene, J.; Tamosiunas, A.; Baceviciene, M.; Luksiene, D.; Sapranaviciute-Zabazlajeva, L.; Radisauskas, R.; et al. The relationship of green space, depressive symptoms and perceived general health in urban population. Scand. J. Public Health 2014, 42, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; Verheij, R.A.; de Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Community Health 2009, 63, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; van Dillen, S.M.E.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and Health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Mezzich, J.E. Positive health: Conceptual place, dimensions and implications. Psychopathology 2005, 38, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Van der Krieke, L.; Jeronimus, B.F.; Blaauw, F.J.; Wanders, R.B.K.; Emerencia, A.C.; Schenk, H.M.; Vos, S.D.; Snippe, E.; Wichers, M.; Wigman, J.T.W.; et al. HowNutsAreTheDutch (HoeGekIsNL): A crowdsourcing study of mental symptoms and strengths. Int. J. Meth. Psychiatr. Res. 2015. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Priebe, S.; Huxley, P.; Knight, S.; Evans, S. Application and results of the manchester short assessment of quality of life (MANSA). Int. J. Soc. Psychiatry 1999, 45, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Statistics Netherlands (CBS). Dutch Land Use Database (Bestand Bodemgebruik). 2010. Available online: https://data.overheid.nl/data/dataset/bestand-bodemgebruik-2010 (accessed on 8 September 2015).
- Twisk, J.; Rijmen, F. Longitudinal tobit regression: A new approach to analyze outcome variables with floor or ceiling effects. J. Clin. Epidemiol. 2009, 62, 953–958. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata: Release 13: Statistical Software; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Mental health benefits of neighbourhood green space are stronger among physically active adults in middle-to-older age: Evidence from 260,061 Australians. Prev. Med. 2013, 57, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Mitchell, R. Gender differences in relationships between urban green space and health in the United Kingdom. Soc. Sci. Med. 2010, 71, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Lottrup, L.; Grahn, P.; Stigsdotter, U.K. Workplace greenery and perceived level of stress: Benefits of access to a green outdoor environment at the workplace. Landscape Urban Plann. 2013, 110, 5–11. [Google Scholar] [CrossRef]
- Beil, K.; Hanes, D. The influence of urban natural and built environments on physiological and psychological measures of stress—A pilot study. Int. J. Environ. Res. Public Health 2013, 10, 1250–1267. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Chang, C.; Sullivan, W.C. A dose of nature: Tree cover, stress reduction, and gender differences. Landscape Urban Plann. 2014, 132, 26–36. [Google Scholar] [CrossRef]
- Jiang, B.; Larsen, L.; Deal, B.; Sullivan, W.C. A dose-response curve describing the relationship between tree cover density and landscape preference. Landscape Urban Plann. 2015, 139, 16–25. [Google Scholar] [CrossRef]
- Jiang, B.; Li, D.; Larsen, L.; Sullivan, W.C. A dose-response curve describing the relationship between urban tree cover density and self-reported stress recovery. Environ. Behav. 2014, 48, 607–629. [Google Scholar] [CrossRef]
- Cohen, D.A.; McKenzie, T.L.; Sehgal, A.; Williamson, S.; Golinelli, D.; Lurie, N. Contribution of public parks to physical activity. Am. J. Public Health 2005, 97, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.; Sasidharan, V.; Elmendorf, W.; Willits, F.; Graefe, A.; Godbey, G. Gender and ethnic variations in urban park preferences, visitation, and perceived benefits. J. Leisure Res. 2005, 37, 281–306. [Google Scholar]
- Virden, R.J. Ethnic/racial and gender variations among meanings given to, and preferences for, the natural environment. Leisure Sci. 1999, 21, 219–239. [Google Scholar]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Van Dillen, S.M.E.; de Vries, S.; Groenewegen, P.P.; Spreeuwenberg, P. Greenspace in urban neighbourhoods and residents’ health: Adding quality to quantity. J. Epidemiol. Community Health 2012, 66, e8. [Google Scholar] [CrossRef] [PubMed]
- Verheij, R.A.; van de Mheen, H.D.; de Bakker, D.H.; Groenewegen, P.P.; Mackenbach, J.P. Urban-rural variations in health in the Netherlands: Does selective migration play a part? J. Epidemiol. Community Health 1998, 52, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Bishop, B. The Big Sort; Mariner Books: New York, NY, USA, 2009. [Google Scholar]
- Basisregistratie Grootschalige Topografie (BGT). Available online: https://www.Kadaster.nl/web/Themas/Registraties/BGT.htm (accessed on 18 April 2016).

{kind=link}
| Characteristic | n (%) or Mean (s.d.) |
|---|---|
| Female, n (%) | 3219 (65%) |
| Age group 18–24 years, n (%) | 358 (7.3%) |
| Age group 25–34 years, n (%) | 779 (15.8%) |
| Age group 35–44 years, n (%) | 739 (15.0%) |
| Age group 45–54 years, n (%) | 1244 (25.3%) |
| Age group 55–64 years, n (%) | 1307 (26.5%) |
| Age group 65 or older, n (%) | 497 (10.1%) |
| Level of education, mean (s.d.) | 7.0 (1.1) |
| Having a partner, n (%) | 3594 (73%) |
| Having paid work, n (%) | 3616 (73%) |
| Dutch native, n (%) | 4780 (97%) |
| Household income (euros/month), mean (s.d.) | 2746 (1038) |
| DASS Total, median (IQR) | 13 (19); range 0–126 |
| MANSA, mean (s.d.) | 62.4 (8.7); range 12–84 |
| Green space in 1 km buffer, mean (s.d.) | 29% (22%); range 0%–98% |
| Green space in 3 km buffer, mean (s.d.) | 47% (23%); range 0%–97% |
| Independent Variables | 1 km Buffer | 3 km Buffer | ||
|---|---|---|---|---|
| DASS n = 4765 | MANSA n = 4924 | DASS n = 4765 | MANSA n = 4924 | |
| Percentage of green space | −17.7 (11.3) | 5.2 (5.5) | −16.9 (8.1) * | 6.3 (4.5) |
| Age group | ||||
| 18–24 years | ref. | ref. | ref. | ref. |
| 25–34 years | −2.7 (3.9) | −1.2 (2.3) | −5.7 (4.5) | −0.0 (2.7) |
| 35–44 years | −0.6 (4.0) | −4.4 (2.3) ~ | −4.2 (4.5) | −3.0 (2.7) |
| 45–54 years | −2.2 (4.1) | −1.9 (2.3) | −8.0 (4.8) ~ | 1.2 (2.8) |
| 55–64 years | −6.5 (4.1) | −1.2 (2.3) | −8.8 (4.9) ~ | −0.7 (2.8) |
| 65 or older | −9.2 (5.1) | 3.5 (2.7) | −7.3 (6.8) | 3.1 (3.6) |
| Gender | ||||
| Female | ref. | ref. | ref. | ref. |
| Male | −2.5 (1.4) | −0.6 (2.7) | −4.7 (1.8) ** | −0.4 (0.9) |
| Green space*Age group | ||||
| Green space*18–24 years | ref. | ref. | ref. | ref. |
| Green space*25–34 years | 22.0 (11.7) ~ | −9.8 (5.6) ~ | 19.5 (8.4) * | −8.2 (4.6)~ |
| Green space*35–44 years | 13.9 (11.6) | −0.8 (5.6) | 15.8 (8.3) ~ | −3.3 (4.6) |
| Green space*45–54 years | 16.9 (11.9) | −7.1 (5.7) | 21.8 (8.9) * | −10.6 (4.8) * |
| Green space*55–64 years | 16.9 (11.9) | −4.5 (5.7) | 14.6 (8.7) ~ | −3.8 (4.8) |
| Green space*65 or older | 10.4 (13.1) | −5.5 (6.5) | 2.6 (11.3) | −2.7 (5.9) |
| Green space*Gender | ||||
| Green space*Female | ref. | ref. | ref. | ref. |
| Green space*Male | 3.3 (3.6) | −1.1 (1.8) | 6.7 (3.3) * | −1.2 (1.7) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bos, E.H.; Van der Meulen, L.; Wichers, M.; Jeronimus, B.F. A Primrose Path? Moderating Effects of Age and Gender in the Association between Green Space and Mental Health. Int. J. Environ. Res. Public Health 2016, 13, 492. https://doi.org/10.3390/ijerph13050492
Bos EH, Van der Meulen L, Wichers M, Jeronimus BF. A Primrose Path? Moderating Effects of Age and Gender in the Association between Green Space and Mental Health. International Journal of Environmental Research and Public Health. 2016; 13(5):492. https://doi.org/10.3390/ijerph13050492
Chicago/Turabian StyleBos, Elisabeth H., Leon Van der Meulen, Marieke Wichers, and Bertus F. Jeronimus. 2016. "A Primrose Path? Moderating Effects of Age and Gender in the Association between Green Space and Mental Health" International Journal of Environmental Research and Public Health 13, no. 5: 492. https://doi.org/10.3390/ijerph13050492
APA StyleBos, E. H., Van der Meulen, L., Wichers, M., & Jeronimus, B. F. (2016). A Primrose Path? Moderating Effects of Age and Gender in the Association between Green Space and Mental Health. International Journal of Environmental Research and Public Health, 13(5), 492. https://doi.org/10.3390/ijerph13050492