
Mercury Exposure Assessment and Spatial Distribution in A Ghanaian Small-Scale Gold Mining Community


Abstract
:1. Introduction
2. Materials and Methods
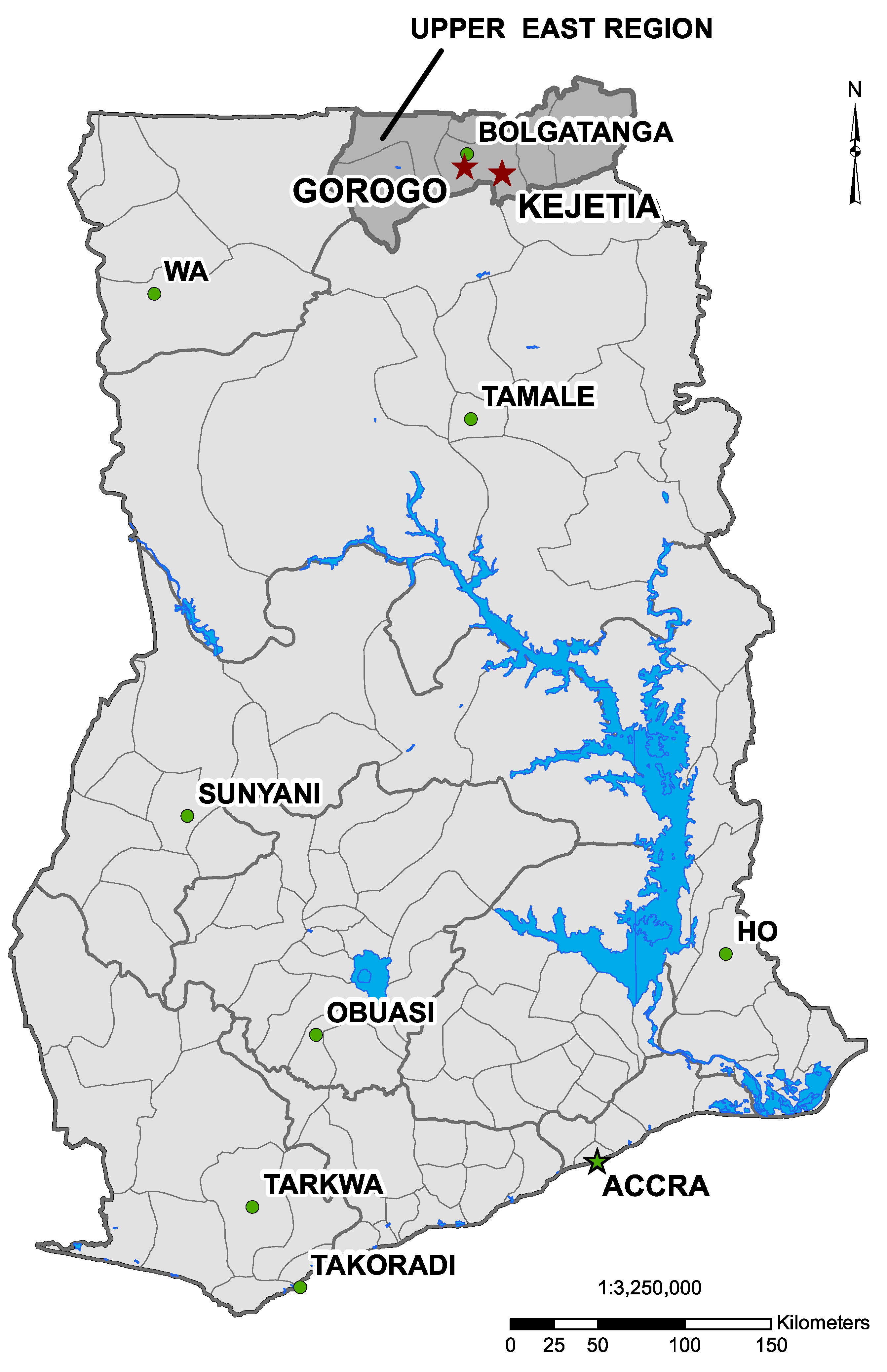
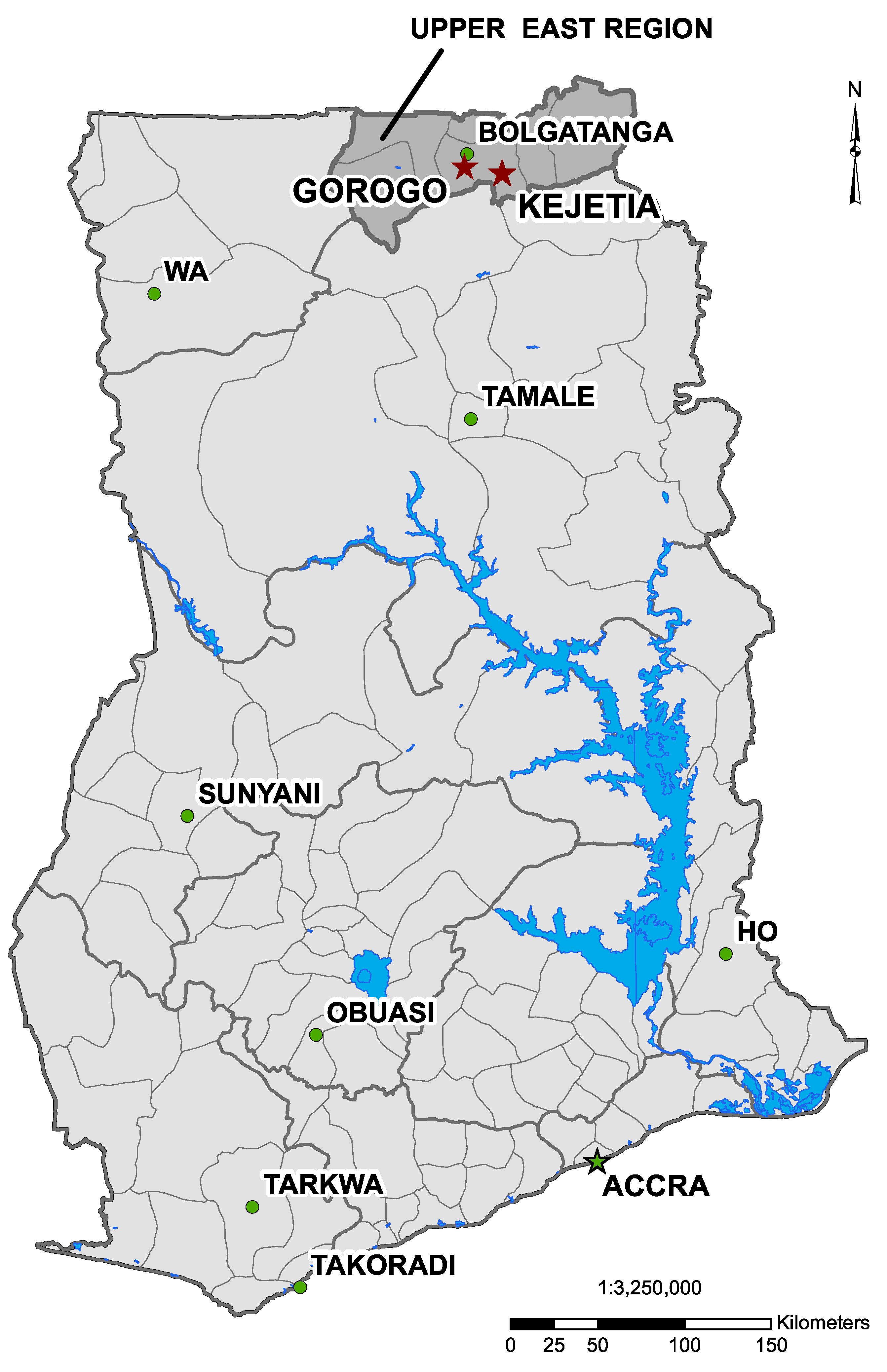
2.1. Sampling Strategy and Study Populations

2.2. Surveys
2.3. Sample Collection
2.4. Sample Mercury Analysis
2.5. Soil and Hg Ingestion
2.6. Statistical and Spatial Analyses
3. Results
3.1. Demographics and Mining

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kejetia | Gorogo | |||
|---|---|---|---|---|
| All | Miners a | Non-miners a | All | |
| n participants | 97 | 71 | 26 | 75 |
| n households | 54 | 41 | 18 | 26 |
| Sex (% Male) | 50 (51.5%) | 43 (60.6%) | 7 (26.9%) | 34 (45.3%) |
| Age (Mean [SD]) | 31.4 (10.8) | 30.6 (9.6) | 33.8 (13.6) | 51.5 (18.8) |
| BMI (Mean [SD]) | 22.7 (3.2) | 22.1 (2.7) | 24.5 (3.7) | 21.8 (3.1) b |
| Occupation | ||||
| Current Miner | 71 (73.2%) | - | - | 0 (0%) |
| Ex-Miner | 4 (4.2%) | 0 (0%) | 4 (15.4%) | 10 (13.3%) |
| Farmer | 7 (7.3%) | 5 (7.0%) | 2 (7.7%) | 71 (94.7%) |
| Cook (food, pito) c | 15 (15.6%) | 5 (7.0%) | 10 (38.5%) | 3 (4.0%) |
| Vendor | 18 (18.8%) | 7 (9.9%) | 11 (42.3%) | 7 (9.3%) |
| Other | 12 (12.5%) | 6 (8.5%) | 6 (23.1%) | 7 (9.3%) |
| Smoking | ||||
| Smoking in home | 45 (46.9%) | 39 (54.9%) | 6 (23.1%) | 39 (52.0%) |
| Current smoker | 15 (15.6%) | 14 (19.7%) | 1 (3.8%) | 14 (18.7%) |
| Ex-smoker | 7 (7.3%) | 6 (8.5%) | 1 (3.8%) | 9 (12.0%) |
| n ever-smokers with pack-years d | 16 | 15 | 1 | 14 |
| Cigarette pack-years d | 15.8 (26.6) | 15.1 (27.4) | 25.5 | 3.9 (2.1) |
| Education | ||||
| No school | 28 (29.2%) | 16 (22.9%) | 12 (46.2%) | 52 (69.3%) |
| Nursery/preschool | 9 (9.4%) | 6 (8.6%) | 3 (11.5%) | 9 (12.0%) |
| Primary | 27(28.1%) | 24 (34.3%) | 3 (11.5%) | 6 (8.0%) |
| Middle/JSS | 20 (20.8%) | 18 (25.7%) | 2 (7.7%) | 1 (1.3%) |
| Secondary/SSS, tech. | 11 (11.5%) | 5 (7.1%) | 6 (23.1%) | 5 (6.7%) |
| Higher than secondary | 1 (1.0%) | 1 (1.4%) | 0 (0%) | 2 (2.7%) |
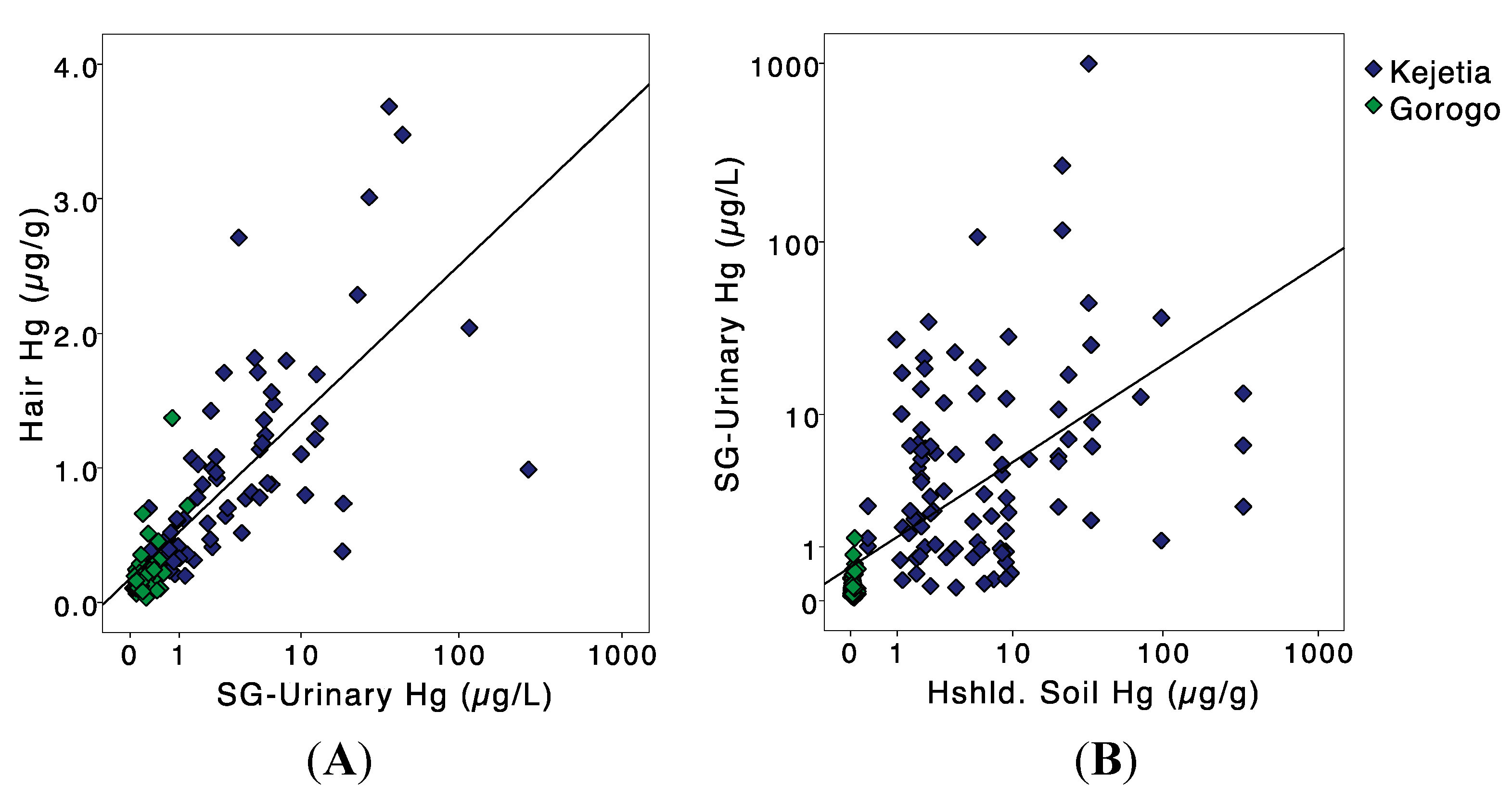
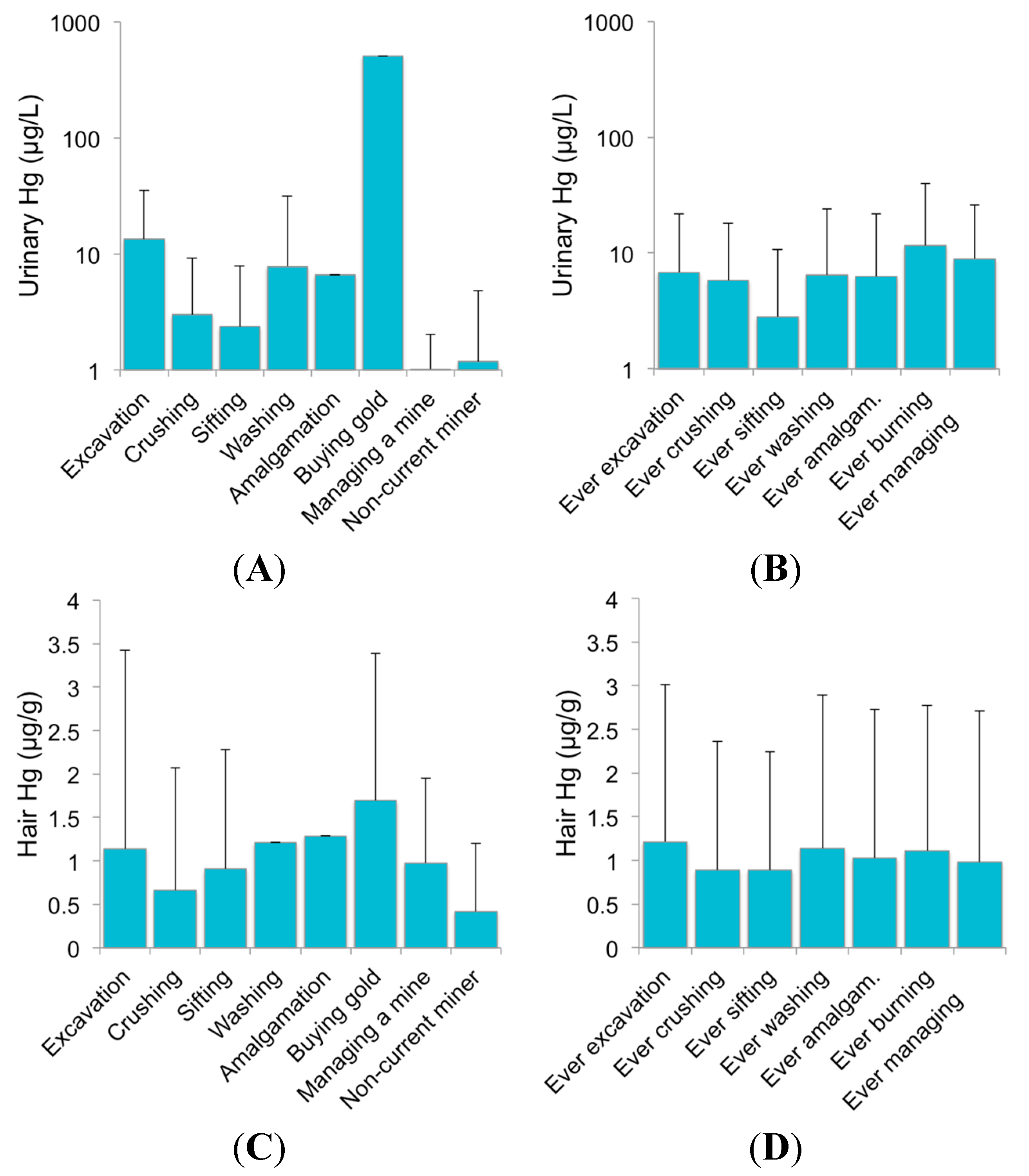
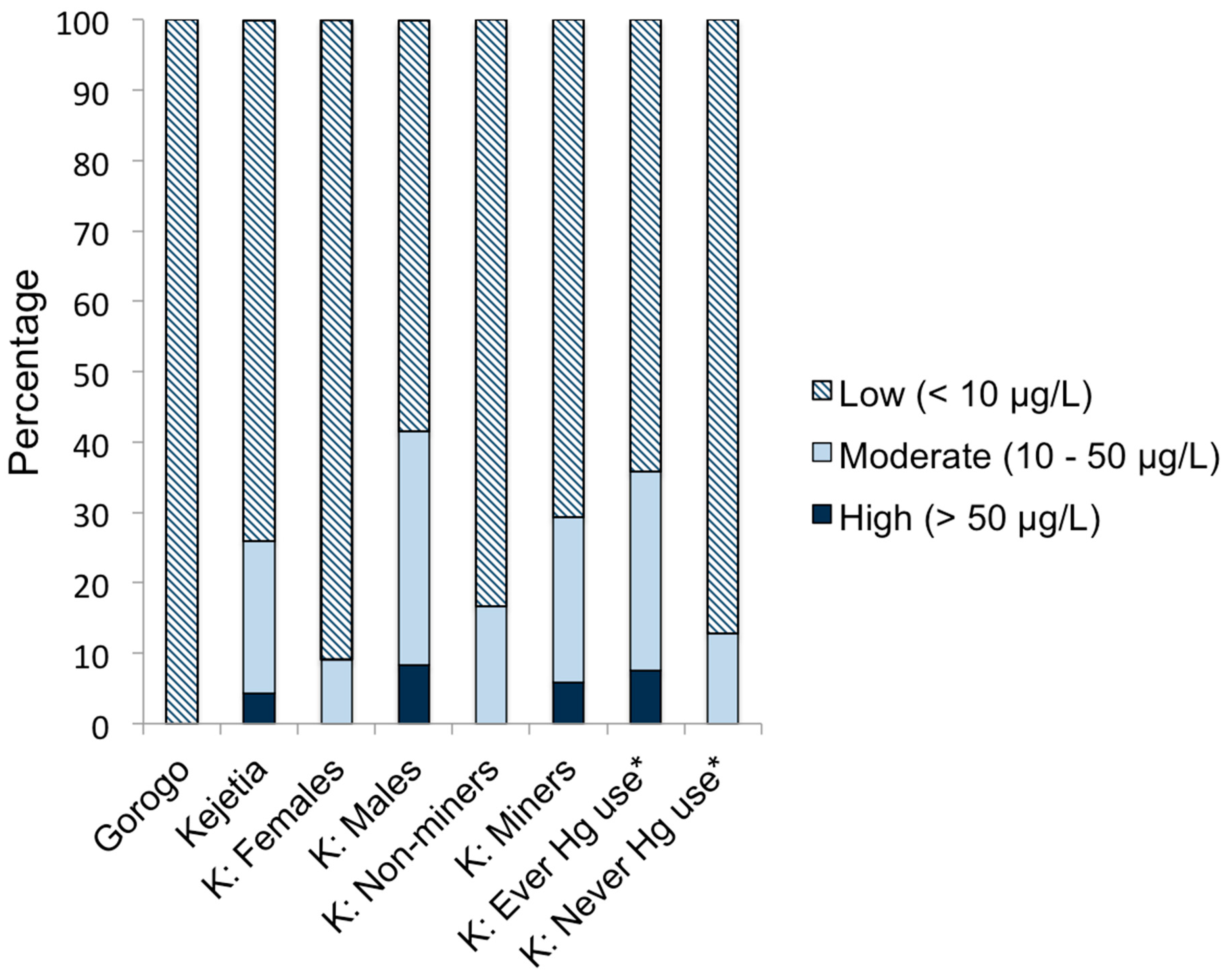
3.2. Mercury in Biological Samples
| Biomarker | Kejetia | Gorogo | |||
|---|---|---|---|---|---|
| All | Miners a | Non-miners a | All | ||
| Urine | n | 92 | 68 | 24 | 70 |
| Urinary Specific Gravity (SG) | |||||
| Mean (SD) | 1.018 (0.007) d | 1.017 (0.007) | 1.020 (0.006) | 1.014 (0.006) | |
| Urinary Hg (µg/L) | |||||
| Mean (SD) | 30.9 (148.5) d | 39.5 (172.1) e | 6.61 (13.2) | 0.161 (0.131) | |
| Median | 2.94 | 4.83 | 1.41 | 0.114 | |
| IQR b | 1.04, 11.0 | 1.26, 12.9 | 0.742, 5.23 | 0.079, 0.217 | |
| Min-Max | 0.160–1372 | 0.160–1372 | 0.199–58.1 | 0.026–0.580 | |
| >10 µg/L Hg (%) | 25 (27.2%) | 21 (30.9%) | 4 (16.7%) | 0 (0%) | |
| >50 µg/L Hg (%) | 8 (8.7%) | 7 (10.3%) | 1 (4.2%) | 0 (0%) | |
| SG-adj. Urinary Hg c (µg/L) | |||||
| Mean (SD) | 22.8 (107.8) d | 29.3 (124.9) e | 4.22 (6.88) | 0.216 (0.194) | |
| Median | 3.35 | 5.18 | 1.18 | 0.154 | |
| IQR b | 1.14, 10.5 | 1.92, 12.7 | 0.733, 3.61 | 0.095, 0.261 | |
| Min-Max | 0.18–998 | 0.188–998 | 0.212–25.8 | 0.042–1.24 | |
| >10 µg/L Hg (%) | 24 (26.0%) | 20 (29.4%) | 4 (16.7%) | 0 (0%) | |
| >50 µg/L Hg (%) | 4 (4.3%) | 4 (5.9%) | 0 (0%) | 0 (0%) | |
| Hair Hg (µg/g) | n | 70 | 51 | 19 | 59 |
| Mean (SD) | 0.974 (0.748) d | 1.13 (0.809) e | 0.558 (0.272) | 0.231 (0.202) | |
| Median | 0.783 | 0.967 | 0.419 | 0.181 | |
| IQR b | 0.408, 1.22 | 0.589, 1.47 | 0.329, 0.781 | 0.119, 0.244 | |
| Min-Max | 0.132–3.69 | 0.132–3.69 | 0.237–1.10 | 0.037–1.37 | |
| Study Location | Media | Year Collected | n | Mean (SD) | Median | Min.-Max. | Exceeds Guideline (%) | Guideline Value |
|---|---|---|---|---|---|---|---|---|
| Kejetia women of childbearing age | Urine | 2010 | 84 | 7.82 (38.2) | 1.38 | 0.096–336.7 | 5 (6.0) | 10 µg/L a |
| Kejetia women of childbearing age | Hair | 2010 | 80 | 1.66 (10.3) | 0.359 | 0.097–92.6 | 1 (1.3) | 11.1 µg/g b |
| Gorogo households | Soil | 2011 | 26 | 0.041 (0.023) | 0.039 | 0.013–0.114 | 0 (0%) | 6.6 µg/g c |
| Kejetia households | Soil | 2010 | 17 | 4.78 (9.78) | 2.16 | 0.096–40.969 | 3 (17.6) | |
| Kejetia households | Soil | 2011 | 54 | 15.6 (46.9) | 3.05 | 0.297–330.04 | 18 (33.3) | |
| Bolgatanga gold refinery | Soil | 2012 | 4 | 57.8 (58.2) | 54.6 | 5.43–116.44 | 3 (75.0) | |
| Kejetia and surrounding areas | Sediment | 2010 | 14 | 0.036 (0.062) | 0.021 | 0.005–0.248 | 1 (7.1) | 0.170 µg/g d |
| Kejetia and surrounding areas | Fish (unknown fresh water species) | 2010 | 12 | 0.070 (0.057) | 0.045 | 0.024–0.220 | 0 (0%) | 0.3 µg/g e |
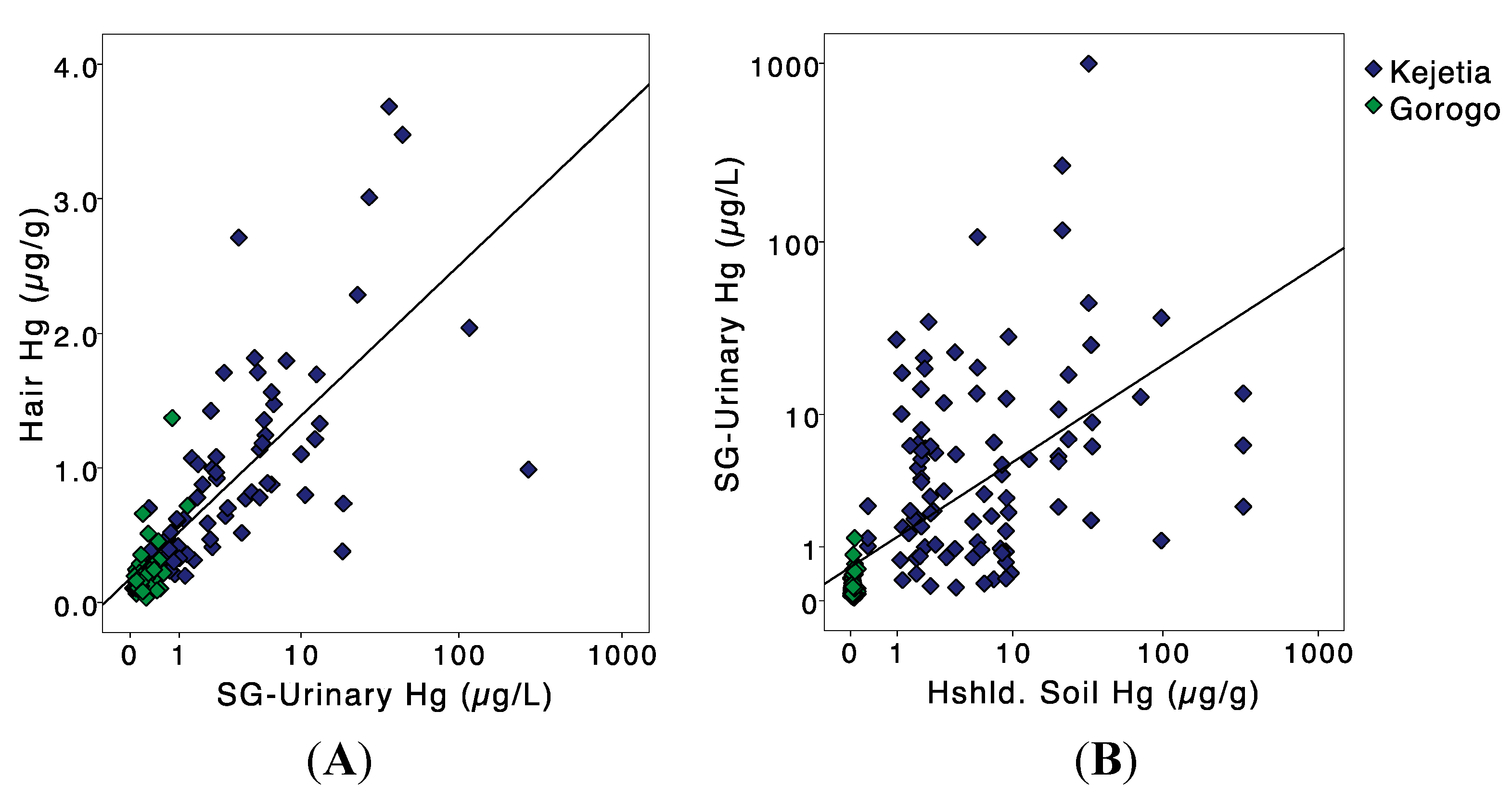


3.3. Mercury in Ecological Samples
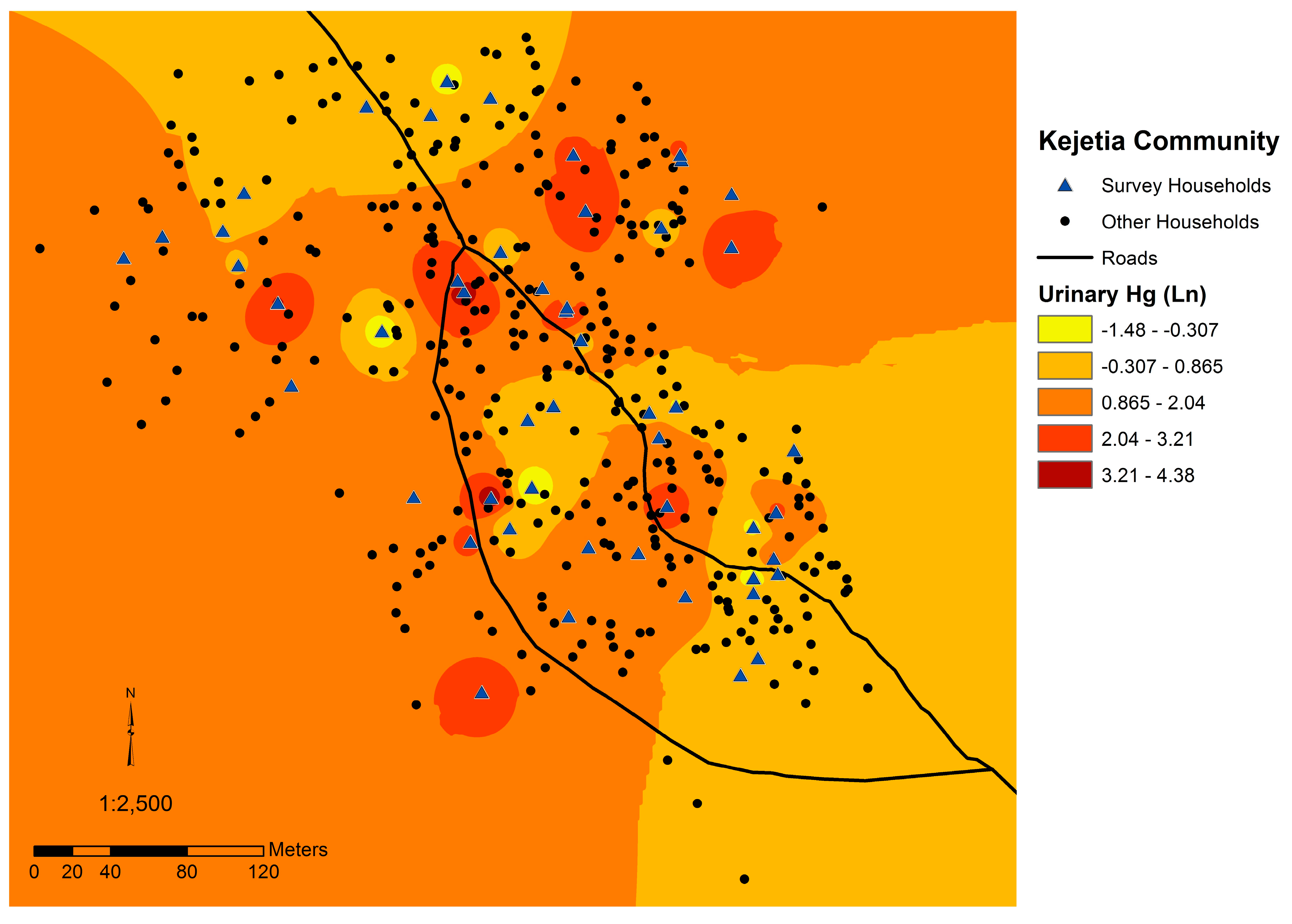
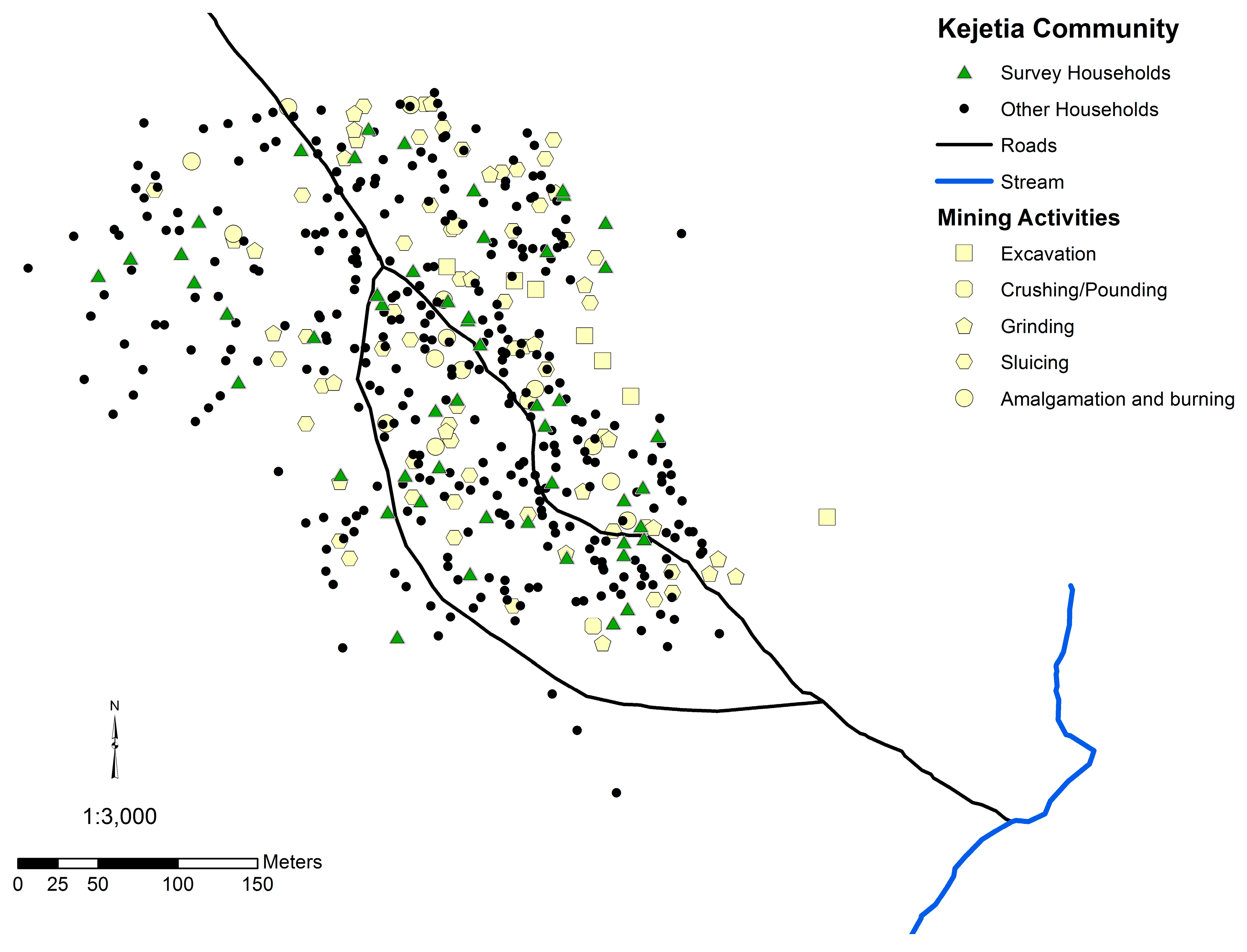
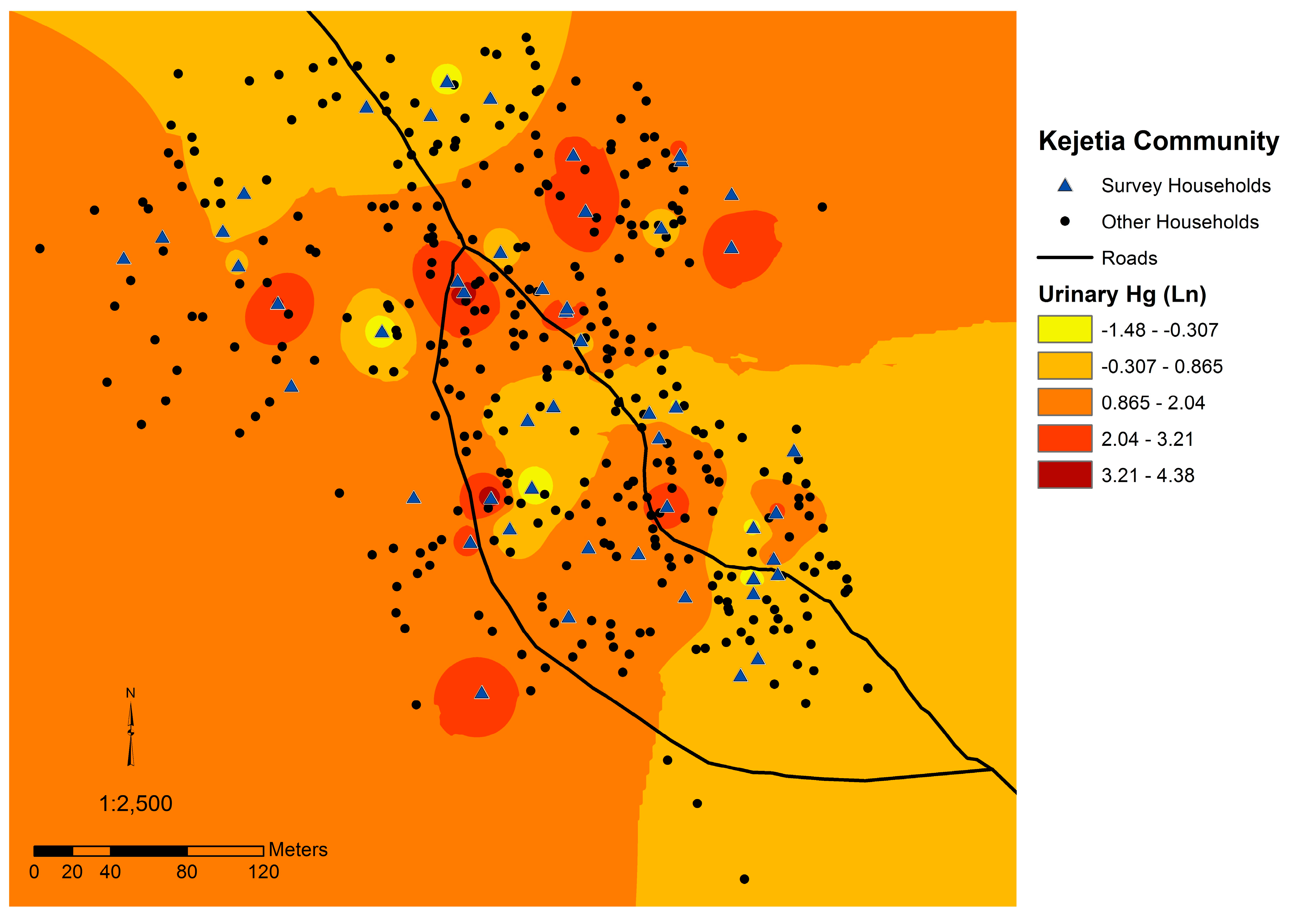
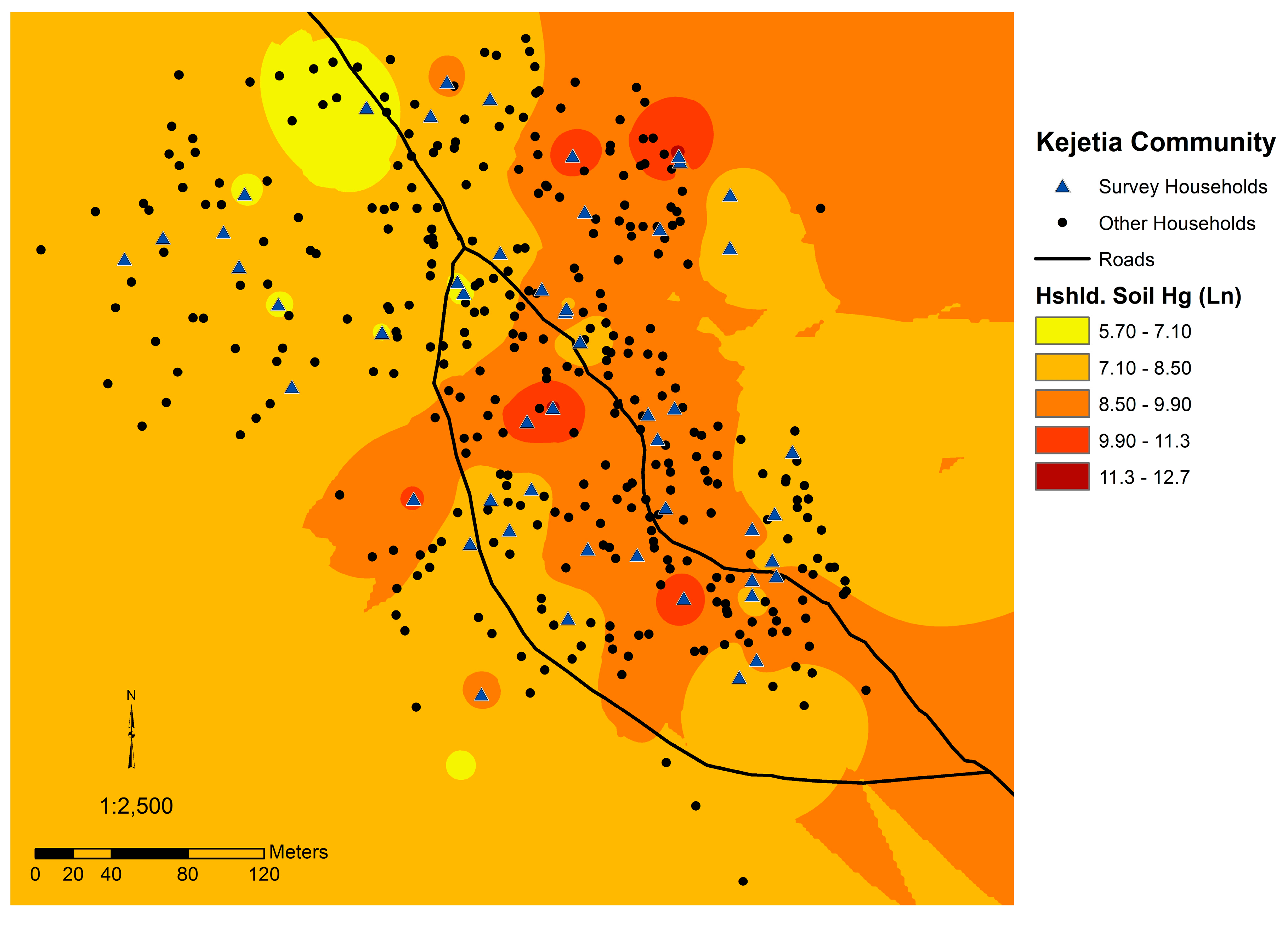
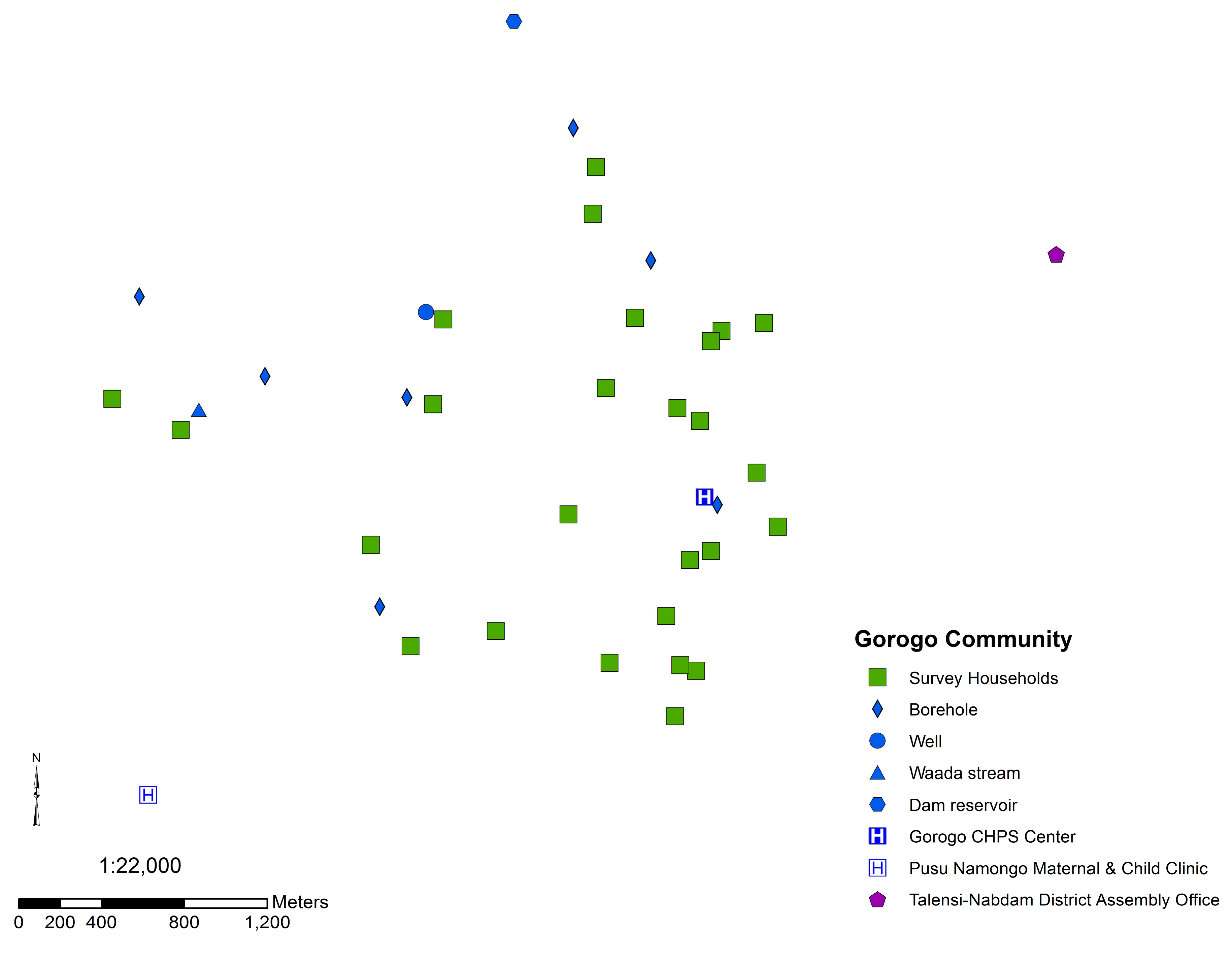
3.4. Spatial Analyses

| Inadvertent Ingestion | Occasional Ingestion (Pica) | Habitual Ingestion (Geophagy) | |||||
|---|---|---|---|---|---|---|---|
| Central Tendency | Worst-case | Central Tendency | Worst-case | Central Tendency | Worst-case | ||
| Population | Reference population: | U.S. adults | US adults; Tanzanians | US adults | Tanzanians | US adults | Tanzanians |
| Reference: | [38] | [38,47,48] | [38] | [48] | [38] | [48] | |
| Soil & dust ingestion (mg/day): a | 50; 110 b | 200 | 1000 | 13600 | 50000 | 85000 | |
| Kejetia | µg Hg ingested/day | 2.06 | 4.68 | 23.4 | 318 | 1170 | 1990 |
| µg Hg/kg body weight/day | 0.037 | 0.082 | 0.409 | 5.57 | 20.5 | 34.8 | |
| n (%) > 0.3 µg Hg/kg body weight/day c | 4 (4.1) | 6 (6.2) | 20 (20.8) | 84 (86.6) | 94 (96.9) | 96 (99.0) | |
| Gorogo | µg Hg ingested/day | 0.002 | 0.008 | 0.042 | 0.574 | 2.11 | 3.58 |
| µg Hg/kg body weight/day | 3.9 × 10−5 | 2.0 × 10−4 | 8.0 × 10−4 | 0.01 | 0.038 | 0.064 | |
| n (%) > 0.3 µg Hg/kg body weight/day c | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Bolgatanga Refinery: Adults | µg Hg ingested/day | 2.89 d | 11.56 | 57.8 | 786.08 | 2890 | 4913 |
| µg Hg/kg body weight/day e | 0.044 | 0.178 | 0.889 | 12.1 | 44.5 | 75.6 | |
3.5. Soil and Hg Ingestion
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
| Mining Activity | Kejetia | Miners a | Females | Males | ||||
|---|---|---|---|---|---|---|---|---|
| n | Percent | n | Percent | n | Percent | n | Percent | |
| Any mining activity | 75 | 77.3 | 71 | 100.0 | 31 | 66.0 | 44 | 88.0 |
| Excavation | 40 | 41.2 | 39 | 54.9 | 2 | 4.3 | 38 | 76.0 |
| Crushing | 45 | 46.4 | 44 | 62.0 | 7 | 14.9 | 38 | 76.0 |
| Sifting | 45 | 46.4 | 42 | 59.2 | 30 | 63.8 | 15 | 30.0 |
| Washing | 46 | 47.4 | 45 | 63.4 | 13 | 27.7 | 33 | 66.0 |
| Amalgamation | 49 | 50.5 | 47 | 66.2 | 16 | 34.0 | 33 | 66.0 |
| Burning | 31 | 32.0 | 31 | 43.7 | 7 | 14.9 | 24 | 48.0 |
| Owning | 21 | 21.6 | 20 | 28.2 | 1 | 2.1 | 20 | 40.0 |
| Ore Mining Stage | n Samples in Ore Stage | Mean (SD) (µg/g Hg) |
|---|---|---|
| Crushed | 4 | 1.486 (0.933) |
| Finely ground | 4 | 0.9263 (0.7609) |
| Washed | 2 | 0.3492 (0.1006) |
Acknowledgments
Author Contributions
Conflicts of Interest
References
- United Nations Environment Programme (UNEP). Global Mercury Assessment 2013: Sources, Emissions, Releases and Environmental Transport; UNEP: Geneva, Switzerland, 2013. [Google Scholar]
- International Labour Organization. Social and Labour Issues in Small-Scale Mines. Report for Discussion at the Tripartite Meeting on Social and Labour Issues in Small-Scale Mines; International Labour Organization: Geneva, Switzerland, 1999. [Google Scholar]
- United Nations Environment Programme (UNEP). Addressing the Social and Financial Challenges of Artisanal and Small Scale Gold Mining: Meeting Summary; UNEP: Geneva, Switzerland, 2010. [Google Scholar]
- United Nations Environment Programme (UNEP). Reducing Mercury in Artisanal and Small-Scale Gold Mining (ASGM). Available online: http://www.unep.org/chemicalsandwaste/Mercury/GlobalMercuryPartnership/ArtisanalandSmall-ScaleGoldMining/tabid/3526/Default.aspx (accessed on 1 May 2015).
- Clarkson, T.W.; Magos, L. The toxicology of mercury and its chemical compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef] [PubMed]
- Basu, N.; Clarke, E.; Green, A.; Long, R.; Calys-Tagoe, B.; Chan, L.H.M.; Dzodzomenyo, M.; Fobil, J.N.; Neitzel, R.L.; Obiri, S.; et al. Integrated Assessment of Artisanal and Small-Scale Gold Mining in Ghana-Part 1: Human Health Review. Int. J. Environ. Res. Public Health 2015, 12, 5143–5176. [Google Scholar]
- Rajaee, M.; Obiri, S.; Green, A.; Long, R.; Cobbina, S.; Nartey, V.; Buck, D.; Antwi, E.; Basu, N. Integrated assessment of artisanal and small-scale gold mining in Ghana-Part 2: Natural sciences review. Int. J. Environ. Res. Public Health 2015, 12, 8971–9011. [Google Scholar] [CrossRef] [PubMed]
- Ghana Chamber of Mines. Performance of the Mining Industry in 2013. Available online: http://ghanachamberofmines.org/en/our-publications.php (accessed on 31 August 2015).
- Ghana Chamber of Mines. Factoid 2011. Available online: http://ghanachamberofmines.org/en/our-publications.php (accessed on 31 August 2015).
- Hilson, G.M.; Clifford, M.J. Small-scale gold mining, the environment and human health: An introduction to the Ghana case. Int. J. Environ. Pollut. 2010, 41, 185–194. [Google Scholar] [CrossRef]
- Hilson, G.M. Child labour in African artisanal mining communities: Experiences from northern Ghana. Dev. Change 2010, 41, 445–473. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency (EPA). Mercury Study Report to Congress Volume III: Fate and Transport of Mercury in the Environment; EPA: Washington, DC, USA, 1997; Volume III. [Google Scholar]
- United Nations Environment Programme (UNEP). Global Mercury Assessment; UNEP: Geneva, Switzerland, 2002. [Google Scholar]
- Sherman, L.S.; Blum, J.D.; Basu, N.; Rajaee, M.; Evers, D.C.; Buck, D.G.; Petrlik, J.; Digangi, J. Assessment of mercury exposure among small-scale gold miners using mercury stable isotopes. Environ. Res. 2015, 137, 226–234. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency (EPA). Mercury Study Report to Congress: Health Effects of Mercury and Mercury Compounds; EPA: Washington, DC, USA, 1997; Volume V. [Google Scholar]
- Bluhm, R.E.; Bobbitt, R.G.; Welch, L.W.; Wood, A.J.J.; Bonfiglio, J.F.; Sarzen, C.; Heath, A.J.; Branch, R.A. Elemental mercury vapor toxicity, treatment, and prognosis after acute, intensive Exposure in chloralkali plant workers. Part I: History, neuropsychological findings and chelator effects. Hum. Exp. Toxicol. 1992, 11, 201–210. [Google Scholar] [PubMed]
- Wranová, K.; Čejchanová, M.; Spěváčková, V.; Korunová, V.; Vobecký, M.; Spěváček, V. Mercury and methylmercury in hair of selected groups of Czech population. Cent. Eur. J. Public Health 2008, 17, 36–40. [Google Scholar]
- Dooyema, C.A.; Neri, A.; Lo, Y.; Durant, J.; Dargan, P.I.; Swarthout, T.; Biya, O.; Gidado, S.O.; Haladu, S.; Sani-Gwarzo, N.; et al. Outbreak of fatal childhood lead poisoning related to artisanal gold mining in northwestern Nigeria, 2010. Environ. Health Perspect. 2012, 120, 601–607. [Google Scholar] [PubMed]
- Plumlee, G.S.; Durant, J.T.; Morman, S.A.; Neri, A.; Wolf, R.E.; Dooyema, C.A.; Hageman, P.L.; Lowers, H.A.; Fernette, G.L.; Meeker, G.P.; et al. Linking geological and health sciences to assess childhood lead poisoning from artisanal gold mining in Nigeria. Environ. Health Perspect. 2013, 121, 744–750. [Google Scholar] [PubMed]
- Njiru, H.; Elchalal, U.; Paltiel, O. Geophagy during pregnancy in Africa: A literature review. Obstet. Gynecol. Surv. 2011, 66, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Vermeer, D.E. Geophagy among the Ewe of Ghana. Ethnology 1971, 10, 56–72. [Google Scholar] [CrossRef]
- Baidoo, S.E.; Tay, S.C. K.; Abruquah, H.H. Intestinal helminth infection and anaemia during pregnancy: A community based study in Ghana. Afr. J. Microbiol. Res. 2010, 4, 1713–1718. [Google Scholar]
- Nyanza, E.C.; Joseph, M.; Premji, S.S.; Thomas, D.S.; Mannion, C. Geophagy practices and the content of chemical elements in the soil eaten by pregnant women in artisanal and small scale gold mining communities in Tanzania. BMC Pregnancy Childbirth 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Paruchuri, Y.; Siuniak, A.; Johnson, N.; Levin, E.; Mitchell, K.; Goodrich, J.M.; Renne, E.P.; Basu, N. Occupational and environmental mercury exposure among small-scale gold miners in the Talensi-Nabdam District of Ghana’s upper east region. Sci. Total Environ. 2010, 408, 6079–6085. [Google Scholar] [CrossRef] [PubMed]
- Renne, E.; Basu, N.; Gager, E.; Koomson, E.; Lee, B.; Lee, S.; Leeth, A.; Manigault, D., III; Rajaee, M.; Sajjad, A.; et al. Women’s Work, Health and the Environment in a Small-Scale Mining Site in Norteastern Ghana. Women Environ. Int. Mag. 2011, 86/87, 13–16. [Google Scholar]
- National Renewable Energy Laboratory (NREL). Geospatial Toolkit GIS Data for Ghana from NREL. Available online: http://en.openei.org/datasets/dataset/integrated-geospatial-toolkit-gis-data-for-ghana-from-nrel (accessed on 1 November 2010).
- Hoshaw-Woodard, S. Description and Comparison of the Methods of Cluster Sampling and Lot Quality Assurance Sampling to Assess Immunization Coverage; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Ghana Statistical Service (GSS); Ghana Health Service (GHS); ICF Macro. Ghana Demographic and Health Survey 2008; GSS, GHS, and ICF Macro: Accra, Ghana, 2009. [Google Scholar]
- Ferris, B.G. Epidemiology standardization project. Am. Thorac. Soc. 1978, 118, 1–120. [Google Scholar]
- Goodrich, J.M.; Wang, Y.; Gillespie, B.; Werner, R.; Franzblau, A.; Basu, N. Methylmercury and elemental mercury differentially associate with blood pressure among dental professionals. Int. J. Hyg. Environ. Health 2012, 216, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Mason, B.J. Preparation of Soil Sampling Protocols: Sampling Techniques and Strategies; U.S. Environmental Protection Agency: Washington, DC, USA, 1992. [Google Scholar]
- U.S. Environmental Protection Agency (EPA). Mercury in Solids and Solutions by Thermal Decomposition, Amalgamation, and Atomic Absorption Spectrophotometry; EPA: Washington, DC, USA, 2007. [Google Scholar]
- Lee, E.; Park, H.K.; Kim, H.J. Adjustment of urinary mercury in health risk assessment of mercury. J. Korean Med. Sci. 1996, 11, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Voinescu, G.C.; Shoemaker, M.; Moore, H.; Khanna, R.; Nolph, K.D. The relationship between urine osmolality and specific gravity. Am. J. Med. Sci. 2002, 323, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Suwanzono, Y.; Akesson, A.; Alfvén, T.; Järup, L.; Vahter, M. Creatinine vs. specific gravity-adjusted urinary cadmium concentrations. Biomarkers 2005, 10, 117–126. [Google Scholar]
- Moriguchi, J.; Ezaki, T.; Tsukahara, T.; Fukui, Y.; Ukai, H.; Okamoto, S.; Shimbo, S.; Sakurai, H.; Ikeda, M. Decreases in urine specific gravity and urinary creatinine in elderly women. Int. Arch. Occup. Env. Health 2005, 78, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Praditpornsilpa, K.; Townamchai, N.; Chaiwatanarat, T.; Tiranathanagul, K.; Katawatin, P.; Susantitaphong, P.; Trakarnvanich, T.; Kanjanabuch, T.; Avihingsanon, Y.; Tungsanga, K.; et al. The need for robust validation for MDRD-based glomerular filtration rate estimation in various CKD populations. Nephrol. Dial. Transplant. 2011, 26, 2780–2785. [Google Scholar] [PubMed]
- U.S. Environmental Protection Agency (EPA). Exposure Factors Handbook: 2011 Edition; EPA: Washington, DC, USA, 2011. [Google Scholar]
- U.S. Environmental Protection Agency (EPA). Mercuric Chloride (HgCl2) (CASRN 7487-94-7). Available online: http://www.epa.gov/iris/subst/0692.htm (accessed on 1 May 2015).
- Risher, J.F. Elemental Mercury and Inorganic Mercury Compounds: Human Health Aspects; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- UNEP DTIE Chemicals Branch; WHO Department of Food Safety; Zoonoses and Foodborne Diseases. Guidance for Identifying Populations At Risk From Mercury Exposure; UNEP and WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Canadian Council of Ministers of the Environment. Canadian soil quality guidelines for the protection of environmental and human health-Mercury (inorganic). In Canadian Environmental Quality Guidelines, 1999; Canadian Council of Ministers of the Environment: Winnipeg, MB, Canada, 1999; pp. 1–8. [Google Scholar]
- Canadian Council of Ministers of the Environment. Canadian sediment quality guidelines for the protection of aquatic life-Mercury. In Canadian Environmental Quality Guidelines, 1999; Canadian Council of Ministers of the Environment: Winnipeg, MB, Canada, 1999; pp. 1–5. [Google Scholar]
- U.S. Environmental Protection Agency (EPA). Water Quality Criterion for the Protection of Human Health: Methylmercury; EPA: Washington, DC, USA, 2001. [Google Scholar]
- World Health Organization. Recommended Health-Based Limits in Occupational Exposure to Heavy Metals; World Health Organization: Geneva, Switzerland, 1980. [Google Scholar]
- Geissler, P.W.; Shulman, C.E.; Prince, R.J.; Mutemi, W.; Mnazi, C.; Friis, H.; Lowe, B. Geophagy, iron status and anaemia among pregnant women on the coast of Kenya. Trans. R. Soc. Trop. Med. Hyg. 1998, 92, 549–553. [Google Scholar] [CrossRef]
- Taylor, H.; Appleton, J.D.; Lister, R.; Smith, B.; Chitamweba, D.; Mkumbo, O.; Machiwa, J.F.; Tesha, A.L.; Beinhoff, C. Environmental assessment of mercury contamination from the Rwamagasa artisanal gold mining centre, Geita District, Tanzania. Sci. Total Environ. 2005, 343, 111–133. [Google Scholar] [CrossRef] [PubMed]
- Appleton, J.D.; Taylor, H.; Lister, T.R.; Smith, B.; Drasch, G.; Boese-O’Reilly, S. Final Report for an Assessment of the Environment and Health in the Rwamagasa Area, Tanzania. UNIDO Project EG/GLO/01/G34; British Geological Survey: Keyworth, Kottingham, 2004. [Google Scholar]
- Bolgatanga Municipal Assembly Bolgatanga Municipal Assembly: About This Municipality. Available online: http://bolga.ghanadistricts.gov.gh/?arrow=atd&_=100&sa=1216 (accessed on 1 May 2015).
- Adimado, A.A.; Baah, D.A. Mercury in Human Blood, Urine, Hair, Nail, and Fish from the Ankobra and Tano River Basins in Southwestern Ghana. Bull. Environ. Contam. Toxicol. 2002, 68, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Donkor, A.K.; Bonzongo, J.C.; Nartey, V.K.; Adotey, D.K. Mercury in different environmental compartments of the Pra River Basin, Ghana. Sci. Total Environ. 2006, 368, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Kwaansa-Ansah, E.E.; Basu, N.; Nriagu, J.O. Environmental and occupational exposures to mercury among indigenous people in Dunkwa-On-Offin, a small scale gold mining area in the South-West of Ghana. Bull. Environ. Contam. Toxicol. 2010, 85, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Anim, E.T.; Agorku, E.S.; Anim, A.K. A comparative analysis on levels of mercury in human scalp hair of students from different locations in Ghana. Res. J. Environ. Earth Sci. 2011, 3, 293–296. [Google Scholar]
- Voegborlo, R.B.; Matsuyama, A.; Adimado, A.A.; Akagi, H. Head hair total mercury and methylmercury levels in some Ghanaian individuals for the estimation of their exposure to mercury: Preliminary studies. Bull. Environ. Contam. Toxicol. 2010, 84, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Asante, K.A.; Agusa, T.; Subramanian, A.; Ansa-Asare, O.D.; Biney, C.A.; Tanabe, S.; Ansong, K. Contamination status of arsenic and other trace elements in drinking water and residents from Tarkwa, a historic mining township in Ghana. Chemosphere 2007, 66, 1513–1522. [Google Scholar] [CrossRef] [PubMed]
- Abrefah, R.; Adotey, D.K.; Mensimah, E.; Ampomah-Amoako, E.; Sogbadji, R.; Opata, N. Biomonitoring of occupational exposure to total arsenic and total mercury in urine of goldmine workers in southwestern Ghana. Environ. Res. Eng. Manag. 2011, 2, 43–48. [Google Scholar] [CrossRef]
- Bonzongo, J.J.; Donkor, A.K.; Nartey, V.K.; Lacerda, L.D. Mercury pollution in Ghana: A case study of environmental impacts of artisanal gold mining in Sub-Saharan Africa. In Environmental Geochemistry in Tropical and Subtropical Environments; Drude de Lacerda, L., Santelli, R.E., Duursma, E.K., Abrão, J.J., Eds.; Springer Berlin Heidelberg: Berlin, Heidelberg, Germany, 2004; pp. 135–156. [Google Scholar]
- Adjorlolo-Gasokpoh, A.; Golow, A.A.; Kambo-Dorsa, J. Mercury in the surface soil and cassava, manihot esculenta (flesh, leaves and peel) near goldmines at Bogoso and Prestea, Ghana. Bull. Environ. Contam. Toxicol. 2012, 89, 1106–1110. [Google Scholar] [CrossRef] [PubMed]
- Azanu, D. Sorption of Inorganic Mercury on Soils from Ankobra Basin in the South-Western Part of Ghana. Master’s Thesis, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana, 2010. [Google Scholar]
- Ahiamadjie, H.; Serfor-Armah, Y.; Tandoh, J.B.; Gyampo, O.; Ofosu, F.G.; Dampare, S.B.; Adotey, D.K.; Nyarko, B.J.B. Evaluation of trace elements contents in staple foodstuffs from the gold mining areas in southwestern part of Ghana using neutron activation analysis. J. Radioanal. Nucl. Chem. 2011, 288, 653–661. [Google Scholar] [CrossRef]
- Amonoo-Neizer, E.H.; Nyamah, D.; Bakiamoh, S.B. Mercury and arsenic pollution in soil and biological samples around the mining town of Obuasi, Ghana. Water Air Soil Pollut. 1996, 91, 363–373. [Google Scholar] [CrossRef]
- Samlafo, B.V.; Sarsah, L.A.; Quarshie, E.; Serfor-Armah, Y. Arsenic and mercury levels in earthenware clays in otsew in gomoa west district of central region of Ghana using instrumental neutron activation analysis. Res. J. Environ. Earth Sci. 2011, 3, 541–545. [Google Scholar]
- Oppong, S.O.B.; Voegborlo, R.B.; Agorku, S.E.; Adimado, A.A. Total mercury in fish, sediments and soil from the River Pra Basin, southwestern Ghana. Bull. Environ. Contam. Toxicol. 2010, 85, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Tetteh, S.; Golow, A.A.; Essumang, D.K.; Zugle, R. Levels of mercury, cadmium, and zinc in the topsoil of some selected towns in the wassa west district of the western region of Ghana. Soil Sediment Contam. 2010, 19, 635–643. [Google Scholar]
- Quarshie, E.; Nyarko, B.J.B.; Serfor-Armah, Y. Studies of the levels of some toxic elements in soil and tailings from bibiani mining area of Ghana. Res. J. Environ. Earth Sci. 2011, 3, 512–520. [Google Scholar]
- United Nations Environment Programme (UNEP). Minamata Convention on Mercury-Text and Annexes; UNEP: Nairobi, Kenya, 2013. [Google Scholar]
- Talensi-Nabdam District Assembly. Strategic Environmental Report for the District Medium Term Development Plan under the Ghana Shered Growth and Development Agenda 2010–2013: Draft; Talensi-Nabdam District Assembly: Accra, Ghana, 2010. [Google Scholar]
- Revis, N.; Osborne, T.; Holdsworth, G.; Hadden, C. Distribution of mercury species in soil from a mercury-contaminated site. Water Air Soil Pollut. 1989, 45, 105–113. [Google Scholar]
- Liu, G.; Cabrera, J.; Allen, M.; Cai, Y. Mercury characterization in a soil sample collected nearby the DOE Oak Ridge Reservation utilizing sequential extraction and thermal desorption method. Sci. Total Environ. 2006, 369, 384–392. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajaee, M.; Long, R.N.; Renne, E.P.; Basu, N. Mercury Exposure Assessment and Spatial Distribution in A Ghanaian Small-Scale Gold Mining Community. Int. J. Environ. Res. Public Health 2015, 12, 10755-10782. https://doi.org/10.3390/ijerph120910755
Rajaee M, Long RN, Renne EP, Basu N. Mercury Exposure Assessment and Spatial Distribution in A Ghanaian Small-Scale Gold Mining Community. International Journal of Environmental Research and Public Health. 2015; 12(9):10755-10782. https://doi.org/10.3390/ijerph120910755
Chicago/Turabian StyleRajaee, Mozhgon, Rachel N. Long, Elisha P. Renne, and Niladri Basu. 2015. "Mercury Exposure Assessment and Spatial Distribution in A Ghanaian Small-Scale Gold Mining Community" International Journal of Environmental Research and Public Health 12, no. 9: 10755-10782. https://doi.org/10.3390/ijerph120910755
APA StyleRajaee, M., Long, R. N., Renne, E. P., & Basu, N. (2015). Mercury Exposure Assessment and Spatial Distribution in A Ghanaian Small-Scale Gold Mining Community. International Journal of Environmental Research and Public Health, 12(9), 10755-10782. https://doi.org/10.3390/ijerph120910755