
Effect of Television on Obesity and Excess of Weight and Consequences of Health

{kind=link}
Abstract
:1. Introduction
2. Prevalence of Obesity
3. Factors Associated with Increases in Obesity
4. Effect of Mass Media and Lack of Physical Activity on the Incidence of Obesity
5. Physical and Psychological Consequences of Obesity
6. Diseases Caused by Obesity
6.1. Cardiovascular Diseases
6.2. Respiratory Disorders
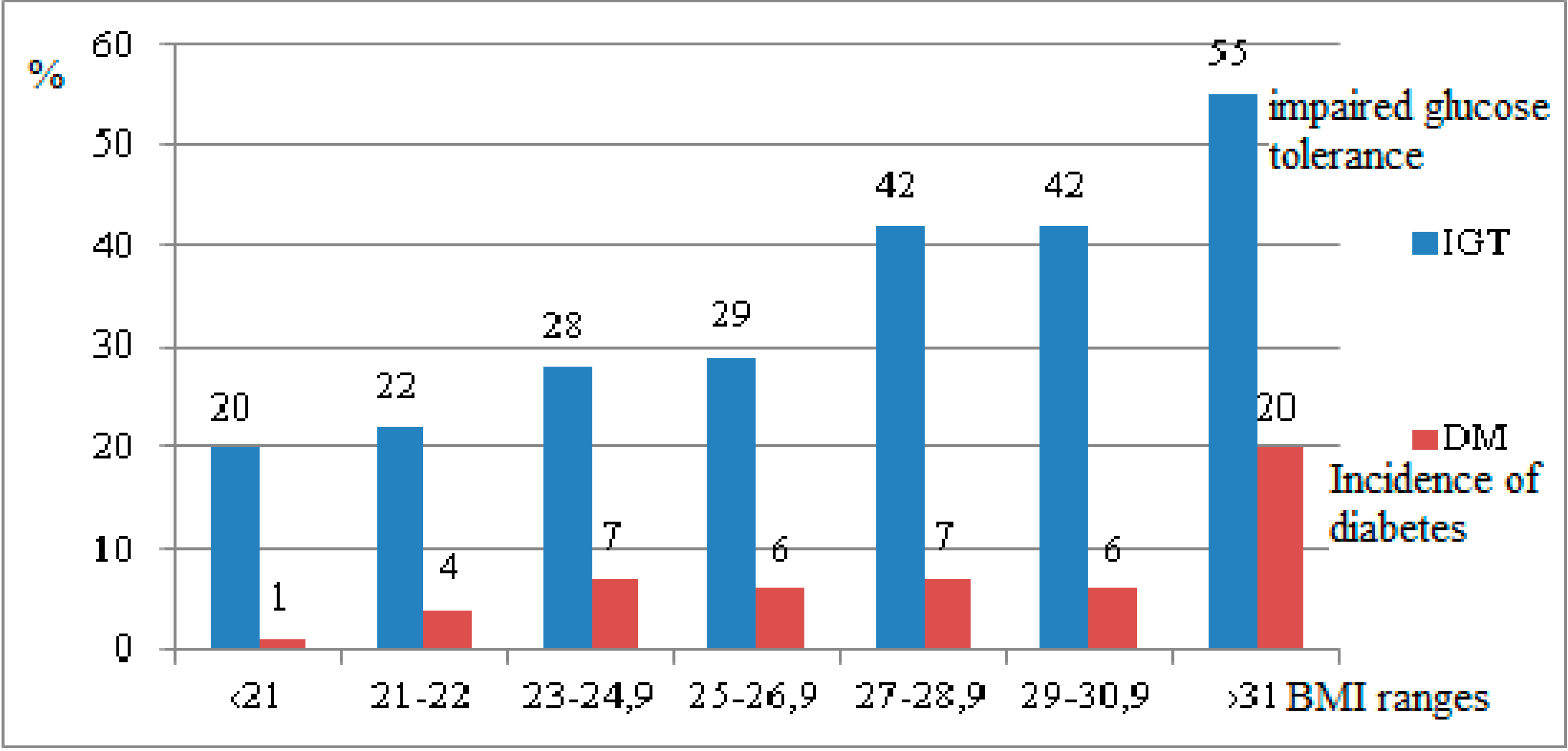
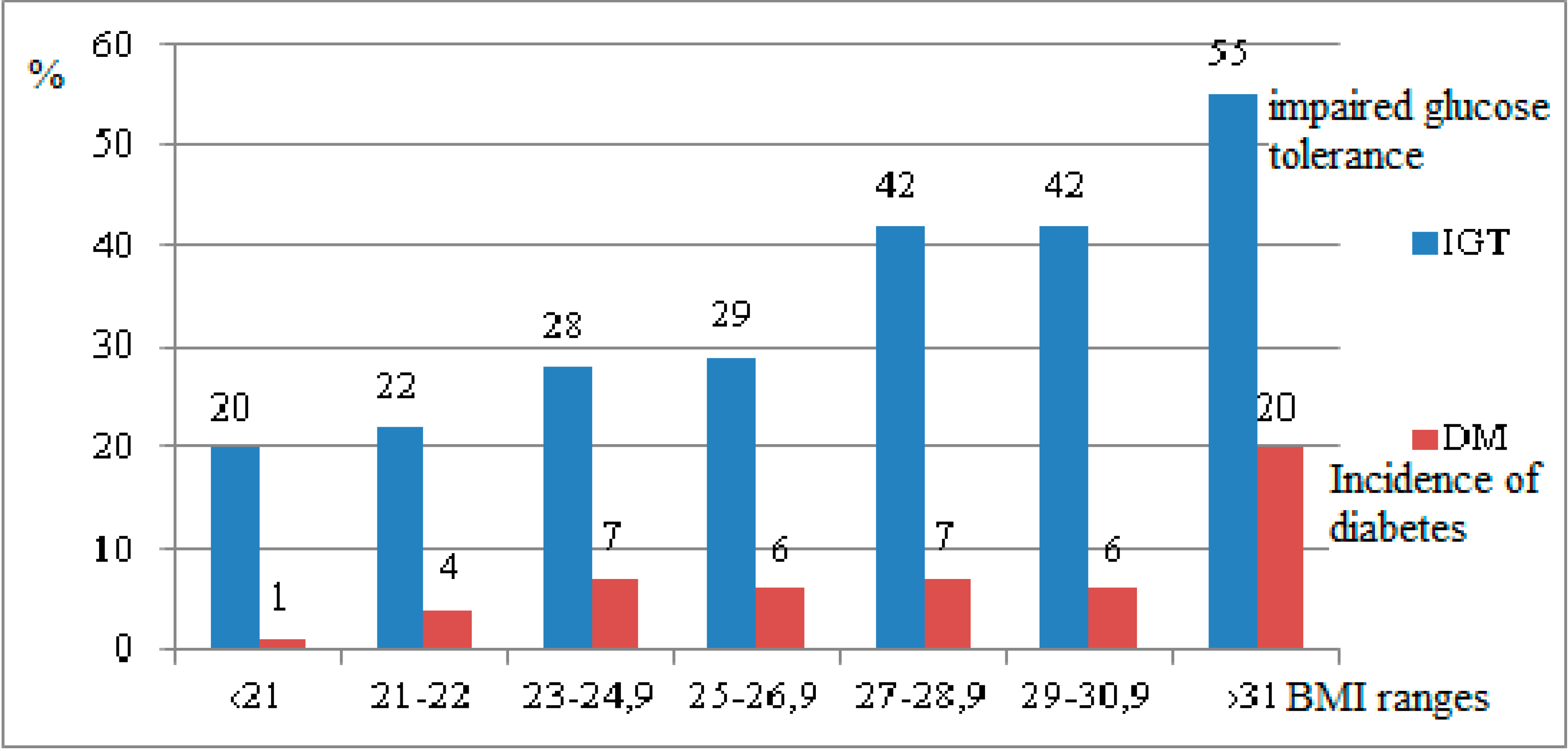
6.3. Diabetes
6.4. Kidney and Cancer Diseases
6.5. Joints and Bones Deformity and Skin Lesions
7. Psychological Consequences of Obesity
8. Prevention of Obesity
9. Summary
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Central Statistical Office. “Population Project 2014–2015”, Statistical Analyses and Studies, Warsaw 2014, Poland. Available online: http://www.stat.gov.pl/ (accessed on 6 August 2015).
- The National Program funded by the Office Marshal Kujawsko-Pomorski. Educational Program—Treatment to Reduce Frequencies. The Prevalence of Overweight and Obesity in Children and Adolescents. Available online: http://wsd.org.pl/Ogloszenia/ (accessed on 6 August 2015).
- Bryła, M.; Maniecka-Bryła, M.; Szymocha, M. Epidemic of obesity in XXI century. Public Health 2009, 119, 207–212. [Google Scholar]
- Mikoś, M.; Mikoś, M.; Mikoś, H.; Obara-Moszyńska, M.; Niedziela, M. Overweight and obesity to children and teenagers. News Med. 2010, 79, 397–402. [Google Scholar]
- Kurowska, M.; Przybylska, D.; Przybylski, P. Obesity and overweight in development population. Hygiena Public Health 2012, 47, 28–35. [Google Scholar]
- Gawęcki, J.; Gerting, H. Nutritional Definitions Dictionary; PWN: Warsawa, Poland, 2001. [Google Scholar]
- Suchocka, Z. Obesity—Grounds and medication, E-newletter of Faculty Pharmaceutical, AMW 2003. no 1.
- Zawistowska, Z. Dietetic Nutrition in Different Kind of Diseases; PZWL: Warsawa, Poland, 1969. [Google Scholar]
- Dietz, W.H.; Bellizzi, M.C. Introduction: The use of body mass index to assess obesity in children. Am. J. Clin. Nutr. 1999, 70, 123S–125S. [Google Scholar] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85. [Google Scholar] [CrossRef]
- Cole, T.; Bellizzi, M.; Flegal, K.; Dietz, W. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Radmacher, S.A.; Sheridan, C.L. Psychology of Health. Challenge for Biomedical Model; Polish Psychology Society: Warsawa, Poland, 1998. [Google Scholar]
- Czarnowska-Misztal, E.; Kunachowicz, H.; Turlejska, H. Rudiments of Human Nutrition; WSiP: Warsawa, Poland, 2000. [Google Scholar]
- Flier, J.S.; Maratos-Flier, E. Cursed with Put on Weight; The Knowledge Word: Warsawa, Poland, 2007. [Google Scholar]
- Bernas, M.; Czech, A.; Tatoń, J. Obesity Metabolic Syndrom; PZWL: Warsawa, Poland, 2006. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. J. Am. Med. A 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Robert Wood Johnson Foundation. Declining Childhood Obesity Rates—Where Are We Seeing the Most Progress? 2012. Available online: http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2012/rwjf401163 (accessed on 6 August 2013).
- Wen, X.; Gillman, M.W.; Rifas-Shiman, S.L.; Sherry, B.; Kleinman, K.; Taveras, E.M. Decreasing prevalence of obesity among young children in Massachusetts from 2004 to 2008. Pediatrics 2012, 129, 823–831. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent and Decrease Overweight and Obesity; U.S. Department of Health and Human Services, Public Health Service, Office of the Surgeon General: Rockville, MD, USA, 2001.
- U.S. Department of Health and Human Services. Prevention Makes Common “Cents”. 2003. Available online: http://aspe.hhs.gov/health/prevention/ (accessed on 6 August 2015). [Google Scholar]
- Duffey, K.J.; Popkin, B.M. Energy density, portion size, and eating occasions: Contributions to increased energy intake in the United States, 1977–2006. PLoS Med. 2011, 8. [Google Scholar] [CrossRef] [PubMed]
- Jahns, L.; Siega-Riz, A.M.; Popkin, B.M. The increasing prevalence of snacking among U.S. children from 1977 to 1996. Pediatrics 2001, 138, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Zizza, C.; Siega-Riz, A.M.; Popkin, B.M. Significant increase in young adults’ snacking between 1977–1978 and 1994–1996 represents a cause for concern! Preve. Med. 2001, 32, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Piernas, C.; Popkin, B.M. Food portion patterns and trends among U.S. children and the relationship to total eating occasion size, 1977–2006. J. Nutr. 2011, 141, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Young, L.R.; Nestle, M. The contribution of expanding portion sizes to the U.S. obesity epidemic. Am. J. Public Health 2002, 92, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Young, L.R.; Nestle, M. Expanding portion sizes in the U.S. marketplace: Implications for nutrition counseling. J. Am. Diet. Assoc. 2003, 103, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Graubard, B.I. Secular trends in patterns of self-reported food consumption of adult Americans: NHANES 1971–1975 to NHANES 1999–2002. Am. J. Clin. Nutr. 2006, 84, 1215–1223. [Google Scholar] [PubMed]
- French, S.A. Public health strategies for dietary change: Schools and worksites. J. Nutr. 2005, 135, 910–912. [Google Scholar] [PubMed]
- Sallis, J.F.; Glanz, K. Physical activity and food environments: Solutions to the obesity epidemic. Milbank Q. 2009, 87, 123–154. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.J.; Frongillo, E.A. Food insecurity and subsequent weight gain in women. Public Health Nutr. 2007, 10, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Chaloupka, F.J. Food prices and obesity: Evidence and policy implications for taxes and subsidies. Milbank Q. 2009, 87, 229–257. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, F.J.; Bell, J.F. Associations of television content type and obesity in children. Am. J. Public Health 2010, 100, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.N. Television viewing and childhood obesity. Pediatr. Clin. North Am. 2001, 48, 1017–1025. [Google Scholar] [CrossRef]
- Ramos, E.; Costa, A.; Araujo, J.; Severo, M.; Lopes, C. Effect of television viewing on food and nutrient intake among adolescents. Nutrition 2013, 29, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Mamun, A.A.; O’Callaghan, M.J.; Williams, G.; Najman, J.M. Television watching from adolescence to adulthood and its association with BMI, waist circumference, waist-to-hip ratio and obesity: A longitudinal study. Public Health Nutr. 2012, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.J.; Biddle, S.J.; Gorely, T.; Cameron, N.; Murdey, I. Relationships between media use, body fatness and physical activity in children and youth: A meta-analysis. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1238–1246. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Ball, K.; Crawford, D. Mediators of longitudinal associations between television viewing and eating behaviours in adolescents. Int. J. Behav. Nutr. Phys. Act. 2011, 8. [Google Scholar] [CrossRef] [PubMed]
- Jeżewska-Zychowicz, M.; Pilska, M. Psychology of Nutrition. Elected Questions; Publishing House SGGW: Warsaw, Poland, 2008. [Google Scholar]
- Temple, J.L.; Giacomelli, A.M.; Kent, K.M.; Roemmich, J.N.; Epstein, L.H. Television watching increases motivated responding for food and energy intake in children. Am. J. Clin. Nutr. 2007, 85, 355–361. [Google Scholar] [PubMed]
- Stankiewicz, M.; Pieszko, M.; Sliwińska, A.; Małgorzewicz, S.; Wierucki, Ł.; Zdrojewski, T.; Wyrzykowski, B.; Łysiak-Szydłowska, W. Obesity and diet awareness among Polish children and adolescents in small towns and villages. Cent. Eur. J. Public Health 2014, 22, 12–16. [Google Scholar] [PubMed]
- Jackson, D.M.; Djafarian, K.; Stewart, J.; Speakman, J.R. Increased television viewing is associated with elevated body fatness but not with lower total energy expenditure in children. Am. J. Clin. Nutr. 2009, 89, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Gorely, T.; Biddle, S.J.; Marshall, S.J. Critical hours: Physical activity and sedentary behavior of adolescents after school. Pediatr. Exerc. Sci. 2008, 20, 446–456. [Google Scholar] [PubMed]
- Arnas, Y. The effects of television food advertisement on children’s food purchasing requests. Pediatr. Int. 2006, 48, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Biddle, S.J.H. Sedentary behavior and dietary intake in children, adolescents, and adults: A systematic review. Am. J. Prev. Med. 2011, 41, 178–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigman, A. Time for a view on screen time. Arch. Dis. Child. 2012, 97, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Pempek, T.A.; Kirkorian, H.L.; Lund, A.F.; Anderson, D.R. The effects of background television on the toy play behavior of very young children. Child Dev. 2008, 79, 1137–1151. [Google Scholar] [CrossRef] [PubMed]
- Strasburger, V.C. Children, adolescents, obesity, and the media. Pediatrics. 2011, 128, 201–208. [Google Scholar] [PubMed]
- Utter, J.; Neumark-Sztainer, D.; Jeffery, R.; Story, M. Couch potatoes or french fries: Are sedentary behaviors associated with body mass index, physical activity, and dietary behaviors among adolescents? J. Am. Diet. Assoc. 2003, 103, 1298–1305. [Google Scholar] [CrossRef]
- Vereecken, C.A.; Todd, J.; Roberts, C.; Mulvihill, C.; Maes, L. Television viewing behaviour and associations with food habits in different countries. Public Health Nutr. 2006, 9, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Sebire, S.J.; Gorely, T.; Cillero, I.H.; Biddle, S.J.H. “I’m on it 24/7 at the moment”: A qualitative examination of multi-screen viewing behaviours among UK 10–11 year olds. Int. J. Behav. Nutr. Phys. Act. 2011, 8. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, I.; Helajarvi, H.; Pahkala, K.; Heinonen, O.J.; Hirvensalo, M.; Palve, K.; Tammelin, T.; Yang, X.; Juonala, M.; Mikkila, V.; et al. Sedentary behaviours and obesity in adults: The Cardiovascular Risk in Young Finns Study. BMJ Open 2013, 3. [Google Scholar] [CrossRef]
- Rideout, V.J.; Foehr, U.G.; Roberts, D.F. Generation of M2 Media in the Lives of 8–18 Year Olds; A Kaiser Family Foundation Study: Menlo, CA, USA, 2010. [Google Scholar]
- Ofcom. Children and Parents: Media Use and Attitudes Report. 2011. Available online: http://stakeholders.ofcom.org.uk/binaries/research/media-literacy/oct2011/Children_and_parents.pdf (accessed on 6 August 2015).
- Routen, A.C. Should our children be sitting comfortably in school? BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed]
- Wijndaele, K.; Brage, S.; Besson, H.; Khaw, K.T.; Sharp, S.J.; Luben, R.; Bhaniani, A.; Wareham, N.J.; Ekelund, U. Increased cardiometabolic risk is associated with increased TV viewing time. Med. Sci. Sports Exerc. 2010, 42, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Grontved, A.; Hu, F.B. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: A meta-analysis. JAMA 2011, 305, 2448–2455. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Li, T.Y.; Colditz, G.A.; Willett, W.C.; Manson, J.E. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA 2003, 289, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haksell, W.L.; Leon, A.S.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, J.R.; Schmitz, K.H.; et al. Compendium of physical activities. Med. Sci. Sports Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Januszewicz, P.; Mazur, A.; Socha, P. Nutrition in Public Health; Publishing House of University in Rzeszow: Rzeszow, Poland, 2009. [Google Scholar]
- Oblacińska, A.; Tabak, I. How Help Corpulent Teenager? Mother and Children Institute: Warsaw, Poland, 2006. [Google Scholar]
- Czech, A.; Bernas, M.; Tatoń, J. Cardiovascular symptoms of obesity. Endocrinology, Obesity and Metabolite Disorders, 2007; no 4. 85–94. [Google Scholar]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.E. Obesity and Cardiovascular Disease: Pathophysiology, Evaluation, and Effect of Weight Loss. Circulation 2006, 113, 898–918. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular disease: Risk factor, paradox, and impact of weight loss. J. Am. Coll. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- Lopes, C. Dietary Factors and Myocardial Infarction: A community-based Case—Control Study. Ph.D. Thesis, University of Porto, Porto, Portugal, November 2000. [Google Scholar]
- Mandecki, T. The Kardiology; PZWL: Warsaw, Poland, 2005. [Google Scholar]
- Lopes, C.; Aro, A.; Azevedo, A.; Ramos, E.; Barros, H. Intake and adipose tissue composition of fatty acids and risk of myocardial infarction in a male Portuguese community sample. J. Am. Diet. Assoc. 2007, 107, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Kavey, R.E.; Daniels, S.R.; Lauer, R.M.; Atkins, D.L.; Hayman, L.L.; Taubert, K. American Heart Association guidelines for primary prevention of atherosclerotic cardiovascular disease beginning in childhood. J. Pediatr. 2003, 142, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Young, J.L. The sclerosis. In Pathophysiology of Heart Diseases; Lilly, L.S., Ed.; Elsevier and Partner: Wroclaw, Poland, 2008. [Google Scholar]
- Cockrill, B.A.; Mandel, J.; Weinberger, S.E. Lungs Diseases; Elsevier and Partner: Wrocław, Poland, 2011. [Google Scholar]
- Kuś, J.; Romińska-Zakrzewska, E. Respiratory Diseases; PZWL: Warsaw, Poland, 2004. [Google Scholar]
- Antczak, A. Great Internal Medicine. Pulmonologist Part II; Medical Tribune Poland: Warsaw, Poland, 2010. [Google Scholar]
- Kowalski, M.L.; Kubsik, B. Asthma and obesity, Allergy Asthma Allergology. 2010; nr 15/1. [Google Scholar] [PubMed]
- Haby, M.M.; Peat, J.K.; Marks, G.B.; Woolcock, A.J.; Leeder, S.R. Asthma in preschool children: Prevalence and risk factors. Thorax 2001, 56, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.K.; Thien, F. Polyunsaturated fats and asthma. Thorax 2002, 57. [Google Scholar] [CrossRef]
- Kokot, F. Internal Diseases. Part 2; PZWL: Warsaw, Poland, 2006. [Google Scholar]
- Bantle, J.P.; Swanson, J.E.; Thomas, W.; Laine, D.C. Metabolic effects of dietary sucrose in type II diabetic subjects. Diabetes Care 1993, 16, 1301–1305. [Google Scholar] [CrossRef] [PubMed]
- Sieradzki, J. Diabetes. Vol I; Via Medica: Gdansk, Poland, 2007. [Google Scholar]
- Bantle, J.P.; Laine, D.C.; Thomas, J.W. Metabolic effects of dietary fructose and sucrose in types I and II diabetic subjects. JAMA 1986, 256, 3241–3246. [Google Scholar] [CrossRef] [PubMed]
- Sieradzki, J. Obesity and diabetes. Medical Guide, 2000; Issue 7. [Google Scholar]
- Szczeklik, A.; Szczeklik’s Internal Medicine. Internal Diseases Student’s book; Practical Medicine: Cracow, Poland, 2012. [Google Scholar]
- Yamada, T. Gastroenterology Student’s Book; Publishing House Czelej Ltd.: Lublin, Poland, 2006. [Google Scholar]
- Konturek, S.J. Gastroenterology and Clinical Hepatology; PZWL: Warsaw, Poland, 2006. [Google Scholar]
- Kokot, F. Internal Diseases. Part I; PZWL: Warsaw, Poland, 2006. [Google Scholar]
- Piecha, G.; Więcek, A. Disorder of reins at corpulent persons—Pathogenesis and medication. Medical Guide, 2012; no 1. [Google Scholar]
- Jeziorski, A. Oncology. Student’s Book for Nurses; PZWL: Warsaw, Poland, 2009. [Google Scholar]
- Kordek, R. Student’s Book for Students and Medicals; Via Medica: Gdansk, Poland, 2007. [Google Scholar]
- Bermeo, S.; Gunaratnam, K.; Duque, G. Fat and bone interactions. Curr. Osteoporos. Rep. 2014, 12, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Hardouin, P.; Pansini, V.; Cortet, B. Bone marrow fat. Joint Bone Spine. 2014, 81, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Jaźwa, P.; Rojek, A.; Snela, S. Impact obesity to result of healing process knee joint’s osteoarthritis with total endoreplacement. Medical review of University in Rzeszow and National Drug Institute in Warsaw: UR, Rzeszow, 2010; no 3. [Google Scholar]
- Scheinfeld, N.S. Obesity and dermatology. Clin. Dermatol. 2004, 22, 303–309. [Google Scholar]
- Hidalgo, L.G. Dermatological Complications of Obesity. Am. J. Clin. Dermatol. 2002, 3, 497–506. [Google Scholar] [CrossRef]
- Burgdorf, W.H.C.; Landthaler, M.; Plewig, G.; Wolff, H.H. Braun—Falco’s Dermatology. Part 3; Publishing House Czelej Ltd.: Lublin, Poland, 2011. [Google Scholar]
- Ogden, J. Psychology of Nourish; Jagiellonian University Publishing House: Cracow, Poland, 2011. [Google Scholar]
- Aue, W. A Man on Environment. Part I; WSiP: Warsaw, Poland, 2006. [Google Scholar]
- Dylewska-Grzelakowska, J. Cosmetology Applied; WSiP: Warsaw, Poland, 1999. [Google Scholar]
- Vandewalle, J.; Moens, E.; Braet, C. Comprehending emotional eating in obese youngsters: The role of parental rejection and emotion regulation. Int. J. Obes. 2013, 38, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Manzoni, G.M.; Pagnini, F.; Gorini, A.; Preziosaet, A.; Castelnuovo, G.; Molinari, E.; Riva, G. “Can Relaxation Training Reduce Emotional Eating in Women with Obesity?”. J. Am. Diet. Assoc. 2009, 109, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Leksy, K. Psychosocial consequences for women with over mass body from a social perspective. Medicine News 2012, 81, 5. [Google Scholar]
- Suchocka, Z. Obesity—Grounds and medication, E-newletter of Faculty Pharmaceutical AMW. 2003; no 1. 16. [Google Scholar]
- Wareham, N.J.; van Sluijs, E.M.; Ekelund, U. Physical activity and obesity prevention: A review of the current evidence. Proc. Nutr. Soc. 2005, 64, 229–247. [Google Scholar] [CrossRef] [PubMed]
- Seo, D.C.; Li, K. Leisure-time physical activity dose-response effects on obesity among US adults: Results from the 1999–2006 National Health and Nutrition Examination Survey. J. Epidemiol. Community Health. 2010, 64, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Tatoń, J. Relatedness between obesity and type 2 diabetes, Polish Weekly Medical. 1995; nr 1, 43–47. [Google Scholar] [PubMed]
- Lee, I.M.; Djousse, L.; Sesso, H.D.; Wang, L.; Buring, J.E. Physical activity and weight gain prevention. JAMA 2010, 303, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Markiewicz, A.; Plewa, M. Physical activity in prophylaxis and medication of obesity. Endocrinology Obesity and Metabolite Disorders 2006, 2, 30–37. [Google Scholar]
- Sallis, J.F.; Glanz, K. Physical activity and food environments: Solutions to the obesity epidemic. Milbank Q. 2009, 87, 123–154. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, M. activity. In Healthy-Polish; Institute of Food and Nutrition: Warszawa, Poland, 2006. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosiek, A.; Maciejewska, N.F.; Leksowski, K.; Rosiek-Kryszewska, A.; Leksowski, Ł. Effect of Television on Obesity and Excess of Weight and Consequences of Health. Int. J. Environ. Res. Public Health 2015, 12, 9408-9426. https://doi.org/10.3390/ijerph120809408
Rosiek A, Maciejewska NF, Leksowski K, Rosiek-Kryszewska A, Leksowski Ł. Effect of Television on Obesity and Excess of Weight and Consequences of Health. International Journal of Environmental Research and Public Health. 2015; 12(8):9408-9426. https://doi.org/10.3390/ijerph120809408
Chicago/Turabian StyleRosiek, Anna, Natalia Frąckowiak Maciejewska, Krzysztof Leksowski, Aleksandra Rosiek-Kryszewska, and Łukasz Leksowski. 2015. "Effect of Television on Obesity and Excess of Weight and Consequences of Health" International Journal of Environmental Research and Public Health 12, no. 8: 9408-9426. https://doi.org/10.3390/ijerph120809408
APA StyleRosiek, A., Maciejewska, N. F., Leksowski, K., Rosiek-Kryszewska, A., & Leksowski, Ł. (2015). Effect of Television on Obesity and Excess of Weight and Consequences of Health. International Journal of Environmental Research and Public Health, 12(8), 9408-9426. https://doi.org/10.3390/ijerph120809408