
Healthy Vinton: A Health Impact Assessment Focused on Water and Sanitation in a Small Rural Town on the U.S.-Mexico Border

Abstract
:1. Introduction
2. Experimental Section
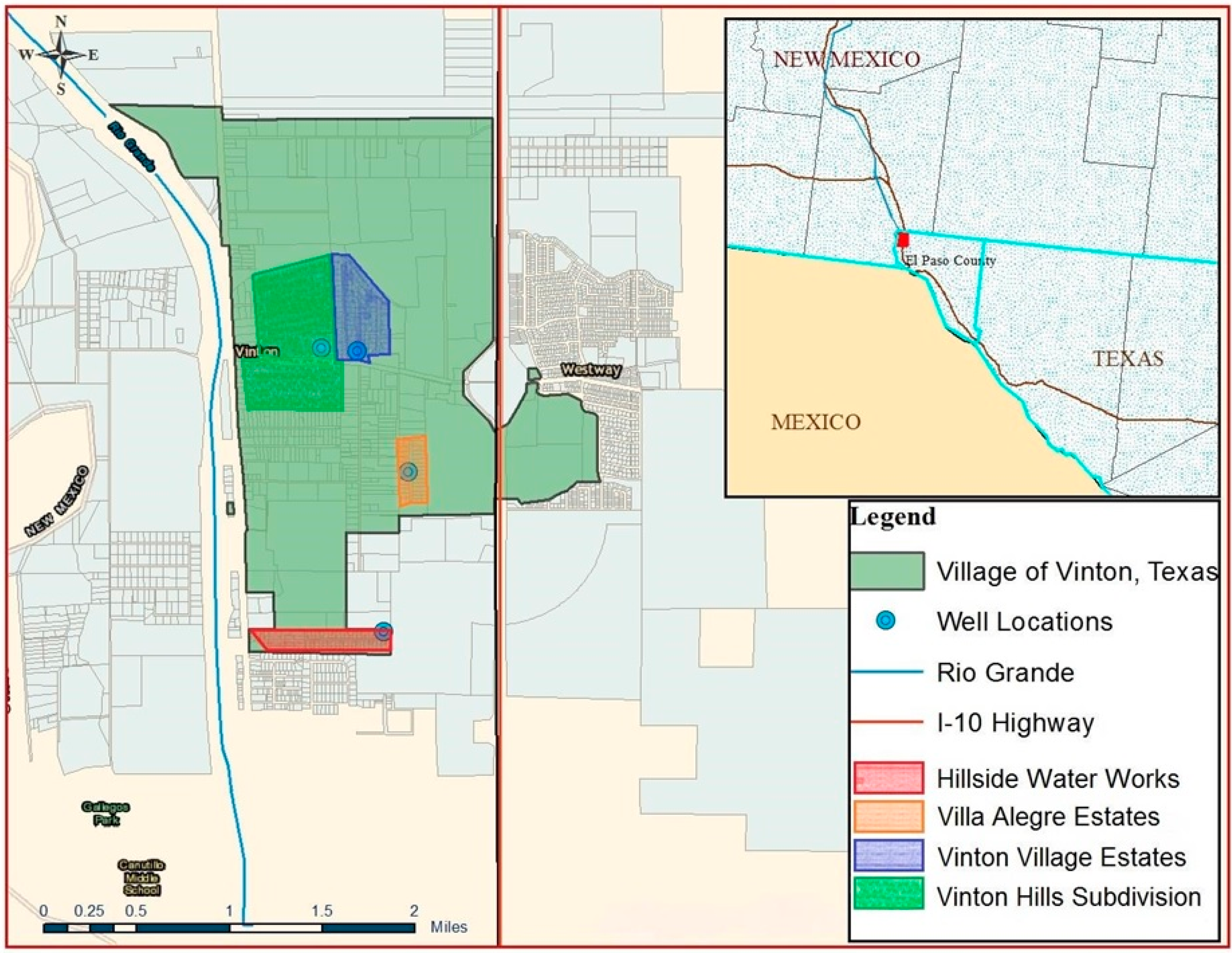
2.1. Case Study Description
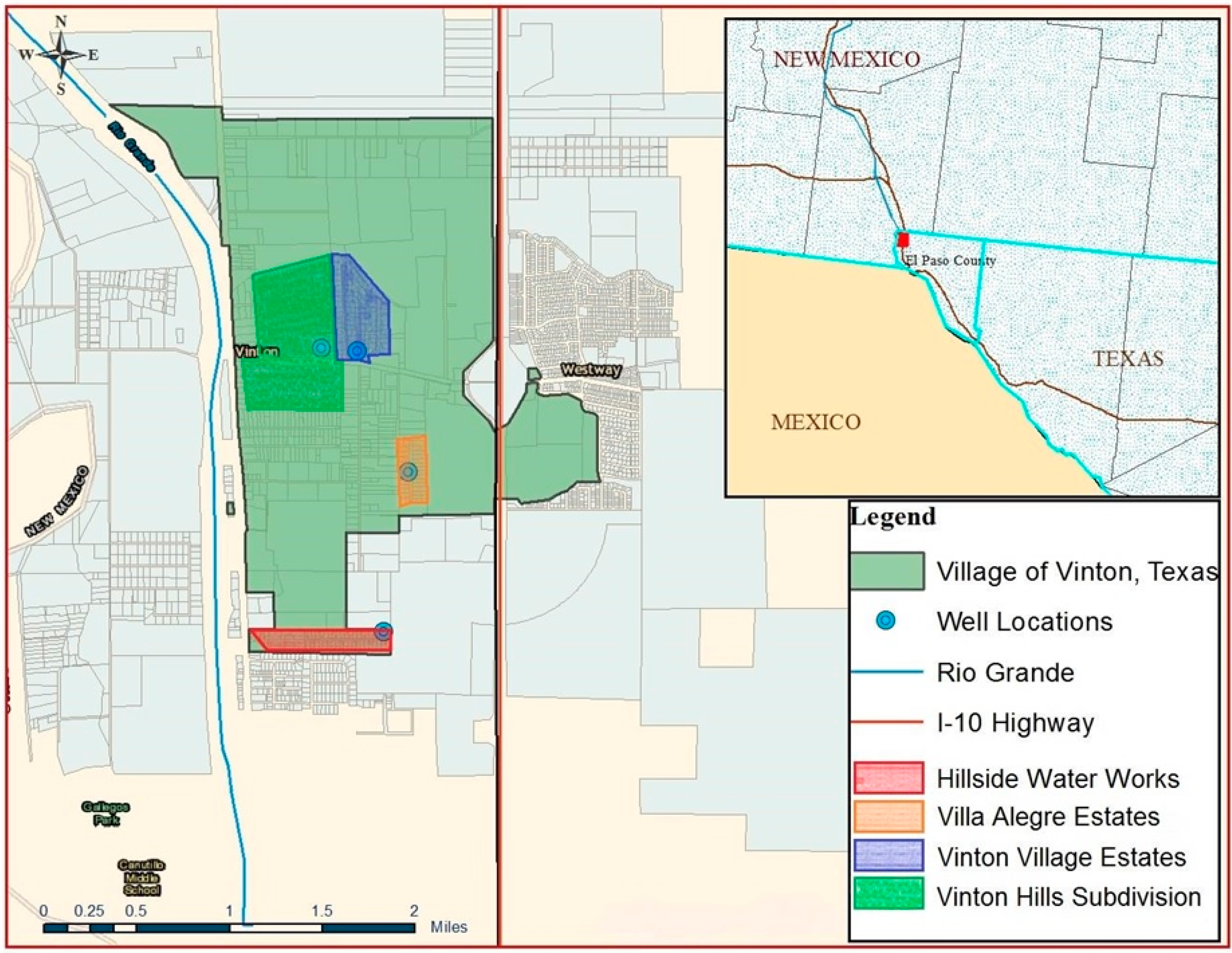
2.1.1. Water System.
2.1.2. Wastewater Collection System.
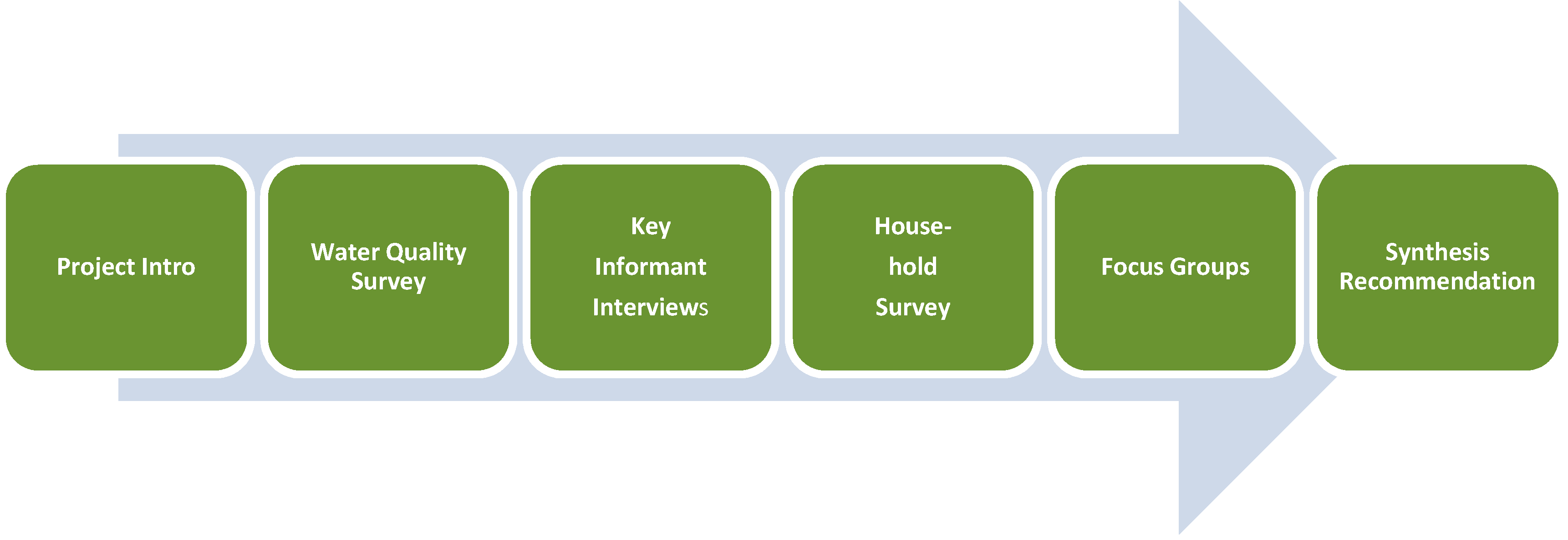
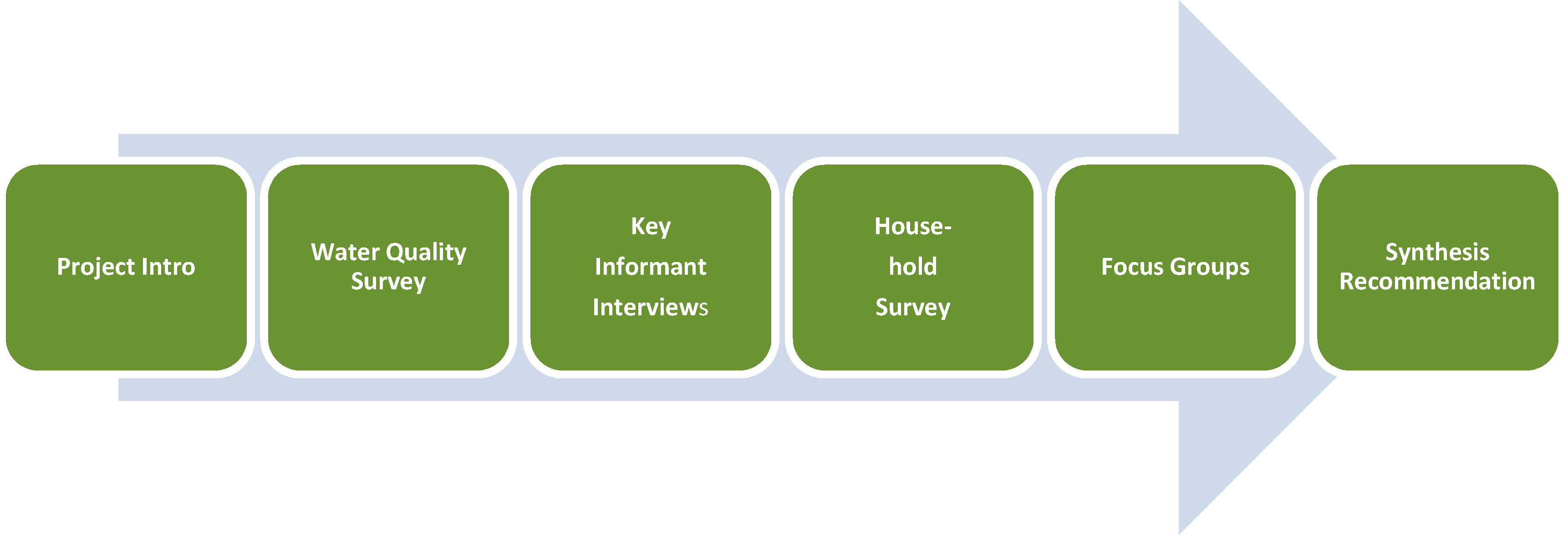
2.2. Methodology

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Water System | Number of Connections | Number of Households with One or Two Water Samples | Number of Surveys | Households with both Water Samples and Survey |
|---|---|---|---|---|
| Vinton Hills Subdivision | 158 | 17 | 40 | 15 |
| Vinton Village Estates | 82 | 9 | 24 | 6 |
| Hillside Water Works | 52 | 13 | 12 | 10 |
| Vinton Mobile Home Park | 36 | 0 ** | 0 ** | 0 ** |
| El Paso Water Utilities | 92 | 12 | 22 | 6 |
| Villa Alegre Estates | 22 | 3 | 5 | 2 |
| Private Wells | 113 * | 15 | 18 | 10 |
| Total (% of Total Households) | 555 | 69 (12%) | 121 (22%) | 49 (9%) |
3. Results and Discussion
3.1. Demographic Characteristics of Vinton and the Participants in Household Surveys in Vinton and Westway
| Characteristics | Vinton | Westway | ||
|---|---|---|---|---|
| Value | % | Value | % | |
| POPULATION | ||||
| Total households surveyed | 121 | 50 | ||
| Median age (respondent) | 48 | 50 | ||
| Total population of participating households | 485 | 170 | ||
| Population of participating households by age range | ||||
| 5 years of age or less | 53 | 11 | 19 | 11 |
| 6 to 17 years of age | 98 | 20 | 30 | 18 |
| 18 to 64 years of age | 300 | 62 | 106 | 62 |
| 65 and more years of age | 34 | 7 | 15 | 9 |
| Mean school years of education (respondent) | 11 | 9.6 | ||
| HOUSING | ||||
| Average household size | 4.0 | 3.4 | ||
| Average years living in this town | 15.6 | 16.7 | ||
| INCOME | ||||
| Median household income estimation | $25,500 | $18,000 | ||
| Household income by range | ||||
| <$10,000–20,000 | 44 | 36 | 29 | 59 |
| $21,000–40,000 | 50 | 41 | 11 | 21 |
| $41,000–60,000 | 11 | 9 | 7 | 14 |
| $61,000–80,000 | 8 | 7 | 3 | 5 |
| >$80,000 | 8 | 7 | 0 | 0 |
| SURVEY | ||||
| Preferred language by participants | ||||
| English | 59 | 49 | 12 | 24 |
| Spanish | 62 | 51 | 38 | 76 |
| Household participation (% of total households contacted who agreed to participate) | 58 | 57 | ||
3.2. Water Quality Survey
| SAMPLE INFORMATION | ARSENIC † | TOTAL DISSOLVED SOLIDS †† | |||||
|---|---|---|---|---|---|---|---|
| Water Sources (total Number connections) | Number of Samples (% of total connections) | Range in As Conc. µg/L | Mean As Conc. ± St. Dev. * µg/L | Number Samples >MCL for As (% > MCL) | Range in TDS Conc. mg/L | Mean TDS Conc. ± St. Dev. * mg/L | Number Samples >Standard for TDS (% > MCL) |
| Hillside Water Works (52) | 23 (44%) | 7.4–12.3 | 10.9 a ± 0.9 | 22 (96%) | 530–830 | 791 b ± 59 | 0 (0%) |
| Vinton Village Estates (82) | 16 (20%) | 8.9–11.1 | 9.5 a,b ± 0.6 | 4 (25%) | 642–692 | 666 b ± 16 | 0 (0%) |
| Domestic Wells (113) | 22 (20%) | 2.6–15.8 | 8.3 a,b ± 5.2 | 9 (39%) | 482–1480 | 832 a,b ± 217 | 3 (14%) |
| El Paso Water Utilities (92) | 22 (24%) | 5.8–13.0 | 6.7 b ± 1.5 | 1 (5%) | 230–802 | 507 b ± 94 | 0 (0%) |
| Vinton Hills Subdivision (158) | 25 (16%) | 4.6–5.6 | 5.0 b ± 0.3 | 0 (0%) | 850–946 | 899 a,b ± 24 | 0 (0%) |
| Villa Alegre Estates (22) | 5 (23%) | 4.6–5.4 | 4.9 b ± 0.3 | 0 (0%) | 988–1020 | 1002 a ± 13 | 2 (40%) |
| Total (519) | 113 (22%) | 2.6–15.8 | 7.8 ± 3.0 | 36 (32%) | 230–1480 | 759 ± 182 | 5 (4%) |
3.3. Household Survey
3.3.1. Practices and Perceptions Regarding Water and Sanitation
| VINTON | |||||
| Water Source | N | Mean | Minimum | Maximum | |
| El Paso Water Utilities 1 | 22 | $58.88 | $13 | $300 | |
| Local Wells/Private Providers 2 | 77 | $32.94 | $12 | $100 | |
| Vinton Hills Subdivision | 38 | $33.39 | $12 | $86 | |
| Vinton Village Estates | 22 | $27.21 | $12 | $62 | |
| Villa Alegre Estates | 5 | $28.40 | $17 | $40 | |
| Hillside Water Works | 12 | $43.92 | $20 | $100 | |
| All Purchased Piped Water 3 | 99 | $38.71 | $12 | $300 | |
| Bottled Water 4 | 103 | $22.52 | $2 | $100 | |
| Total 5 | 115 | $53.12 | $4 | $324 | |
| WESTWAY | |||||
| Water Source | N | Mean | Minimum | Maximum | |
| El Paso Water Utilities 6 | 46 | $71.11 | $35 | $175 | |
| Estimated Sewage 7 | 46 | $21.33 | $10 | $52 | |
| Estimated Water Only 8 | 46 | $49.78 | $25 | $123 | |
| Bottled Water 9 | 41 | $18.56 | $1 | $75 | |
| Total 10 | 46 | $66.32 | $25 | $145 | |
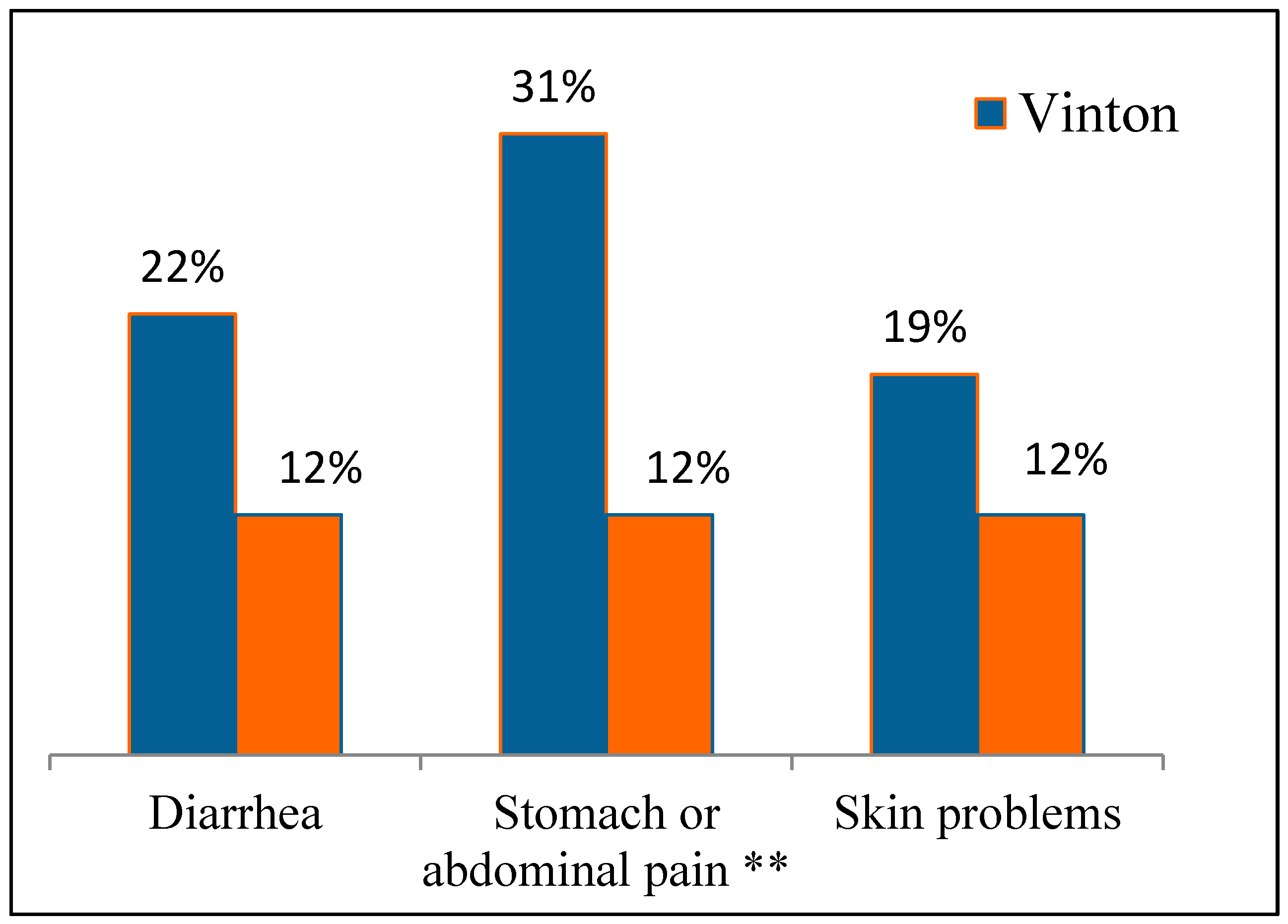
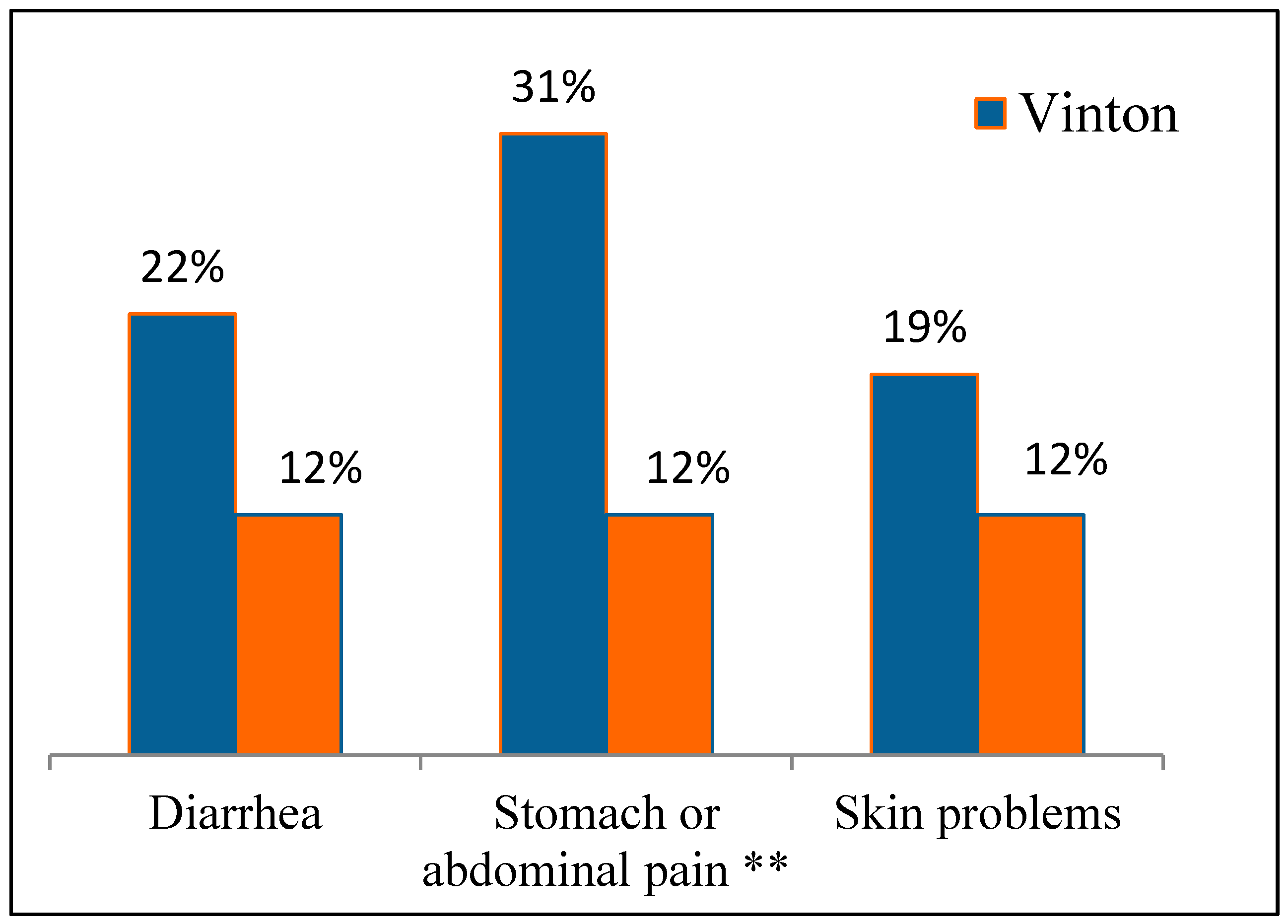
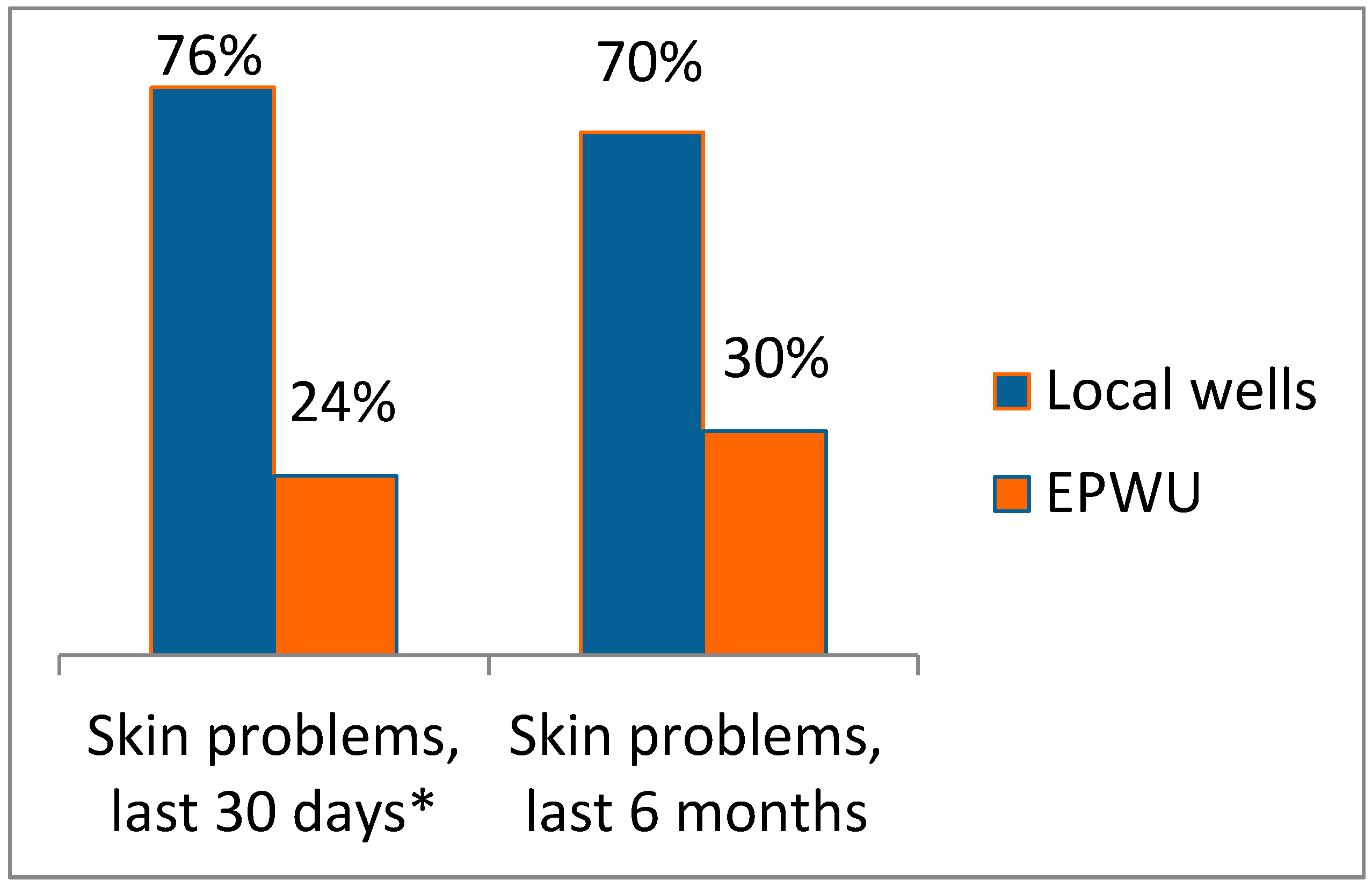
3.3.2. Public Health Condition: Self-Reported Illnesses

3.4. Discussion of Contaminants in Water, Health Outcomes, and Relative Risks in Vinton
3.4.1. Arsenic in Drinking Water
3.4.2. Total Dissolved Solids in Water
3.4.3. Bacteria and Other Biological Contaminants
- Campylobacteriosis—716 cases/100,000 people
- Salmonellosis—14.5 cases/100,000 people
- E. coli—0.24 cases/100,000 people
3.4.4. Relative Risks
3.5. Other Findings: Results from Focus Groups and Interviews
3.6. Summary of Existing Conditions, Impacts, Recommendations, and Outcomes
| Existing Condition | Impacts |
|---|---|
| Poor water quality: As, TDS, Coliform Bacteria | Gastrointestinal ailments Skin problems |
| Reliance on bottled water for drinking | High cost of drinking water |
| Poor septic tank management | Risk of overflows leading to: Exposure/gastrointestinal ailments Odors Contamination of groundwater |
| Inadequate fire hydrants | High cost of fire insurance Inability to fight fires |
| Lack of local health clinics | Lack of local access to health care, especially preventative care |
| Lack of water availability at local parks | Lack of drinking water fountains and shade lead to less use |
| Prolonged drought | Unreliability of water supply; periods of no service |
| Lack of retail businesses | Lack of economic vitality Poor job opportunities locally |
- Connect to EPWU for water and sanitation; this should lead to improved public health, economic development, and improved quality of life in the community.
- Seek financial assistance for the project from government agencies, including not only assistance for the basic infrastructure but also assistance for individual households to meet the costs of connection; this should lead to reducing the financial burden on the residents, especially those who are disadvantaged by low income and limited resources.
- Install the appropriate number of functioning water hydrants; this should lower the cost of fire insurance and improve public safety.
- Develop a strategic plan for economic and community development; this should improve economic opportunity and overall vitality of the community.
- Develop and implement educational campaigns to educate residents, politicians and decision makers, and youth of the benefits of improving water quality and sanitation in terms of public health; this should improve political and overall community support for the proposed infrastructure projects.
- Develop and implement an educational campaign focused on water conservation measures that might help residents reduce water use, lessening their monthly fees, i.e., improved water efficient appliances, water efficient showerheads and toilets, and water-efficient landscaping; this should lessen the financial burden of higher monthly fees for water for many households.
3.7. General Observations and Lessons Learned from this HIA
3.7.1. Lack of Data
3.7.2. Culture and Language
3.7.3. Building Awareness, Education, Civic Engagement and Discourse
3.7.4. The Value of HIA to Informed Decision Making
3.7.5. Access to Water, Human Security and Resilience
3.7.6. University Participation
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Disclaimer
References
- Bhatia, R.; Katz, M. Estimation of health benefits from a local living wage ordinance. Am. J. Public Health 2001, 91, 1398–1402. [Google Scholar] [PubMed]
- Health Impact Project. The Rise of HIAs in the U.S. Pew Charitable Trusts, Washington, DC. 2013. Available online: http://www.pewhealth.org/reports-analysis/data-visualization/the-rise-of-hias-in-the-united-states-85899464695 (accessed on 18 February 2015).
- Harris-Roxas, B.; Viliani, F.; Bond, A.; Cave, B.; Divall, M.; Furu, P.; Harris, P.; Soeberg, M.; Wernham, A.; Winkler, M. Health impact assessment: The state of the art. Impact Assess. Proj. Apprais. 2012, 30, 43–52. [Google Scholar] [CrossRef]
- Rhodus, J.; Fulk, F.; Bradley, A.; O’Shea, S.; Roth, A. A review of Health Impact Assessments in the U.S.: Current State-of-Sicence, Best Practices, and Areas for Improvement; EPA/600/R-13/354; U.S. EPA: Washington, DC, USA, 2013.
- Lusk, M.; Staudt, K.; Moya, E. Social justice in the US-Mexico Border Region. In Social Justice in the U.S.-Mexico Border Region; Lusk, M., Staudt, K., Moya, E., Eds.; Springer: New York, NY, USA, 2012; pp. 3–38. [Google Scholar]
- US Environmental Protection Agency & Secretaria de Medio Ambiente y Recurso Naturales. US-Mexico Environmental Program: Border 2012. A Mid-Course Refinement (2008–2012). Available online: nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P1001x6U.TXT (accessed on 15 February 2015).
- United States-Mexico Border Health Commission (USMBHC). Healthy Border 2010. An. Agenda for Improving Health on the United States-Mexico Border. Available online: http://www.borderhealth.org/files/res_63.pdf (accessed on 18 February 2015).
- VanDerslice, J. Drinking water infrastructure and environmental disparities: Evidence and methodological considerations. Am. J. Public Health 2011, 101, S109–S114. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, L.; Kaufmann, R.B.; Kay, D.; Enanoria, W.; Haller, L.; Colford, J.M., Jr. Water, sanitation, and hygiene interventions to reduce diarrhea in less developed countries: A systematic review and meta-analysis. Lancet Infect. Dis. 2005, 5, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Gundry, S.; Wright, J.; Conroy, R. A systematic review of the health outcomes related to household water quality in developing countries. J. Water Health 2004, 2, 1–14. [Google Scholar] [PubMed]
- Sobsey, M.D.; Handzel, T.; Venczel, L. Chlorination and safe storage of household drinking water in developing countries to reduce waterborne disease. Water Sci. Technol. 2003, 47, 221–228. [Google Scholar] [PubMed]
- Neumann, L.E.; Moglia, M.; Cook, S.; Nguyen, M.N.; Sharma, A.K.; Nguyen, T.H.; Nguyen, B.V. Water use, sanitation, and health in a fragmented urban water system: Case study and household survey. Urban. Water J. 2014, 11, 198–210. [Google Scholar] [CrossRef]
- Korc, M.E.; Ford, P.B. Application of the water poverty index in border colonias of west Texas. Water Policy 2013, 15, 79–97. [Google Scholar] [CrossRef]
- Lee, E.; Wilson, C.; Lara-Valencia, F.; de la Parra, C.; Van Schoik, R.; Patron-Soberano, K.; Olson, E.; Selee, A. The State of Border Report: A Comprehensive Analysis of the U.S.-Mexico Border; Mexico Institute of the Woodrow Wilson International Center for Scholars: Washington, DC, USA, 2013. [Google Scholar]
- McDonald, Y.; Grineski, S. Disparities in access to residential plumbing: A binational comparison of environmental injustice in El Paso and Ciudad Juarez. Popul. Environ. 2012, 34, 194–216. [Google Scholar] [CrossRef]
- North American HIA Practice Standards Working Group (). Minimum Elements and Practice Standards for Health Impact Assessment; Version 2; Bastia, R., Branscomb, J., Farhang, L., Lee, M., Orenstein, M., Richardson, M., Eds.; North American HIA Practice Standards Working Group: Oakland, CA, USA, 2010. [Google Scholar]
- USEPA Region 8 Laboratory. Quick Guide to Drinking Water Sample Collection; USEPA Region 8 Laboratory: Golden, CO, USA, 2005; p. 20.
- Creed, J.T.; Brockhoff, C.A.; Martin, T.D. Determination of trace elements in waters and wastes by inductively coupled plasma-mass spectrometry, Method 200.8, Revision 5.4. In EPA Methods for Chemical Analysis of Water and Waste; EPA-6--/4-79-020; EPA: Washington, D.C., USA, 1994. [Google Scholar]
- USEPA. Total Dissolved Solids Dried at 180 °C, Method 2540C. In Standard Methods for the Examination of Water and Waste, 21st Ed. edUSEPA: Washington, D.C., USA, 2005. [Google Scholar]
- USEPA. Total Coliform bacteria and E. coli, Method 9223A,B. In Standard Methods for the Examination of Water and Waste, 21st Ed. edUSEPA: Washington, D.C., USA, 2005. [Google Scholar]
- USEPA. Method 1623: Cryptosporidium and Giardia in Water by Filtration/IMS/FA. Office of Water (4607), EPA 815-R-05-002. Available online: http://www.epa.gov/microbes/ (accessed on 15 February 2015).
- U.S. Census Bureau (USCB). 2008–2012 American Community Survey; USCB: Suitland, MA, USA, 2014.
- U.S. Census Bureau (USCB). American Community Survey 2006–2010; USCB: Suitland, MA, USA, 2014.
- WHO. Arsenic. Available online: http://www.who.int/mediacentre/factsheets/fs372/en/index.html# (accessed on Date December 2012).
- Bhattacharjee, P.; Chatterjee, D.; Singh, K.; Ak, G. Systems biology approaches to evaluate arsenic toxicity and carcinogenicity: An overview. Int. J. Hyg. Environ. Health 2013. [Google Scholar] [CrossRef]
- Valentine, J.; He, S.; Reisboro, L.; Pa, L. Health response by questionnaire in arsenic-exposed populations. J. Clin. Epidemiol. 1992, 45, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Yamauchi, H.; FanSun, G. Chronic health effects in people exposed to arsenic via the drinking water: Dose-response relationships in review. Toxicol. Appl. Pharmacol. 2004, 198, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Dutton, R.; Weldon, M.; Shannon, J.; Bowcock, C.; Tackett-Gibson, M.; Blakely, C.; Dyer, J.; Jayasuriya, B.; Worrall, W.; Betru, R. Survey of Health and Environmental Conditions in Texas Border Counties and Colonias. Executive Summary; Office of Border Health-Texas State Health Department: Austin, TX, USA, 2000.
- ATSDR. Toxicological Profile for Arsenic. CAS# 7440-38-2. Available online: http://www.atsdr.cdc.gov/ToxProfiles/TP.asp?id=22&tid=3 (accessed on 15 February 2015).
- Ramsey, K.; Foong, R.; Sly, P.; Larcombe, N.; Zosky, G. Early life arsenic exposure and acute and long-term responses to Influenza A infection in mice. Environ. Health Perspect. 2013, 121, 1187–1193. [Google Scholar] [PubMed]
- Wasserman, G.; Liu, X.; Lolacono, N.; Klilne, J.; Factor-Litvak, P.; va Green, A.; Mey, J.; Levy, D.; Abramson, R.; Schartz, A.; et al. A cross- sectional study of well water arsenic and child IQ in Main schoolchildren. Environ. Health 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- U.S. EPA. Factoids: Drinking Water and Ground Water Statistics for 2009. Office of Water (4601M). Available online: http://www.epa.gov/ogwdw/databases/pdfs/data_factoids_2009.pdf (accessed on Date Month 2009).
- World Health Organization. Total Dissolved Solids in Drinking-Water. Background Document for Development of Who Guidelines for Drinking-Water Quality; WHO/SDE/WSH/03.04/16; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- El Paso Department of Public Health. Available online: http://home.elpasotexas.gov/health/epidemiology.php (accessed on 12 September 2013).
- Escobedo, M.; Homedes, N.; Aldana, V.; vo Alt, K.; Serrano, B.; Garcia, R. Assessment of Parasitic Disease in Children in Five Communities in the Border Region of Far West Texas; Texas Department of Health Office of Border Health: El Paso, TX, USA, 2003.
- Cardenas, V.; Mena, K.; Ortiz, M.; Karri, S.; Behravesh, V.E.C.; Snowden, K.; Flisser, A.; Bristol, J.; Mayberry, L.; Ortega, Y.; et al. Hyperendemic H. pylori and tapeworm infetions in a U.S.-Mexico border population. Public Health Rep. 2010, 125, 441–447. [Google Scholar] [PubMed]
- Redlinger, T.; O’Rourke, K.; VanDerslice, J. Hepatitis A among schoolchildren in a U.S.-Mexico border community. Am. J. Public Health 1997, 87, 1715–1717. [Google Scholar] [CrossRef] [PubMed]
- Hennekens, C.; Buring, J. Epidemiology in Medicine; Mayrent, S., Ed.; Little, Brown and Company: Boston, MA, USA; Toronto, Canada, 1987. [Google Scholar]
- USGS. Groundwater Monitoring Network. Available online: http://groundwaterwatch.usgs.gov/AWLSites.asp?S=315712106361201 (accessed on 15 February 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hargrove, W.L.; Juárez-Carillo, P.M.; Korc, M. Healthy Vinton: A Health Impact Assessment Focused on Water and Sanitation in a Small Rural Town on the U.S.-Mexico Border . Int. J. Environ. Res. Public Health 2015, 12, 3864-3888. https://doi.org/10.3390/ijerph120403864
Hargrove WL, Juárez-Carillo PM, Korc M. Healthy Vinton: A Health Impact Assessment Focused on Water and Sanitation in a Small Rural Town on the U.S.-Mexico Border . International Journal of Environmental Research and Public Health. 2015; 12(4):3864-3888. https://doi.org/10.3390/ijerph120403864
Chicago/Turabian StyleHargrove, William L., Patricia M. Juárez-Carillo, and Marcelo Korc. 2015. "Healthy Vinton: A Health Impact Assessment Focused on Water and Sanitation in a Small Rural Town on the U.S.-Mexico Border " International Journal of Environmental Research and Public Health 12, no. 4: 3864-3888. https://doi.org/10.3390/ijerph120403864
APA StyleHargrove, W. L., Juárez-Carillo, P. M., & Korc, M. (2015). Healthy Vinton: A Health Impact Assessment Focused on Water and Sanitation in a Small Rural Town on the U.S.-Mexico Border . International Journal of Environmental Research and Public Health, 12(4), 3864-3888. https://doi.org/10.3390/ijerph120403864