
South African Foundation Phase Teachers’ Perceptions of ADHD at Private and Public Schools

Abstract
:1. Introduction
- ▪
- Medical Interventions which are central nervous system stimulants.
- ▪
- Behavioural Interventions, and
- ▪
- Academic Interventions.
2. Experimental Section
2.1. Context of the Study
2.2. Research Design
2.2.1. Sampling Procedures
2.2.2. Participants
2.2.3. Testing and Intervention Procedure
2.2.4. Data Analysis
2.3. Instrumentation
3. Results and Discussion
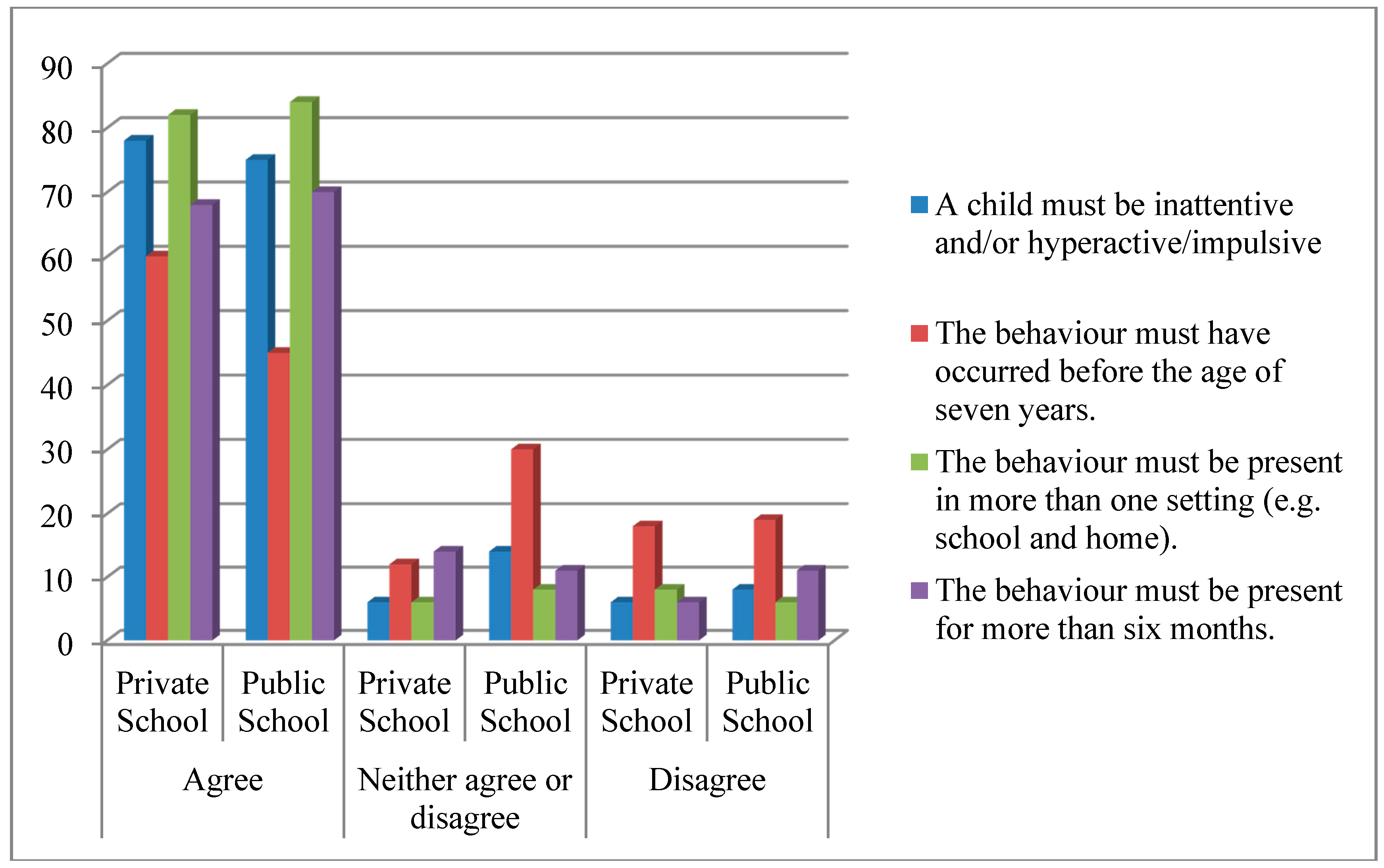
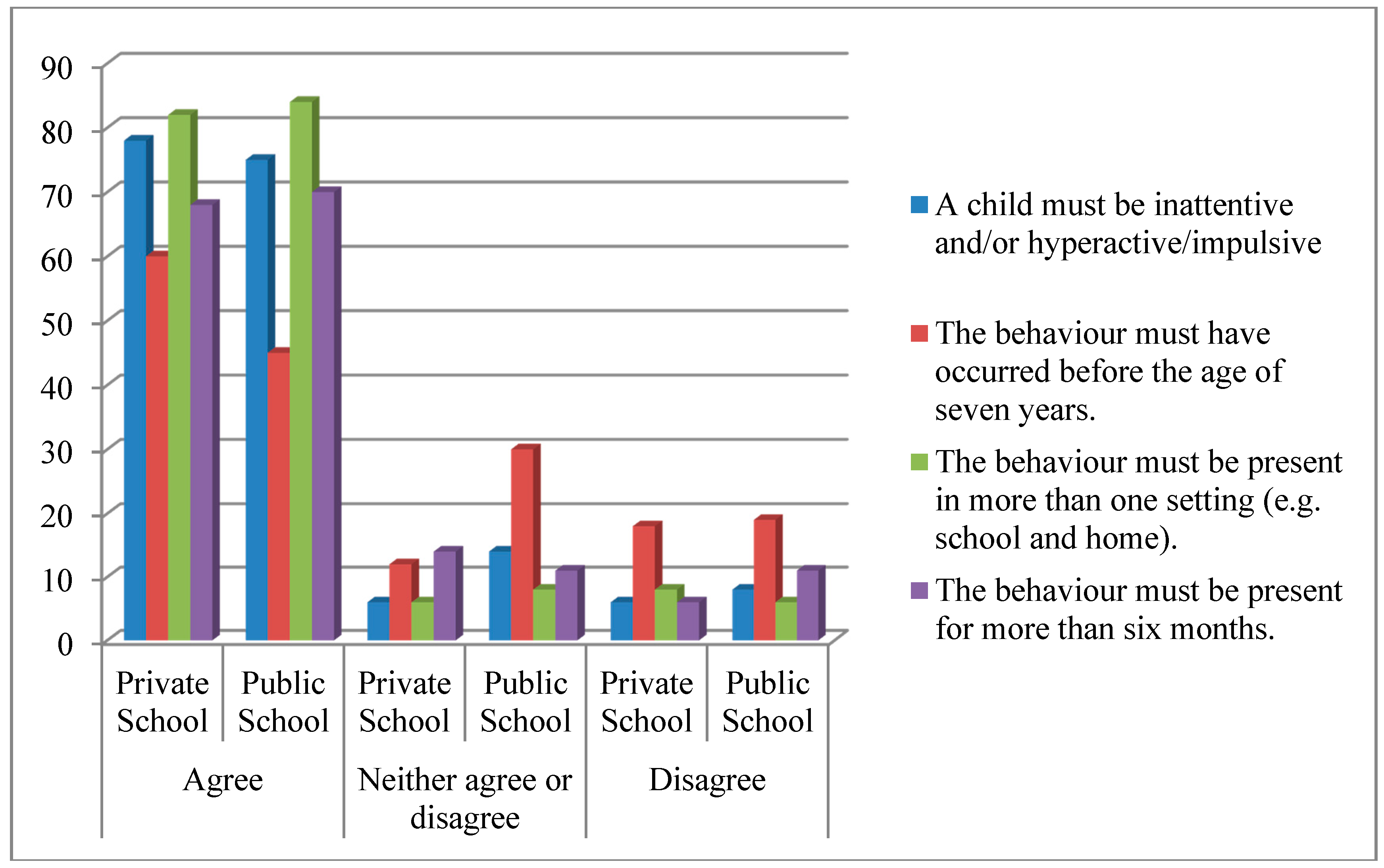
3.1. Understanding of ADHD
3.2. Incidence and Ratios
3.3. Perceived Causes of ADHD

{kind=link}
{kind=link}
| Causes | Private School Educators | Public School Educators | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Agree | Neither Agree nor Disagree | Disagree | Agree | Neither Agree nor Disagree | Disagree | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Physiological | 28 | 56 | 10 | 20 | 5 | 10 | 45 | 56 | 19 | 24 | 6 | 8 |
| Emotional | 13 | 26 | 13 | 26 | 17 | 34 | 26 | 33 | 25 | 31 | 18 | 23 |
| Diet | 38 | 76 | 4 | 8 | 6 | 12 | 56 | 70 | 7 | 8 | 9 | 11 |
| Parenting | 24 | 48 | 10 | 20 | 12 | 24 | 31 | 39 | 17 | 21 | 18 | 23 |
| Other barriers to learning | 26 | 52 | 7 | 14 | 13 | 26 | 46 | 55 | 16 | 20 | 11 | 14 |
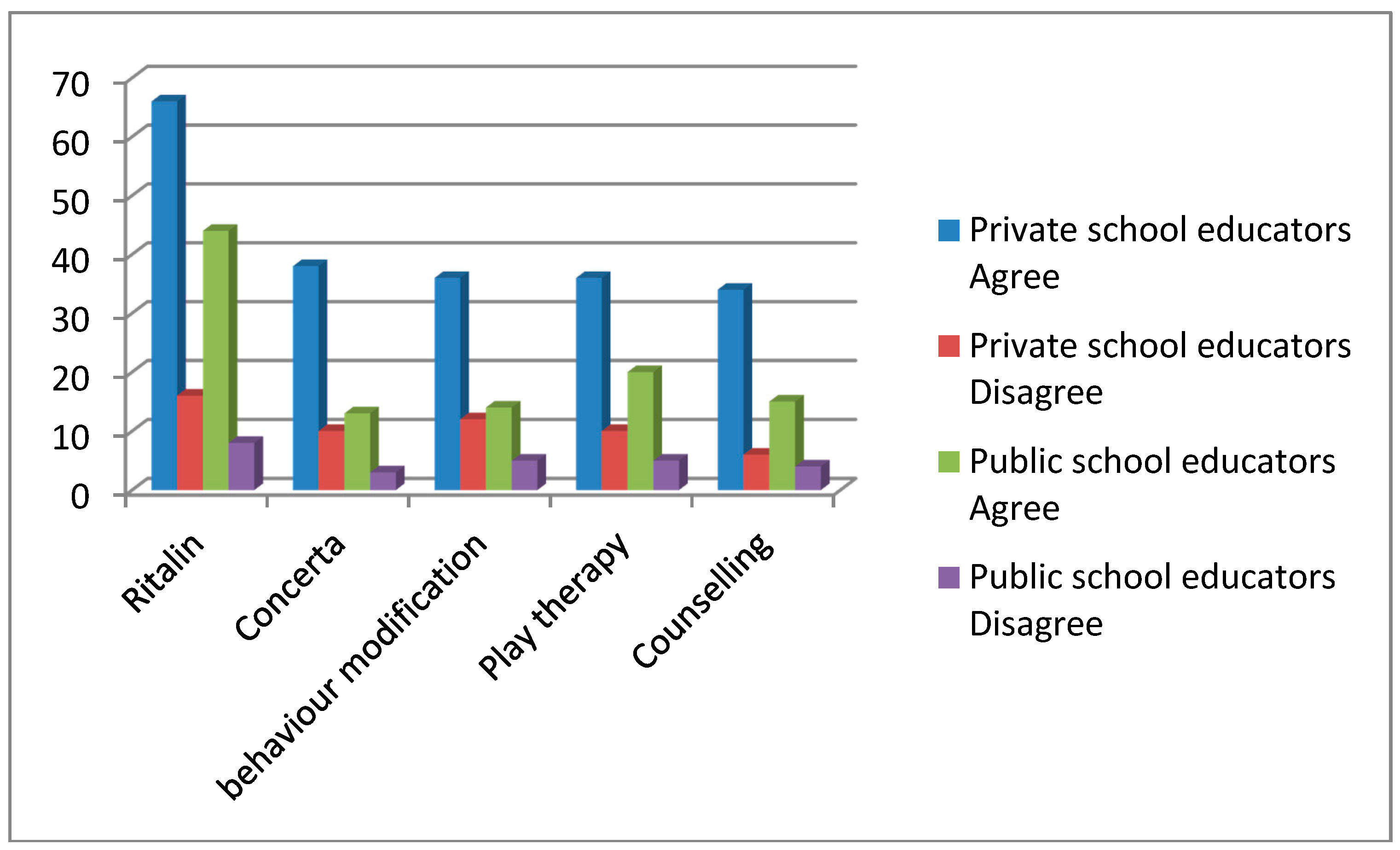
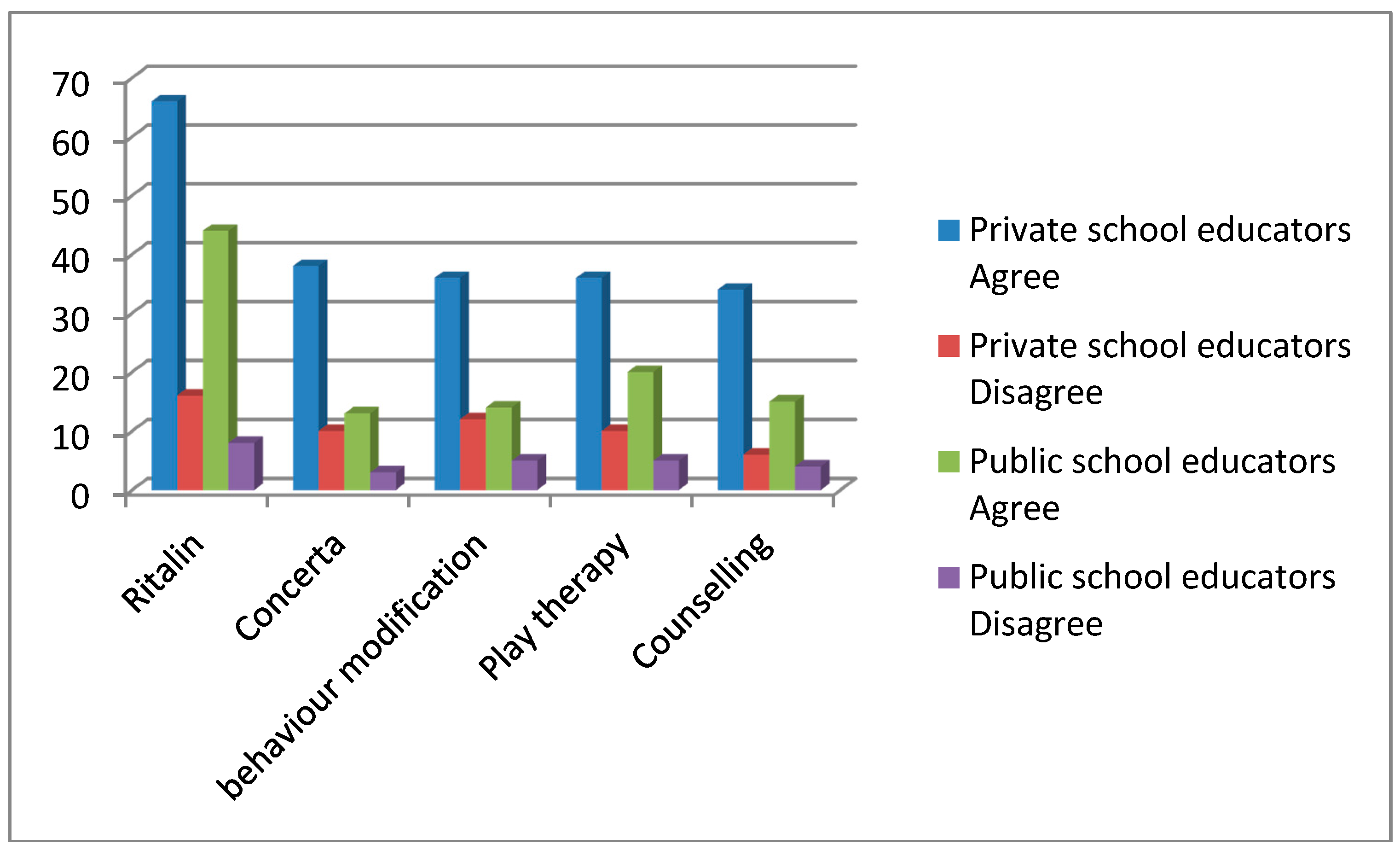
3.4. Interventions for ADHD
| Treatment Modalities | Agree | Disagree | ||
|---|---|---|---|---|
| n | % | n | % | |
| Ritalin | 68 | 52 | 14 | 11 |
| Concerta | 29 | 22 | 7 | 5 |
| Behaviour modification | 29 | 22 | 10 | 8 |
| Play Therapy | 34 | 26 | 9 | 7 |
| Counselling | 29 | 22 | 6 | 5 |
3.5. Limitations of the Study and Implications of the Findings
3.6. Implications for Future Research
4. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Glass, C.S.; Wegar, K. Teacher perceptions of the incidence and management of Attention Deficit Hyperactivity Disorder. Education 2000, 121, 412–420. [Google Scholar]
- McCarthy, S.; Wilton, L.; Murray, M.L.; Hodgkins, P.; Asherson, P.; Wong, I.C. The epidemiology of pharmacologically treated attention deficit hyperactivity disorder (ADHD) in children, adolescents and adults in UK primary care. BMC Pediatr. 2012, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, A. Cross-cultural issues in ADHD research. J. Psychol. Afr. 2005, 10, 101–106. [Google Scholar]
- Amod, A.; Vorster, A.; Lazarus, K. Attention-Deficit/Hyperactivity Disorder (ADHD) as a barrier to learning & development within the South African context: The perspective of teachers. In Attention Deficit Hyperactivity Disorder in Children and Adolescents; Banerjee, S., Ed.; Intech Publishers: Rijeka, Croatia, 2013. [Google Scholar]
- Perold, M.; Louw, C.; Kleynhans, S. Primary school teachers’ knowledge and misperceptions of attention deficit hyperactivity disorder (ADHD). S. Afr. J. Educ. 2010, 30, 457–473. [Google Scholar]
- Curtis, D.F.; Pisecco, S.; Hamilton, R.J.; Moore, D.W. Teacher perceptions of classroom interventions for children with ADHD: A cross-cultural comparison of teachers in the United States and New Zealand. Sch. Psychol. Q. 2006, 21, 171–197. [Google Scholar] [CrossRef]
- Demaray, M.K.; Schaefer, K.; Delong, L. Attention-deficit/hyperactivity disorder (ADHD): A national survey of training and current assessment practices in the schools. Psychol. Sch. 2003, 40, 583–596. [Google Scholar] [CrossRef]
- Polanczyk, G.; Rohde, L. Epidemiology of attention-deficit/hyperactivity disorder across the lifespan. Curr. Opin. Psychiatr. 2007, 20, 386–392. [Google Scholar] [CrossRef]
- Raman, N.; van Rensburg, A.J. Clinical and psychosocial profile of child and adolescent mental health care users and services at an urban child mental health clinic in South Africa. Afr. J. Psychiatr. 2013, 16, 356–363. [Google Scholar]
- Akram, G.; Thomson, A.; Boyter, A.; McLarty, M. ADHD and the role of medication: Knowledge and perceptions of qualified and student teachers. Eur. J. Spec. Needs Educ. 2009, 24, 423–436. [Google Scholar] [CrossRef]
- Kos, J.; Richdale, A.; Jackson, M. Knowledge about Attention Deficit/Hyperactivity Disorder: A comparison of in-service and preservice teachers. Psychol. Sch. 2004, 41, 517–526. [Google Scholar] [CrossRef]
- Goldstein, L.F. Special education: Views on ADHD. Educ. Week 2002, 22, 6. [Google Scholar]
- Havey, J.; Olsen, J.; McCormick, C. Teachers’ perceptions of the incidence and management of attention deficit hyperactivity disorder. Appl. Neuropsychol. 2005, 12, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Kern, A.; Seabi, J. Educators’ perceptions of Attention Deficit Hyperactivity Disorder: An exploratory study. J. Psychol. Afr. 2008, 18, 641–644. [Google Scholar]
- Moldavsky, M.; Sayal, K. Knowledge and Attitudes about Attention-deficit/hyperactivity disorder (ADHD) and its treatment: The views of children, adolescents, parents, teachers and healthcare professionals. Curr. Psychiat. Rep. 2013, 15. [Google Scholar] [CrossRef]
- Holz, T.; Lessing, A. Aid to the teacher to identify the learner with ADHD in the classroom: A literature study. Educare 2002, 31, 236–249. [Google Scholar]
- Education White Paper 6: Special Needs Education: Building an Inclusive Education and Training System; Department of Education: Pretoria, South Africa, 2001.
- Mulholland, S.; Cumming, T.; Jung, J. Teacher attitudes towards students who exhibit ADHD-type behaviours. Australas. J. Spec. Educ. 2015. [Google Scholar] [CrossRef]
- Sciutto, M.; Terjesen, M.; Frank, A. Teachers’ knowledge and misperceptions of Attention Deficit/Hyperactivity Disorder. Psychol. Sch. 2000, 37, 115–122. [Google Scholar] [CrossRef]
- American Psychiatric Association. Neurodevelopmental disorders. In Diagnostic and Statistical Manual of Mental Disorders (DSM-V), 5th ed.; American Psychiatric Publishing (APPI): Washington, DC, USA, 2013. [Google Scholar]
- Guerra, F.; Brown, M. Teacher knowledge of attention deficit hyperactivity disorder amongst middle school students in South Texas. Res. Middle Level Educ. Online 2012, 36, 1–6. [Google Scholar]
- Fuermaier, A.; Tucha, L.; Koerts, J.; Mueller, A.; Lange, K.; Tucha, O. Measurement of Stigmatization towards adults with Attention Deficit Hyperactivity Disorder. PLoS One 2012, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moldavsky, M.; Pass, S.; Sayal, K. Primary school teachers’ attitudes about children with attention deficit/hyperactivity disorder and the role of pharmacological treatment. Clin. Child Psychol. Psychiatr. 2014, 19, 202–216. [Google Scholar] [CrossRef]
- Mowbray, C. Time to pay attention. Jr. Educ. 2003, 27, 12–13. [Google Scholar]
- Faraone, S.V. The scientific foundation for understanding attention-deficit/hyperactivity disorder as a valid psychiatric disorder. Eur. Child Adolesc. Psychiatr. 2005, 14, 1–10. [Google Scholar] [CrossRef]
- Sadock, B.J.; Sadock, V.A. Kaplan and Sadock’s Synopsis of Psychiatry. Behavioural Sciences/Clinical Psychiatry, 10th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Halasz, G.; Vance, A. Attention Deficit Hyperactivity Disorder in children: Moving forward with divergent perspectives. Med. J. Aust. 2002, 177, 554–557. [Google Scholar] [PubMed]
- Vorster, A. Developmental psychopathology. In Abnormal Psychology: A South African Perspective, 2nd ed.; Burke, A., Ed.; Oxford University Press: Cape Town, South Africa, 2012; pp. 512–559. [Google Scholar]
- Nel, N.; Nel, M.; Hugo, A. Learner Support in a Diverse Classroom: A Guide for Foundation, Intermediate and Senior Phase Teachers of Language and Mathematics; Van Schaik Publishers: Pretoria, South Africa, 2012. [Google Scholar]
- Storbeck, C. Educating the deaf and hard of hearing learner. In Addressing Barriers to Learning. A South African Perspective; Landsberg, E., Ed.; Van Schaik Publishers: Pretoria, South Africa, 2005. [Google Scholar]
- McGee, R.; Brodeur, D.; Symons, D.; Andrade, B.; Fahie, C. Time perception: Does it distinguish ADHD and RD children in a clinical sample? J. Abnormal Child Psychol. 2004, 32, 481–490. [Google Scholar] [CrossRef]
- Stanley, I.; Greenspan, M.D. Understanding attention problems. Scholast. Parent Child 2006, 13, 46–48. [Google Scholar]
- Kantrowitz, B.; Springen, K. Why sleep matters. Newsweek, 2003; 142, 75–77. [Google Scholar] [PubMed]
- Foley, M.; McClowry, S.; Castellanos, F. The relationship between attention deficit hyperactivity disorder and child temperament. J. Appl. Dev. Psychol. 2008, 29, 157–169. [Google Scholar] [CrossRef]
- Attention Deficit/Hyperactivity Disorder Fact Sheet 19. 2004. Available online: http://www.nichcy.org/pubs/factshe/fs19txt.htm (accessed on 27 June 2006).
- DuPaul, G.; White, G. ADHD: Behavioural, educational, and medication interventions. Educ. Dig. 2006, 71, 57–60. [Google Scholar]
- Miller-Horn, J.; Kaleyias, J.; Valencia, I.; Melvin, J.; Khurana, D.S.; Hardison, H.H.; Marks, H.; Legido, A.; Kothare, S.V. Efficacy and tolerability of ADHD medications in a clinical practice. J. Pediatr. Neurol. 2008, 6, 5–10. [Google Scholar]
- O’Neill, M. Attention Deficit/Hyperactivity Disorder: A Closer Look. Master’s Thesis, Graduate College of Wisconsin-Stout, Wisconsin, DC, USA, 1999. [Google Scholar]
- Newcorn, J.; Kratochvil, C.; Allen, A.; Casat, C.; Ruff, D.D.; Moore, R.J.; Michelson, D.; Atomoxetine/Methylphenidate Comparative Study Group. Atomoxetine and osmotically released methylphenidate for the treatment of attention deficit hyperactivity disorder: Acute comparison and differential response. Am. J. Psychiatr. 2008, 165, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Grandy, S.E.; McLaughlin, T.F. School Interventions for students with Attention Deficit Hyperactivity Disorder: Some implications for school personnel. Int. J. Spec. Educ. 1999, 14, 59–70. [Google Scholar]
- Evans, S.; Schultz, B.; Sadler, J. Psychosocial interventions used to treat children with ADHD: Safety and efficacy. J. Psychosoc. Nurs. 2008, 46, 49–57. [Google Scholar]
- Swart, E.; Pettipher, R. A framework for understanding inclusion. In Addressing Barriers to Learning. A South African Perspective; Landsberg, E., Ed.; Van Schaik Publishers: Pretoria, South Africa, 2005. [Google Scholar]
- Van Rooyen, B.; Le Grange, L.; Newmark, R. (De)Construction of functionalist discourses in South Africa’s education White Paper 6: Special needs education. Int. J. Spec. Educ. 2002, 17, 1–12. [Google Scholar]
- Rosnow, R.; Rosenthal, R. Beginning Behavioural Research. A Conceptual Primer, 2nd ed.; Prentice-Hall Inc.: Upper Saddle River, NJ, USA, 1996. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Mayring, P. Qualitative Content Analysis. Available online: http://www.utsc.utoronto.ca/~kmacd/IDSC10/Readings/Readings/text%20analysis/CA.pdf (accessed on 6 March 2015).
- Terre Blanche, M.; Durrheim, K. Research in Practice: Applied Methods for the Social Sciences; University of Cape Town Press: Cape Town, South Africa, 1999. [Google Scholar]
- Fabiano, W.; Pelham, W.; Majumdar, A.; Evans, S.; Manos, M.; Caserta, D.; Girio-Herrera, E.; Pisecco, S.; Hannah, J.; Carter, R. Elementary and middle school teacher perceptions of attention-deficit hyperactivity disorder prevalence. Child Youth Care Forum 2013, 42, 87–99. [Google Scholar] [CrossRef]
- Hallowell, E.M.; Ratey, J.J. Driven to Distraction: Recognizing and Coping with Attention Deficit Disorder from Childhood through Adulthood; Touchstone: New York, NY, USA, 1994. [Google Scholar]
- Tamhne, R. 5 Ages of mental health behavioural problems in children. Update 2004, 68, 459–465. [Google Scholar]
- Calhoun, G.; Greenwell-Iorillo, E.; Chung, S. Attention deficit disorder: Mountain or a mote hill? Education 1997, 118, 244–252. [Google Scholar]
- Abelman, D. Parent and Teacher Perceptions of Children with Learning Difficulties: A survey of Selected Primary Schools in the Northern Suburbs of Johannesburg. Unpublished Master’s Thesis, Department of Psychology, University of the Witwatersrand, Gauteng, South Africa, 2001. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kern, A.; Amod, Z.; Seabi, J.; Vorster, A. South African Foundation Phase Teachers’ Perceptions of ADHD at Private and Public Schools. Int. J. Environ. Res. Public Health 2015, 12, 3042-3059. https://doi.org/10.3390/ijerph120303042
Kern A, Amod Z, Seabi J, Vorster A. South African Foundation Phase Teachers’ Perceptions of ADHD at Private and Public Schools. International Journal of Environmental Research and Public Health. 2015; 12(3):3042-3059. https://doi.org/10.3390/ijerph120303042
Chicago/Turabian StyleKern, Anwynne, Zaytoon Amod, Joseph Seabi, and Adri Vorster. 2015. "South African Foundation Phase Teachers’ Perceptions of ADHD at Private and Public Schools" International Journal of Environmental Research and Public Health 12, no. 3: 3042-3059. https://doi.org/10.3390/ijerph120303042