
Towards Effective and Socio-Culturally Appropriate Sanitation and Hygiene Interventions in the Philippines: A Mixed Method Approach

Abstract
:1. Introduction
2. Methods
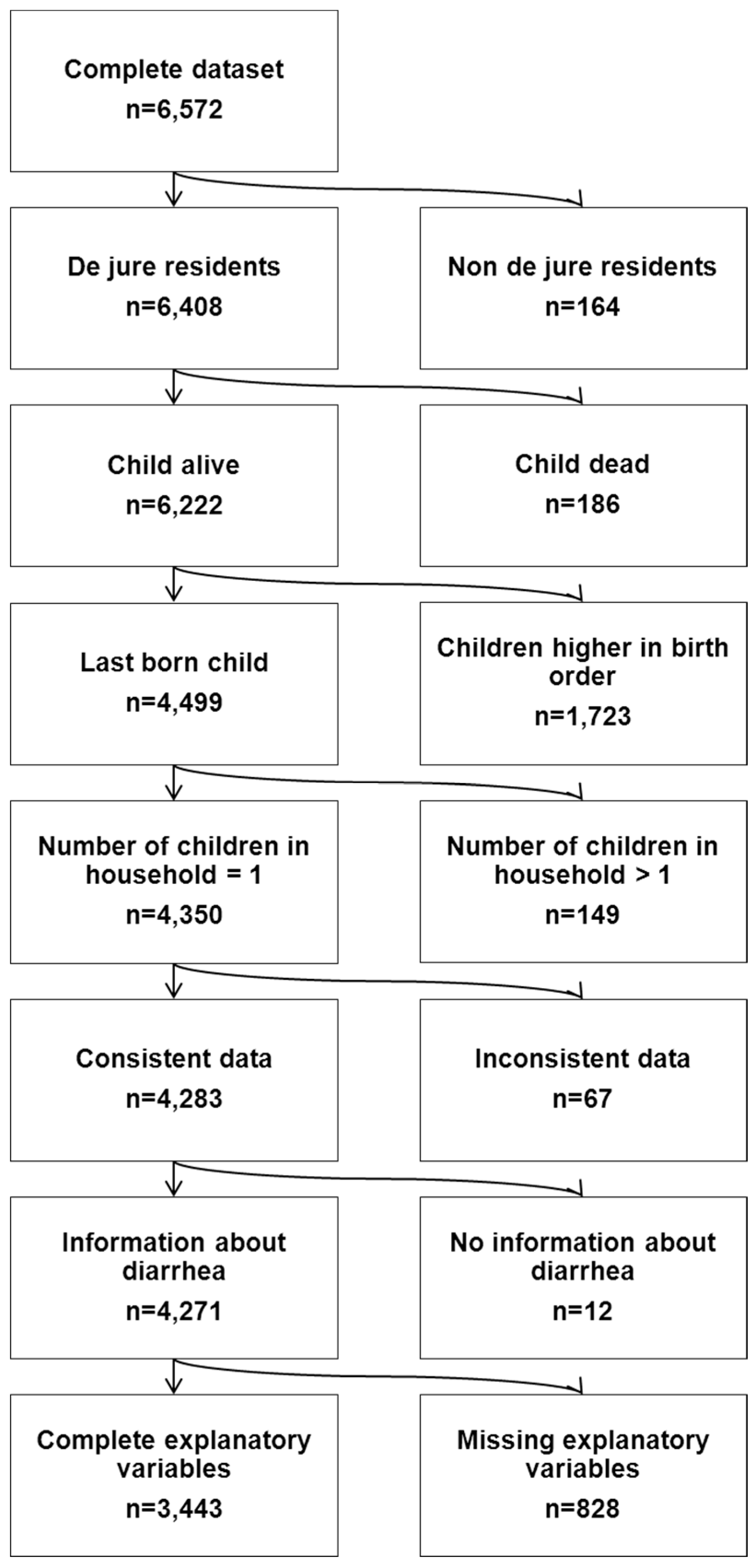
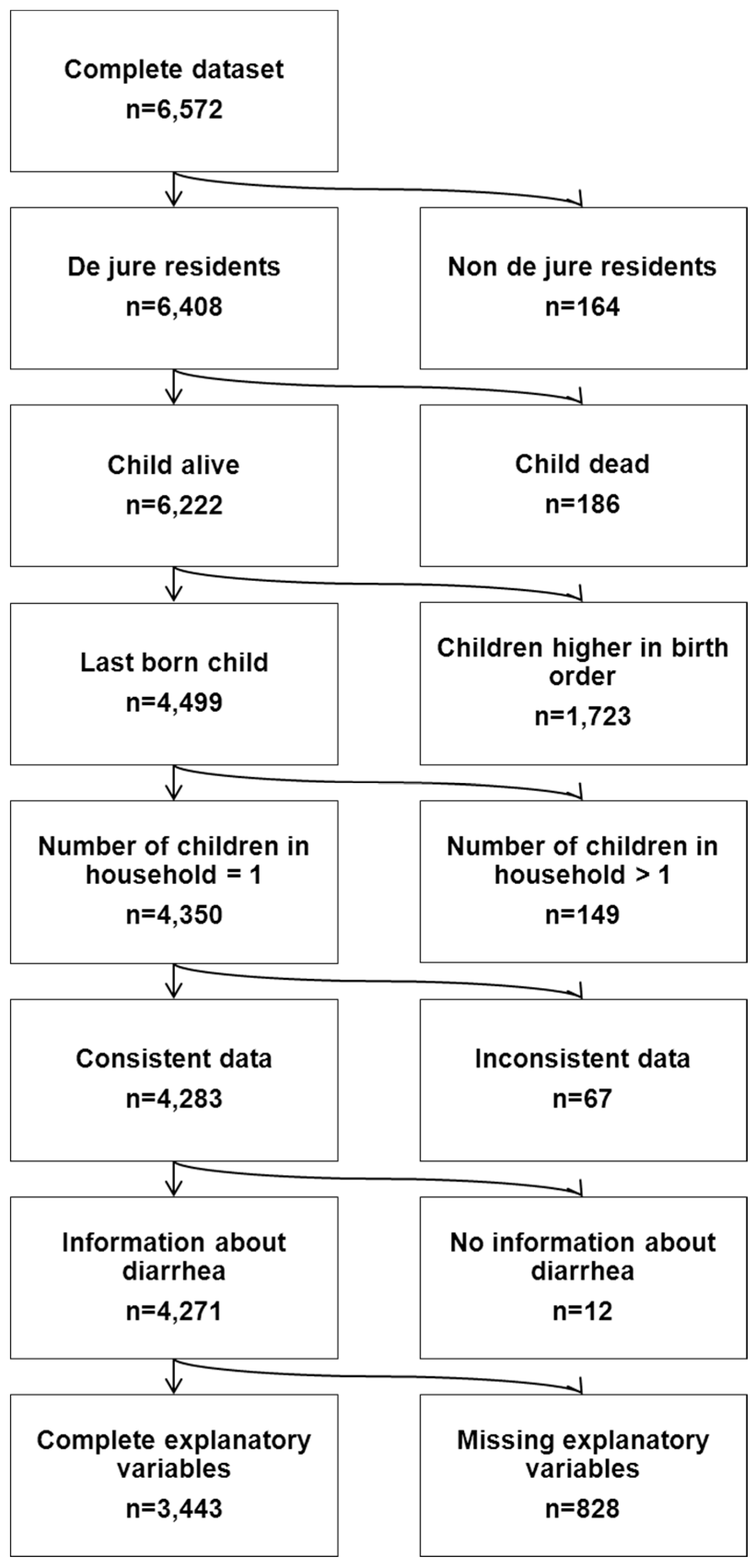
2.1. Quantitative Methods

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factor | No Diarrhea (N = 3091, 89.78) | Diarrhea (N = 352, 10.22) | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Water, Sanitation and Hygiene (WASH) | |||||
| Sanitation | Improved | 1888 | 61.08 | 193 | 54.83 |
| Improved, shared | 732 | 23.68 | 76 | 21.59 | |
| Unimproved | 137 | 4.43 | 29 | 8.24 | |
| Open defecation | 334 | 10.81 | 54 | 15.34 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Disposal of Children’s Stool | Sanitary | 1758 | 56.87 | 159 | 45.17 |
| Unsanitary | 1333 | 43.13 | 193 | 54.83 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Water Source | Piped | 842 | 27.24 | 80 | 22.73 |
| Improved | 1371 | 44.35 | 183 | 51.99 | |
| Unimproved | 863 | 27.92 | 87 | 24.72 | |
| Surface | 15 | 0.49 | 2 | 0.57 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Distance to Water Source | On premises or delivered | 2096 | 67.81 | 212 | 60.23 |
| <5 Min | 521 | 16.86 | 65 | 18.47 | |
| ≥5 Min | 474 | 15.33 | 75 | 21.31 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Non-Modifiable Characteristics | |||||
| Child Age (months) | Mean: 27.43; Median: 25.00, SD: 16.02; Range: 1.00–59.00 | Mean: 20.91; Median: 18.00; SD: 11.87; Range: 2.00–58.00 | |||
| Child Sex | Female | 1460 | 47.23 | 159 | 45.17 |
| Male | 1631 | 52.77 | 193 | 54.83 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Twin | Single birth | 3062 | 99.06 | 351 | 99.72 |
| Multiple birth | 29 | 0.94 | 1 | 0.28 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Region | Ilocos Region | 157 | 5.08 | 17 | 4.83 |
| Central Luzon | 136 | 4.40 | 12 | 3.41 | |
| Bicol Region | 243 | 7.86 | 30 | 8.52 | |
| Western Visayas | 199 | 6.44 | 13 | 3.69 | |
| Central Visayas | 199 | 6.44 | 35 | 9.94 | |
| Eastern Visayas | 203 | 6.57 | 22 | 6.25 | |
| Zamboanga Peninsula | 156 | 5.05 | 20 | 5.68 | |
| Northern Mindanao | 151 | 4.89 | 20 | 5.68 | |
| Davao Peninsula | 154 | 4.98 | 9 | 2.56 | |
| SOCCSKSARGEN | 174 | 5.63 | 10 | 2.84 | |
| Caraga | 139 | 4.50 | 33 | 9.38 | |
| National Capital Region | 171 | 5.53 | 20 | 5.68 | |
| Cordillera Admin Region | 328 | 10.61 | 34 | 9.66 | |
| ARMM | 134 | 4.34 | 10 | 2.84 | |
| CALABARZON | 105 | 3.40 | 21 | 5.97 | |
| MIMAROPA | 299 | 9.67 | 27 | 7.67 | |
| Total | 143 | 4.63 | 19 | 5.40 | |
| Residence | Urban | 1365 | 44.16 | 147 | 41.76 |
| Rural | 1726 | 55.84 | 205 | 58.24 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Susceptibility | |||||
| Breastfeeding Status | Never breastfed | 290 | 9.38 | 28 | 7.95 |
| Ever breastfed | 2801 | 90.62 | 324 | 92.05 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Vitamin A Supplementation (past 6 months) | No | 520 | 16.82 | 54 | 15.34 |
| Yes | 2571 | 83.18 | 298 | 84.66 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Iron Supplementation | No | 1869 | 60.47 | 223 | 63.35 |
| Yes | 1222 | 39.53 | 129 | 36.65 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Intestinal Parasite Medication (past 6 months) | No | 1975 | 63.90 | 247 | 70.17 |
| Yes | 1116 | 36.10 | 105 | 29.83 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Vaccination Index (cumulative recommended vaccine shots against BCG (1), DPT(3), polio(3) and measles (1)) | Low (0–2) | 148 | 4.79 | 18 | 5.11 |
| Intermediate (3–5) | 256 | 8.28 | 37 | 10.51 | |
| High (6–8) | 2687 | 86.93 | 297 | 84.38 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Socioeconomic Characteristics | |||||
| Maternal Age (years) | Mean: 30.53; Median: 30.00; SD: 6.84; Range: 15.00–49.00 | Mean: 29.41; Median: 29.00; SD: 6.62; Range: 16.00–49.00 | |||
| Maternal Education | None or primary | 724 | 23.42 | 109 | 30.97 |
| Secondary | 1463 | 47.33 | 165 | 46.88 | |
| Higher | 904 | 29.25 | 78 | 22.16 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Maternal Working Status | Not working | 1711 | 55.35 | 204 | 57.95 |
| Working | 1380 | 44.65 | 148 | 42.05 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Household Wealth Index (composite measure based on asset ownership; households are grouped in quintiles) | Poorest | 788 | 25.49 | 118 | 33.52 |
| Poorer | 707 | 22.87 | 96 | 27.27 | |
| Middle | 616 | 19.93 | 62 | 17.61 | |
| Richer | 569 | 18.41 | 43 | 12.22 | |
| Richest | 411 | 13.30 | 33 | 9.38 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Religion | Roman Catholic | 2407 | 77.87 | 265 | 75.28 |
| Protestant | 154 | 4.98 | 25 | 7.10 | |
| Islam | 159 | 5.14 | 16 | 4.55 | |
| Other | 371 | 12.00 | 46 | 13.07 | |
| Total | 3091 | 100.00 | 352 | 100.00 | |
| Number of household members | Mean: 5.96; Median: 6.00; SD: 2.20; Range: 2.00–19.00 | Mean: 6.02; Median: 6.00; SD: 2.43; Range: 2.00–18.00 | |||
| Number of under five children in household | Mean: 1.55; Median: 1.00; SD: 0.71; Range: 1.00–7.00 | Mean: 1.65; Median: 2.00; SD: 0.76; Range: 1.00–6.00 | |||
2.2. Qualitative Methods
2.3. Integration of Findings
2.4. Ethic Statement
3. Results
3.1. Quantitative Component
| Risk Factor | Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | OR (95% CI) | p Value * | OR | OR (95% CI) | p Value * | OR | OR (95% CI) | p Value * | OR | OR (95% CI) | p Value * | |||||||||
| WASH | ||||||||||||||||||||
| Sanitation | Improved | 1.00 | -- | -- | 0.04 | 1.00 | -- | -- | 0.03 | -- | -- | 0.02 | -- | -- | 0.11 | |||||
| Improved, shared | 0.95 | 0.72 | 1.26 | 0.73 | 0.97 | 0.73 | 1.29 | 0.83 | 0.97 | 0.72 | 1.29 | 0.83 | 0.86 | 0.63 | 1.16 | 0.32 | ||||
| Unimproved | 1.77 | 1.14 | 2.76 | 0.01 | 1.98 | 1.23 | 3.18 | 0.00 | 2.01 | 1.24 | 3.24 | 0.00 | 1.63 | 0.99 | 2.69 | 0.05 | ||||
| Open defecation | 1.27 | 0.90 | 1.81 | 0.17 | 1.26 | 0.87 | 1.84 | 0.22 | 1.33 | 0.91 | 1.94 | 0.14 | 1.10 | 0.73 | 1.67 | 0.65 | ||||
| Unsanitary Disposal of Children’s Stool | 1.54 | 1.23 | 1.94 | 0.00 | 1.07 | 0.83 | 1.39 | 0.60 | 1.07 | 0.83 | 1.39 | 0.59 | 1.08 | 0.83 | 1.40 | 0.58 | ||||
| Water Source | Piped | 1.00 | 0.19 | 1.00 | 0.26 | 0.26 | 0.61 | |||||||||||||
| Improved | 1.25 | 0.91 | 1.70 | 0.16 | 1.17 | 0.84 | 1.63 | 0.35 | 1.15 | 0.83 | 1.60 | 0.40 | 1.08 | 0.78 | 1.51 | 0.64 | ||||
| Unimproved | 0.93 | 0.67 | 1.29 | 0.66 | 0.88 | 0.62 | 1.24 | 0.46 | 0.86 | 0.61 | 1.22 | 0.41 | 0.90 | 0.63 | 1.29 | 0.57 | ||||
| Surface | 0.84 | 0.19 | 3.85 | 0.83 | 0.61 | 0.13 | 2.92 | 0.53 | 0.56 | 0.12 | 2.71 | 0.47 | 0.56 | 0.12 | 2.75 | 0.48 | ||||
| Distance to Water Source | On premises or delivered | 1.00 | 0.25 | 1.00 | 0.09 | 0.10 | 0.27 | |||||||||||||
| <5 min | 1.02 | 0.74 | 1.42 | 0.90 | 1.05 | 0.74 | 1.47 | 0.80 | 1.00 | 0.71 | 1.42 | 0.98 | 0.91 | 0.64 | 1.30 | 0.62 | ||||
| ≥5 min | 1.29 | 0.94 | 1.77 | 0.11 | 1.43 | 1.03 | 2.00 | 0.04 | 1.40 | 1.00 | 1.96 | 0.05 | 1.23 | 0.87 | 1.75 | 0.24 | ||||
| Non-Modifiable Characteristics | ||||||||||||||||||||
| Child Age | 0.97 | 0.96 | 0.98 | 0.00 | 0.99 | 0.96 | 1.02 | 0.39 | 0.99 | 0.96 | 1.02 | 0.40 | ||||||||
| Male Sex | 1.05 | 0.84 | 1.32 | 0.65 | 1.04 | 0.83 | 1.31 | 0.74 | 1.04 | 0.82 | 1.31 | 0.75 | ||||||||
| Multiple Birth | 0.35 | 0.05 | 2.66 | 0.31 | 0.36 | 0.05 | 2.69 | 0.32 | 0.35 | 0.05 | 2.70 | 0.32 | ||||||||
| Region | Ilocos Region | 1.00 | 0.00 | 0.00 | 0.00 | |||||||||||||||
| Cagayan Valley | 0.72 | 0.33 | 1.57 | 0.41 | 0.69 | 0.31 | 1.52 | 0.35 | 0.65 | 0.29 | 1.43 | 0.28 | ||||||||
| Central Luzon | 1.19 | 0.63 | 2.26 | 0.60 | 1.16 | 0.61 | 2.21 | 0.65 | 1.17 | 0.61 | 2.25 | 0.63 | ||||||||
| Bicol Region | 0.51 | 0.24 | 1.11 | 0.09 | 0.48 | 0.22 | 1.04 | 0.06 | 0.46 | 0.21 | 1.00 | 0.05 | ||||||||
| Western Visayas | 1.53 | 0.80 | 2.90 | 0.20 | 1.47 | 0.77 | 2.81 | 0.24 | 1.44 | 0.75 | 2.76 | 0.27 | ||||||||
| Central Visayas | 0.95 | 0.48 | 1.91 | 0.89 | 0.93 | 0.46 | 1.87 | 0.84 | 0.87 | 0.43 | 1.76 | 0.70 | ||||||||
| Eastern Visayas | 1.00 | 0.49 | 2.05 | 1.00 | 0.95 | 0.46 | 1.95 | 0.88 | 0.93 | 0.45 | 1.94 | 0.86 | ||||||||
| Zamboanga Peninsula | 1.11 | 0.55 | 2.25 | 0.77 | 1.12 | 0.55 | 2.27 | 0.76 | 1.03 | 0.50 | 2.13 | 0.93 | ||||||||
| Northern Mindanao | 0.51 | 0.22 | 1.21 | 0.13 | 0.49 | 0.21 | 1.16 | 0.11 | 0.48 | 0.20 | 1.14 | 0.10 | ||||||||
| Davao Peninsula | 0.49 | 0.21 | 1.13 | 0.10 | 0.48 | 0.21 | 1.10 | 0.08 | 0.45 | 0.19 | 1.04 | 0.06 | ||||||||
| SOCCSKARGEN | 2.04 | 1.06 | 3.91 | 0.03 | 1.98 | 1.03 | 3.80 | 0.04 | 1.96 | 1.00 | 3.83 | 0.05 | ||||||||
| Caraga | 0.95 | 0.47 | 1.93 | 0.89 | 0.90 | 0.44 | 1.83 | 0.77 | 0.85 | 0.41 | 1.74 | 0.65 | ||||||||
| National Capital Region | 1.08 | 0.56 | 2.08 | 0.82 | 1.06 | 0.55 | 2.06 | 0.86 | 1.09 | 0.56 | 2.13 | 0.80 | ||||||||
| Cordillera Admin Region | 0.75 | 0.32 | 1.71 | 0.49 | 0.72 | 0.31 | 1.66 | 0.44 | 0.71 | 0.30 | 1.67 | 0.44 | ||||||||
| ARMM | 1.34 | 0.63 | 2.82 | 0.44 | 1.37 | 0.64 | 2.94 | 0.41 | 1.92 | 0.68 | 5.38 | 0.22 | ||||||||
| CALABARZO | 0.87 | 0.45 | 1.68 | 0.67 | 0.85 | 0.44 | 1.66 | 0.64 | 0.86 | 0.44 | 1.67 | 0.65 | ||||||||
| MIMAROPA | 1.10 | 0.54 | 2.26 | 0.79 | 1.01 | 0.49 | 2.09 | 0.97 | 0.97 | 0.47 | 2.02 | 0.94 | ||||||||
| Rural Residence | 0.93 | 0.71 | 1.22 | 0.61 | 0.91 | 0.69 | 1.19 | 0.48 | 0.86 | 0.65 | 1.13 | 0.28 | ||||||||
| Susceptibility | ||||||||||||||||||||
| Ever breastfed | 0.98 | 0.64 | 1.51 | 0.94 | 0.92 | 0.60 | 1.42 | 0.71 | ||||||||||||
| Vitamin A Supplementation | 1.19 | 0.86 | 1.64 | 0.29 | 1.19 | 0.87 | 1.65 | 0.28 | ||||||||||||
| Iron Supplementation | 0.93 | 0.73 | 1.20 | 0.59 | 1.00 | 0.77 | 1.29 | 0.99 | ||||||||||||
| Intestinal Parasites Medication | 1.21 | 0.91 | 1.61 | 0.20 | 1.17 | 0.87 | 1.56 | 0.30 | ||||||||||||
| Vaccination Index (VI) | Low | 1.00 | 0.00 ** | 1.00 | 0.00 ** | |||||||||||||||
| Intermediate | 0.89 | 0.36 | 2.23 | 0.81 | 0.91 | 0.36 | 2.30 | 0.85 | ||||||||||||
| High | 2.29 | 1.02 | 5.14 | 0.04 | 2.43 | 1.07 | 5.50 | 0.03 | ||||||||||||
| Interaction VI and Child Age | Low VI—Child Age | 0.00 ** | 0.00 ** | |||||||||||||||||
| Intermediate VI—Child Age | 1.03 | 0.99 | 1.07 | 0.17 | 1.03 | 0.99 | 1.07 | 0.20 | ||||||||||||
| High VI—Child Age | 0.97 | 0.94 | 1.00 | 0.10 | 0.97 | 0.94 | 1.01 | 0.11 | ||||||||||||
| Socioeconomic Characteristics | ||||||||||||||||||||
| Maternal Age | 0.99 | 0.97 | 1.01 | 0.31 | ||||||||||||||||
| Maternal Education | None or primary | 0.17 | ||||||||||||||||||
| Secondary | 0.78 | 0.58 | 1.04 | 0.09 | ||||||||||||||||
| Higher | 0.73 | 0.50 | 1.07 | 0.11 | ||||||||||||||||
| Mother working | 1.16 | 0.91 | 1.47 | 0.24 | ||||||||||||||||
| Household Wealth Index | Poorest | 0.28 | ||||||||||||||||||
| Poorer | 1.03 | 0.73 | 1.45 | 0.86 | ||||||||||||||||
| Middle | 0.83 | 0.54 | 1.27 | 0.39 | ||||||||||||||||
| Richer | 0.62 | 0.37 | 1.05 | 0.08 | ||||||||||||||||
| Richest | 0.67 | 0.36 | 1.24 | 0.20 | ||||||||||||||||
| Religion | Roman Catholic | 0.68 | ||||||||||||||||||
| Protestant | 0.71 | 0.32 | 1.57 | 0.40 | ||||||||||||||||
| Islam | 0.82 | 0.46 | 1.46 | 0.50 | ||||||||||||||||
| Other | 1.10 | 0.78 | 1.56 | 0.60 | ||||||||||||||||
| Number of Household Members | 1.00 | 0.94 | 1.06 | 0.96 | ||||||||||||||||
| Number of Under Five Children in Household | 1.00 | 0.84 | 1.19 | 0.96 | ||||||||||||||||
| Nagelkerkes R2 0.023 | Nagelkerkes R2 0.072 | Nagelkerkes R2 0.085 | Nagelkerkes R2 0.094 | |||||||||||||||||
3.2. Qualitative Component
| No. | Setting | Number and Sex of Participants | Range | ||
|---|---|---|---|---|---|
| Female | Male | Total | |||
| 1 | Rural | 73 | 10 | 83 | 19–81 |
| 2 | Urban | 15 | 0 | 15 | 18–39 |
| 3 | Rural | 112 | 2 | 114 | 18–72 |
| 4 | Urban | 10 | 0 | 10 | 35–58 |
| 5 | Urban | 32 | 0 | 32 | 19–73 |
| 6 | Urban | 9 | 0 | 9 | 37–58 |
3.2.1. Defecation and Anal Cleansing Behaviours
“[...] now since we are living in the city, it’s [other cleansing materials] not necessary anymore especially as water is always available.”(FGD 2, Urban)
“You wouldn’t want it [toilet paper] because you prefer water more because it is clean.”(FGD 4, Urban)

“Others just bring water in a pail when they feel the urge.”(FGD 1, Rural)
“When in the middle of the banana plantation, we just use the old banana leaves.”(FGD 1, Rural)
“Especially the urban poor they also use that one [toilet paper], also newspapers. [...] I think they use it because sometimes it is really hard to bring in all the water you need for cleaning.”(FGD 6, Urban)
“[...] usually I also use water, but if there is no water available and I do not want to go out to get water at the faucet I just use the paper.”(FGD 6, Urban)
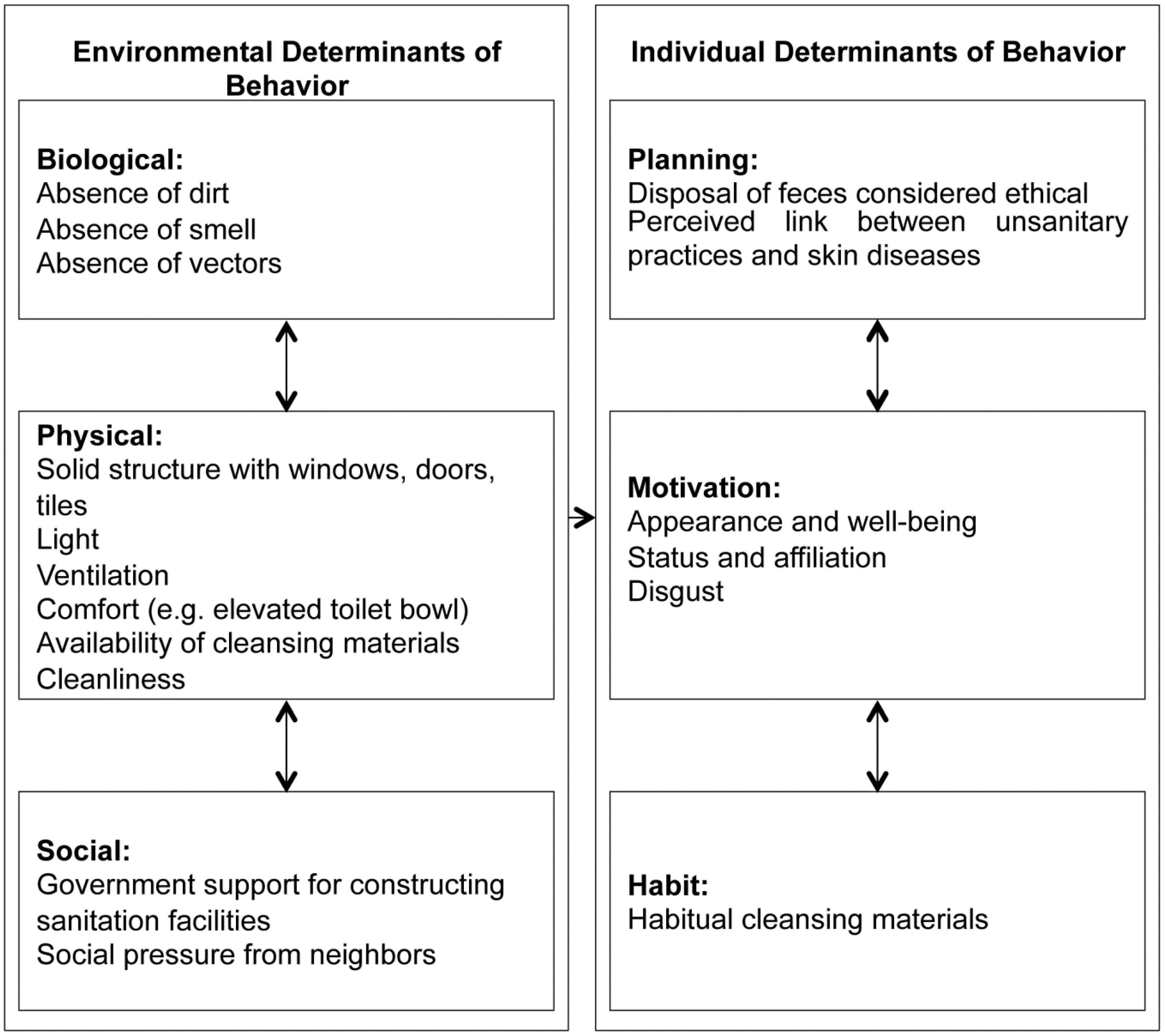
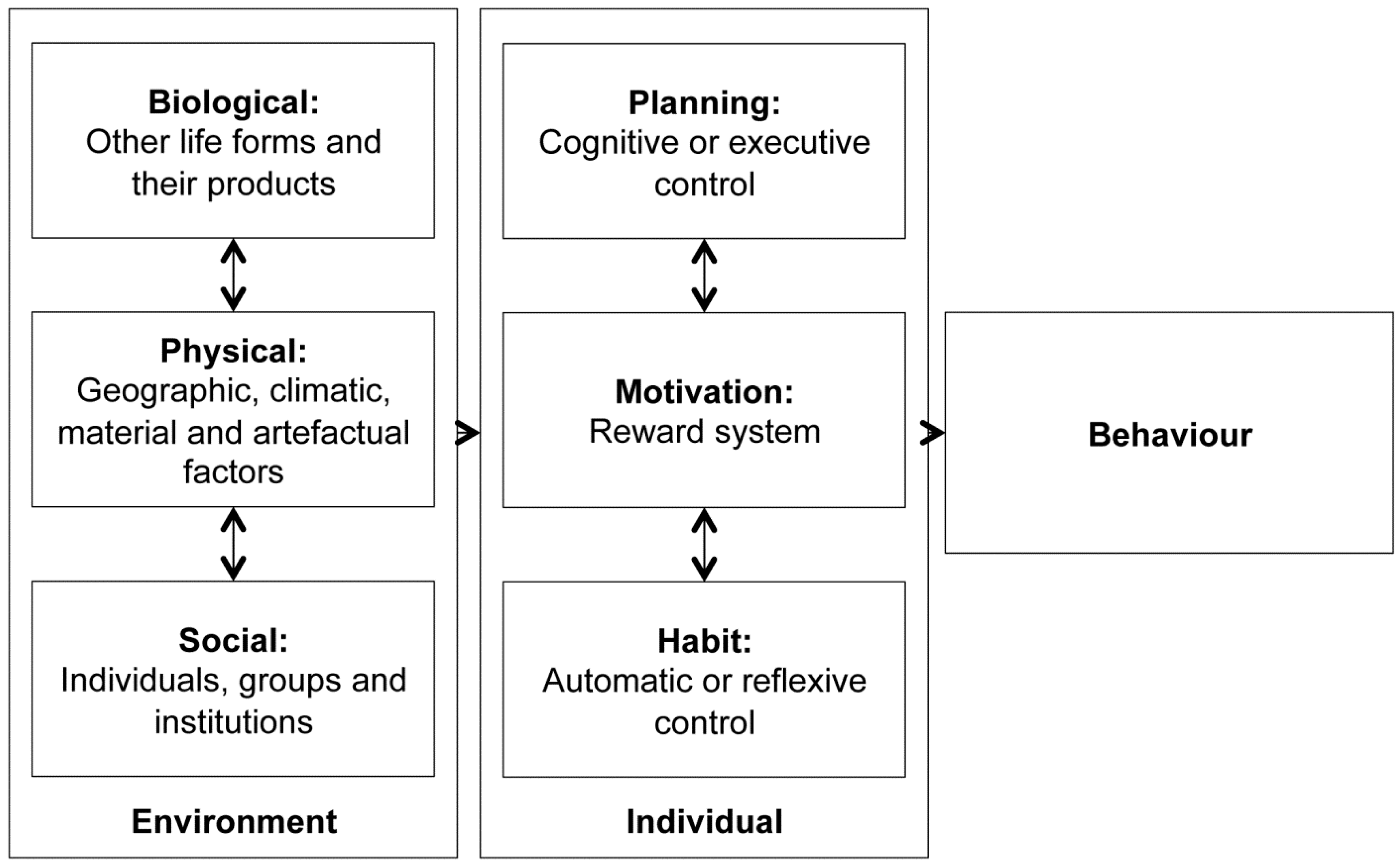
3.2.2. Environmental Determinants of Behaviour
“For me, we used bamboo as wall and it’s really closed. No one can see you when you are inside. So really comfortable.”(FGD 1, Rural)
“The important thing is that there’s that bowl where we can sit down, never mind if someone is there watching us.”(FGD 1, Rural)
“There are also others that just like to do squatting position even though it’s supposedly done in sitting position because the toilet bowl is dirty. They are not comfortable.”(FGD 2, Urban)
“Before, when we used the Antipolo type, our neighbour complained because of the awful smell.”(FGD 1, Rural)
“There are lots of skin problems with their kids. And there are a lot of flies and mosquitoes.”(FGD 4, Urban)
3.2.3. Environmental Determinants of Behaviour: Insights Related to Children
“[…] there was no available water at that time and they were asked to fetch water first from a distant source before they were allowed to use the toilet.”(FGD 4, Urban)
“[The school] is quite distant from our house but they still want to go home. There was this one time that my kid was really uneasy and he wanted to run home. He failed to reach home and defecated in his pants.”(FGD 4, Urban)
“They have [a] toilet in every classroom. But then, the private schools don’t have the same facilities. The toilets are communal. The public have much better sanitation facilities.”(FGD 4, Urban)
3.2.4. Individual Determinants of Behaviour
“Others still bring water along with them even when they are at the banana plantation area.”(FGD 1, Rural)
“It had already become a habit to bring in water when going to the toilet.”(FGD 4, Urban)
“It’s really smelly when we don’t use soap for anal washing.”(FGD 2, Urban)
“There is this bushy area in our vicinity, it really smells like shit. I hate it when we pass there. It is where they dispose of all their wastes.”(FGD 5, Urban)
“I have neighbours who defecate in plastic bags or newspapers and throw them in garbage bins. Their kids also, I noticed that they use newspapers for defecating, and the mother just puts the newspaper in the plastic and then in the bin.”(FGD 4, Urban)
3.2.5. Individual Determinants of Behaviour: Insights Related to Children
“Although our toilet is not that nice, [...] he feels really comfortable using it because it is clean. And we always have water inside the toilet because we have a 6 gallon container.”(FGD 4, Urban)
“They [Ecosan toilets] are not often used by children. [...] They were taught but they don’t like to use it. It is too complicated for them.”(FGD 1, Rural)
“In our community [...], the kids even defecate in an open area and just anywhere.”(FGD 6, Urban)
“My kids are all naked when they use the toilet. [...] They have their own towel. They use it right after defecating. They will take a bath but not including the head and then wipe themselves.”(FGD 4, Urban)
4. Discussion
4.1. Integration of Findings

4.2. Locating Findings in the Literature
4.3. Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 1095–2128. [Google Scholar] [CrossRef]
- Prüss-Üstün, A.; Corvalán, C.F.; World Health Organization. Preventing Disease Through Healthy Environments: Towards an Estimate of the Environmental Burden of Disease: Executive Summary; World Health Organization: Geneva, Switzerland, 2006; p. 16. [Google Scholar]
- Lim, S.; Vos, T.; Flaxman, A.; Danaei, G. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990—2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [PubMed]
- Esrey, S.A.; Potash, J.B.; Roberts, L.; Shiff, C. Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bull. World Health Organ. 1991, 69, 609–621. [Google Scholar] [PubMed]
- Fewtrell, L.; Kaufmann, R.B.; Kay, D.; Enanoria, W.; Haller, L.; Colford, J.M., Jr. Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: A systematic review and meta-analysis. Lancet Infect. Dis. 2005, 5, 42–52. [Google Scholar] [CrossRef]
- Waddington, H.; Snilstveit, B.; White, H.; Fewtrell, L. Water, Sanitation and Hygiene Interventions to Combat Childhood Diarrhoea in Developing Countries; The Internationale Initiative for Impact Evaluation (3ie): New Delhi, India, 2009. [Google Scholar]
- Cairncross, S.; Hunt, C.; Boisson, S.; Bostoen, K.; Curtis, V.; Fung, I.C.; Schmidt, W.P. Water, sanitation and hygiene for the prevention of diarrhoea. Int. J. Epidemiol. 2010, 39, 193–205. [Google Scholar] [CrossRef]
- Aiello, A.E.; Coulborn, R.M.; Perez, V.; Larson, E.L. Effect of hand hygiene on infectious disease risk in the community setting: A meta-analysis. Am. J. Public Health 2008, 98, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Curtis, V.; Cairncross, S. Effect of washing hands with soap on diarrhoea risk in the community: A systematic review. Lancet Infect. Dis. 2003, 3, 275–281. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Country profile of Environmental Burden of Disease: Philippines. In Public Health and the Environment; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation. Progress on Drinking Water and Sanitation: 2012 Update; World Health Organization: Geneva, Switzerland, 2012; p. 60. [Google Scholar]
- Philippine Institute of Development Studies (PIDS). Global Study on Child Poverty and Disparities; National Report Philippines; PIDS Discussion Paper Series No. 2009-27; UNICEF: New York, NY, USA, 2009. [Google Scholar]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behaviour; Englewood Cliffs: Prentice Hall, NJ, USA, 1980. [Google Scholar]
- Ajzen, I. The theory of planned behaviour. Organ. Behav. Hum. Decis Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Aunger, R.; Curtis, V. Kinds of Behaviour. Biol. Philos. 2009, 23, 317–345. [Google Scholar] [CrossRef]
- Ortony, A.; Norman, D.; Revelle, W. Affect and Proto-Affect in Effective Functioning; Fellous, J.M., Arbib, M.A., Eds.; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Rolls, E. The Brain and Emotion; Oxford University Press: Oxford, UK, 1999. [Google Scholar]
- Sloman, A. Beyond shallow models of emotion. Cognit. Process. Int. Q. Cognit. Sci. 2001, 2, 177–198. [Google Scholar]
- Curtis, V.; Danquah, L.; Aunger, R. Planned, motivated and habitual hygiene behaviour: An eleven country review. Health Educ. Res. 2009, 24, 655–673. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Dept. of Noncommunicable Disease Prevention and Health Promotion. Creating an Environment for emotional and Social Well-Being: An Important Responsibility of A Health Promoting and Child-Friendly School; World Health Organization: Geneva, Switzerland, 2003; pp. 12–13. [Google Scholar]
- Measure DHS. In Children Recode Philippines; ICF Macro, Inc.: Calverton, MD, USA, 2008.
- World Health Organization. Diarrhoea: Why Children Are Still Dying and What Can Be Done; World Health Organization: Geneva, Switzerland, 2009; p. 58. [Google Scholar]
- WHO/UNICEF Joint Monitoring Programme (JMP) for Water Supply and Sanitation. Improved and Unimproved Water and Sanitation Facilities. Available online: http://www.webcitation.org/6W5f9cdyv (archived on 4 February 2015).
- Guy, H.; Jamie, B.; World Health Organization; Water Sanitation and Health Team. Domestic Water Quantity, Service Level and Health; World Health Organization: Genev, Switzerland, 2003; p. 33. [Google Scholar]
- World Health Organization; WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation; UNICEF. Core Questions on Drinking Water and Sanitation for Household Surveys; World Health Organization: Geneva, Switzerland, 2006; p. 24. [Google Scholar]
- O’Donnell, O.; van Doorslaer, E.; Wagstaff, A.; Lindelow, A. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation; World Bank: Washington, DC, USA, 2008; pp. 115–129. [Google Scholar]
- IBM SPSS Statistics for Windows; Version 20.0.; IBM Corporation: Armonk, NY, USA.
- Boyatzis, R.E. Transforming Qualitative Information-Thematic Analysis and Code Development; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Farmer, T.; Robinson, K.; Elliott, S.J.; Eyles, J. Developing and implementing a triangulation protocol for qualitative health research. Qual. Health Res. 2006, 16, 377–394. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Murphy, E.; Nicholl, J. Three techniques for integrating data in mixed methods studies. BMJ 2010, 341, c4587. [Google Scholar] [CrossRef]
- Cairncross, S.; Kochar, V. Studying Hygiene Behaviour: Methods, Issues, and Experiences; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Murray, C.J.; Lopez, A.D. Evidence-based health policy—Lessons from the Global Burden of Disease Study. Science 1996, 274, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Vander Hoorn, S.; Murray, C.J. Selected major risk factors and global and regional burden of disease. Lancet 2002, 360, 1347–1360. [Google Scholar] [CrossRef] [PubMed]
- Heijnen, M.; Cumming, O.; Peletz, R.; Chan, G.K.; Brown, J.; Baker, K.; Clasen, T. Shared sanitation vs. individual household latrines: A systematic review of health outcomes. PLoS One 2014, 9. [Google Scholar] [CrossRef]
- Esrey, S.A.; Feachem, R.; Hughes, J. Interventions for the control of diarrhoeal diseases among young children: Improving water supplies and excreta disposal facilities. Bull. World Health Organ. 1985, 63, 757–772. [Google Scholar] [PubMed]
- Curtis, V.; Cairncross, S.; Yonli, R. Review: Domestic Hygiene and Diarrhoea: Pinpointing the Problem. Trop. Med. Int. Health 2000, 5, 22–23. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.; Caruso, B.A.; Obure, A.; Okumu, F.; Rheingans, R.D. Anal cleansing practices and faecal contamination: A preliminary investigation of behaviours and conditions in schools in rural Nyanza Province, Kenya. Trop. Med. Int. Health 2011, 16, 1536–1540. [Google Scholar] [CrossRef] [PubMed]
- Curtis, V.; de Barra, M.; Aunger, R. Disgust as an adaptive system for disease avoidance behaviour. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2011, 366, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Koopman, J.S. Diarrhea and school toilet hygiene in Cali, Colombia. Am. J. Epidemiol. 1978, 107, 412–420. [Google Scholar] [PubMed]
- Freeman, M.C.; Greene, L.E.; Dreibelbis, R.; Saboori, S.; Muga, R.; Brumback, B.; Rheingans, R. Assessing the impact of a school-based water treatment, hygiene and sanitation programme on pupil absence in Nyanza Province, Kenya: A cluster-randomized trial. Trop. Med. Int. Health 2012, 17, 380–391. [Google Scholar] [PubMed]
- Njuguna, V.; Karanja, B.; Thuranira, M.; Shordt, K.; Snel, M.; Cairncross, S.; Biran, A.; Schmidt, W.-P. The Sustainability and Impact of School Sanitation, Water and Hygiene Education in Kenya; UNICEF and IRC International Water and Sanitation Centre: New York, USA; Delft, The Netherlands, 2008. [Google Scholar]
- Stanton, B.F.; Clemens, J.D.; Aziz, K.M.; Rahman, M. Twenty-four-hour recall, knowledge-attitude-practice questionnaires, and direct observations of sanitary practices: A comparative study. Bull. World Health Organ. 1987, 65, 217–222. [Google Scholar] [PubMed]
- Becker, S.; Pullman, T. External Evaluation of the Peru Continuous Survey Experiment; Report No. 07-001-48; USAID: Washington, DC, USA, 2007. [Google Scholar]
- The United States Global Health Strategy. The United States Global Health Strategy: Senegal Global Health Initiative Strategy; The United States Global Health Initiative: Washington, DC, USA, 2011. [Google Scholar]
- Hunt, C. How Safe is Safe?: A Concise Review of the Health Impacts of Water Supply, Sanitation and Hygiene; Water, Engineering and Development Centre, Loughborough University of Technology, WEDC: Loughborough, UK, 2001. [Google Scholar]
- Boerma, J.T.; Black, R.E.; Sommerfelt, A.E.; Rutstein, S.O.; Bicego, G.T. Accuracy and completeness of mothers’ recall of diarrhoea occurrence in pre-school children in demographic and health surveys. Int. J. Epidemiol. 1991, 20, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Gundry, S.; Wright, J.; Conroy, R. A systematic review of the health outcomes related to household water quality in developing countries. J. Water Health 2004, 2, 1–13. [Google Scholar] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Mitchie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337. [Google Scholar] [CrossRef]
- Zomerplaag, J.; Mooijman, A. Child-Friendly Hygiene and Sanitation Facilities in Schools: Indispensable to Effective Hygiene Education; IRC International Water and Sanitation Centre: Delft, The Netherlands, 2005. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pfadenhauer, L.M.; Rehfuess, E. Towards Effective and Socio-Culturally Appropriate Sanitation and Hygiene Interventions in the Philippines: A Mixed Method Approach. Int. J. Environ. Res. Public Health 2015, 12, 1902-1927. https://doi.org/10.3390/ijerph120201902
Pfadenhauer LM, Rehfuess E. Towards Effective and Socio-Culturally Appropriate Sanitation and Hygiene Interventions in the Philippines: A Mixed Method Approach. International Journal of Environmental Research and Public Health. 2015; 12(2):1902-1927. https://doi.org/10.3390/ijerph120201902
Chicago/Turabian StylePfadenhauer, Lisa Maria, and Eva Rehfuess. 2015. "Towards Effective and Socio-Culturally Appropriate Sanitation and Hygiene Interventions in the Philippines: A Mixed Method Approach" International Journal of Environmental Research and Public Health 12, no. 2: 1902-1927. https://doi.org/10.3390/ijerph120201902