Effect of Different Disinfection Protocols on Microbial and Biofilm Contamination of Dental Unit Waterlines in Community Dental Practices

 ,
, 

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dental Units
2.2. Collection and Processing of Water Samples
2.3. Biofilm
2.4. Statistical Analysis
3. Results and Discussion
3.1. Water Samples

{kind=link}
| Control | Intermittent Disinfection | Continuous Disinfection | |||
|---|---|---|---|---|---|
| Microbiological indicators | untreated | hydrogen peroxide, peracetic acid 0.26% | hydrogen peroxide, peracetic acid 0.26% | hydrogen peroxide, silver ions 0.02% | stabilized ClO2 0.22% |
| mains water n: 18 | mains water n: 18 | deionized water n: 18 | deionized water n: 18 | reverse osmosis n: 18 | |
| HPC 22 °C | |||||
| positive samples (%) | 100% | 100% | 100% | 22.2% | 55.6% |
| range (log10 CFU/mL) | (2.00–3.87) | (1.30–2.96) | (0.30–3.86) | (0.00–1.00) | (0.00–1.85) |
| mean ± SD (log10 CFU/mL) | 3.11 ± 0.47 | 1.95 ± 0.60 | 2.20 ± 1.18 | 0.14 ± 0.30 | 0.68 ± 0.73 |
| HPC 36 °C | |||||
| positive samples (%) | 100% | 100% | 94.14% | 27.8% | 100% |
| range (log10 CFU/mL) | (3.00–4.00) | (0.56–2.96) | (0.00–3.57) | (0.00–1.04) | (0.30–2.20) |
| mean ± SD (log10 CFU/mL) | 3.41 ± 0.37 | 2.26 ± 0.43 | 2.30 ± 1.01 | 0.19 ± 0.36 | 1.06 ± 0.60 |
| Pseudomonas aeruginosa | |||||
| positive samples (%) | 27.8% | 55.6% | 27.8% | absent in all samples | absent in all samples |
| range (log10 CFU/100 mL) | (0.00–1.49) | (0.00–1.41) | (0.00–3.00) | ||
| mean ± SD (log10 CFU/100 mL) | 0.17 ± 0.38 | 0.55 ± 0.60 | 0.61 ± 1.05 | ||
| Control | Intermittent Disinfection | Continuous Disinfection | ||||
|---|---|---|---|---|---|---|
| Microbiological indicators | untreated | hydrogen peroxide, peracetic acid 0.26% | hydrogen peroxide, peracetic acid 0.26% | hydrogen peroxide, silver ions 0.02% | stabilized ClO2 0.22% | |
| mains water n: 18 | mains water n: 18 | deionized water n: 18 | deionized water n: 18 | reverse osmosis n: 18 | ||
| HPC 22 °C | ||||||
| 2003 CDC Guidelines
(≤500 CFU/mL) | 16.7% | 66.7% | 61.1% | 100% | 100% | |
| Council Directive 98/83/EC
(≤100 CFU/mL) | 0 | 38.9% | 38.9% | 100% | 100% | |
| HPC 36 °C | ||||||
| Council Directive 98/83/EC (≤20 CFU/mL) | 0 | 0 | 12.4% | 100% | 72.2% | |
| Pseudomonas aeruginosa | ||||||
| Council Directive 98/83/EC (absence in 100 mL) | 72.2% | 44.4% | 72.2% | 100% | 100% | |
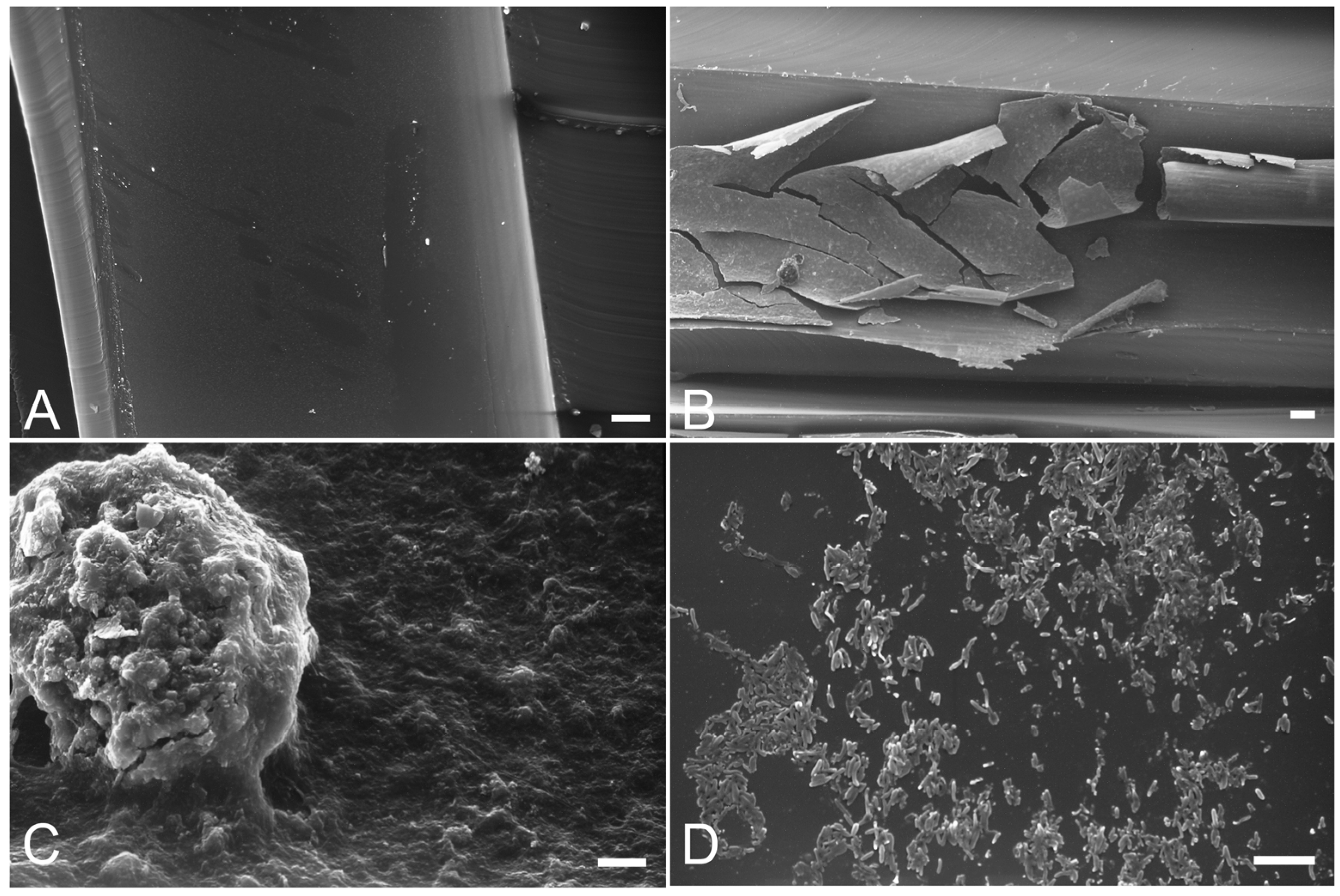
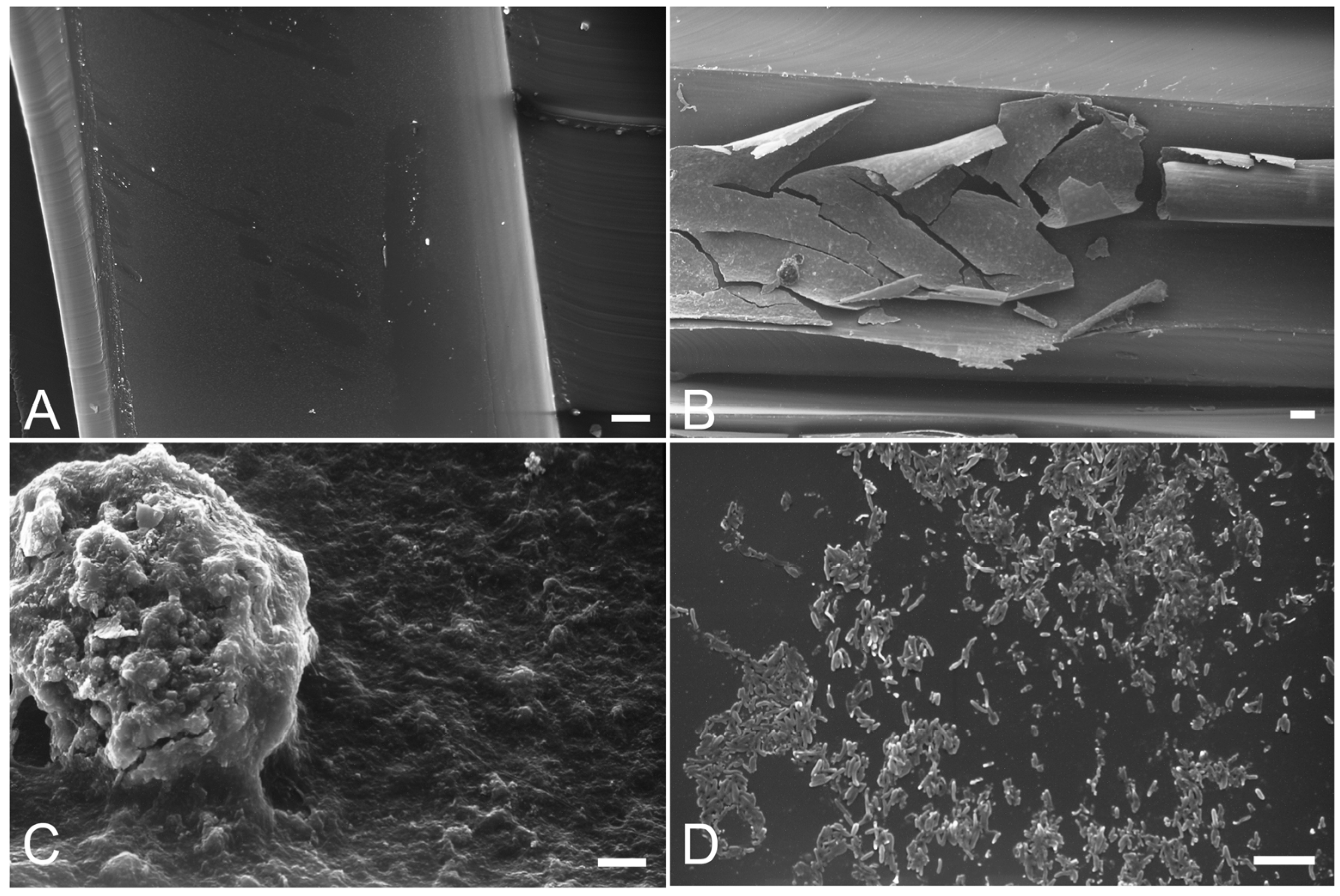
3.2. Biofilm
| Control | Intermittent Disinfection | Continuous Disinfection | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | T0 vs. T1 | T0 | T1 | T0 vs. T1 | ||
| surface covered by biofilm <1 μm (%) | 15.0 | 7.5 | 6.6 | 46.7 | 15.3 | 75.3 | |||
| Thickness | surface covered by biofilm 1–3 μm (%) | 42.5 | 50.0 | 46.7 | 30.8 | p < 0.001 | 44.7 | 23.0 | p < 0.001 |
| surface covered by biofilm >3 μm (%) | 42.5 | 42.5 | 46.7 | 22.5 | 40.0 | 1.7 | |||
| Friability | surface with detached and fragmented biobilm (%) | 70.0 | 67.5 | 57.5 | 67.5 | n.s. | 63.7 | absent | p < 0.001 |
| Bulging | surface with bulging (%) | 65.0 | 45.0 | 36.7 | 3.3 | p < 0.001 | 65.0 | 8.3 | p < 0.001 |
4. Conclusions
- (1)
- S. aureus and β-haemolytic streptococci were never isolated from the water of any f the units. The risk of contamination by retrograde aspiration was therefore negligible. Also Legionella spp and sulphite-reducing Clostridium spores were never detected. This satisfactory result could be indirect proof that the recommended preventive measures and good practices were generally applied.
- (2)
- The high microbial loads found in the untreated control dental unit confirm what has already been widely shown in the literature and highlight the necessity of supplying the DUWLs with disinfection systems. The application of the various disinfection protocols brought about statistically significant reductions in the microbial loads compared to the control, but only continuous disinfection ensured the total abatement of P. aeruginosa.
- (3)
- Biofilm was present to a greater extent and in thicker and more friable layers in the syringe and turbine tubes of the control dental unit than in those undergoing intermittent disinfection and, even more so, continuous disinfection systems. Also the bulk aggregates were significantly more present in the tubes of the control dental unit.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Depaola, L.G.; Mangan, D.; Mills, S.E.; Costerton, W.; Barbeau, J.; Shearer, B.; Bartlett, J. A review of the science regarding dental unit waterlines. J. Am. Dent. Assoc. 2002, 133, 1199–1206. [Google Scholar] [CrossRef]
- Forde, A.; O’Reilly, P.; Fitzgerald, G.; O’Mullane, D.; Burke, F.M.; O’Sullivan, M. Microbial contamination of dental unit water systems. J. Ir. Dent. Assoc. 2005, 51, 115–118. [Google Scholar]
- Pankhurst, C.L. Risk assessment of dental unit waterline contamination. Prim. Dent. Care 2003, 10, 5–10. [Google Scholar] [CrossRef]
- Pasquarella, C.; Veronesi, L.; Napoli, C.; Castiglia, P.; Liguori, G.; Rizzetto, R.; Torre, I.; Righi, E.; Farruggia, P.; Tesauro, M.; et al. Microbial environmental contamination in Italian dental clinics: A multicenter study yielding recommendations for standardized sampling methods and threshold values. Sci. Total Environ. 2012, 420, 289–299. [Google Scholar] [CrossRef]
- Szymańska, J.; Sitkowska, J. Opportunistic bacteria in dental unit waterlines: Assessment and characteristics. Fut. Microbiol. 2013, 8, 681–689. [Google Scholar] [CrossRef]
- Szymańska, J.; Sitkowska, J. Bacterial contamination of dental unit waterlines. Environ. Monit. Assess. 2013, 185, 3603–3611. [Google Scholar] [CrossRef]
- Coleman, D.C.; O’Donnell, M.J.; Shore, A.C.; Russell, R.J. Biofilm problems in dental unit water systems and its practical control. J. Appl. Microbiol. 2009, 106, 1424–1437. [Google Scholar] [CrossRef]
- O’Donnell, M.J.; Boyle, M.A.; Swan, J.; Russell, R.J.; Coleman, D.C. Management of dental unit waterline biofilms in the 21th century. Fut. Microbiol. 2011, 6, 1209–1226. [Google Scholar] [CrossRef]
- Wirthlin, M.R.; Marshall, G.W., Jr.; Rowland, R.W. Formation and contamination of biofilms in dental unit waterlines. J. Periodontol. 2003, 74, 1595–1609. [Google Scholar] [CrossRef]
- Laheij, A.M.; Kistler, J.O.; Belibasakis, G.N.; Välimaa, H.; de Soet, J.J.; European Oral Microbiology Workshop (EOMW 2011). Healthcare-associated viral and bacterial infections in dentistry. J. Oral Microbiol. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Ricci, M.L.; Fontana, S.; Pinci, F.; Fiumana, E.; Pedna, M.F.; Farolfi, P.; Sabattini, M.A.; Scaturro, M. Pneumonia associated with a dental unit waterline. Lancet 2012, 379. [Google Scholar] [CrossRef]
- Lohr, D.C.; Goeken, J.A.; Doty, D.B.; Donta, S.T. Mycobacterium gordonae infection of a prosthetic aortic valve. JAMA 1978, 239, 1528–1530. [Google Scholar] [CrossRef]
- Barbot, V.; Robert, A.; Rodier, M.H.; Imbert, C. Update on infectious risks associated with dental unit waterlines. FEMS Immunol. Med. Microbiol. 2012, 65, 196–204. [Google Scholar] [CrossRef]
- Martin, M.V. The significance of the bacterial contamination of dental unit water systems. Brit. Dent. J. 1987, 163, 152–154. [Google Scholar] [CrossRef]
- Barbeau, J. Lawsuit against a dentist related to serious ocular infection possibly linked to water from a dental handpiece. J. Can. Dent. Assoc. 2007, 73, 618–622. [Google Scholar]
- Pankhurst, C.L.; Coulter, W.A.; Philpott-Howard, J.N.; Surman-Lee, S.; Warburton, F.; Challacombe, S. Evaluation of the potential risk of occupational asthma in dentists exposed to contaminated dental unit waterlines. Prim. Dent. Care 2005, 12, 53–59. [Google Scholar] [CrossRef]
- Borella, P.; Bargellini, A.; Marchesi, I.; Rovesti, S.; Stancanelli, G.; Scaltriti, S.; Moro, M.; Montagna, M.T.; Tatò, D.; Napoli, C.; et al. Prevalence of anti-legionella antibodies among Italian hospital workers. J. Hosp. Infect. 2008, 69, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Kohn, W.G.; Collins, A.S.; Cleveland, J.L.; Harte, J.A.; Eklund, K.J.; Malvitz, D.N. Guidelines for infection control in dental health-care settings—2003. MMWR 2003, 52, 1–61. [Google Scholar]
- Schel, A.J.; Marsh, P.D.; Bradshaw, D.J.; Finney, M.; Fulford, M.R.; Frandsen, E.; Østergaard, E.; ten Cate, J.M.; Moorer, W.R.; Mavridou, A.; et al. Comparison of the efficacies of disinfectants to control microbial contamination in dental unit waterline systems in general dental practices across the European Union. Appl. Environ. Microbiol. 2006, 72, 1380–1387. [Google Scholar] [CrossRef]
- US Environmental Protection Agency. National Primary Drinking Water Regulations, 1999: List of Contaminants. Washington DC, USA. US Environmental Protection Agency. 1999. Available online: http://www.epa.gov/safewater/mcl.html (access on 30 June 2012).
- Italian Republic, Legislative Decree 2.02.2001, n. 31. Implementation of Directive 98/83/EC on the Quality of Water Intended for Human Consumption. G.U. n. 52, 3.03.2001. 2001. Available online: http://www.parlamento.it/parlam/leggi/deleghe/01031dl.htm (access on 30 June 2012).
- Council Directive 98/83/EC of 3 November 1998 on the quality of water intended for human consumption. Off. J. Eur. Commun. 1998, 330, 32–54.
- Linger, J.B.; Molinari, J.A.; Forbes, W.C.; Farthing, C.F.; Winget, W.J. Evaluation of a hydrogen peroxide disinfectant for dental unit waterlines. J. Am. Dent. Assoc. 2001, 132, 1287–1291. [Google Scholar] [CrossRef]
- Zanetti, F.; de Luca, G.; Tarlazzi, P.; Stampi, S. Decontamination of dental unit water systems with hydrogen peroxide. Lett. Appl. Microbiol. 2003, 37, 201–206. [Google Scholar] [CrossRef]
- Jatzwauk, L.; Reitemeier, B. A pilot study of three methods for the reduction of bacterial contamination of dental unit water systems in routine use. Int. J. Hyg. Environ. Health 2002, 204, 303–308. [Google Scholar] [CrossRef]
- Szymanska, J. Bacterial decontamination of DUWL biofilm using oxygenal 6. Ann. Agric. Environ. Med. 2006, 13, 163–167. [Google Scholar]
- Smith, A.J.; Bagg, J.; Hood, J. Use of chlorine dioxide to disinfect dental unit waterlines. J. Hosp. Infect. 2001, 49, 285–288. [Google Scholar] [CrossRef]
- Bansal, R.; Puttaiah, R.; Harris, R.; Reddy, A. Evaluation of two methods in controlling dental treatment water contamination. J. Contemp. Dent. Pract. 2011, 12, 73–83. [Google Scholar]
- Montebugnoli, L.; Chersoni, S.; Prati, C.; Dolci, G. A between-patient disinfection method to control water line contamination and biofilm inside dental units. J. Hosp. Infect. 2004, 56, 297–304. [Google Scholar] [CrossRef]
- Liaqat, I.; Sabri, A.N. Effect of biocides on biofilm bacteria from dental unit water lines. Curr. Microbiol. 2008, 56, 619–624. [Google Scholar] [CrossRef]
- Walker, J.T.; Bradshaw, D.J.; Fulford, M.R.; Marsh, P.D. Microbiological evaluation of a range of disinfectant products to control mixed-species biofilm contamination in a laboratory model of a dental unit water system. Appl. Environ. Microbiol. 2003, 69, 3327–3332. [Google Scholar] [CrossRef]
- American Public Health Association. Standard Methods for the Examination of Water and Wastewater, 21st ed.; APHA, AWWA and WEF: Washington, DC, USA, 2005. [Google Scholar]
- Leoni, E.; Legnani, P.P. Comparison of selective procedures for isolation and enumeration of Legionella from hot water systems. J. Appl. Microbiol. 2001, 90, 27–33. [Google Scholar] [CrossRef]
- Leoni, E.; Sacchetti, R.; Zanetti, F.; Legnani, P.P. Control of Legionella pneumophila contamination in a system for respiratory hydrotherapy with sulphurous spa water. Infect. Control Hosp. Epidemiol. 2006, 27, 716–721. [Google Scholar] [CrossRef]
- ImageProPlus Software (MediaCybernetics). Available online: http://www.mediacy.com (accessed on 14 February 2014).
- Aprea, L.; Cannova, L.; Firenze, A.; Bivona, M.S.; Amodio, E.; Romano, N. Can technical, functional and structural characteristics of dental units predict Legionella pneumophila and Pseudomonas aeruginosa contamination? J. Oral. Sci. 2010, 52, 641–646. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Dallolio, L.; Scuderi, A.; Rini, M.S.; Valente, S.; Farruggia, P.; Sabattini, M.A.B.; Pasquinelli, G.; Acacci, A.; Roncarati, G.; Leoni, E. Effect of Different Disinfection Protocols on Microbial and Biofilm Contamination of Dental Unit Waterlines in Community Dental Practices. Int. J. Environ. Res. Public Health 2014, 11, 2064-2076. https://doi.org/10.3390/ijerph110202064
Dallolio L, Scuderi A, Rini MS, Valente S, Farruggia P, Sabattini MAB, Pasquinelli G, Acacci A, Roncarati G, Leoni E. Effect of Different Disinfection Protocols on Microbial and Biofilm Contamination of Dental Unit Waterlines in Community Dental Practices. International Journal of Environmental Research and Public Health. 2014; 11(2):2064-2076. https://doi.org/10.3390/ijerph110202064
Chicago/Turabian StyleDallolio, Laura, Amalia Scuderi, Maria S. Rini, Sabrina Valente, Patrizia Farruggia, Maria A. Bucci Sabattini, Gianandrea Pasquinelli, Anna Acacci, Greta Roncarati, and Erica Leoni. 2014. "Effect of Different Disinfection Protocols on Microbial and Biofilm Contamination of Dental Unit Waterlines in Community Dental Practices" International Journal of Environmental Research and Public Health 11, no. 2: 2064-2076. https://doi.org/10.3390/ijerph110202064