Female University Students’ Physical Activity Levels and Associated Factors—A Cross-Sectional Study in Southwestern Saudi Arabia

Abstract
:1. Introduction
2. Experimental Section
2.1. Design and Participants
2.2. Anthropometric Measurements
2.3. Instrument for Lifestyle Patterns
2.4. Statistical Analysis

{kind=link}
{kind=link}
| Activity levels based on METs tertiles | |||
|---|---|---|---|
| Low, n = 220 | Moderate, n = 220 | High, n = 220 | |
| Age, mean (SD) | 20.5 (1.5) | 20.4 (1.4) | 20.3 (1.5) |
| Anthropometrics | |||
| Waist to height ratio, mean (SD) | 45.1 (6.3) | 45.7 (6.0) | 45.5 (6.7) |
| BMI, mean (SD) | 22.1 (4.3) | 22.9 (4.0) | 23.0 (4.4) |
| BMI classification, n (%) | |||
| UW (BMI ≤ 18,49) | 46 (47) | 26 (26.5) | 26 (26.5) |
| NW (BMI = 18.5–24.99) * | 119 (31) | 130 (35) | 127 (34) |
| OW (BMI = 25–29.99) | 32 (27) | 45 (38) | 42 (35) |
| Obesity (BMI ≥ 30) | 11 (29) | 11 (29) | 16 (42) |
| PA behaviors | |||
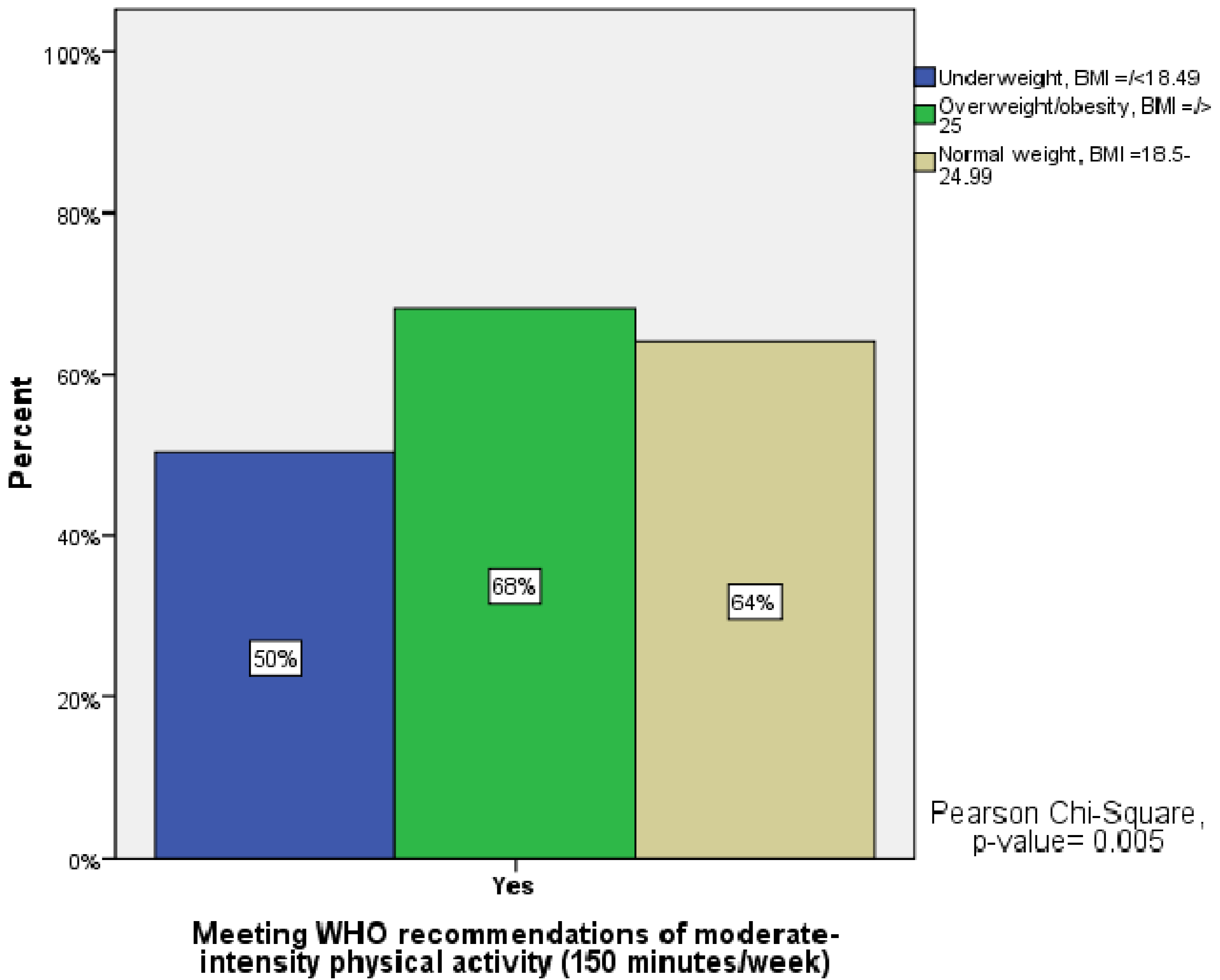
| Meeting WHO recommendations of moderate-intensity PA (150 minutes/week), n (%) | |||
| Yes * | 18 (4) | 177 (43) | 217 (53) |
| No | 202 (82) | 43 (17) | 3 (1) |
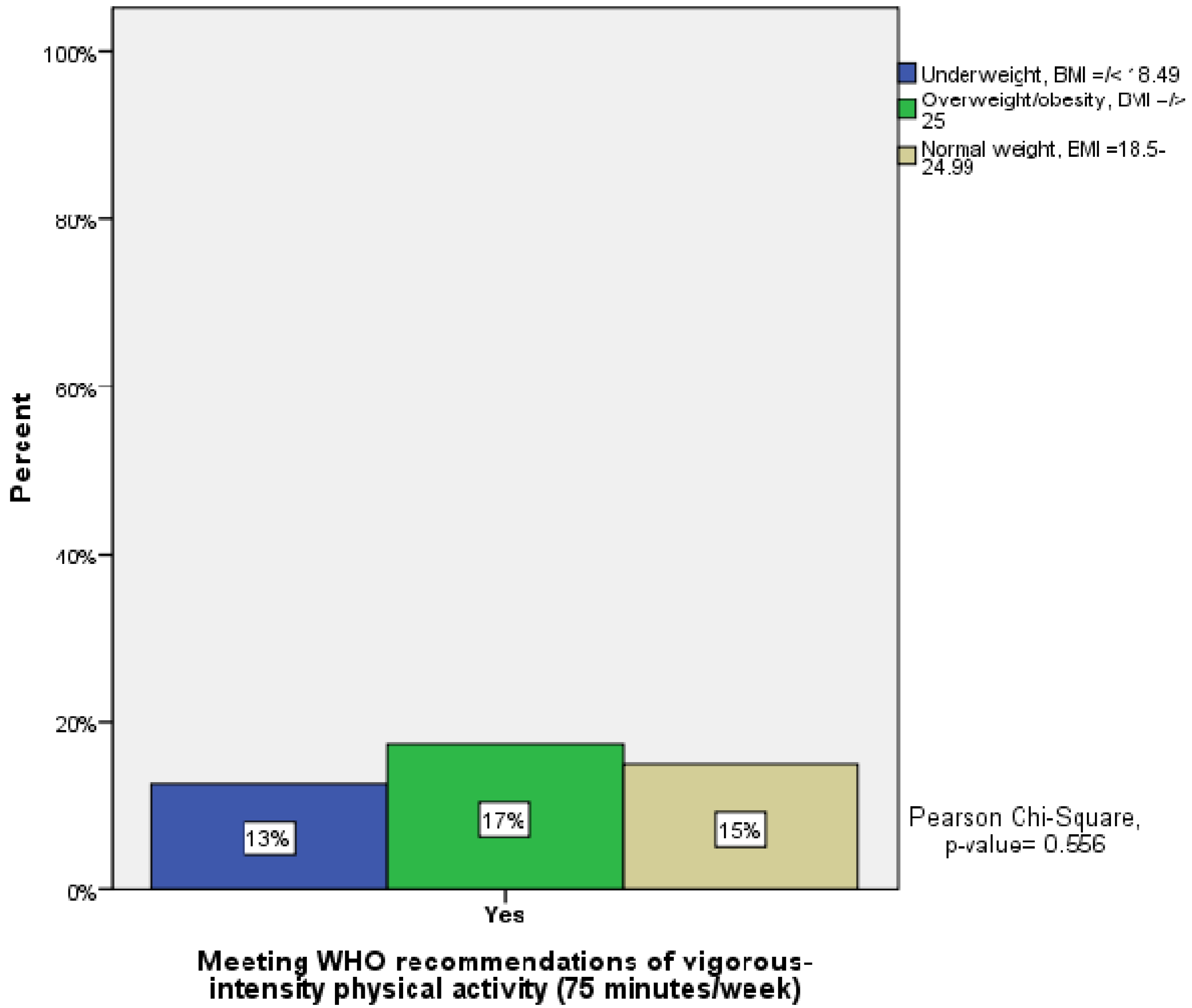
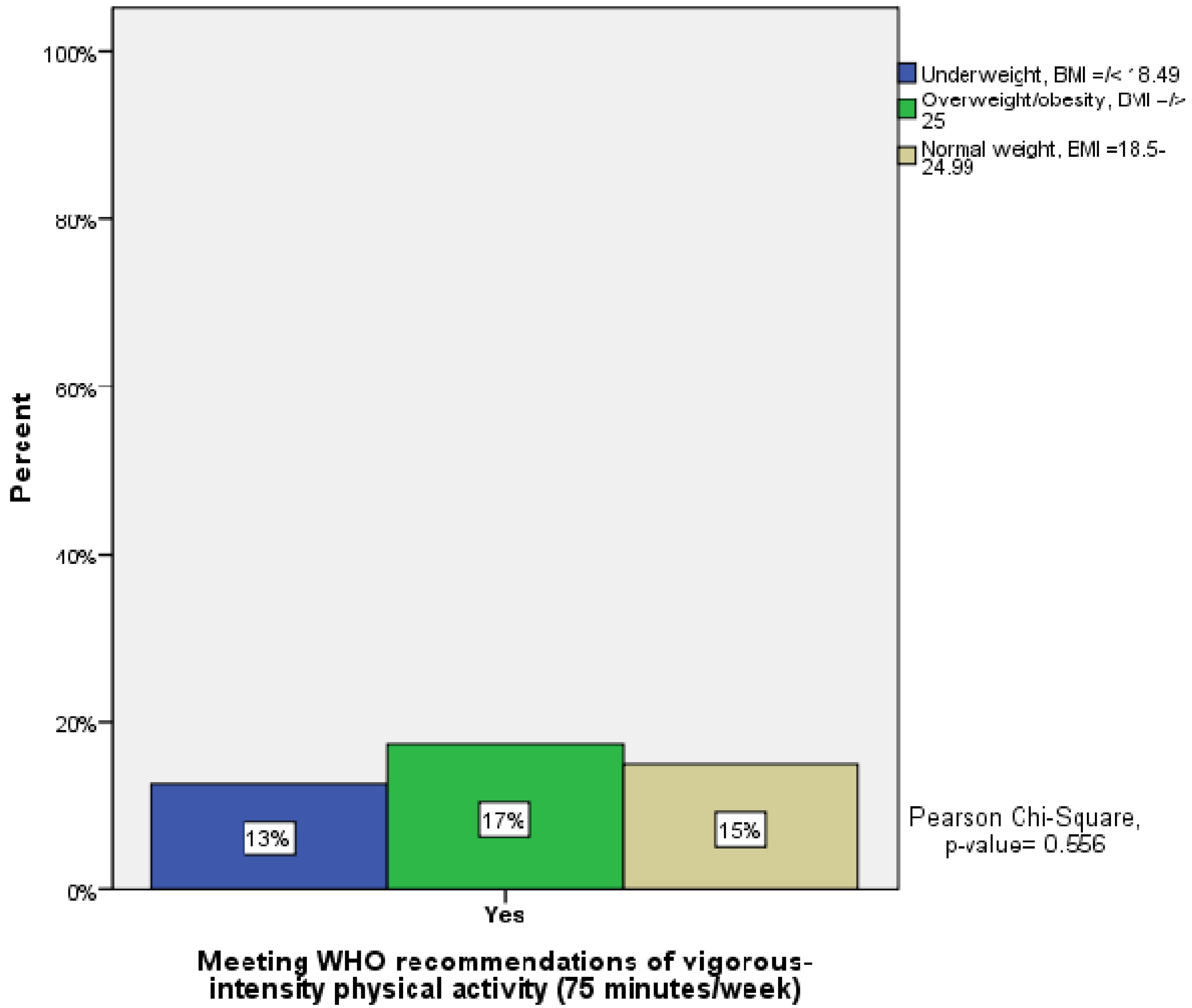
| Meeting WHO recommendations of vigorous-intensity PA (75 minutes/week), n (%) | |||
| Yes * | 0 (0) | 14 (14) | 85 (86) |
| No | 220 (39) | 206 (37) | 135 (24) |
| Parents’ support for regular exercise, n (%) | |||
| Yes * | 123 (32) | 126 (32) | 142 (36) |
| No | 76 (35) | 79 (37) | 61 (28) |
| My parents discourage me from exercising | 21 (40) | 15 (28) | 17 (32) |
| Reasons for regular exercise, n (%) | |||
| For health * | 80 (37) | 73 (34) | 61 (29) |
| To lose weight | 58 (28) | 77 (38) | 69 (34) |
| To have fun | 55 (31) | 54 (31) | 67 (38) |
| Other reasons | 16 (36) | 11 (25) | 17 (39) |
| Reasons for not exercising regularly, n (%) | |||
| Time scarcity * | 123 (34) | 115 (31) | 130 (35) |
| Lack of a suitable place | 44 (38) | 41 (36) | 30 (26) |
| No one is exercising with me | 21 (31) | 27 (40) | 19 (29) |
| Other reasons | 21 (41) | 13 (26) | 17 (33) |
| Presence of regularly exercising parents or siblings, n (%) | |||
| Yes * | 138 (32) | 142 (33) | 150 (35) |
| No | 82 (36) | 78 (34) | 70 (30) |
3. Results
| Activity levels based on METs tertiles | |||
|---|---|---|---|
| Low, n = 220 | Moderate, n = 220 | High, n = 220 | |
| Socioeconomic factors | |||
| Marital status, n (%) | |||
| Unmarried * | 204 (33) | 210 (34) | 199 (33) |
| Married without children | 7 (25) | 6 (21) | 15 (54) |
| Married with children | 9 (47) | 4 (21) | 6 (32) |
| Number of sisters, n (%) | |||
| None * | 9 (37) | 10 (42) | 5 (21) |
| Only one | 16 (29) | 18 (33) | 21 (38) |
| Two–three | 67 (31) | 79 (37) | 69 (32) |
| Four–five | 84 (38) | 70 (32) | 67 (30) |
| Six or more | 43 (30) | 43 (30) | 58 (40) |
| Number of brothers, n (%) | |||
| None * | 5 (46) | 3 (27) | 3 (27) |
| Only one | 21 (43) | 12 (24) | 16 (33) |
| Two–three | 65 (28) | 86 (37) | 81 (35) |
| Four–five | 75 (37) | 61 (30) | 65 (33) |
| Six or more | 54 (33) | 57 (34) | 55 (33) |
| Fathers’ level of education, n (%) | |||
| Primary or less * | 42 (36) | 36 (30) | 40 (34) |
| Primary higher | 43 (34) | 47 (37) | 36 (29) |
| Secondary | 50 (33) | 48 (32) | 53 (35) |
| Bachelor | 68 (33) | 72 (35) | 64 (32) |
| Master or PhD | 17 (28) | 17 (28) | 27 (44) |
| Mothers’ level of education, n (%) | |||
| Primary or less * | 135 (38) | 118 (33) | 104 (29) |
| Primary higher | 27 (23) | 45 (38.5) | 45 (38.5) |
| Secondary | 32 (35) | 30 (32) | 31 (33) |
| Bachelor | 23 (29) | 23 (29) | 34 (42) |
| Master or PhD | 3 (23) | 4 (31) | 6 (46) |
| Cars in the household, n (%) | |||
| No cars * | 2 (67) | 0 (0) | 1 (33) |
| One car | 22 (44) | 14 (28) | 14 (28) |
| Two cars | 74 (37) | 63 (31.5) | 63 (31.5) |
| Three cars or more | 122 (30) | 143 (35) | 142 (35) |
| Type of residence, n (%) | |||
| Apartment * | 33 (40) | 24 (29) | 25 (31) |
| Villa | 126 (31) | 125 (31) | 153 (38) |
| One floor in villa | 50 (33) | 63 (42) | 37 (25) |
| Environmental factors | |||
| Proximity to supermarkets, n (%) | |||
| Very close * | 40 (28) | 52 (37) | 50 (35) |
| Kind of close | 145 (37) | 125 (31) | 126 (32) |
| Far from house | 35 (29) | 43 (35) | 44 (36) |
| Proximity to malls, n (%) | |||
| Very close * | 13 (46) | 10 (36) | 5 (18) |
| Kind of close | 72 (29) | 87 (35) | 90 (36) |
| Far from house | 135 (35) | 123 (32) | 125 (33) |
| Proximity to parks, n (%) | |||
| Very close * | 35 (36) | 36 (37) | 26 (27) |
| Kind of close | 85 (39) | 70 (32) | 63 (29) |
| Far from house | 100 (29) | 114 (33) | 130 (38) |

| Variable | n | Estimate | Std. Error | p-value | OR | 95% CI for OR |
|---|---|---|---|---|---|---|
| Parents’ support for regular exercise | ||||||
| Yes * | 391 | |||||
| No | 216 | −0.26 | 0.16 | 0.092 b) | 0.77 | 0.57–1.04 |
| My parents don’t like exercising | 53 | −0.29 | 0.27 | 0.286 | 0.75 | 0.44–1.27 |
| Reasons for regular exercise | ||||||
| For health * | 214 | |||||
| To lose weight | 204 | 0.32 | 0.18 | 0.077 b) | 1.38 | 0.97–1.96 |
| To have fun | 176 | 0.36 | 0.19 | 0.056 b) | 1.43 | 0.99–2.07 |
| Other reasons | 44 | 0.26 | 0.30 | 0.402 | 1.29 | 0.71–2.34 |
| Marital status | ||||||
| Not married * | 613 | |||||
| Married without children | 28 | 0.73 | 0.37 | 0.047a) | 2.07 | 1.01–4.24 |
| Married with children | 19 | −0.37 | 0.43 | 0.386 | 0.69 | 0.30–1.60 |
| Mothers’ level of education | ||||||
| Primary or less * | 357 | |||||
| Primary higher | 117 | 0.53 | 0.20 | 0.007 a) | 1.70 | 1.16–2.51 |
| Secondary | 93 | 0.17 | 0.21 | 0.420 | 1.19 | 0.78–1.81 |
| Bachelor | 80 | 0.52 | 0.23 | 0.023 a) | 1.68 | 1.07–2.63 |
| Master or PhD | 13 | 0.73 | 0.53 | 0.166 | 2.08 | 0.74–5.83 |
| Type of residence | ||||||
| Flat * | 82 | |||||
| Villa | 404 | 0.38 | 0.22 | 0.088 b) | 1.46 | 0.95–2.27 |
| One floor in villa | 150 | 0.04 | 0.25 | 0.863 | 1.04 | 0.64–1.72 |
| Traditional house | 23 | −0.26 | 0.44 | 0.555 | 0.77 | 0.33–1.82 |
| Proximity to malls | ||||||
| Very close * | 28 | |||||
| Kind of close | 249 | 0.80 | 0.38 | 0.034 a) | 2.22 | 1.06–4.62 |
| Far from house | 383 | 0.58 | 0.37 | 0.118 | 1.78 | 0.86–3.65 |
| Proximity to parks | ||||||
| Very close * | 97 | |||||
| Kind of close | 218 | −0.03 | 0.23 | 0.907 | 0.97 | 0.63–1.51 |
| Far from house | 344 | 0.40 | 0.21 | 0.058 | 1.49 | 0.99–2.26 |
| BMI classification | ||||||
| NW (BMI = 18.5–24.99) * | 376 | |||||
| UW (BMI ≤ 18.49) | 98 | −0.54 | 0.21 | 0.011 a) | 0.59 | 0.39–0.89 |
| OW (BMI = 25–29.99) | 119 | 0.14 | 0.19 | 0.480 | 1.15 | 0.79–1.68 |
| Obesity (BMI ≥ 30) | 38 | 0.26 | 0.31 | 0.406 | 1.30 | 0.70–2.40 |
| Variable | Estimate | Std. Error | p-value | OR | 95% CI for OR |
|---|---|---|---|---|---|
| Marital status | |||||
| Not married * | |||||
| Married without children | 1.20 | 0.43 | 0.005 a) | 3.33 | 1.45–7.64 |
| Married with children | −0.73 | 0.47 | 0.121 | 0.48 | 0.19–1.21 |
| Mothers' level of education | |||||
| Primary or less * | |||||
| Primary higher | 0.64 | 0.22 | 0.004 a) | 1.89 | 1.23–2.91 |
| Secondary | 0.27 | 0.25 | 0.274 | 1.31 | 0.81–2.12 |
| Bachelor | 0.29 | 0.26 | 0.263 | 1.33 | 0.81–2.19 |
| Master or PhD | 0.74 | 0.57 | 0.195 | 2.10 | 0.68–6.47 |
| Proximity to Parks | |||||
| Very close * | |||||
| Kind of close | −0.00 | 0.25 | 0.997 | 1.00 | 0.61–1.64 |
| Far from house | 0.62 | 0.24 | 0.009 a) | 1.86 | 1.17–2.96 |
| BMI classification | |||||
| NW (BMI 18.5–24.99) * | |||||
| UW (BMI ≤ 18,49) | −0.53 | 0.22 | 0.018 a) | 0.59 | 0.38–0.91 |
| OW/obesity (BMI ≥ 25) | 0.11 | 0.21 | 0.610 | 1.12 | 0.73–1.69 |
4. Discussion
5. Conclusions
Conflict of Interest
Acknowledgements
References
- Khawaja, M.; Dawns, J.; Meyerson-Knox, S.; Yamout, R. Disparities in child health in the Arab region during the 1990s. Int. J. Equity Health 2008, 7, 24. [Google Scholar] [CrossRef]
- Al-Nozha, M.M.; Al-Hazzaa, H.M.; Arafah, M.R.; Al-Khadra, A.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Khan, N.B.; Al-Marzouki, K.; Al-Harthi, S.S.; Abdullah, M.; et al. Prevalence of physical activity and inactivity among Saudis aged 30–70 years. A population-based cross-sectional study. Saudi Med. J. 2007, 28, 559–568. [Google Scholar]
- Al-Hazzaa, H.M. Physical inactivity in Saudi Arabia. An under served public health issue. Saudi Med. J. 2010, 31, 1278–1279, author reply 9–80. [Google Scholar]
- Sisson, S.B.; Katzmarzyk, P.T. International prevalence of physical activity in youth and adults. Obes. Rev. 2008, 9, 606–614. [Google Scholar] [CrossRef]
- Bauman, A.; Bull, F.; Chey, T.; Craig, C.L.; Ainsworth, B.E.; Sallis, J.F.; Bowles, H.R.; Hagstromer, M.; Sjostrom, M.; Pratt, M.; The IPS Group. The International Prevalence Study on Physical Activity: Results from 20 countries. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 21. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Popkin, B.M. The nutrition transition and obesity in the developing world. J. Nutr. 2001, 131, 871S–873S. [Google Scholar]
- Beets, M.W.; Bornstein, D.; Beighle, A.; Cardinal, B.J.; Morgan, C.F. Pedometer-measured physical activity patterns of youth: A 13-country review. Am. J. Prev. Med. 2010, 38, 208–216. [Google Scholar] [CrossRef]
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Al-Eisa, E.S.; Al-Sobayel, H.I. Physical activity and health beliefs among saudi women. J. Nutr. Metab. 2012, 2012, 642187. [Google Scholar]
- Mahfouz, A.A.; Shatoor, A.S.; Khan, M.Y.; Daffalla, A.A.; Mostafa, O.A.; Hassanein, M.A. Nutrition, physical activity, and gender risks for adolescent obesity in southwestern Saudi Arabia. Saudi J. Gastroenterol. 2011, 17, 318–322. [Google Scholar] [CrossRef]
- Musaiger, A.O.; Al-Hazzaa, H.M.; Al-Qahtani, A.; Elati, J.; Ramadan, J.; AboulElla, N.A.; Mokhtar, N.; Kilani, H.A. Strategy to combat obesity and to promote physical activity in Arab countries. Diabetes Metab. Syndr. Obes. 2011, 4, 89–97. [Google Scholar]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- WHO. Global recommendations on physical activity for health. 2010. Available online: http://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf (accessed on 29 June 2013).
- The world health report 2002. Reducing risks, promoting healthy life. Available online: http://www.who.int/whr/2002/en/whr02_en.pdf (accessed on 28 February 2013).
- Al-Hazzaa, H.M.; Abahussain, N.A.; Al-Sobayel, H.I.; Qahwaji, D.M.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 140. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N. Ecological Models of Health Behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 3rd ed.; Glanz, K., Rimer, B.K., Lewis, F.M., Eds.; Jossey-Bass: San Francisco, CA, USA; pp. 462–484.
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Musaiger, A.O. Convergent validity of the Arab Teens Lifestyle Study (ATLS) physical activity questionnaire. Int. J. Environ. Res. Public Health 2011, 8, 3810–3820. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Musaiger, A.O. Arab Teens Lifestyle Study (ATLS): Objectives, design, methodology and implications. Diabetes Metab. Syndr. Obes. 2011, 4, 417–426. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Al-Ahmadi, M. A self-reported questionnaire for the assessment of physical activity in youth 15–25 years: Development, reliability and construct validity. Arab J. Food Nutr. 2003, 4, 279–291. [Google Scholar]
- Al-Ahmadi, M.; Al-Hazzaa, H.M. Validity of a self-reported questionnaire for youth 15–25 years: Comparison with accelerometer, pedometer and heart rate telemetry. Saudi Sports Med. J. 2004, 7, 2–14. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M. Health-enhancing physical activity among Saudi adults using the International Physical Activity Questionnaire (IPAQ). Public Health Nutr. 2007, 10, 59–64. [Google Scholar]
- Al-Hazzaa, H.M. The public health burden of physical inactivity in saudi arabia. J. Family Commun. Med. 2004, 11, 45–51. [Google Scholar]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Vereecken, C.; Mulvihill, C.; Roberts, C.; Currie, C.; Pickett, W.; The Health Behaviour in School-Aged Children Obesity Working Group. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes. Rev. 2005, 6, 123–132. [Google Scholar] [CrossRef]
- Wang, Y.; Monteiro, C.; Popkin, B.M. Trends of obesity and underweight in older children and adolescents in the United States, Brazil, China, and Russia. Am. J. Clin. Nutr. 2002, 75, 971–977. [Google Scholar]
- Dumith, S.C.; Hallal, P.C.; Reis, R.S.; Kohl, H.W., III. Worldwide prevalence of physical inactivity and its association with human development index in 76 countries. Prev. Med. 2011, 53, 24–28. [Google Scholar] [CrossRef]
- Al-Nuaim, A.A.; Al-Nakeeb, Y.; Lyons, M.; Al-Hazzaa, A.M.; Nevill, A.; Collins, P.; Duncan, M.J. The prevalence of physical activity and sedentary behaviours relative to obesity among adolescents from Al-Ahsa, Saudi Arabia: Rural versus urban variations. J. Nutr. Metab. 2012, 2012, 417589. [Google Scholar]
- Varela-Mato, V.; Cancela, J.M.; Ayan, C.; Martín, V.; Molina, A. Lifestyle and Health among Spanish University Students: Differences by gender and academic discipline. Int. J. Environ. Res. Public Health 2012, 9, 2728–2741. [Google Scholar] [CrossRef]
- Kimm, S.Y.; Glynn, N.W.; Kriska, A.M.; Barton, B.A.; Kronsberg, S.S.; Daniels, S.R.; Crawford, P.B.; Sabry, Z.I.; Liu, K. Decline in physical activity in black girls and white girls during adolescence. N. Engl. J. Med. 2002, 347, 709–715. [Google Scholar] [CrossRef]
- Al-Nakeeb, Y.; Lyons, M.; Collins, P.; Al-Nuaim, A.A.; Al-Hazzaa, A.M.; Duncan, M.J.; Nevill, A. Obesity, physical activity and sedentary behavior amongst British and Saudi youth: A cross-cultural study. Int. J. Environ. Res. Public Health 2012, 9, 1490–1506. [Google Scholar] [CrossRef] [Green Version]
- Stang, J.; Story, M. Guidelines for Adolescent Nutrition Services. 2005, p. page 93. Available online: http://www.epi.umn.edu/let/pubs/adol_book.shtm (accessed on 20 May 2013).
- Neumark-Sztainer, D.; Goeden, C.; Story, M.; Wall, M. Associations between body satisfaction and physical activity in adolescents: Implications for programs aimed at preventing a broad spectrum of weight-related disorders. Eat. Disord. 2004, 12, 125–137. [Google Scholar] [CrossRef]
- Harris, K.C.; Kuramoto, L.K.; Schulzer, M.; Retallack, J.E. Effect of school-based physical activity interventions on body mass index in children: A meta-analysis. Can. Med. Assoc. J. 2009, 180, 719–726. [Google Scholar] [CrossRef]
- Kahan, D. Overweight and its relationship to Middle Eastern American college students’ sociodemographics and physical activity. Res. Q. Exerc. Sport 2007, 78, 248–256. [Google Scholar]
- Levin, S.; Lowry, R.; Brown, D.R.; Dietz, W.H. Physical activity and body mass index among US adolescents – Youth risk behavior survey, 1999. Arch. Pediatr. Adolesc. Med. 2003, 157, 816–820. [Google Scholar] [CrossRef]
- Mabry, R.M.; Reeves, M.M.; Eakin, E.G.; Owen, N. Evidence of physical activity participation among men and women in the countries of the Gulf cooperation council: A review. Obes. Rev. 2010, 11, 457–464. [Google Scholar]
- Alderman, B.L.; Benham-Deal, T.B.; Jenkins, J.M. Change in parental influence on children’s physical activity over time. J. Phys. Act. Health 2010, 7, 60–67. [Google Scholar]
- Ainsworth, B.E.; Caspersen, C.J.; Matthews, C.E.; Masse, L.C.; Baranowski, T.; Zhu, W. Recommendations to improve tne accuracy of estimates of physical activity derived from self report. J. Phys. Act. Health 2012, 9 (Suppl 1), S76–S84. [Google Scholar]
© 2013 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Khalaf, A.; Ekblom, Ö.; Kowalski, J.; Berggren, V.; Westergren, A.; Al-Hazzaa, H. Female University Students’ Physical Activity Levels and Associated Factors—A Cross-Sectional Study in Southwestern Saudi Arabia. Int. J. Environ. Res. Public Health 2013, 10, 3502-3517. https://doi.org/10.3390/ijerph10083502
Khalaf A, Ekblom Ö, Kowalski J, Berggren V, Westergren A, Al-Hazzaa H. Female University Students’ Physical Activity Levels and Associated Factors—A Cross-Sectional Study in Southwestern Saudi Arabia. International Journal of Environmental Research and Public Health. 2013; 10(8):3502-3517. https://doi.org/10.3390/ijerph10083502
Chicago/Turabian StyleKhalaf, Atika, Örjan Ekblom, Jan Kowalski, Vanja Berggren, Albert Westergren, and Hazzaa Al-Hazzaa. 2013. "Female University Students’ Physical Activity Levels and Associated Factors—A Cross-Sectional Study in Southwestern Saudi Arabia" International Journal of Environmental Research and Public Health 10, no. 8: 3502-3517. https://doi.org/10.3390/ijerph10083502