Factors Increasing Vulnerability to Health Effects before, during and after Floods


Abstract
:1. Introduction
2. Experimental Section
- “floods”[MeSH Terms] OR
- “floods”[All Fields] OR
- “flood”[All Fields]
- AND risk factor terms
- “risk factors”[MeSH Terms] OR
- “risk”[All Fields] AND "factors”[All Fields] OR
- “risk factors”[All Fields]
- AND in humans
- “humans”[MeSH Terms]
- What are the demographic, socioeconomic, health status, or other factors associated with increased risk of morbidity or mortality, among flooded populations?
- What are the health effects of floods when compared to non-flooded groups?
- What are the characteristics of individuals who experienced flood-related morbidity or mortality?
- With reference to a source population.
- Without reference to source population.
3. Results
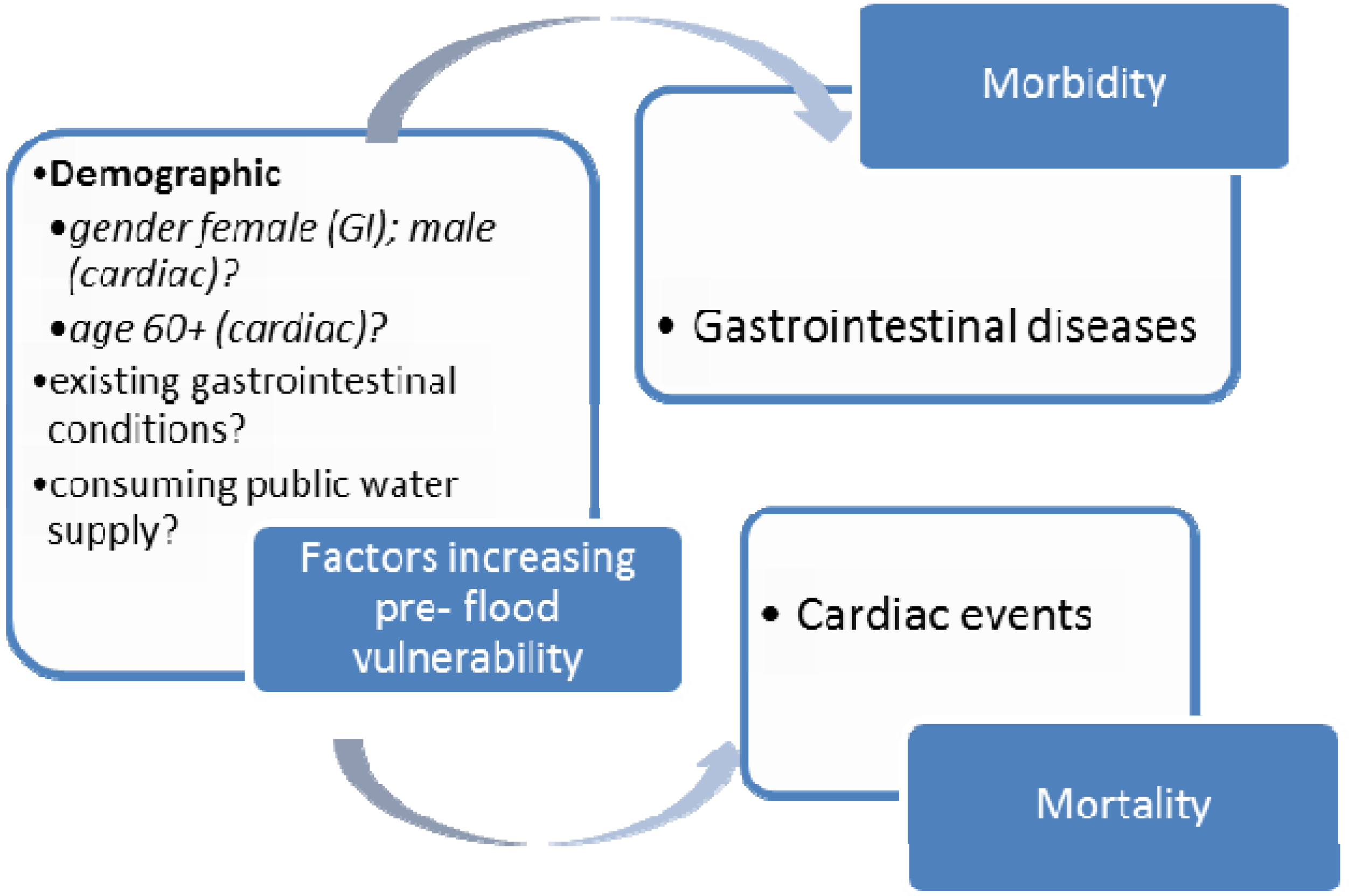
3.1. Health Effects Observed Pre-Flood
3.2. Pre-Flood Vulnerability Factors
3.2.1. Mortality
3.2.2. Morbidity
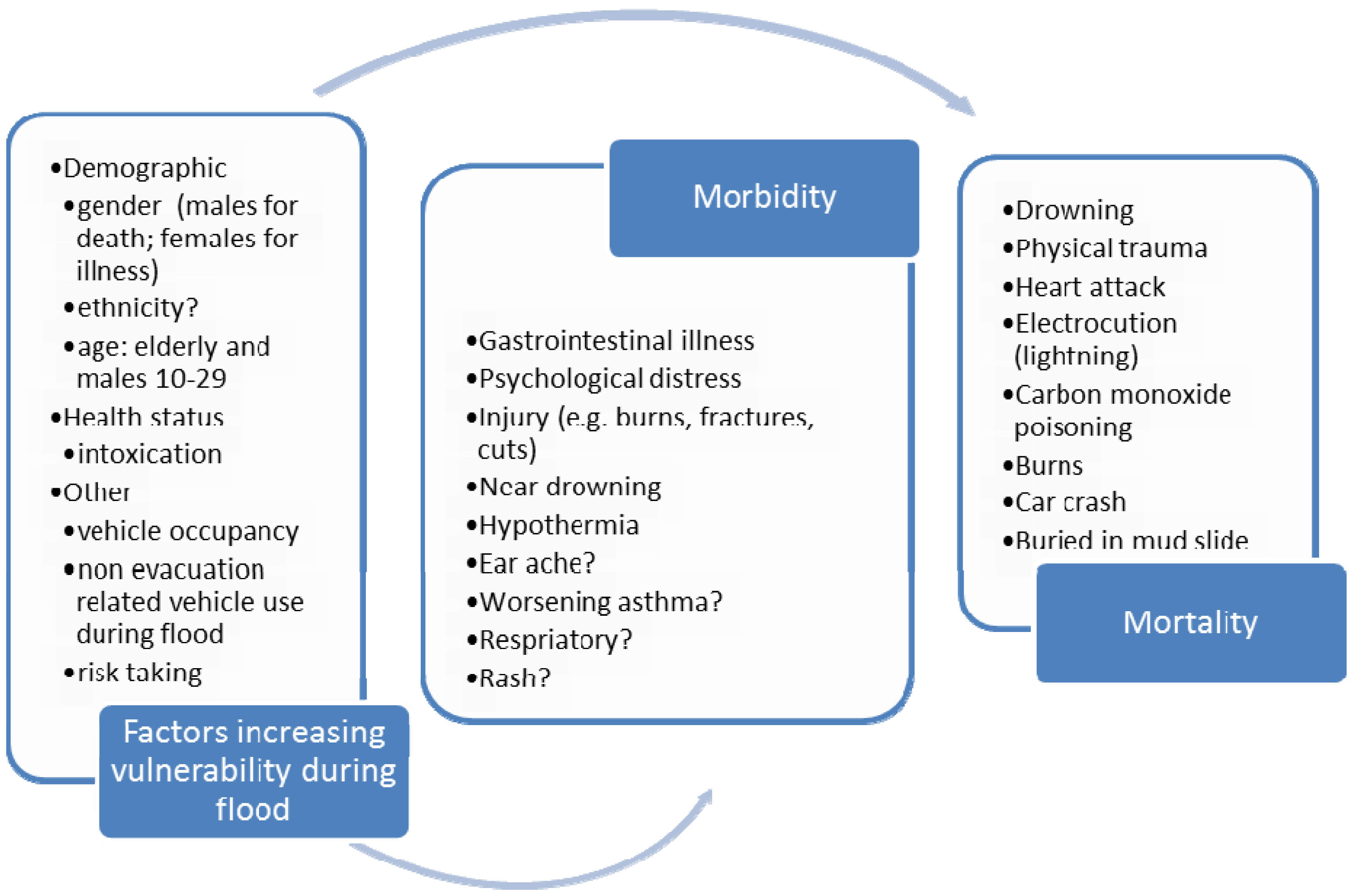
3.3. Health Effects Observed during Flood
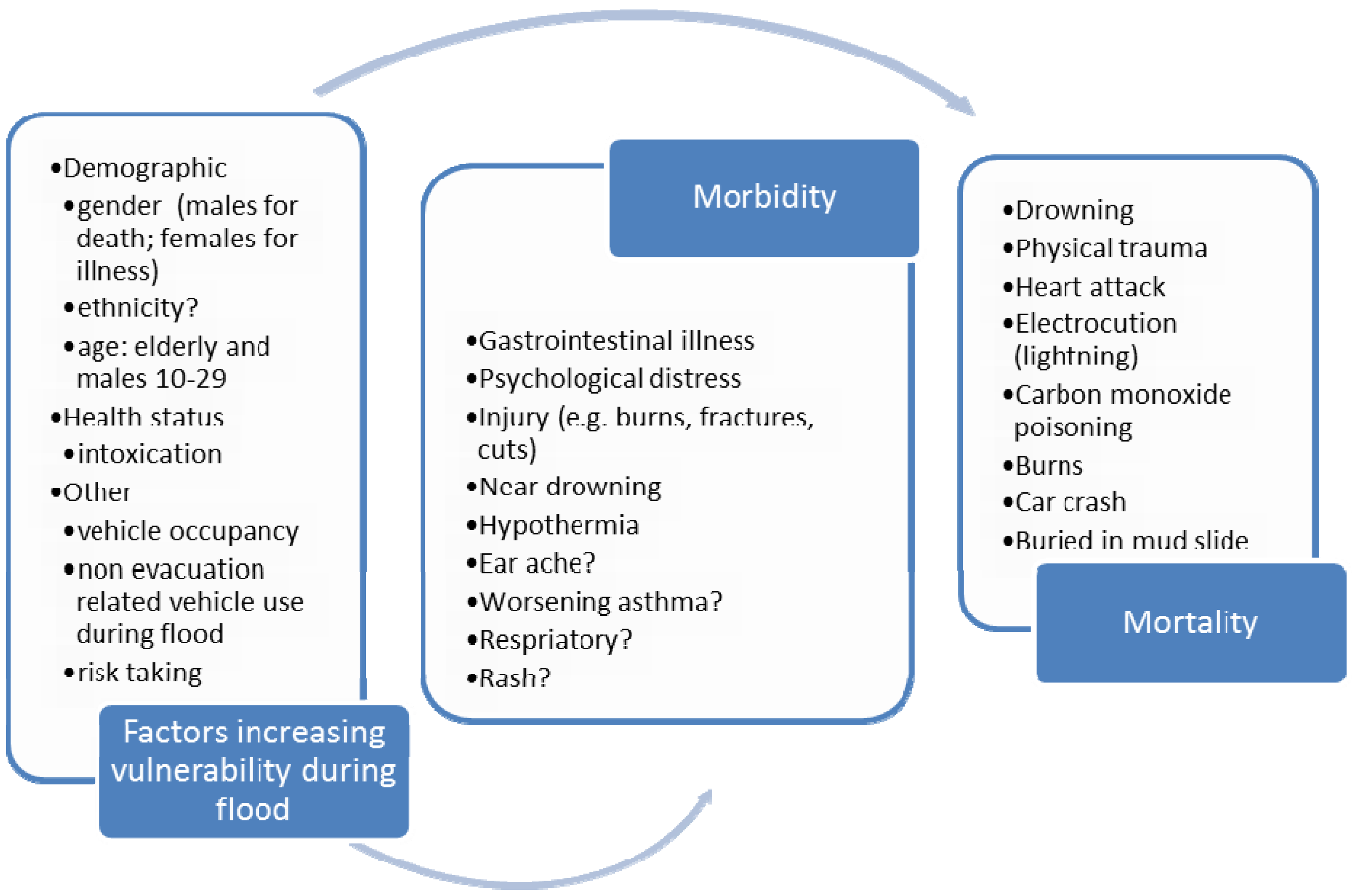
3.4. During-Flood Vulnerability Factors
3.4.1. Mortality
Gender and Age
Ethnicity
Other Factors
3.4.2. Morbidity
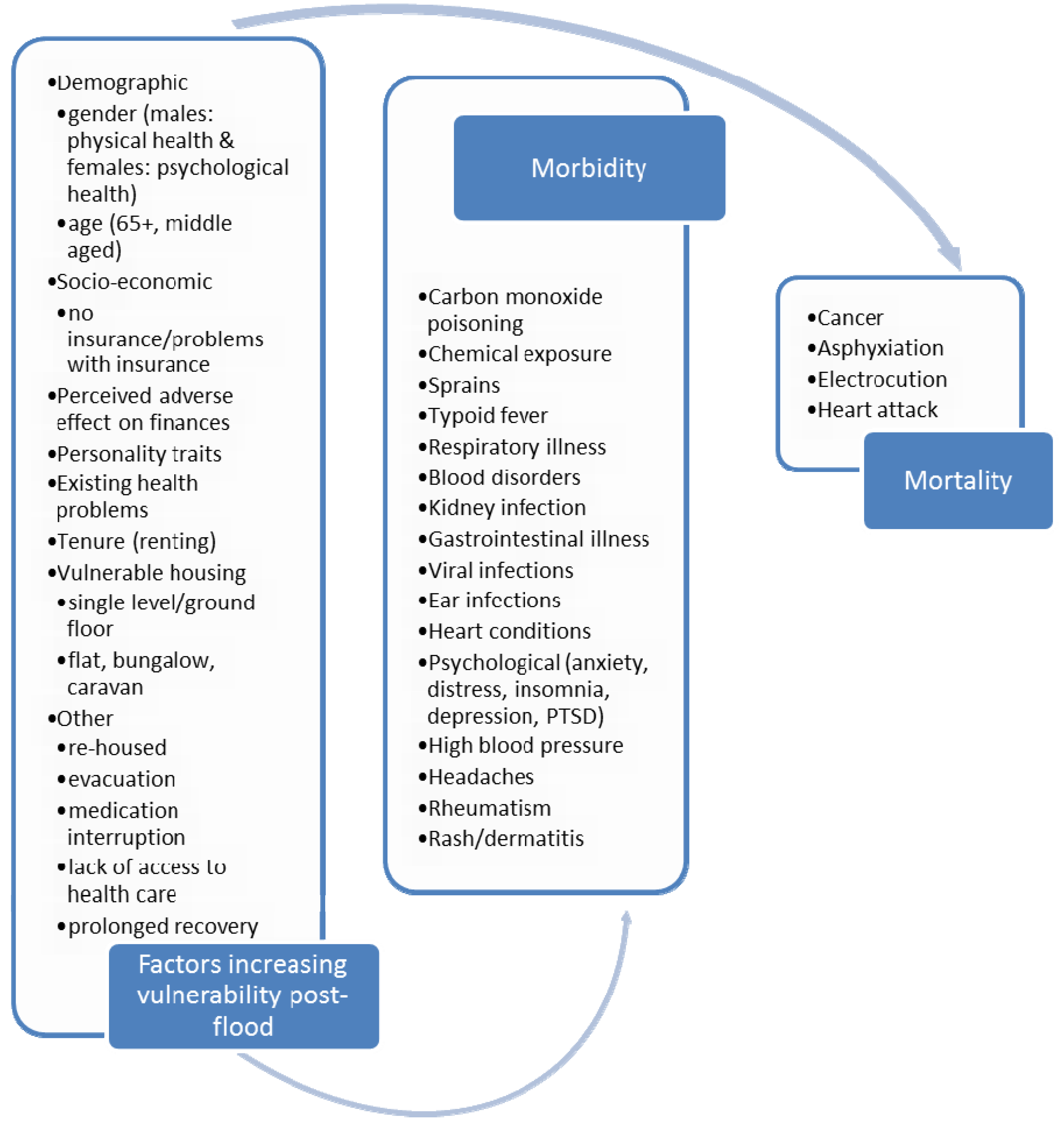
3.5. Health Effects Observed Short-Term (up to 3 Months) Post-Flood
3.6. Short-Term (up to 3 Months) Post-Flood Vulnerability Factors
3.6.1. Mortality
3.6.2. Morbidity
3.7. Health Impacts Observed Long-Term (3 Months Plus) Post-Flood
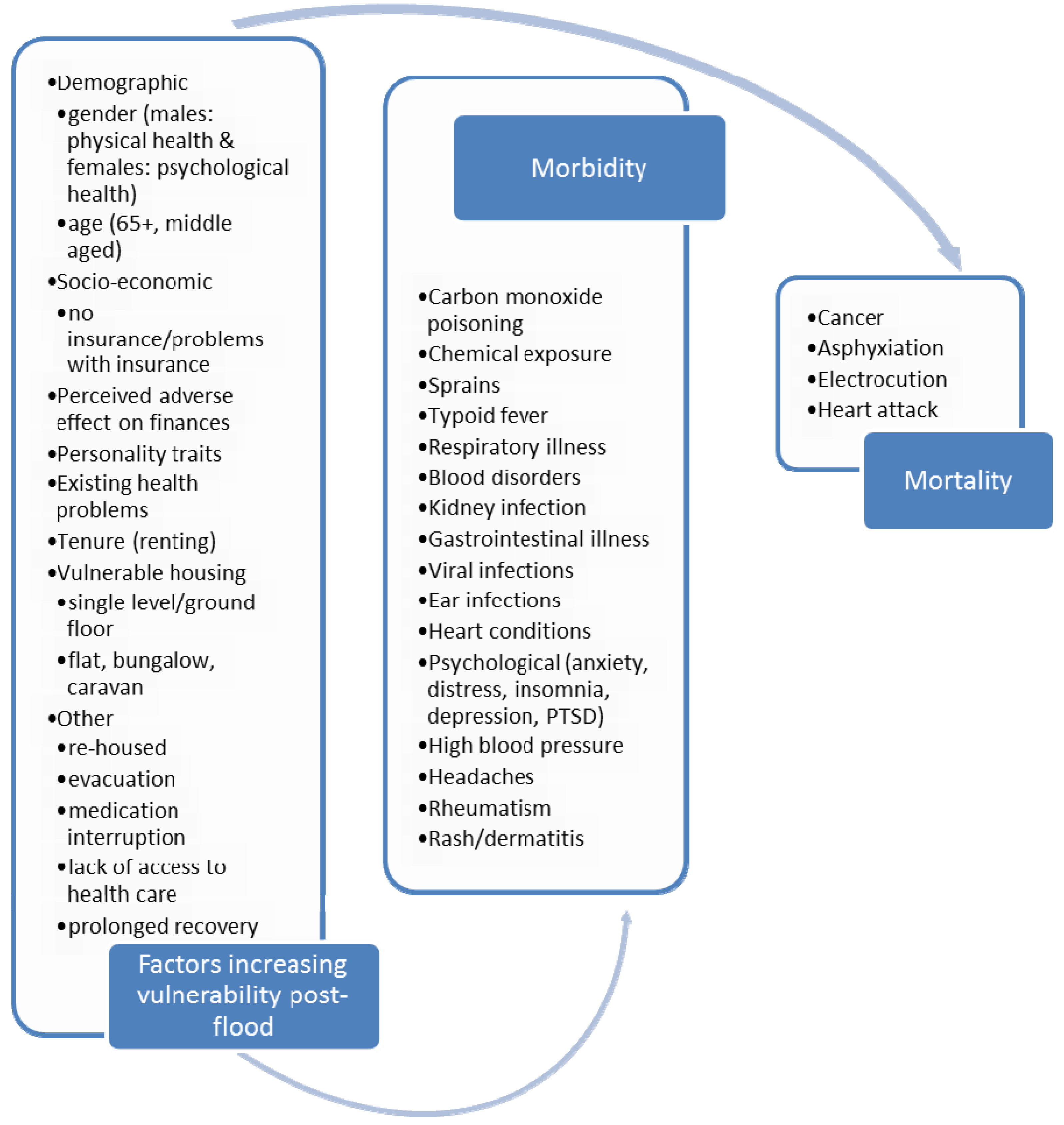
3.8. Long-Term (3 Months Plus) Post-Flood Vulnerability Factors
3.8.1. Mortality
3.8.2. Morbidity
3.9. Psychological Health
3.9.1. Degree of Flood Impact
3.9.2. Gender and Age
3.9.3. Location and Residential Status
3.9.4. Education and Socio-Economic Status
3.9.5. Existing Psychological Factors
3.9.6. Social Connectedness
3.9.7. Other
3.9.8. In Utero Flood Exposure
4. Discussion
5. Conclusions
Author’s Contributions
Acknowledgments
Conflicts of Interest
References
- Jonkman, S.N. Global Perspectives on Loss of Human Life Caused by Floods. Natural Hazards 2005, 34, 151–175. [Google Scholar] [CrossRef]
- Greenough, G.; McGeehin, M.; Bernard, S.M.; Trtanj, J.; Riad, J.; Engelberg, D. The potential impacts of climate variability and change on health impacts of extreme weather events in the United States. Environ. Health Perspect. 2001, 109 (Suppl 2), 191–198. [Google Scholar] [CrossRef]
- Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation; IPCC: Cambridge, UK, 2012.
- Diaz, J.H. Global climate changes, natural disasters, and travel health risks. J. Travel Med. 2006, 13, 361–372. [Google Scholar] [CrossRef]
- Du, W.; FitzGerald, G.J.; Clark, M.; Hou, X.Y. Health impacts of floods. Prehosp. Disaster Med. 2010, 25, 265–272. [Google Scholar]
- Dankers, R.; Feyen, L. Flood hazard in Europe in an ensemble of regional climate scenarios. J. Geophys. Res. 2009, 114. [Google Scholar] [CrossRef]
- Dankers, R.; Feyen, L. Climate change impact on flood hazard in Europe: An assessment based on high resolution climate simulations. J. Geophys. Res. 2008, 113. [Google Scholar] [CrossRef]
- Bankoff, G. Constructing vulnerability: The historical, natural and social generation of flooding in metropolitan Manila. Disasters 2003, 27, 224–238. [Google Scholar] [CrossRef]
- Aragón-Durand, F. Urbanisation and flood vulnerability in the peri-urban interface of Mexico City. Disasters 2007, 31, 477–494. [Google Scholar] [CrossRef]
- Castonguay, S. The Production of Flood as Natural Catastrophe: Extreme Events and the Construction of Vulnerability in the Drainage Basin of the St. Francis River (Quebec), Mid-Nineteenth to Mid-Twentieth Century. Environ. Hist. 2007, 12, 820–844. [Google Scholar] [CrossRef]
- Dutta, D.; Khatun, F.; Herath, S. Analysis of flood vulnerability of urban buildings and populations in Hanoi, Vietnam. Seisankenkyu 2005, 57, 338–342. [Google Scholar]
- Whittle, R.; Medd, W.; Deeming, H.; Kashefi, E.; Mort, M.; Twigger Ross, C.; Walker, G.; Watson, N. After the Rain—Learning the Lessons from Flood Recovery in Hull, Final Project Report for Flood, Vulnerability and Urban Resilience: A Real-Time Study of Local Recovery Following the Floods of June 2007 in Hull; Lancaster University: Lancaster, UK, 2010. [Google Scholar]
- Walker, G.; Burningham, K. Flood risk, vulnerability and environmental justice: Evidence and evaluation of inequality in a UK context. Crit. Soc. Policy 2011, 31, 216–240. [Google Scholar] [CrossRef] [Green Version]
- Adelekan, I. Vulnerability assessment of an urban flood in Nigeria: Abeokuta flood 2007. Natural Hazards 2011, 56, 215–231. [Google Scholar] [CrossRef]
- Christoplos, I.; Mitchell, J.; Liljelund, A. Re-framing risk: The changing context of disaster mitigation and preparedness. Disasters 2001, 25, 185–198. [Google Scholar] [CrossRef]
- Ashley, S.; Ashley, W. Flood Fatalities in the United States. J. Appl. Meteorol. Climatol. 2008, 47, 805–818. [Google Scholar] [CrossRef]
- Thacker, M.T.; Lee, R.; Sabogal, R.I.; Henderson, A. Overview of deaths associated with natural events, United States, 1979–2004. Disasters 2008, 32, 303–315. [Google Scholar] [CrossRef]
- Schnitzler, J.; Benzler, J.; Altmann, D.; Mucke, I.; Krause, G. Survey on the population’s needs and the public health response during floods in Germany 2002. J. Public Health Manag. Pract. 2007, 13, 461–464. [Google Scholar] [CrossRef]
- Duclos, P.; Vidonne, O.; Beuf, P.; Perray, P.; Stoebner, A. Flash flood disaster—Nimes, France, 1988. Eur. J. Epidemiol. 1991, 7, 365–371. [Google Scholar] [CrossRef]
- Staes, C.; Orengo, J.C.; Malilay, J.; Rullan, J.; Noji, E. Deaths due to flash floods in Puerto Rico, January 1992: Implications for prevention. Int. J. Epidemiol. 1994, 23, 968–975. [Google Scholar] [CrossRef]
- Wade, T.J.; Sandhu, S.K.; Levy, D.; Lee, S.; LeChevallier, M.W.; Katz, L.; Colford, J.M., Jr. Did a severe flood in the Midwest cause an increase in the incidence of gastrointestinal symptoms? Am. J. Epidemiol. 2004, 159, 398–405. [Google Scholar] [CrossRef]
- Tunstall, S.; Tapsell, S.; Green, C.; Floyd, P.; George, C. The health effects of flooding: Social research results from England and Wales. J. Water Health 2006, 4, 365–380. [Google Scholar]
- Tapsell, S.M.; Penning-Rowsell, E.C.; Tunstall, S.M.; Wilson, T.L. Vulnerability to flooding: Health and social dimensions. Philos. Transact. A Math. Phys. Eng. Sci. 2002, 360, 1511–1525. [Google Scholar] [CrossRef]
- Hubalek, Z.; Zeman, P.; Halouzka, J.; Juricova, Z.; Stovickova, E.; Balkova, H.; Sikutova, S.; Rudolf, I. Mosquitoborne viruses, Czech Republic, 2002. Emerg. Infect. Dis. 2005, 11, 116–118. [Google Scholar] [CrossRef]
- Handmer, J.; Smith, D. Health hazards of floods: Hospital admissions for Lismore. Aust. Geograph. Stud. 1983, 21, 221–230. [Google Scholar] [CrossRef]
- Strelau, J.; Zawadzki, B. Trauma and Temperament as Predictors of Intensity of Posttraumatic Stress Disorder Symptoms after Disaster. Eur. Psychol. 2005, 10, 124–135. [Google Scholar] [CrossRef]
- Norris, F.H.; Kaniasty, K.; Conrad, M.L.; Inman, G.L.; Murphy, A.D. Placing Age Differences in Cultural Context: A Comparison of the Effects of Age on PTSD after Disasters in the United States, Mexico, and Poland. J. Clin. Geropsychol. 2002, 8, 153–173. [Google Scholar] [CrossRef]
- Collins, T.W.; Jimenez, A.M.; Grineski, S.E. Hispanic health disparities after a flood disaster: Results of a population-based survey of individuals experiencing home site damage in El Paso (Texas, USA). J. Immigr. Minor. Health 2013, 15, 415–426. [Google Scholar] [CrossRef]
- Jimenez, A.M.; Collins, T.W.; Grineski, S.E. Intra-ethnic disparities in respiratory health problems among Hispanic residents impacted by a flood. J. Asthma 2013, 50, 463–471. [Google Scholar] [CrossRef]
- Heo, J.H.; Kim, M.H.; Koh, S.B.; Noh, S.; Park, J.H.; Ahn, J.S.; Park, K.C.; Shin, J.; Min, S. A prospective study on changes in health status following flood disaster. Psychiatry Investig. 2008, 5, 186–192. [Google Scholar] [CrossRef]
- Phifer, J.F. Psychological distress and somatic symptoms after natural disaster: Differential vulnerability among older adults. Psychol. Aging 1990, 5, 412–420. [Google Scholar] [CrossRef]
- Ginexi, E.M.; Weihs, K.; Simmens, S.J.; Hoyt, D.R. Natural disaster and depression: A prospective investigation of reactions to the 1993 midwest floods. Am. J. Community Psychol. 2000, 28, 495–518. [Google Scholar]
- Canino, G.; Bravo, M.; Rubio-Stipec, M.; Woodbury, M. The Impact of Disaster on Mental Health: Prospective and Retrospective Analyses. Int. J. Mental Health 1990, 19, 51–69. [Google Scholar]
- Steinfuhrer, A.; Kuhlicke, C. Social Vulnerability and the 2002 Flood: Country Report Germany (Mulde River); FLOODsite Report T11–07–08; UFZ: Leipzig, Germany, 2007. [Google Scholar]
- FitzGerald, G.; Du, W.; Jamal, A.; Clark, M.; Hou, X.Y. Flood fatalities in contemporary Australia (1997–2008). Emerg. Med. Australas 2010, 22, 180–186. [Google Scholar] [CrossRef]
- Coates, L. Flood Fatalities in Australia, 1788–1996. Aust. Geographer 1999, 30, 391–408. [Google Scholar] [CrossRef]
- Reacher, M.; McKenzie, K.; Lane, C.; Nichols, T.; Kedge, I.; Iversen, A.; Hepple, P.; Walter, T.; Laxton, C.; Simpson, J. Health impacts of flooding in Lewes: A comparison of reported gastrointestinal and other illness and mental health in flooded and non-flooded households. Commun. Dis. Public Health 2004, 7, 39–46. [Google Scholar]
- Bennet, G. Bristol floods 1968. Controlled survey of effects on health of local community disaster. Br. Med. J. 1970, 3, 454–458. [Google Scholar] [CrossRef]
- Milojevic, A.; Armstrong, B.; Kovats, S.; Butler, B.; Hayes, E.; Leonardi, G.; Murray, V.; Wilkinson, P. Long-term effects of flooding on mortality in England and Wales, 1994–2005: Controlled interrupted time-series analysis. Environ. Health 2011, 10. [Google Scholar] [CrossRef]
- Paranjothy, S.; Gallacher, J.; Amlot, R.; Rubin, G.J.; Page, L.; Baxter, T.; Wight, J.; Kirrage, D.; McNaught, R.; Palmer, S.R. Psychosocial impact of the summer 2007 floods in England. BMC Public Health 2011, 11. [Google Scholar] [CrossRef]
- Tomio, J.; Sato, H.; Mizumura, H. Interruption of medication among outpatients with chronic conditions after a flood. Prehosp. Disaster Med. 2010, 25, 42–50. [Google Scholar]
- Price, J. Some age-related effects of the 1974 Brisbane floods. Aust. N. Z. J. Psychiatry 1978, 12, 55–58. [Google Scholar] [CrossRef]
- Selten, J.P.; van der Graaf, Y.; van Duursen, R.; Gispen-de Wied, C.C.; Kahn, R.S. Psychotic illness after prenatal exposure to the 1953 Dutch Flood Disaster. Schizophr. Res. 1999, 35, 243–245. [Google Scholar] [CrossRef]
- Gordon, K.H.; Bresin, K.; Dombeck, J.; Routledge, C.; Wonderlich, J.A. The impact of the 2009 Red River Flood on interpersonal risk factors for suicide. Crisis 2011, 32, 52–55. [Google Scholar] [CrossRef]
- De Leo, D.; San Too, L.; Kolves, K.; Milner, A.; Ide, N. Has the Suicide Rate Risen with the 2011 Queensland Floods? J. Loss Trauma Int. Perspect. Stress Coping 2013, 18, 170–178. [Google Scholar]
- Norris, F.H.; Murphy, A.D.; Baker, C.K.; Perilla, J.L. Postdisaster PTSD over four waves of a panel study of Mexico’s 1999 flood. J. Trauma Stress 2004, 17, 283–292. [Google Scholar] [CrossRef]
- Krug, E.G.; Kresnow, M.; Peddicord, J.P.; Dahlberg, L.L.; Powell, K.E.; Crosby, A.E.; Annest, J.L. Retraction: Suicide after natural disasters. N. Engl. J. Med. 1999, 340, 148–149. [Google Scholar] [CrossRef]
- Jonkman, S.; Kelman, I. An analysis of the causes and circumstances of flood disaster deaths. Disasters 2005, 29, 75–97. [Google Scholar] [CrossRef]
- Duclos, P.; Isaacson, J. Preventable deaths related to floods. Am. J. Public Health 1987, 77, 1474. [Google Scholar] [CrossRef]
- Smith, J.K.; Young, M.M.; Wilson, K.L.; Craig, S.B. Leptospirosis following a major flood in Central Queensland, Australia. Epidemiol. Infect. 2012, 25, 1–6. [Google Scholar]
- CCDR. Waterborne Outbreak of Gastroenteritis Associated with a Contaminated Municipal Water Supply, Walkerton, Ontario, May–June 2000. Can. Commun. Dis. Rep. 2000, 26, 170–173. [Google Scholar]
- French, J.; Ing, R.; Von Allmen, S.; Wood, R. Mortality from flash floods: A review of national weather service reports, 1969–81. Public Health Rep. 1983, 98, 584–588. [Google Scholar]
- Cann, K.F.; Thomas, D.R.; Salmon, R.L.; Wyn-Jones, A.P.; Kay, D. Extreme water-related weather events and waterborne disease. Epidemiol. Infect. 2013, 141, 671–686. [Google Scholar] [CrossRef]
- Milojevic, A.; Armstrong, B.; Hashizume, M.; McAllister, K.; Faruque, A.; Yunus, M.; Kim Streatfield, P.; Moji, K.; Wilkinson, P. Health effects of flooding in rural Bangladesh. Epidemiology 2012, 23, 107–115. [Google Scholar] [CrossRef]
- Zaki, S.A.; Shanbag, P. Clinical manifestations of dengue and leptospirosis in children in Mumbai: an observational study. Infection 2010, 38, 285–291. [Google Scholar] [CrossRef]
- Socolovschi, C.; Angelakis, E.; Renvoise, A.; Fournier, P.E.; Marie, J.L.; Davoust, B.; Stein, A.; Raoult, D. Strikes, flooding, rats, and leptospirosis in Marseille, France. Int. J. Infect. Dis. 2011, 15, e710–e715. [Google Scholar] [CrossRef]
- Bhardwaj, P.; Kosambiya, J.K.; Desai, V.K. A case control study to explore the risk factors for acquisition of leptospirosis in Surat city, after flood. Indian J. Med. Sci. 2008, 62, 431–438. [Google Scholar] [CrossRef]
- Schmid, D.; Lederer, I.; Much, P.; Pichler, A.M.; Allerberger, F. Outbreak of norovirus infection associated with contaminated flood water, Salzburg, 2005. Euro. Surveill. 2005, 10. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=2727 (3 December 2013).
- Ivers, L.C.; Ryan, E.T. Infectious diseases of severe weather-related and flood-related natural disasters. Curr. Opin. Infect. Dis. 2006, 19, 408–414. [Google Scholar]
- Vanasco, N.B.; Fusco, S.; Zanuttini, J.C.; Manattini, S.; Dalla Fontana, M.L.; Prez, J.; Cerrano, D.; Sequeira, M.D. Outbreak of human leptospirosis after a flood in Reconquista, Santa Fe, 1998. Rev. Argent. Microbiol. 2002, 34, 124–131. [Google Scholar]
- Curriero, F.C.; Patz, J.A.; Rose, J.B.; Lele, S. The association between extreme precipitation and waterborne disease outbreaks in the United States, 1948–1994. Am. J. Public Health 2001, 91, 1194–1199. [Google Scholar] [CrossRef]
- Thomas, K.M.; Charron, D.F.; Waltner-Toews, D.; Schuster, C.; Maarouf, A.R.; Holt, J.D. A role of high impact weather events in waterborne disease outbreaks in Canada, 1975–2001. Int. J. Environ. Health Res 2006, 16, 167–180. [Google Scholar] [CrossRef]
- Griffith, D.C.; Kelly-Hope, L.A.; Miller, M.A. Review of reported cholera outbreaks worldwide, 1995–2005. Am. J. Trop. Med. Hyg. 2006, 75, 973–977. [Google Scholar]
- Tornevi, A.; Axelsson, G.; Forsberg, B. Association between Precipitation Upstream of a Drinking Water Utility and Nurse Advice Calls Relating to Acute Gastrointestinal Illnesses. PLoS One 2013, 8. [Google Scholar] [CrossRef]
- Hashizume, M.; Wagatsuma, Y.; Faruque, A.S.; Hayashi, T.; Hunter, P.R.; Armstrong, B.; Sack, D.A. Factors determining vulnerability to diarrhoea during and after severe floods in Bangladesh. J. Water Health 2008, 6, 323–332. [Google Scholar] [CrossRef]
- Health assessment of the population affected by flood conditions—Khartoum, Sudan. MMWR Morb. Mortal. Wkly. Rep. 1989, 37, 785–788.
- Guidance on Water Supply and Sanitation in Extreme Weather Events; UNECE/WHO: Copenhagen, Denmark, 2010.
- Doocy, S.; Daniels, A.; Murray, S.; Kirsch, T. The Human Impacts of Floods: A Historical Review of Events 1980–2009 and Systematic Literature Review. PLoS Curr. 2013. [Google Scholar] [CrossRef]
- Ahern, M.; Kovats, R.S.; Wilkinson, P.; Few, R.; Matthies, F. Global health impacts of floods: Epidemiologic evidence. Epidemiol. Rev. 2005, 27, 36–46. [Google Scholar]
- Floods in the WHO European Region: Health Effects and Their Prevention; WHO Regional Office for Europe: Copenhagen, Denmark, 2013.
- De Marchi, B.; Scolobig, A.; Delli Zotti, G.; Del Zotto, M. Risk Construction and Social Vulnerability in an Italian Alpine Region; Institute of International Sociology: Gorizia, Italy, 2007. [Google Scholar]
- Pelling, M. What determines vulnerability to floods; a case study in Georgetown, Guyana. Environ. Urban. 1997, 9, 203–226. [Google Scholar] [CrossRef]
- Brouwer, R.; Akter, S.; Brander, L.; Haque, E. Socioeconomic vulnerability and adaptation to environmental risk: A case study of climate change and flooding in Bangladesh. Risk Anal. 2007, 27, 313–326. [Google Scholar] [CrossRef]
- Kuhlicke, C.; Scolobig, A.; Tapsell, S.; Steinfuhrer, A.; De Marchi, B. Contextualizing social vulnerability: findings from case studies across Europe. Natural Hazards 2011, 58, 789–810. [Google Scholar] [CrossRef]
- Tapsell, S.; McCarthy, S.; Faulkner, H.; Alexander, M. Social Vulnerability to Natural Hazards; Flood Hazard Research Centre: London, UK, 2010. [Google Scholar]
- Thieken, A.; Kreibich, H.; Muller, M.; Merz, B. Coping with floods; preparedness, response and recovery of flood affected residents in Germany in 2002. J. Hydrol. Sci. 2007, 52, 1016–1037. [Google Scholar] [CrossRef]
- Haque, E. Perspectives of Natural Disasters in East and South Asia, and the Pacific Island States: Socio-economic Correlates and Needs Assessment. Natural Hazards 2003, 29, 465–483. [Google Scholar] [CrossRef]
- Fielding, J.; Burningham, K. Environmental Inequality and Flood Hazard. Local Environ. 2005, 10, 379–395. [Google Scholar] [CrossRef]
- Bubeck, P.; Botzen, W.J.; Aerts, J.C. A review of risk perceptions and other factors that influence flood mitigation behavior. Risk Anal. 2012, 32, 1481–1495. [Google Scholar] [CrossRef]
- Parker, D.J.; Priest, S.J.; Tapsell, S.M. Understanding and enhancing the public’s behavioural response to flood warning information. Meteorol. Appl. 2009, 16, 103–114. [Google Scholar] [CrossRef]
- Becker, G.; Aerts, J.; Huitema, D. Influence of flood risk perception and other factors on risk-reducing behaviour: A survey of municipalities along the Rhine. J. Flood Risk Manage. 2013. [Google Scholar] [CrossRef]
Appendix

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference Country | Study type Event Area of focus | Methods | Findings |
|---|---|---|---|
| Schnitzler, Benzler
et al. 2007 [18] Germany | Qualitative survey
Saxony flood 2002 Risk factors for health (diarrhea or injury) | Random survey of 477 flooded in 42 Saxony communities. Included an analysis of onset of diarrhea or injury during or immediately after flood. Univariate and multivariate analysis of exposures associated with onset of diarrhea or injury. Risk factors analysed were age (51+), gender (female), skin contact with floodwater, indoor living area flooded, cleanup involvement, consuming flood exposed food, drinking private water supply, consuming bottle water, mains water boiled/unboiled, water from tank). | During-flood: Thirty-two out of 465 (6.9%) had diarrhea during or shortly after the flood; 55 out of 472 (11.7%), had injuries. Multivariate analysis suggests exposures associated with onset of diarrhea were skin contact with floodwater (OR 5.8, 95%CI: 1.3, 25.1), being female (OR 3.9, 95%CI: 1.5, 10.0) and private water supply (OR 3.5, 95%CI: 1.2, 10.5), flooding indoors was significant for univariate only. A multivariate analysis showed that the risk for injuries was only significantly increased for skin contact with floodwater (OR 17.8, 95% CI: 2.4, 130.5), cleanup involvement and flooding indoors were significant for univariate only. Age was not a risk factor. |
| Steinführer & Kuhlicke [34] Germany | Qualitative survey
Mulde catchment flood August 2002 Risk factors for psychological and physical health | Survey of 404 households affected by the 2002 Mulde catchment flood carried out in five locations. Included a question on health effects both psychological and physical (not otherwise described). Collected social and demographic as well as flood-related risk factors. | During-floods: Among those flooded, those over 60 were at increased risk of evaluating both the psychological and physical consequences of floods significantly more often as “very bad”. The very old and very young varied in their perceptions significantly for psychological consequences; p < 0.05). Tenure, gender, and location were not significant predictors of psychological or physical consequences. |
| Staes, Orengo
et al. 1994 [20] Puerto Rico | Case-control study Puerto Rico floods 1992 Flood mortality | Descriptive study: time, place, and circumstances of death compared with water-level, rainfall and the timing of official warnings. Case control study: controls selected from the exposed population to estimate the risk of death by age, gender and vehicle occupancy during flood. | During-floods: Fatalities: 23; 20 were vehicle occupants and many died prior to official warning as water rose rapidly. Case control results: Gender or age did not alter the estimated mortality risk. Vehicle occupancy elevated mortality significantly [OR 15.9 (95% CI: 3.5, 144)] N.B control group had significantly less income than census details of exposed population and may not be representative exposed population ownership of cars. Vehicle occupancy to evacuate flash flood area was protective; other reasons for vehicle occupancy increased the risk of mortality. Blood alcohol content was positive for 12/16 adult deaths: 5 exceeded 0.1%. |
| Wade, Sandhu
et al. 2004 [21] US | Prospective longitudinal cohort
Severe flooding in the midwestern United States April and May of 2001 Examined rates of gastrointestinal illness during the flood, stratified for sensitive groups and whether contact with floodwater was associated with increased risk of gastrointestinal illness | Randomized trial of in-home drinking water treatment (the Water Evaluation Trial or “WET” Study) underway at the time of the flooding. Participants completed daily diaries detailing their incidence of gastrointestinal symptoms. 456 households (1,296 persons) were enrolled, and follow-up was for 1 year. A total of 1,110 of 1,118 subjects in the WET cohort who completed the flood survey provided health data, 143 (13%) reported some type of direct (e.g., walking through floodwater) or indirect (e.g., clean up floodwater contaminated items) contact with floodwater. Data was stratified in the models by age (≤12 years and ≥50 years), frequency of gastrointestinal symptoms in past year, and the presence of an existing chronic gastrointestinal condition to examine whether the impact of the flood was greater in certain potentially sensitive groups. | During-flood: Crude rates, of both gastrointestinal symptoms and diarrhea, were higher during the flood, than the rates for winter. Rates of gastrointestinal symptoms and diarrhea among, participants were higher in winter compared to other seasons. Adjusted rates of highly credible gastrointestinal symptom episodes were 1.29 times higher during the flood, than during the rest of the follow-up period (95 % CI: 1.06, 1.58). Post-flood: Numbers of diarrhea episodes, as well as hospitalizations, for gastrointestinal conditions were non-significantly elevated. Doctor’s visit for diarrhea; days of missed work or school due to gastrointestinal symptoms; and days of vomiting were all non-significant. Six participants were hospitalized for a total of 29 days for gastrointestinal conditions. Among those ≤12 years, the presence of a septic tank on the home property was not associated with elevated incidence rate ratios (IRRs) of gastrointestinal symptoms, and although any type contact with floodwater or flood-contaminated items was associated with elevated IRR of gastrointestinal symptoms, this association was significant only for those who participated in flood cleanup (IRR 1.40, 95% CI: 1.07, 1.82) or whose house or yard was flooded (IRR 2.42, 95% CI: 1.22, 4.82). For the ≥50 years old, any flood contact had higher symptoms (IRR 1.46, 95%CI: 0.65, 3.27) and as did those whose homes or yards had been flooded (IRR 6.20, 95%CI: 3.34, 11.51). Among those ≤5 years any flood contact was associated with credible gastrointestinal symptoms (IRR 3.18, 95%CI: 1.79, 5.66). The effect of the flood was more severe among persons self-rating health as poor, fair, or good; and those with frequent gastrointestinal symptoms (such as irritable bowel syndrome), particularly for severe gastro illness. There was no evidence that gastrointestinal symptoms increased in those who consumed public water nor was there evidence of a dose response relationship. |
| Tunstall, Tapsell
et al. 2006 [22] England and Wales | Qualitative study
England and Wales Floods 30 locations from 1998 to 2002 Health and psychological effects of floods and the gender, age, socio-economic predictors | Surveys conducted on flooded sample (983 adults 18+ years whose homes had been flooded above floor level) compared with at risk sample (527 residents 18+ in the same areas but who did not experience flooding) general health questionnaire (GHQ-12); post-traumatic stress scale (PTS); self-reported health effects checklist. | Post-flood: Suggests that among the flooded risk factors for worse psychological health (GHQ12 scores) were female gender; poorer prior health; problems with insurers/being uninsured; evacuation; longer time to recovery; contamination by floodwater; living in rental property and less warning time. Among the flooded risk factors for PTS were female gender; poorer prior health; being younger than 65; problems with insurer; deeper water; vulnerable housing; contamination by floodwater; less warning time; evacuation; and longer recovery. |
| Duclos, Vidonne
et al. 1991 [19] France | Case study (included an injured uninjured case control comparison) Nîmes flood 1988 Flood-health effect (mortality, injury and disease). Age only | Assessed overall flood-health impact by data on medical care delivery & surveillance of infectious diseases. Survey of 108 families (228 persons). Describes 1) the factors that limited mortality, 2) the reaction of the population to the disaster, & 3) the health effects during the impact & post-impact phases of the disaster. | During-flood: Among flooded respondents, average age similar for those injured 46.4 years compared with 48 years for all respondents. |
| Tapsell, Penning-Rowsell
et al. 2002 [23] England | Qualitative Northeast England floods June 2000 Health effects of flooding & vulnerability mapping | Focus groups 3 to 4 months after floods to determine the health effects of the flood. Developed an index to measure the impact floods may have on communities using SFVI (a composite additive index based on 3 social indicators: age, lone parents, & pre-existing health problems & 4 financial indicators, non-home owners, unemployed, non-car owners, and overcrowding). | Post-flood: Reported health problems: blood disorder; chest infections /asthma /coughs /colds /flu /pleurisy; kidney infection; diarrhea/ vomiting/ upset stomachs; headaches; high blood pressure; skin irritations/rashes/ spots; panic attacks; swollen glands; throat and ear infections /laryngitis; viral infections Using SFV1, populations can be categorized into bands of: 1) low 3) average & 5) high vulnerability. Maidenhead flood plains are populated by relatively affluent communities with slightly lower average SFVI values than in the surrounding areas. Manchester flood plains are much more vulnerable to flooding than Maidenhead, with a large, vulnerable community in the southwest of the flood-plain area. More research is needed to determine the accuracy of SFVI scores at predicting actual vulnerability to flooding. |
| Hubalek, Zeman
et al. 2005 [24] Czech Republic | Case series
Czech floods 2002 Screened the human population of the flooded area to estimate the risk for infections with mosquito-borne viruses | Specimens from residents (N = 497) of an area in the Czech Republic affected by the 2002 flood were examined serologically for mosquito-borne Tahyna (TAHV), Sindbis (SINV), Batai (BATV) viruses, and West Nile (WNV) viruses. Determined the difference in rates based on 4 zones, proximity to flooded areas, gender and age. | Post-flood: Antibodies were detected against Tahyna (TAHV) (16%), Sindbis (SINV) (1%), and Batai (BATV) (0.2%) viruses, but not West Nile (WNV) viruses. Association found with decreasing distance from floodplain and increasing prevalence of TAHV seroconversion (χ2 = 8.51; p = 0.003) for Zones A, B and C. The highest TAHV seroprevalence in zone A (28%), lower seroprevalences in zones B and C, and 5% in the control zone D (χ2 = 14.57; p = 0.002). There were no differences in TAHV seroprevalence based on gender, (15.8%) males and (16.9%) females (χ2 = 0.11; p = 0.744). The prevalence of TAHV increased significantly with increasing age (χ2 = 39.809; p <0.001). Four cases of TAHV were observed in testing, but not corroborated by GP (suggesting mild symptoms). No recent cases of infection to WNV, SINV, and BATV viruses were observed in study. |
| Handmer & Smith 1983 [25] Australia | Comparison
Flooding in Lismore Australia, 1974 Hospital admission and mortality risks associated with flooding | Used data from hospital admission and death certificates and from an earlier survey. Compared mortality and hospital admissions before and after the flood; and differential health effects by level of flood and gender; included residents outside flood plain. | Post-flood: there were gender differences among the severely flooded, admissions doubled for males, while female admissions halved. |
| Strelau, Zawadzki
et al. 2005 [26] Poland | Cross-sectional Great Polish Flood (Southern Poland) in 1997; Northern Poland floods in 2001 Post-traumatic stress (PTS) disorder predictors | Four studies of flood victims (562/1041 were female). We focus here only on those flooded (study included other disaster events). Post-traumatic stress disorder symptoms (PTS-Factorial Version inventory) were measured at varying time points (3, 15 months, or 3 years after flooding). Slight differences in methods between studies, however common measures included Trauma Intensity index, which examined threat to life during the flood, injuries of the body, and material damage. Prolonged trauma consequences index including financial problems; problems with housing; and decline in SES after the flood. Temperament Inventory comprised six scales: Briskness, Perseveration, Sensory Sensitivity, Endurance, Emotional Reactivity and Activity. | Post-flood: Among those who experienced floods, PTS scores decreased between a few weeks to two years after trauma. Of the traits, emotional reactivity and perseveration positively correlated with intensity of PTS symptoms however, briskness, endurance, and activity were negatively correlated. Sensory sensitivity did not count, when the first measure of PTS was taken into account, but at two years after flood this temperament trait correlated negatively with PTS. For all time points (3 months, 15 months, or 3 years after flooding) trauma and emotional reactivity were the strongest predictors of intensity of PTS symptoms experienced during the flood. Predictors PTS intensity symptoms at 3 years post-flood were emotional reactivity and prolonged trauma consequences of flooding and there was evidence of an interaction between the two predictors explaining, the variance of PTS symptoms. |
| Norris, Kaniasty
et al. 2002 [27] Poland | Cross-sectional
Flooding in Poland 1997 Post-traumatic stress disorder (PTS using a 30-item Revised Civilian Mississippi Scale) and effect of age | Purposeful sample of flood- affected. Symptoms of post-traumatic stress disorder (PTS) were measured (6–12 months) post-flood (n = 285). NB study also looked at impact of hurricanes in US and Mexico but this is beyond the scope of this review. | Post-flood: Women reported significantly more symptoms than men (t = 5:22, p ≤ 001). Symptoms increased as trauma increased (t = 6:51, p ≤ 001) and increased with decreasing education (t = 3:98, p ≤ 001). Among those flooded, there was a linear and positive relation with PTS with older people being most distressed. |
| Collins, Jimenez
et al. 2013 [28] US | Cross-sectional survey (retrospective) Flooding in El Paso County, Texas US, 2006 Physical health, mental health and injury post-flood and logistic regression of independent variables | Surveyed, by mail 475 individuals, whose homes were flood damaged four months following flood event. Ten independent variables including: flood exposure (serious home damage, adverse event experiences), gender, age, socio-economic status, access to medical care, Hispanic ethnicity, US citizenship status, foreign-birth, and English-language proficiency. | Post-flood: Survey respondents had high rates of physical (43%) or mental (18%) health problems in the 4 months post-flood and 28% had one or more injury, or acute effect, related to post-flood cleanup. Common physical health problems included allergies, throat irritations/coughing/wheezing, headaches and nose/eye/skin irritations. Mental health problems included depression (17%) and PTS (8.6%). Injuries and acute effects, related to cleanup, were stiffness/ soreness, strained muscles and bruises/ sprains/ abrasions. Negative physical and mental health outcomes post-flood, were associated with adverse event experiences, older age, lower socio-economic status, lack of access to healthcare, non-US citizenship and English proficiency. Hispanic ethnicity was associated with physical health. Native-birth was associated with mental health. Adverse event experiences, older age, lower socioeconomic status and more serious home damage were significant risk factors for clean-up injuries. Flooding resulted in higher negative health effects among people more exposed, poorer, older, and with less resources. Hispanic ethnicity and a lack of US citizenship were associated with higher risks of health effects, being English-deficient appears to be protective against physical and or foreign-born protective for mental health effects of floods. |
| Jimenez, Collins
et al. 2013 [29] US | Cross-sectional survey (retrospective)
Flooding in El Paso County, Texas US, 2006 Respiratory health and relationship with age, gender, SES, mold exposure, family conflict, English-language proficiency and US citizenship status among those with Hispanic ethnicity | 4 years post-flood retrospective mail-out survey assessed respiratory health effects for 363 people (176 households), who self-identify Hispanic ethnicity and whose homes were damaged by flood. Analysis of respiratory health and the relationship with age, gender, SES, mold exposure, family conflict, English-language proficiency and US citizenship status, among those with Hispanic ethnicity, was assessed, using logistic regression. | Post-flood: Among Hispanic respondents 41% had one or more post-flood respiratory illnesses. Significant associations with respiratory illness were observed among Hispanic respondents with lower income (OR: 0.53 95%CI: 0.36, 0.78), exposed to mold (OR: 2.27, 95%CI: 1.56, 3.29), or increased family conflict (OR: 1.45, 95%CI: 1.05, 2.01), with greater English-language proficiency (OR: 4.02, 95%CI: 1.91, 8.50) or lacking US citizenship (OR: 13.11, 95%CI: 1.75, 98.33). Gender (female OR: 1.36 (95% CI: 0.75, 2.46) and age (under 15 years OR: 1.30 (95%CI: 0.68, 2.47); over 64 years OR: 0.64 (95%CI: 0.17, 2.38)) were not significant factors for post-flood respiratory illnesses. |
| Ginexi, Weihs
et al. 2000 [32] US | Prospective cohort study before and after floods Flood Iowa US 1993 (Midwest floods) Depression (CES-D scale) and socio-demographic modifiers pre and post-flood among those exposed to flood effects and those unexposed to flood impact | 2379 people (over 18 years) were randomly sampled and assessed 1 year, pre- flooding. 1735 people were assessed 30 to 90 days post-flooding. 893 respondents were impacted. Risk factors for depression, including age, gender, education, marital status, race and income, and community size, were sought during telephone interviews. Those, who were not followed up, were more likely to be male, never married, with slighter lower SES, depressed pre-flood, and reside in non-farm, rural communities. While the means and variances were affected by attrition, the overall relationship between independent variables and depression were not. | Post-flood: significant predictors of post-flood depression included pre-flood depression (OR 8.6, 95%CI: 5.54, 13.21), flood impact level (OR 1.10, 95%CI: 1.02, 1.18), age (OR 0.98, 95%CI: 0.96, 0.99), income (OR 0.84, 95%CI: 0.76, 0.94) and those separated or divorced (relative to those married p˂0.001). Multiplicative interactions were observed for elevated post-flood depressive symptoms among males, those with lower SES, and residents of small towns and rural nonfarm communities. Although flood impact levels were significantly higher among farm residents, it was small communities without farms that had high rates of depression. |
| Heo, Kim
et al. 2008 [30] Korea | Prospective before and after study
Flood July 15th, 2006, Korea (Garisan-ni, Inje-gun, Gangwon-do) Health (SF-36); depression (Beck Depression Index) post-traumatic stress disorder (Minnesota Multiphasic Personality Inventory and the Revised version of the Korean Impact of Event Scale) | A brief survey of 83 subjects was completed two weeks prior to floods. A follow-up post-flood (18 months) survey sought data from 58 of the original subjects on: general health status, depression, PTS, and potential predictors and confounders of mental health outcomes. Survey included: demographic data, (age, gender, and marital status) of the respondents. | Post-flood: 6 of the original subject, died due to flood. At follow-up, 53% respondents were, at least, mildly depressed and 17% had severe depression, 22.41% had PTS (as measured by both the IES-R and MMPI-PTS). Of the eight SF-36-K health status categories, physical functioning, role limitation due to emotional conditions, social functioning, and bodily pain were impaired post-flood. General health, role limitation due to physical conditions and vitality were improved post-flood. Logistic regression of the 64% who had deteriorated health post-flood (a reduction of 1 or more in SF-36K), suggests factors associated with this reduction included previous experience of a number of disaster events and those with a score indicating more than mild depression on the BDI. Demographic characteristics increasing risk of deterioration in health post-flood included being a non-smoker or non-drinker, younger, male, married, or having higher educational level or income. |
| Phifer 1990 [31] US | Prospective before and after cohort study Flooding in southeastern Kentucky US, 1984 Examined effect of age, gender, marital status, occupational status, education level, pre-flood anxiety, depression, well-being and general health before and after flood | 200 adults (55 years and older) were interviewed before and after flood to determine differential vulnerability to increases in psychological and physical symptoms by age, gender, marital and occupational status, education level, and pre-flood symptom levels anxiety (State -Trait Anxiety Inventory), depression (Center for Epidemiologic Studies Depression Scale); well-being (General Well-Being Scale) and general health (from a revised 20-item self-report scale of functional health and specific ailments) before and after flood. Follow-up was 18 months. | Post-flood: Flood-impacted (i.e., those respondents reporting personal losses) and unexposed groups were similar on distributions of sex, education, occupational status, marital status and pre-disaster symptoms. The only significant difference was in terms of age distribution, where the age 65-74 group was under-represented among the impacted group χ2 (N = 222) = 5.14, p < 0.03). The flood had effects on anxiety, depressive and physical symptoms, when measured at 16-18 months post-flood. Risk factors for psychological symptoms post-flood were being male, lower occupational status and those 55–64 years. Socio-demographic factors do not appear to increase risk, of deterioration of physical health, post-flood. |
| Canino 1990 [33] Puerto Rico | Prospective cohort study, before and after floods, un-impacted served as controls; combined with retrospective cohort Flooding and landslides Puerto Rico 1985 Mental health (major depressive episode, dysthymia, post- traumatic stress disorder (PTS), alcohol and drug abuse/or dependence (DAD), generalized anxiety (GA), panic, and antisocial personality disorder (ASP)) Diagnostic Interview Schedule/Disaster Supplement (DIS/DS) | 912 interviews post-flood (375 were prospective sample and 537 retrospective sample). Note that PTS, GA, DAD, and ASP was not assessed in 1984; so no pre-flood comparison is available for these outcomes. Interviews were conducted in 1887, flood occurred in 1985). 77 of the prospective sample were exposed to the flood (significantly more males exposed than females), half retrospective sample were exposed to the flood. In both samples, the exposed were significantly less educated than the unexposed, but did not differ on other characteristics. | Post-flood: New symptoms could not be explained by risk factors, such as, sex, age, education, and previous symptoms. |
| Reference Country | Study type Event Area of focus | Methods | Findings |
|---|---|---|---|
| FitzGerald, Du
et al. 2010 [35] Australia | Historical case series Australian floods (1997–2008) Deaths (demographic only- age and gender) | Flood fatality data in Australia (1997–2008), derived from newspapers & historic accounts, government & scientific data on the date, location, age, gender & cause of death. | During-flood: 73 deaths. Gender: males 71.2%. Age: those between 10–29 and 70+ years are over represented among those drowned (not comparative with source populations). Cause: 48.5% fatalities related to motor vehicle use, 26.5% fatalities occurred as a result of inappropriate or high-risk behaviour during floods (i.e., swimming in or trying to surf in flooded water ways); 16% were associated with crossing in flooded water ways. |
| Thacker, Lee
et al. 2008 [17] US | Cross-sectional study of deaths Summary of mortality reports from 1979–2004, Overview of deaths from all natural events (report here on flood-related), in United States, demographic vulnerability, ethnicity, gender and age | Using National Center for Health Statistics (NCHS) Compressed Mortality File crude death rates were calculated by dividing the number of condition-specific deaths by the 2000 US census population and converting the rate to per million people. Demographic characteristics of the groups affected are described by age, race, gender, geographic location & year of death. | During-flood: 2,741 of the 21,491 (13%) deaths, due to natural events are from storms and floods. Crude death rates did not vary between race and gender. Highest death rates were among those 55+. All age categories had a death rate of less than one per million. |
| Coates 1999 [36] Australia | Historical case series report Flooding events between 1788 and 1996 Flood deaths | Flood fatalities in Australia compiled from sources; activity of death and death rates in year age intervals, from 0 ± 4 years up to 85 years and older. Population figures were used to calculate a death rate per 100,000 population. The total fatalities, within the population, were divided by the annual, 10, or 50 year average annual population figure for that group. | During-flood: From 1788 to September 1996 at least 2,213 flood deaths occurred in Australia. For 1,513 fatalities, gender was reported, 80.6 per cent were male. Increase in fatalities among those 59+ & less than 25 years & slight increase in 35–54 age group. The vast majority of female fatalities were in the 80–84 age group. 1947 to 1996 data show a general increase in male fatalities with age, particularly middle-age males (35–54 years). Most fatalities are from attempting to travel across floodwater (38.5%), being inside a building or campsite (31.5%) or attempting to rescue someone/something else. |
| Ashley & Ashley 2008 [16] US | Review of case series US all floods from 1959–2005 Mortality by activity; location and demographics | Review of database of 1959–2005 flood-related fatalities compiled from the National Climatic Data Center’s (NCDC) Storm Data. Included data on: flood event type, year, season and state; activity/location surrounding the incident and demographics (age and gender) of a total of 4,586 flood-related fatalities in United States. Study only included those fatalities directly attributed to floodwater (and not those indirect e.g., carbon monoxide poisoning). | During-flood: Av. /year 97.6, flood-related fatalities (median value 81/yr). Suggests 10–29 and 60+ years are most vulnerable to flood-related deaths and this is higher statistically relative to the percent of the U.S. population (United States Census Bureau 2000). Those 30–59 years appear less vulnerable to flood-related fatality relative to the percent of the U.S. population. Males comprised the majority of flood fatalities (where gender was known) and among them, 35% were 10–29 years. However, age was not known in 63% of fatalities, while for 49%, gender was unknown. Of flood-deaths, 64% were attributed to an activity or location of occurrence; of these, 63% were vehicle related, 19% in/on permanent structures or outside or alongside the flood (i.e., accidental), 9% were intentionally inside flood-water (of these, 12+ years: 43% walked through floodwaters to evacuate, or reach car/house; 16% entered floodwater to help others). |
| Reference Country | Study type Event Area of focus | Methods | Findings |
|---|---|---|---|
| Duclos, Vidonne
et al. 1991 [19] France | Case study (inc. injured uninjured case control comparison) Nîmes flood 1988 Flood-health impact (mortality, injury and disease) Age only | Assessed overall flood-health impact by data on medical care delivery & surveillance of infectious diseases. Survey of 108 families (228 persons). Describes: (1) factors that limited mortality, (2) reactions of the population to the disaster, (3) health effects during the impact & post-impact phases of the disaster. | Pre-flood: No incidence of death During-flood: Fatalities: 9 (drowning, 2 rescuers) Injuries: 3 severe (1 burns, 1 fractured leg. 1 broken arm; 2 hypothermia; 3 near drowning; & 10 minor injuries Post-flood: No deaths; 12 twelve cases of carbon monoxide poisonings; 3 chemical exposures and few sprains. 2 cases of typhoid fever were confirmed by culture, suspected waterborne, unlinked regionally. Survey results: 32% had flood-related health problems; of these 59 reported stress-related problems (insomnia/ anxiety); other health problems included: influenza, bronchitis, rhinitis, sinusitis & rheumatism. Only 2% with routine scheduled medical treatments or drug prescriptions, experienced flood-related difficulty obtaining medical care. |
| Reacher, McKenzie
et al. 2004 [37] England | Cohort study Qualitative Lewes flood 2000 Heath effects of flooding | 103 flooded households (227 residents) and 104 non-flooded households (240 residents) in same area randomly selected for the survey. Interviews took place, over the phone, 9 months after flood. | Post-flood: Flooding was associated with earache (RR 2.2 [95%CI: 1.1, 4.1]), and a significant increase in risk of gastroenteritis with depth of flooding (RR 1.7 [95%CI: 0.9, 3.0]). For flooded adults risk of worsening asthma (RR 3.1 [95% CI: 1.2, 4.4]) and distress (score more than 4 on GHQ-12) (RR 4.1 [95%CI: 2.6, 6.4]) were higher than non-flooded. Weaker associations were observed for skin rash (RR 3.4 [0.8, 15] p = 0.1), respiratory illness (RR1.3 [0.8, 2.1] p = 0.32) and all categories of injury (RR 1.6 [0.9, 2.8] p = 0.14) (table 2). Sprains, broken bones, burns or scalds, and inhalation of gas, smoke or vapours were reported by flooded and non-flooded individuals. Among the respondents with pre-existing asthma, a non-significant association was observed (RR 1.9 [0.8, 4.2] p = 0.13) for worsening asthma. Associations between flooding and new episodes of physical illness in adults diminished after adjustment for psychological distress. Flooding remained highly significantly associated with psychological distress after adjustment for physical illnesses. |
| Tunstall, Tapsell
et al. 2006 [22] England and Wales | Qualitative study England and Wales Floods 30 locations from 1998 to 2002 Health and psychological effects of floods and the gender, age, socio-economic predictors | Surveys conducted on flooded sample (983 adults 18+ years whose homes had been flooded above floor level) compared with at risk sample (527 residents 18+ in the same areas, but who did not experience flooding) general health questionnaire (GHQ-12); post-traumatic stress scale (PTS); self-reported health effects checklist. | During-flood: Up to 64% had a score of 4+ on GHQ-12 (psychological distress). Post-flood: Psychological effects were much more common after flooding than physical ones, with the most frequently mentioned symptoms being anxiety when it rains; 25% respondents experienced deterioration of health (10% gastrointestinal illness; 9% joint stiffness; 8% respiratory illnesses; 7% high blood pressure and 6% skin conditions) Significant differences between GHQ-12 scores for flooded and those at risk for all age groups except those 60+ years; differences were significant for gender, social class, length of residence (5 years). Gender and age effect was also seen when compared with national average GHQ-12 scores. More than 2/5 flooded perceived the flood as a traumatic event. 15% had mild- moderate PTS; 10 individuals had high and 4 had extreme. |
| Bennet 1970 [38] England | Controlled survey before and after study Bristol flood 1968 Deaths, hospital referrals and admissions and GP attendance compared with a year prior to floods and following flood. Demographic and social class vulnerability | A comparison was made between people who had been flooded and people who had not, with regard to surgery attendances, hospital referrals and admissions, immediately following the flood, regarding the year before and again the year after. A controlled survey of number of deaths, from flood affected addresses, in the 12 months before and the 12 months after the floods was compared with those from the rest (not flooded) of the city. | Post-flood: 50% increase in all-cause mortality among the flooded population in the 12 months following flooding, with a notable rise in deaths from cancer. Highest rise in the age group 45 to 64. Male deaths rose from 7 to 20 and female deaths from 5 to 9 mainly during the third three month period following the flooding. Also significant rise in adults 65+ especially females 75+ (a rise from 9 to 19). GP attendances rose by 53% (males 81%, females 25%), those between 1 and 4 and 55+ years and over had increased attendance rates, but there were no differences associated with social class. Subgroup analysis, of those who were extensively flooded and those who were not re-housed, showed significant shift in attendance pattern (0–2 or 3+ GP attendances) for males (non-significant increase for females). Referrals to hospital and hospital admissions more than doubled, significant in males only. Significant increase in new symptoms in flooded group the year after, 33% flooded males reported new physical symptoms compared with 16% of non-flooded males. Among the flooded females, 18% reported psychiatric symptoms (including psychiatric symptoms which might have been present before the floods), but only 6% of the non-flooded females did so. |
| Milojevic, Armstrong
et al. 2011 [39] England and Wales | Case-controlled interrupted time-series analysis 319 Flood events in England and Wales, 1994–2005 Long-term flooding mortality | Compared relative change in mortality, for pre-flood year/ post-flood year deaths in flooded & control (within 5 km of flood) areas. Results were stratified by age group, gender. disease classification (ICD-9, ICD-10), cause of death, urban rural status, quintile of the Index of Multiple Deprivation score for the LLSOA of residence and place of death as on death certificate. | Post-flood: 771 deaths, in the year before flooding, and 693 deaths, in the year after (post-/pre-flood ratio of 0.90, 95% CI 0.82, 1.00). This flood ‘deficit’ of deaths did not vary substantially by age, sex, population density or deprivation. Concludes that results are counter-intuitive, may be biased by displacement of flood affected individuals (particularly frail and elderly at increased risk of dying & therefore not represented in the study) to non-flooded areas or that the increased support, from networks, positively effects well-being & reduces mortality. |
| Paranjothy, Gallacher
et al. 2011 [40] UK | Qualitative survey 2007 UK floods in South Yorkshire and Worcestershire Prevalence and risk factors for mental health | A population-based survey (n = 2,166) to identify prevalence of, and risk factors for, the psychosocial effects of the 2007 floods in the United Kingdom (3–6 months after floods). Examined psychological distress (GHQ-12), anxiety (GAD-7), depression (PHQ-9), and post-traumatic stress disorder (PTS check list short form) compared to individuals whose homes were not flooded. Also examined risk factors: concern that the floods would affect people’s health; perception of an adverse impact on finances; disruption to essential and evacuation. | Post-flood: Prevalence of each mental health measure was significantly higher for those who reported floodwater in the home: psychological distress (GHQ-12) 69%, probable anxiety (GAD-7) 48%, probable depression (PHQ-9) 43%, probable post-traumatic stress disorder (PTS check list short form) 22%, compared to individuals whose homes were not flooded. Risk factors, associated with all mental health measures, were considered in the adjusted analysis and an association was seen for all mental health measures for: concern that the floods would affect people’s health (OR 3.0–4.7); perception of an adverse impact on finances (OR 1.8–3.2); disruption to essential services (OR 1.8–3.1). Evacuation was associated with psychological distress (OR 1.7; 95% CI 1.2, 2.5) only. |
| Tomio, Sato
et al. 2010 [41] Japan | Cross-sectional survey Flash flood 2005 Kagoshima, Japan Medication interruption risk factors | Cross-sectional survey of 810 individuals who attended 15 medical facilities. | Post-flood: Elderly and chronically ill are at high risk for interruption of medications and those who experienced interruption of medication were more likely to have deteriorated health status one month after the flood (OR 4.5; 95% CI: 1.2, 17.6). |
| Price 1978 [42] Australia | Case controlled survey and before (immediately following) and 1 year after based study. Brisbane floods 1974 Longer-term vulnerability (demographic: age and gender) to psychological and physical health effects of floods | Survey of the mental and physical health of 246 flooded households (695 people, 69 who were 65+) compared with that of 194 non-flooded households (507 persons, of whom 59 who were 65+) living in the same suburbs of Brisbane. Compared (a) the health of the flooded before the flood with their health afterwards, and (b) the health of the flooded after the flood with that of controls during the same period. | Post-flood: Higher proportion claimed worsened health the year following flood, except those 75+ who were the group least affected by the flood experience. The impact of the floods on health increased in 35+ (more likely to be householders). GP visits did not differ in the year after the flood compared to before, however, the young and the very old were likely to have changed their pattern of attendance to GPs after the flood compared to control. Females under 65 years had more psychiatric symptoms than males, but this gender difference disappeared in the 65+ group (working age males not constantly confronted with home damage, like other age groups were). |
| Selten, van der Graaf
et al. 1999 [43] Netherlands | Case control Netherlands Flood 1953 Longer-term psychosocial effect of disaster exposure on unborn | Data from the Dutch Psychiatric Registry was examined for an effect of the flood disaster of February 1953. Compared rates of schizophrenia for babies born to mothers who were pregnant during flood and those in utero before or after floods, (but not during). | Post-flood: No significant association between prenatal exposure to maternal stress and risk of non-affective psychosis in those, born to mothers, who experienced flooding. |
| Gordon, Bresin et al. 2011 [44] US | Cohort North Dakota 2009 Flood Effect of natural disaster on the desire for suicide | Sample of 210 undergraduate students were surveyed for interpersonal risk factors associated with the desire for suicide (feeling like one does not belong and feeling like one is a burden on others). | Post-flood: Association found between greater amounts of time spent volunteering in flood efforts and increased feelings of belongingness and decreased feelings of burdensomeness. |
| De Leo, San Too,
et al. 2013 [45] Australia | Case control rate comparison Queensland floods Jan 2011 Suicide rates and characteristics | Examined the rates, and characteristics of suicides, compared to the same time the previous 11 years (based on Australian Bureau of Statistics population numbers for 2000–2010), 6 months after severe flooding in two Queensland towns (Ipswich and Toowoomba). Poisson regression for linear and nonlinear trends in location based suicides; chi-square tests for characteristics of suicide, and Fisher’s exact tests, where counts were less than five in 20% of cells. | Post-flood: No significant difference in suicides, compared to the same time the previous year, six months after severe flooding, in two Queensland towns. Follow up may have been too short, and the period of support following floods may have acted to protect individuals from feeling suicidal. Suggest a follow-up time of two years. Previous suicide attempt and communicating suicidal intent were significant risk factors for those who committed suicide post-flood. Among those that committed suicide, there were no differences in rates of suicide by gender, marital status, ethnicity, employment status, living arrangements, or stressful life event, in those that were flooded in 2011 compared to the previous 11 years. For a single suicide, floods were explicitly attributed as one of the contributing factors, however, the authors note that natural disaster exposure is not routinely collected on the generic form for reporting of suicides. |
| Handmer & Smith 1983 [25] Australia | Comparison Flooding in Lismore Australia, 1974 Hospital admission and mortality risks associated with flooding | Used data from hospital admission and death certificates and from an earlier survey. Compared mortality and hospital admissions before and after the flood; and differential health effects by level of flood and gender; included residents outside flood plain. | Post-flood: While there was no overall difference in hospital admissions or deaths pre-flood compared to post-flood, residents whose homes were exposed to a metre or more of floodwater over floor level were twice as likely to be admitted to hospital as residents of the flood free areas. |
| Norris, Murphy
et al. 2004 [46] Mexico | Interview and between city comparison Flooding and landslides in Tezuitl’an, Puebla and Villahermosa, Tobasco Mexico, 1999 Post-traumatic stress disorder (PTS) and major depressive disorder (MDD) | 561 participants, who were exposed to landslides or floods in Mexico, were interviewed and assessed four times, at 6 month intervals, 6 months post-flood, to examine the course of post-flood PTS symptoms and other outcomes over time. 500 participants, who were located in two flooded towns were interviewed and assessed four times at 6 month intervals (starting 6 months post-flood), to examine the course of post-flood PTS symptoms, and other outcomes over time. | Post-flood: PTS was highly prevalent (24% combined sites). Analyses of mean data for counts of PTS symptoms indicated that PTS symptoms initially decreased, but then stabilized around 18-months post-flood. If recovery is not achieved by this time, PTS is likely to be chronic (in approx. 1/3 of cases). For many people recovery occurred after 1 year, suggesting distress may be quite prolonged in the aftermath of floods. Evidence of a strong (F (1, 557) = 51.43, p < 0.001) relationship between education and PTS was observed but the direction of the relationship is unclear from the study report. |
| Ginexi, Weihs
et al. 2000 [32] US | Prospective cohort study before and after floods Flood Iowa US 1993 (Midwest floods) Depression (CES-D scale) and socio-demographic modifiers pre and post-flood, among those exposed to flood effects and those unexposed to flood impact | 2,379 individuals (18 years or older) were randomly sampled and assessed 1 year, pre- flooding and 1,735 respondents were assessed 30 to 90 days post- flooding. Data on risk factors for depression including age, gender, education, marital status, race and income, and community size were sought, during telephone interviews. Those who were not followed up were more likely to be male, never married, with slighter lower SES, depressed pre-flood, and reside in non-farm, rural communities. While the means and variances were affected by attrition the overall relationship, between independent variables and depression, were not. Impacted respondents numbered 893. | Post-flood: Depression scores were, on average, higher among those impacted compared to control respondents, however, the number with depression was not different between groups. |
| Canino, Bravo
et al. 1990 [33] Puetro Rico | Prospective cohort study before and after floods; unimpacted served as controls; combined with retrospective cohort Flooding and landslides Puetro Rico 1985 Mental health (major depressive episode, dysthymia, post- traumatic stress disorder (PTS), alcohol and drug abuse/or dependence (DAD), generalized anxiety (GA), panic and antisocial personality disorder (ASP)) Diagnostic Interview Schedule/Disaster Supplement (DIS/DS) | Total 912 interviews post-flood (375 were prospective sample and 537 retrospective sample). Note that PTS, GA, DAD, and ASP was not assessed in 1984; so no pre-flood comparison is available for these outcomes. Interviews were conducted in 1887, flood occured in 1985). 77 of the prospective sample were exposed to the flood (significantly more males exposed than females), half retrospective sample were exposed to the flood. In both samples, the exposed were significantly less educated than the unexposed, but did not differ on other demographic charactersitics. | Post-flood: Among the retrospective and prospective samples, there was a trend for the exposed group to have a non-significant higher rate of new cases of depressive disorders and alcohol abuse and/or dependence, than the unexposed. For level of depressive symptoms, in both the retrospective and prospective samples, the differences between groups reached significance. New somatic symptoms and the total number of symptoms in the retrospective sample were found to be significantly more frequent in the flood exposed group. Significant differences for PTS and generalized anxiety, were observed in retrospective sample, in exposed group compared to unexposed, however, these conditions were not measured in the first interview for the prospective sample. |
| Krug, Kresnow
et al. 1999 [47] US | Archival case series Floods in America, between 1982 and 1989 Suicide rates | Examined predisaster and postdisaster suicide rates per 100,000 population, 1982 to 1989. Outcomes for earthquakes, hurricanes, severe storms and tornados are beyond the scope of the review. | Post-flood: Study found that there was no significant difference between the pre-flood and post-flood suicide rates per 100,000 population. |
| Reference Country | Study type Event Area of focus | Methods | Findings |
|---|---|---|---|
| Jonkman and Kelman 2005 [48] Europe and US | Case series Worldwide 13 flooding events Deaths and demographic description: age and gender only | 247 flood fatalities from 13 flood disaster events, analysed to determine cause and circumstances of death. | Pre-flood: 0% deaths During-flood: Age at death: <20 yrs = 13.4%; 20–60 yrs = 39%; over 60 = 16.6%, not reported = 30.4%. N.B: Cannot determine age related vulnerability without age distribution of the flood effected population. Gender: assuming that there is an equal gender distribution in the flood affected population males (58.7%) appear to be at great risk of flood mortality than females (25.1%) NB gender was unknown for 16.2%. 75.7 % deaths (83 for Europe) (104 for US), drowning (167) 67.6%; all physical trauma (29) 11.7%; heart attack (14) 5.7%; electrocution (7) 2.8%; carbon monoxide poisoning (2) 0.8%; fire (9) 3.6%; other (3) 1.2%; unknown or not reported 16 (6.5%). Overall: numbers of flood deaths are due to unnecessary risky behaviour. Suggestions of increased vulnerability of the elderly to heart attacks. Post-flood: 10.9% of deaths related to clean-up (heart attack and vehicle-related drowning) (4 in Europe and 10 in US)NB 13.4% timing of death not determinable for 8 in Europe and 24 in US. |
| French, Ing
et al. 1983 [52] US | Historical summary Various flash floods during 1969–1981 Mortality | A summary of the National Weather Service survey reports on flash floods issued during 1969–1981 to determine the flood mortality, the effect of warnings on mortality, and the cause of death. | During-flood: A total of 1,185 deaths were associated with the 32 flash floods, an average of 37 deaths per flood. Of 190 deaths with cause, 93% were due to drowning and 42% of these drownings were car related. The other drownings occurred in homes, at campsites, or when persons were crossing bridges and streams. Other deaths were due to trauma, heart attacks, electrocution or being buried in mud slide. |
| Jonkman 2005 [1] Worldwide | Database analysis Worldwide flooding events between 1975–2002 (n = 1,902) Loss of life statistics from the OFDA/CRED database concerning a large number of flood events worldwide | Using the Centre for research on the epidemiology of disasters (CRED) & United States Office for foreign disaster assistance (OFDA) databases, analysed flood events between Jan 1975 & June 2002. | During-flood: No significant differences between continents for average mortality per flood event (=number of killed/number of affected). Significant regional (17 regions as defined in EM-DAT) differences observed for average flood mortality mainly caused by the dominance of some high mortality events in the regional datasets. No indication of a relationship between mortality and the underlying determinants of the region. |
| Duclos and Isaacson 1987 [49] US | Case series Floods in Illinois, Oklahoma, Missouri, Michigan 1986 Deaths and demographic vulnerability: gender only | Description of the 24 deaths due to flood. | Pre-flood: 3 heart attacks (lifting furniture & sandbagging) During-flood: 17/24 deaths male. Age range only reported: 8–78 years. Causes: 9 drowned (1 boat related, 2 car related, entered barricaded area, 1 slipped off embankment, & 1 child played near swollen stream), 2 heart attacks (evacuating), 3 lightning related (1 in car hit by tree struck by lightning; 1 in house burned after lightning strike, 1 struck by lightning while cleaning metal milking cans), 1 in car crash (avoiding flooded river involved another car). Post-flood: 4 heart attacks (cleaning up flooded basements), 1 asphyxiation (gas pump use in basement), 1 electrocution (used pump in flooded basement). |
| Smith, Young
et al. 2013 [50] Australia | Case reports Queensland floods Dec 2010–Jan 2011 Cases of leptospirosis (and other flood-related infections) in flood-affected communities | Standard notification case reporting and usual laboratory surveillance, plus enhanced surveillance through health service providers. Surveyed cases on residential history 1 month prior to onset of illness (including temporary relocation due to flooding), consumption of food contaminated by floodwater; injuries (particularly breaches to skin related to flood exposure), contact with animals; and exact details of exposure to floodwater and involvement in flood recovery. | During/Post-flood: Nine confirmed leptospirosis cases were associated with floodwater. All of the cases of leptospirosis were: ill within 2 to 30 days, from floods events, all were hospitalised, all male and the median age was 34 and all had direct exposure with floodwater and most had cuts or abrasions. |
| CCDR 2000 [51] Canada | Case report and cross sectional study Heavy rainfall leading to flooding of water into Canadian water supply 2000 Determines the scope, the likely cause, and the contributing factors of the outbreak of gastroenteritis in Walkerton, Ontario, in May and June 2000 | The investigation comprised a descriptive study and a cross-sectional study. Intensive case-finding for the descriptive study identified 1,346 reported cases of gastroenteritis exposed to municipal water. | Post-flood: 1,304 of 1,346 reported E. coli cases were primary, 39 were secondary (exposed to a primary case and not to public water supply), and three were unclassified. 27 of 65 patients admitted to hospital developed hemolytic uremic syndrome. Six deaths were attributed to the outbreak. 57% of cases were female and the median age of cases was 29 years (range < 1 to 97 years). Several cases were prior to the floods (earliest April 15), the majority of cases were contracted between 16 and 26 May. Homes connected to and consuming public water supply, were 11.7 times more likely to develop gastroenteritis than those not exposed to public water supply. A dose response relationship with the risk of illness increasing with the quantity of water consumed was observed. Some residents continued to expose themselves to the water, despite the extensive publicity and a “boil water” advisory, via brushing teeth with the water and occasionally drinking it. |
| Mortality | Gastro illness | Mental illness | Physical illness | Injuries | |
|---|---|---|---|---|---|
| Gender (M= male; F= female) | − [17,20] M 10–29↑ [16] M 35–54↑ [36] M↑ [16,36] | F↑ [18] | − [34] | − [34] | − [18] |
| Age | − [20] 10–29↑ [16,35] 30–59↓ [16] >55↑ [17] >60↑ [16] >70↑ [35] | − [18] | >60↑ [34] | >60↑[34] | − [18,19] |
| Ethnicity | − [17] | ||||
| Tenure | − [34] | − [34] | |||
| Flooding indoors | − [18] | ↑ [18] | |||
| Clean up involvement | ↑ [18] | ↑ [18] | |||
| Skin exposure to water | ↑ [18] | ↑ [18] | |||
| Exposed food | − [18] | ||||
| Private pond water supply | ↑ [18] | ||||
| Public water supply | − [18] | ||||
| Tank water | − [18] | ||||
| Location (distance to flood) | − [34] | − [34] | |||
| Vehicle occupancy | ↑ [20] | ||||
| Used car to evacuate | ↓ [20] | ||||
| Used car for other reason | ↑ [20] | ||||
| High blood alcohol content | ↑ [20] (not comparative) |
| Physical illness | Mental illness | PTS | Injuries | Respiratory illness | Gastro illness | Health care use | |
|---|---|---|---|---|---|---|---|
| Age | <45↑ [30] − [31] older age ↑[28] | >60− [22,32] younger age↑ [31] 55–64↑ [31] older age ↑[28] | <65↑[22] older age↑[27] | older age −[28] | <15− [29] >65− [29] | increasing age↑ [24] | |
| Gender | M↑ [30] − [28,31] | F↑[22] M↑[31] −[28,32] | F↑[22,27] | −[28] | − [29] | − [24] | M↑ [25] |
| Married | ↑[30] | ↓[32] | |||||
| Lower education | − [31] ↓[30] | − [32] | ↑[27] | ||||
| Lower SES | − [31] ↑[28] ↓[30] | ↑[28,31,32] | ↑[28] | ↑[29] | |||
| Existing health/ previous symptoms | ↑[22,32] − [31,33] | ↑[22] | ↑[21] | ||||
| Access to health care | ↓[28] | ↓[28] | − [28] | ||||
| Medication interruption | ↑[41] | ||||||
| Non-US citizen | ↑[28] | ↑[28] | − [28] | ↑[29] | |||
| Greater local language proficiency | ↑[28] | ↑[28] | − [28] | ↑[29] | |||
| Ethnicity (Hispanic) | ↑[28] | −[28] | − [28] | ||||
| Foreign born | − [28] | ↓[28] | − [28] | ||||
| Mold exposure | ↑[29] | ||||||
| Family conflict | ↑[29] | ||||||
| Non-smoker | ↑[30] | ||||||
| Non-drinker | ↑[30] | ||||||
| Existing chronic GI | ↑[21] | ||||||
| Public water supply | −[21] | ||||||
| Drinking water dose response | − [21] | ||||||
| Direct floodwater contact | ↑[21] | ||||||
| Indirect floodwater contact | ↑[21] | ||||||
| Adverse event from flooding/ trauma | ↑[28] | ↑[28] | ↑[27] | ↑[28] | |||
| Flooding to home/property | − [28] | − [28] ↑[22] | ↑[22] | ↑[28] | ↑[21] | ||
| Problems with insurance | ↑[22] | ↑[22] | |||||
| Uninsured | ↑[22] | −[22] | |||||
| Evacuation | ↑[22] | ↑[22] | |||||
| Prolonged recovery/ trauma consequences | ↑[22] | ↑[22,26] | |||||
| Less warning time | ↑[22] | ↑[22] | |||||
| Rental housing | ↑[22] | − [22] | |||||
| Water depth | − [22] | ↑[22] | |||||
| Vulnerable housing | − [22] | ↑[22] | |||||
| Decreasing distance from flood | ↑[24] | ||||||
| Personality trait: | |||||||
| Briskness | ↓[26] | ||||||
| Perseveration | ↑[26] | ||||||
| Sensory sensitivity | − [26] ↓@15 months [26] | ||||||
| Endurance | ↓[26] | ||||||
| Emotional reactivity | ↑[26] | ||||||
| Activity | ↓@15 months; − @3 months & 3 yrs [26] |
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lowe, D.; Ebi, K.L.; Forsberg, B. Factors Increasing Vulnerability to Health Effects before, during and after Floods. Int. J. Environ. Res. Public Health 2013, 10, 7015-7067. https://doi.org/10.3390/ijerph10127015
Lowe D, Ebi KL, Forsberg B. Factors Increasing Vulnerability to Health Effects before, during and after Floods. International Journal of Environmental Research and Public Health. 2013; 10(12):7015-7067. https://doi.org/10.3390/ijerph10127015
Chicago/Turabian StyleLowe, Dianne, Kristie L. Ebi, and Bertil Forsberg. 2013. "Factors Increasing Vulnerability to Health Effects before, during and after Floods" International Journal of Environmental Research and Public Health 10, no. 12: 7015-7067. https://doi.org/10.3390/ijerph10127015