Ivabradine Prevents Heart Rate Acceleration in Patients with Chronic Obstructive Pulmonary Disease and Coronary Heart Disease after Salbutamol Inhalation

 ,
,
Abstract
:1. Introduction
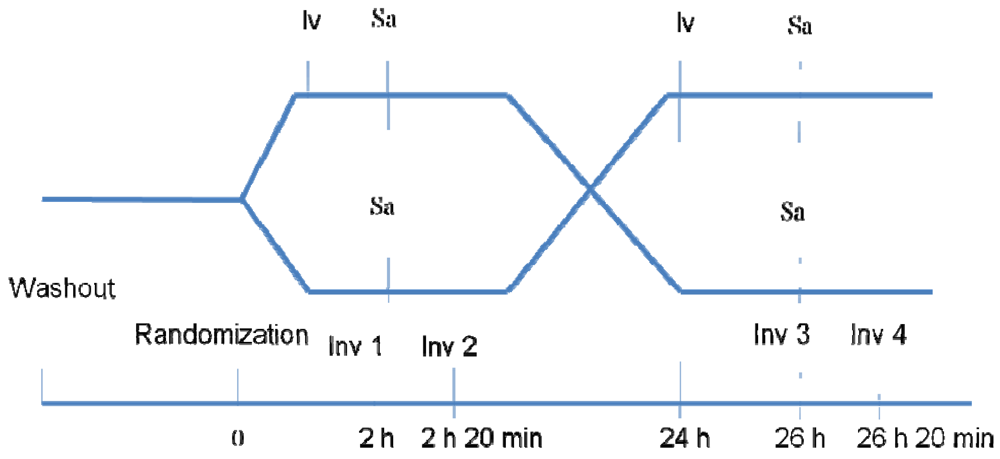
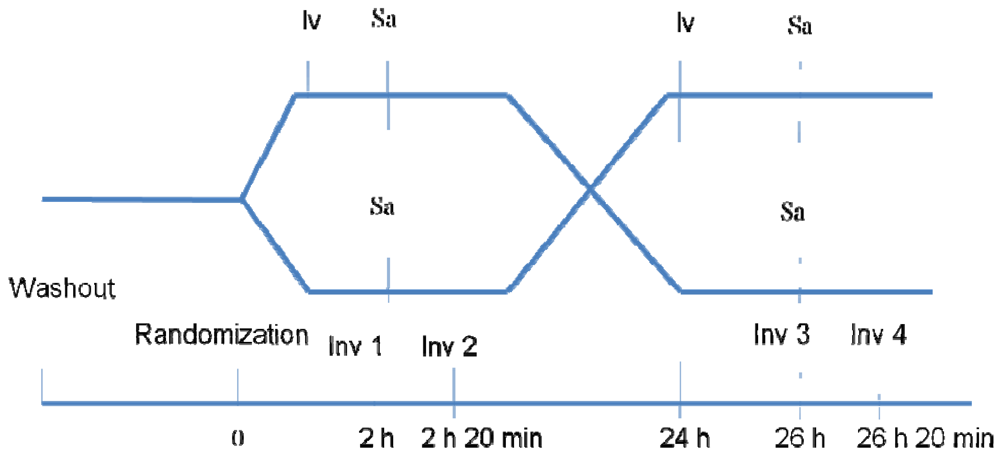
2. Experimental Section
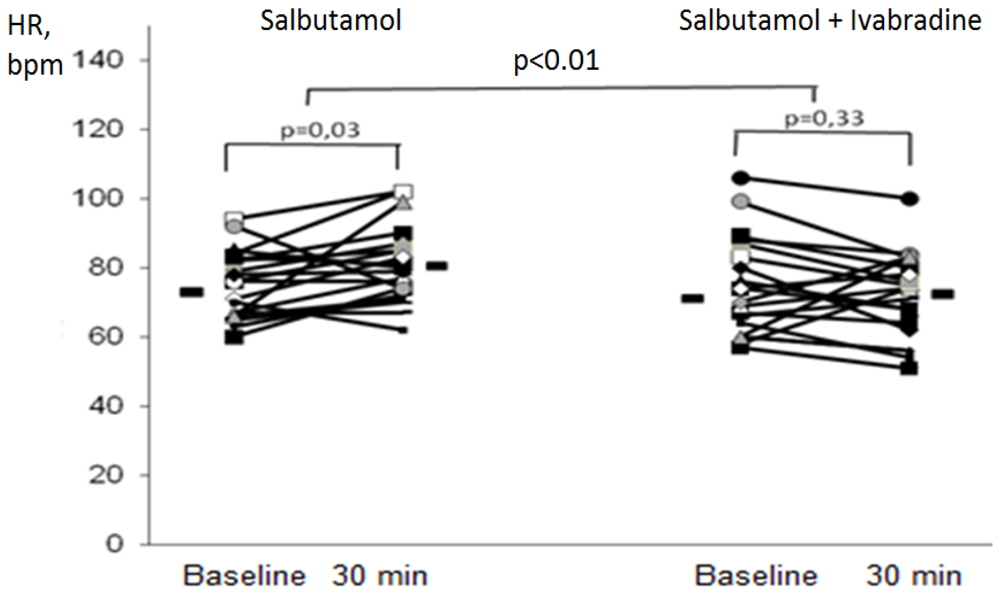
3. Results

{kind=link}
{kind=link}
| Parameters | Values |
|---|---|
| Age, years | 62.0 (57.0–72.0) |
| BMI, kg/m2 | 26.3 (21.1–28.5) |
| Smoking, packs × years | 40.0 (30.0–73.5) |
| Postbronchodilatory FEV1, % pred. | 46.7 (26.0–67.1) |
| SPAP, mmHg | 32.5 (26.0–39.0) |
| 6-min. walktest, m | 439 (411–480) |
| Heart rate, bpm | 77 (66–87) |
| SAP, mmHg | 128 (118–146) |
| DAP, mmHg | 80 (72–90) |

| Group I | Group II | |||
|---|---|---|---|---|
| Salbutamol | Ivabradine+Salbutamol | Ivabradine+Salbutamol | Salbutamol | |
| Heart rate, bpm | 78 (69-90) | 79 (69-86) | 74 (62-84) | 76 (67-82) |
| SAP, mm Hg | 124 (120-136) | 120 (115-130) | 128 (125-144) | 130 (120-148) |
| DAP, mm Hg | 80 (74-80) | 84 (74-90) | 84 (80-90) | 86 (70-94) |
| FEV1, % pred., | 39.6 (24.3-67.2) | 31,1 (25.7-65.3) | 43.4 (29.6-63.6) | 48.4 (28.5-52.5) |
| Salbutamol | Ivabradine+Salbutamol | |
|---|---|---|
| Heart rate, bpm | 5.5 (0.8; 10.2) * | −2.4 (−7.0; 2.3) |
| SAP, mm Hg | 0.3 (−3.5; 4.2) | −2.0 (−7.8; 3.8) |
| DAP, mm Hg | −1.3 (−4.1; 1.4) | −2.0 (−5.4; 1.4) |
| FEV1, % pred. | 6.0 (2.7; 9.3) ** | 7.7 (2.8; 12.6) ** |
4. Discussion
5. Conclusions
Conflict of Interest
References
- Curkendall, S.M.; de Luise, C.; Jones, J.K.; Lanes, S.; Stang, M.R.; Goehring, E., Jr.; She, D. Cardiovascular disease in patients with chronic obstructive pulmonary disease.Saskatchewan Canada cardiovascular disease in COPD patients. Ann. Epidemiol. 2006, 16, 63–70. [Google Scholar] [CrossRef]
- Falk, J.A.; Kadiev, S.; Criner, G.J.; Scharf, S.M.; Minai, O.A.; Diaz, P. Cardiac disease in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2008, 5, 543–548. [Google Scholar]
- Gunes, Y.; Tuncer, M.; Guntekin, U.; Gumrukcuoglu, H.A.; Akdag, S.; Ozbay, B.; Sertogullarindan, B. Reliability of symptoms suggestive of angina in patients with chronic obstructive pulmonary disease. Arq. Bras. Cardiol. 2009, 92, 334–338. [Google Scholar]
- Macie, C.; Wooldrage, K.; Manfreda, J.; Anthonisen, N. Cardiovascular morbidity and the use of inhaled bronchodilators. Int. J. Chron. Obstruct. Pulmon. Dis. 2008, 3, 163–169. [Google Scholar]
- Salpeter, S.R.; Ormiston, T.M.; Salpeter, E.E. Cardiovascular effects of beta-agonists in patients with asthma and COPD: A meta-analysis. Chest 2004, 125, 2309–2321. [Google Scholar] [CrossRef]
- Fisher, A.A.; Davis, M.W.; McGill, D.A. Acute myocardial infarction associated with albuterol. Ann. Pharmacother. 2004, 38, 2045–2049. [Google Scholar]
- Zodionchenko, V.S.; Manzurova, A.V.; Grineva, Z.O.; Sviridov, A.A. Silent myocardial ischemia in patients with chronic obstructive lung disease and treatment options. Rossiyskiy kardiologicheskiy zhurnal (rus) 2000, 1, 66–72. [Google Scholar]
- Joint National Committee. The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch. Intern. Med. 1997, 157, 2413–2446. [CrossRef]
- Borer, J.; Fox, K.; Jaillon, P. Antianginal and antiischemic effects of ivabradine, an If inhibitor, in stable angina. A randomized, double-blind, multicentered, placebo-controlled trial. Circulation 2003, 107, 817–823. [Google Scholar] [CrossRef]
- Fox, K.; Garcia, M.A.; Ardissino, D.; Buszman, P.; Camici, P.G.; Crea, F.; Daly, C.; de Backer, G.; Hjemdahl, P.; Lopez-Sendon, J.; et al. Guidelines on the management of stable angina pectoris: Executive summary: The task force on the management of stable angina pectoris of the European Society of Cardiology. Eur. Heart J. 2006, 27, 1341–1381. [Google Scholar]
- Prasad, U.K.; Gray, D.; Purcell, H. Review of the If selective channel inhibitorivabradinein the treatment of chronic stable angina. Adv. Ther. 2009, 26, 127–137. [Google Scholar]
- Fox, K.; Ferrari, R.; Tendera, M.; Steg, P.G.; Ford, I. Rationale and design of a randomized, double-blind, placebo-controlled trial of Ivabradine in patients with stable coronary artery disease and left ventricular systolic function the morbidity-mortality evaluation of the If inhibitor Ivabradine in patients with coronary disease and left ventricular dysfunction (BEAUTIFUL) study. Am. Heart J. 2006, 152, 860–866. [Google Scholar] [CrossRef]
- van Gestel, Y.R.; Hoeks, S.E.; Sin, D.D.; Welten, G.M.; Schouten, O.; Witteveen, H.J.; Simsek, C.; Stam, H.; Mertens, F.W.; Bax, J.J.; et al. Impact of cardioselective beta-blockers on mortality in patients with chronic obstructive pulmonary disease and atherosclerosis. Am. J. Respir. Crit. Care Med. 2008, 178, 695–700. [Google Scholar] [CrossRef]
- Cazzola, M.; Noschese, P.; D’Amato, G.; Matera, M.G. The pharmacologic treatment of uncomplicated arterial hypertension in patients with airway dysfunction. Chest 2002, 121, 230–241. [Google Scholar]
- van der Woude, H.J.; Zaagsma, J.; Postma, D.S.; Winter, T.H.; van Hulst, M.; Aalbers, R. Detrimental effects of beta-blockers in COPD: A concern for nonselective b-blockers. Chest 2005, 127, 818–824. [Google Scholar]
- Ling, Y.; Saleem, W.; Shee, C.D. Concomitant use of beta-blockers and beta2-agonists. Eur. Respir. J. 2008, 31, 905–906. [Google Scholar]
- Andrus Miranda, R.; Holloway Katherine, P.; Clark Deidre, B. Use of β-blockers in patients with COPD. Ann. Pharmacother. 2004, 38, 142–145. [Google Scholar]
- Kolomoets, N.M.; Bakshiev, V.I.; Zarubina, E.G.; Usenko, S.V.; Arkad’eva, N.M.; Kostycheva, T.V.; Uvaĭsova, K.U. Clinical efficiency of ivabradine in patients with cardiorespiratory pathology. Klin. Med. (Mosk) 2008, 86, 44–54. [Google Scholar]
- Guth, T.H.; Dietze, T. If current mediates β-adrenergic enhancement of heart rate but not contractility in vivo. Basic Res. Cardiol. 1995, 90, 192–202. [Google Scholar] [CrossRef]
- di Francesco, D.; Tortora, P. Direct activation of cardiac pacemaker channels by intracellular cyclic AMP. Nature 1991, 351, 145–147. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zulkarneev, R.; Zagidullin, N.; Abdrahmanova, G.; Hoppe, U.C.; Zagidullin, S. Ivabradine Prevents Heart Rate Acceleration in Patients with Chronic Obstructive Pulmonary Disease and Coronary Heart Disease after Salbutamol Inhalation. Pharmaceuticals 2012, 5, 398-404. https://doi.org/10.3390/ph5040398
Zulkarneev R, Zagidullin N, Abdrahmanova G, Hoppe UC, Zagidullin S. Ivabradine Prevents Heart Rate Acceleration in Patients with Chronic Obstructive Pulmonary Disease and Coronary Heart Disease after Salbutamol Inhalation. Pharmaceuticals. 2012; 5(4):398-404. https://doi.org/10.3390/ph5040398
Chicago/Turabian StyleZulkarneev, Rustem, Naufal Zagidullin, Guzel Abdrahmanova, Uta C. Hoppe, and Shamil Zagidullin. 2012. "Ivabradine Prevents Heart Rate Acceleration in Patients with Chronic Obstructive Pulmonary Disease and Coronary Heart Disease after Salbutamol Inhalation" Pharmaceuticals 5, no. 4: 398-404. https://doi.org/10.3390/ph5040398