
Comparison of Heart Rate Monitoring Accuracy between Chest Strap and Vest during Physical Training and Implications on Training Decisions


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Study Protocol
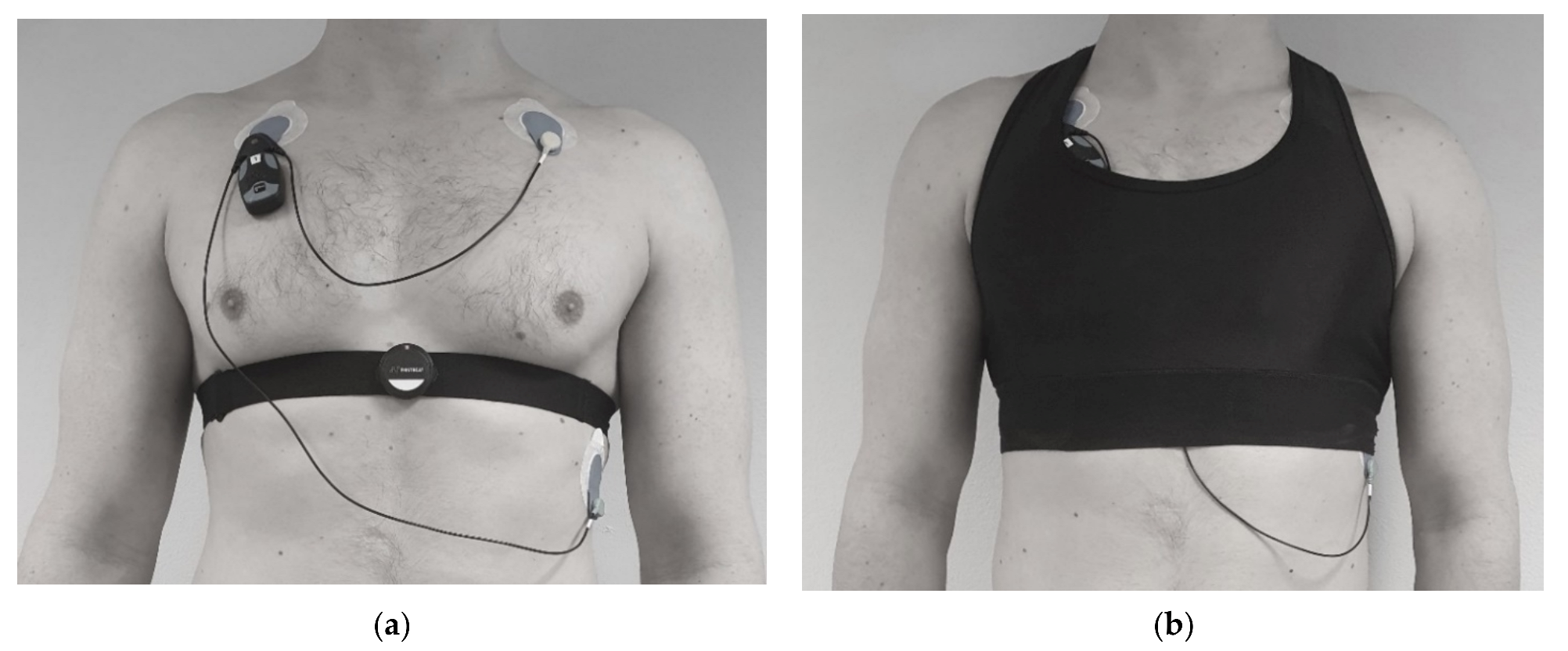
2.2. Data Aqusition
2.3. Signal Processing
2.4. Estimation of the Measurement Error
2.5. Statistical Analyzes
3. Results
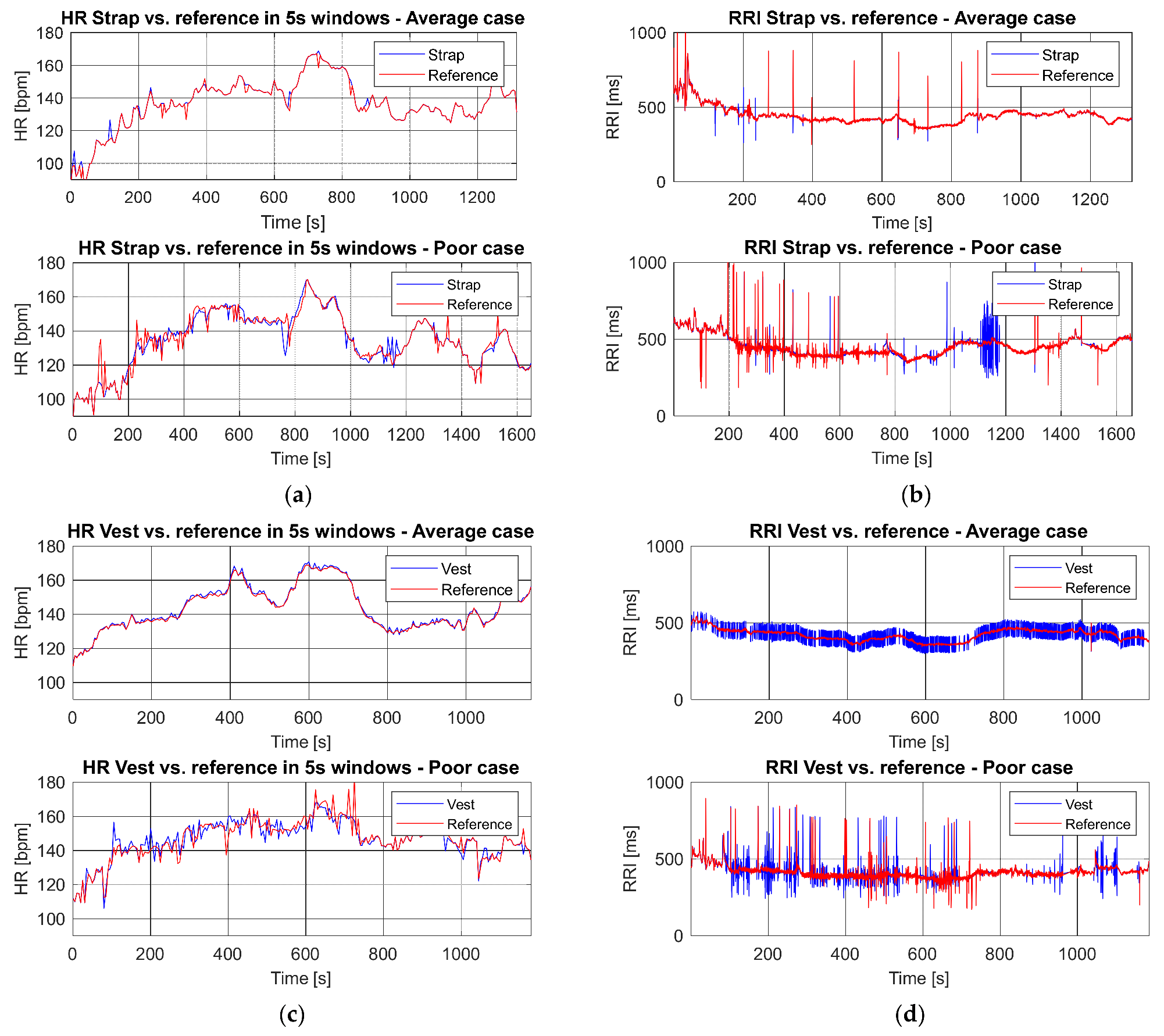
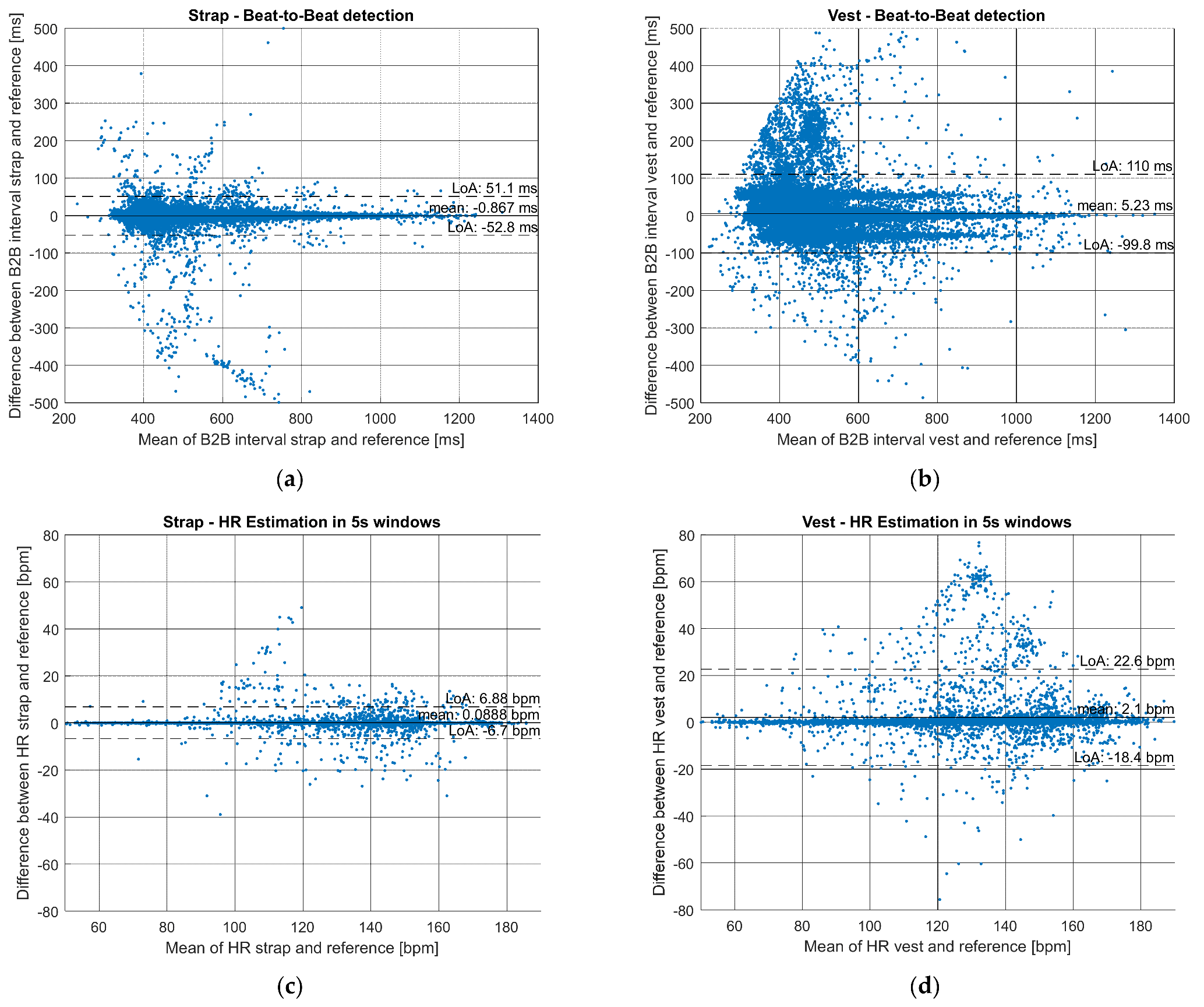
3.1. Heart Rate Measurement Accuracy
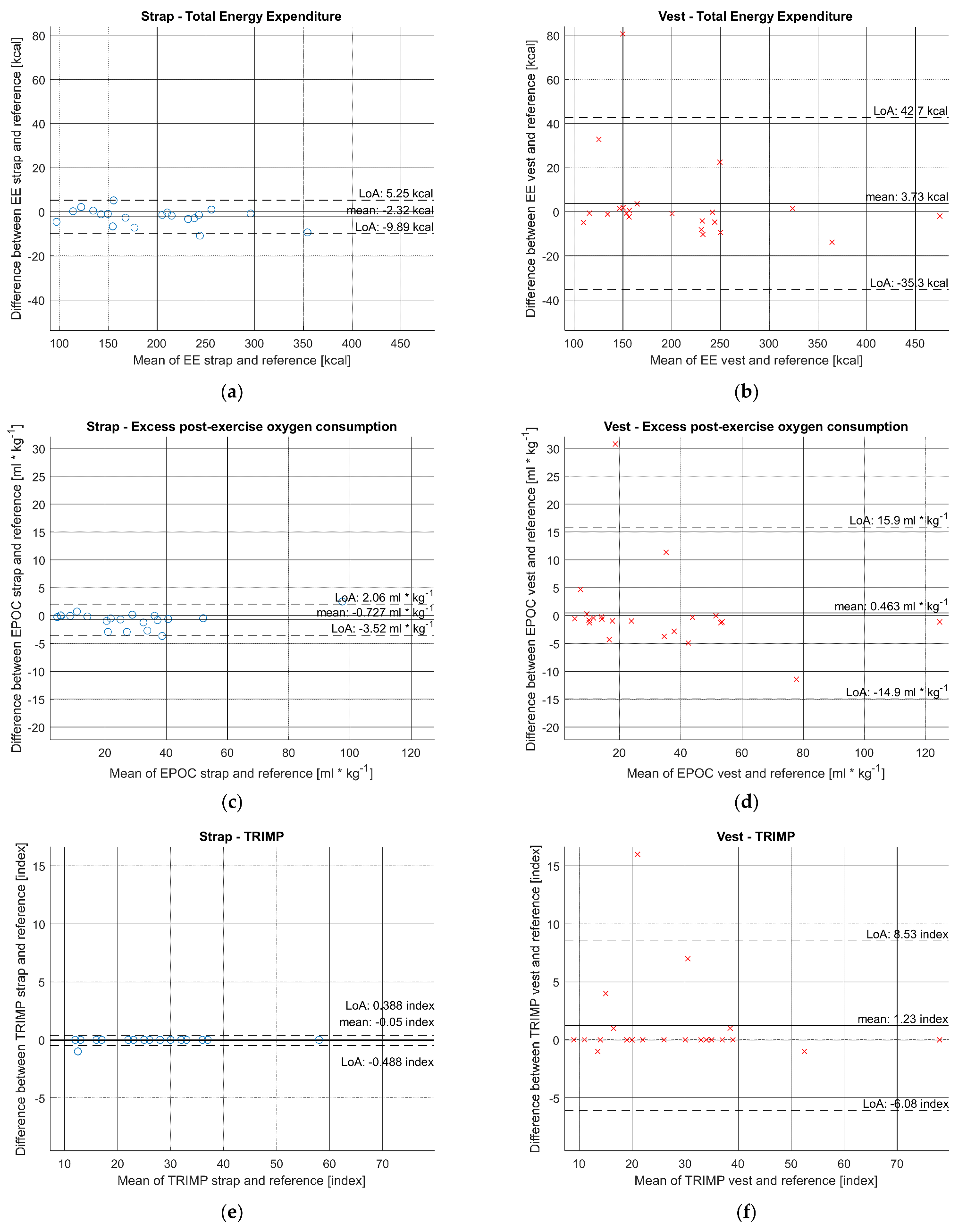
3.2. Training Parameters Estimation Accuracy
4. Discussion
4.1. Principal Findings
4.2. Limitations and Strenghts of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Subject (Gender, Height, Weight) | Strap | Reference | MAE | MAPE | Vest | Reference | MAE | MAPE |
|---|---|---|---|---|---|---|---|---|---|
| Average HR (bpm) | M 178/80 | 87 | 87 | 0.00 | 0.00% | 95 | 88 | 7.00 | 7.95% |
| M 177/70 | 119 | 120 | 1.00 | 0.83% | 134 | 135 | 1.00 | 0.74% | |
| M 183/95 | 131 | 131 | 0.00 | 0.00% | 141 | 127 | 14.00 | 11.02% | |
| F 167/74 | 136 | 136 | 0.00 | 0.00% | - | - | - | - | |
| M 193/115 | 134 | 134 | 0.00 | 0.00% | 137 | 137 | 0.00 | 0.00% | |
| F 177/68 | 114 | 114 | 0.00 | 0.00% | 107 | 106 | 1.00 | 0.94% | |
| M 172/76 | 98 | 98 | 0.00 | 0.00% | 100 | 100 | 0.00 | 0.00% | |
| F 164/55 | - | - | - | - | 137 | 137 | 0.00 | 0.00% | |
| M 178/70 | 121 | 121 | 0.00 | 0.00% | 112 | 112 | 0.00 | 0.00% | |
| F 154/51 | 145 | 145 | 0.00 | 0.00% | 147 | 147 | 0.00 | 0.00% | |
| M 188/99 | - | - | - | - | 102 | 102 | 0.00 | 0.00% | |
| M 185/81 | 101 | 101 | 0.00 | 0.00% | 114 | 92 | 22.00 | 23.91% | |
| M 181/74 | 131 | 131 | 0.00 | 0.00% | 125 | 125 | 0.00 | 0.00% | |
| M 184/78 | 137 | 137 | 0.00 | 0.00% | 143 | 144 | 1.00 | 0.69% | |
| M 181/74 | 108 | 108 | 0.00 | 0.00% | 110 | 111 | 1.00 | 0.90% | |
| M 172/115 | - | - | - | - | 156 | 156 | 0.00 | 0.00% | |
| M 184/85 | 140 | 140 | 0.00 | 0.00% | 148 | 148 | 0.00 | 0.00% | |
| F 176/67 | 128 | 128 | 0.00 | 0.00% | 125 | 126 | 1.00 | 0.79% | |
| F 169/75 | 160 | 160 | 0.00 | 0.00% | 152 | 152 | 0.00 | 0.00% | |
| M 174/72 | 128 | 128 | 0.00 | 0.00% | 114 | 114 | 0.00 | 0.00% | |
| M 190/92 | 97 | 97 | 0.00 | 0.00% | 99 | 100 | 1.00 | 1.00% | |
| M 177/93 | 126 | 126 | 0.00 | 0.00% | 120 | 120 | 0.00 | 0.00% | |
| M 181/76 | 122 | 122 | 0.00 | 0.00% | 136 | 136 | 0.00 | 0.00% | |
| Mean | - | 123.15 | 123.20 | 0.05 | 0.04% | 125.18 | 123.41 | 2.23 | 2.18% |
| Energy Expenditure. Total (kcal) | M 178/80 | 94.40 | 98.98 | 4.58 | 4.63% | 141.63 | 108.82 | 32.81 | 30.15% |
| M 177/70 | 204.47 | 205.88 | 1.41 | 0.68% | 241.76 | 246.46 | 4.70 | 1.91% | |
| M 183/95 | 213.98 | 215.71 | 1.73 | 0.80% | 260.59 | 238.16 | 22.43 | 9.42% | |
| F 167/74 | 172.95 | 180.15 | 7.20 | 4.00% | - | - | - | - | |
| M 193/115 | 349.38 | 358.71 | 9.33 | 2.60% | 357.56 | 371.34 | 13.78 | 3.71% | |
| F 177/68 | 113.84 | 113.62 | 0.22 | 0.19% | 107.18 | 112.06 | 4.88 | 4.35% | |
| M 172/76 | 123.12 | 120.97 | 2.15 | 1.78% | 115.30 | 115.95 | 0.65 | 0.56% | |
| F 162/58 | - | - | - | - | - | - | - | - | |
| F 164/55 | - | - | - | - | 156.74 | 156.14 | 0.60 | 0.38% | |
| M 178/70 | 166.11 | 168.83 | 2.72 | 1.61% | 155.18 | 157.46 | 2.28 | 1.45% | |
| F 154/51 | 149.00 | 149.93 | 0.93 | 0.62% | 133.72 | 134.79 | 1.07 | 0.79% | |
| M 188/99 | - | - | - | - | 151.04 | 149.16 | 1.88 | 1.26% | |
| M 185/81 | 134.59 | 134.12 | 0.47 | 0.35% | 190.08 | 109.47 | 80.61 | 73.64% | |
| M 181/74 | 242.03 | 243.45 | 1.42 | 0.58% | 229.26 | 233.38 | 4.12 | 1.77% | |
| M 184/78 | 236.58 | 239.49 | 2.91 | 1.22% | 226.36 | 234.46 | 8.10 | 3.45% | |
| M 181/74 | 157.84 | 152.67 | 5.17 | 3.39% | 166.31 | 162.70 | 3.61 | 2.22% | |
| M 172/115 | - | - | - | - | 473.98 | 475.94 | 1.96 | 0.41% | |
| F 162/63 | - | - | - | - | - | - | - | - | |
| M 184/85 | 295.42 | 296.21 | 0.79 | 0.27% | 324.80 | 323.31 | 1.49 | 0.46% | |
| F 176/67 | 151.10 | 157.73 | 6.63 | 4.20% | 153.35 | 153.98 | 0.63 | 0.41% | |
| F 169/75 | 256.15 | 255.17 | 0.98 | 0.38% | 245.48 | 254.89 | 9.41 | 3.69% | |
| M 174/72 | 230.04 | 233.34 | 3.30 | 1.41% | 199.91 | 200.73 | 0.82 | 0.41% | |
| M 190/92 | 141.85 | 143.02 | 1.17 | 0.82% | 147.07 | 145.57 | 1.50 | 1.03% | |
| M 177/93 | 238.35 | 249.20 | 10.85 | 4.35% | 226.92 | 237.19 | 10.27 | 4.33% | |
| M 181/76 | 210.04 | 210.40 | 0.36 | 0.17% | 241.62 | 241.85 | 0.23 | 0.10% | |
| Mean | - | 194.06 | 196.38 | 3.22 | 1.70% | 211.17 | 207.45 | 9.45 | 6.63% |
| EPOC Peak (ml/kg) | M 178/80 | 4.30 | 4.56 | 0.26 | 5.70% | 9.61 | 4.92 | 4.69 | 95.33% |
| M 177/70 | 21.64 | 22.14 | 0.50 | 2.26% | 36.42 | 39.24 | 2.82 | 7.19% | |
| M 183/95 | 29.01 | 28.85 | 0.16 | 0.55% | 40.90 | 29.54 | 11.36 | 38.46% | |
| F 167/74 | 36.86 | 40.51 | 3.65 | 9.01% | - | - | - | - | |
| M 193/115 | 32.50 | 35.20 | 2.70 | 7.67% | 32.75 | 36.48 | 3.73 | 10.22% | |
| F 177/68 | 14.13 | 14.28 | 0.15 | 1.05% | 11.30 | 11.74 | 0.44 | 3.75% | |
| M 172/76 | 5.59 | 5.69 | 0.10 | 1.76% | 5.12 | 5.66 | 0.54 | 9.54% | |
| F 162/58 | - | - | - | - | - | - | - | - | |
| F 164/55 | - | - | - | - | 43.71 | 44.00 | 0.29 | 0.66% | |
| M 178/70 | 20.05 | 21.01 | 0.96 | 4.57% | 13.93 | 14.57 | 0.64 | 4.39% | |
| F 154/51 | 51.83 | 52.31 | 0.48 | 0.92% | 52.94 | 54.07 | 1.13 | 2.09% | |
| M 188/99 | - | - | - | - | 9.45 | 9.17 | 0.28 | 3.05% | |
| M 185/81 | 5.55 | 5.49 | 0.06 | 1.09% | 34.06 | 3.29 | 30.77 | 935.26% | |
| M 181/74 | 31.94 | 33.16 | 1.22 | 3.68% | 23.39 | 24.37 | 0.98 | 4.02% | |
| M 184/78 | 36.74 | 37.54 | 0.80 | 2.13% | 39.99 | 44.90 | 4.91 | 10.94% | |
| M 181/74 | 11.20 | 10.47 | 0.73 | 6.97% | 9.52 | 10.81 | 1.29 | 11.93% | |
| M 172/115 | - | - | - | - | 123.98 | 125.11 | 1.13 | 0.90% | |
| F 162/63 | - | - | - | - | - | - | - | - | |
| M 184/85 | 40.36 | 40.96 | 0.60 | 1.46% | 52.49 | 53.75 | 1.26 | 2.34% | |
| F 176/67 | 19.51 | 22.43 | 2.92 | 13.02% | 17.19 | 18.15 | 0.96 | 5.29% | |
| F 169/75 | 98.77 | 96.24 | 2.53 | 2.63% | 72.07 | 83.49 | 11.42 | 13.68% | |
| M 174/72 | 24.71 | 25.41 | 0.70 | 2.75% | 14.01 | 14.24 | 0.23 | 1.62% | |
| M 190/92 | 8.62 | 8.66 | 0.04 | 0.46% | 9.66 | 10.47 | 0.81 | 7.74% | |
| M 177/93 | 25.67 | 28.59 | 2.92 | 10.21% | 14.53 | 18.83 | 4.30 | 22.84% | |
| M 181/76 | 36.17 | 36.20 | 0.03 | 0.08% | 51.46 | 51.49 | 0.03 | 0.06% | |
| Mean | 27.76 | 28.49 | 1.08 | 3.90% | 32.66 | 32.20 | 3.82 | 54.15% | |
| TRIMP (index) | M 178/80 | 13.00 | 13.00 | 0.00 | 0.00% | 17.00 | 13.00 | 4.00 | 30.77% |
| M 177/70 | 28.00 | 28.00 | 0.00 | 0.00% | 37.00 | 37.00 | 0.00 | 0.00% | |
| M 183/95 | 25.00 | 25.00 | 0.00 | 0.00% | 34.00 | 27.00 | 7.00 | 25.93% | |
| F 167/74 | 37.00 | 37.00 | 0.00 | 0.00% | - | - | - | - | |
| M 193/115 | 33.00 | 33.00 | 0.00 | 0.00% | 34.00 | 34.00 | 0.00 | 0.00% | |
| F 177/68 | 17.00 | 17.00 | 0.00 | 0.00% | 17.00 | 16.00 | 1.00 | 6.25% | |
| M 172/76 | 12.00 | 12.00 | 0.00 | 0.00% | 11.00 | 11.00 | 0.00 | 0.00% | |
| F 162/58 | - | - | - | - | - | - | - | - | |
| F 164/55 | - | - | - | - | 35.00 | 35.00 | 0.00 | 0.00% | |
| M 178/70 | 22.00 | 22.00 | 0.00 | 0.00% | 19.00 | 19.00 | 0.00 | 0.00% | |
| F 154/51 | 36.00 | 36.00 | 0.00 | 0.00% | 33.00 | 33.00 | 0.00 | 0.00% | |
| M 188/99 | - | - | - | - | 9.00 | 9.00 | 0.00 | 0.00% | |
| M 185/81 | 16.00 | 16.00 | 0.00 | 0.00% | 29.00 | 13.00 | 16.00 | 123.08% | |
| M 181/74 | 28.00 | 28.00 | 0.00 | 0.00% | 26.00 | 26.00 | 0.00 | 0.00% | |
| M 184/78 | 28.00 | 28.00 | 0.00 | 0.00% | 30.00 | 30.00 | 0.00 | 0.00% | |
| M 181/74 | 13.00 | 13.00 | 0.00 | 0.00% | 14.00 | 14.00 | 0.00 | 0.00% | |
| M 172/115 | - | - | - | - | 78.00 | 78.00 | 0.00 | 0.00% | |
| F 162/63 | - | - | - | - | - | - | - | - | |
| M 184/85 | 32.00 | 32.00 | 0.00 | 0.00% | 39.00 | 38.00 | 1.00 | 2.63% | |
| F 176/67 | 23.00 | 23.00 | 0.00 | 0.00% | 22.00 | 22.00 | 0.00 | 0.00% | |
| F 169/75 | 58.00 | 58.00 | 0.00 | 0.00% | 52.00 | 53.00 | 1.00 | 1.89% | |
| M 174/72 | 26.00 | 26.00 | 0.00 | 0.00% | 20.00 | 20.00 | 0.00 | 0.00% | |
| M 190/92 | 12.00 | 13.00 | 1.00 | 7.69% | 13.00 | 14.00 | 1.00 | 7.14% | |
| M 177/93 | 23.00 | 23.00 | 0.00 | 0.00% | 20.00 | 20.00 | 0.00 | 0.00% | |
| M 181/76 | 30.00 | 30.00 | 0.00 | 0.00% | 39.00 | 39.00 | 0.00 | 0.00% | |
| Mean | 25.60 | 25.65 | 0.05 | 0.38% | 28.55 | 27.32 | 1.41 | 8.99% |
References
- Banister, E.W. Modeling Elite Athletic Performance. In Physiological Testing of the High-Performance Athlete; MacDougall, J.D., Wenger, H.A., Green, H.J., Canadian Association of Sport Sciences, Eds.; Human Kinetics Books: Champaign, IL, USA, 1991; ISBN 978-0-87322-300-3. [Google Scholar]
- Rusko, H.K.; Pulkkinen, A.; Saalasti, S.; Hynynen, E.; Kihu, J.K. Pre-prediction of epoc: A tool for monitoring fatigue accumulation during exercise? Med. Sci. Sports Exerc. 2003, 35, S183. [Google Scholar] [CrossRef] [Green Version]
- Pulkkinen, A.; Saalasti, S.; Rusko, H. Energy Expenditure Can Be Accurately Estimated from HR without Individual Laboratory Calibration. Med. Sci. Sports Exerc. 2005, 37, S113. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, P.G.; Green, D.J.; Etxebarria, N.; Pyne, D.B.; Saunders, P.U.; Minahan, C.L. Validation of Heart Rate Monitor-Based Predictions of Oxygen Uptake and Energy Expenditure. J. Strength Cond. Res. 2009, 23, 1489–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlot, K.; Cornolo, J.; Borne, R.; Brugniaux, J.V.; Richalet, J.-P.; Chapelot, D.; Pichon, A. Improvement of Energy Expenditure Prediction from Heart Rate during Running. Physiol. Meas. 2014, 35, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.; Hanakam, F.; Wiewelhove, T.; Döweling, A.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Heart Rate Monitoring in Team Sports—A Conceptual Framework for Contextualizing Heart Rate Measures for Training and Recovery Prescription. Front. Physiol. 2018, 9, 639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieman, D.C. Exercise Testing and Prescription: A Health-Related Approach, 7th ed.; McGraw-Hill: Boston, MA, USA, 2011; ISBN 978-0-07-337648-6. [Google Scholar]
- Weippert, M.; Kumar, M.; Kreuzfeld, S.; Arndt, D.; Rieger, A.; Stoll, R. Comparison of Three Mobile Devices for Measuring R–R Intervals and Heart Rate Variability: Polar S810i, Suunto T6 and an Ambulatory ECG System. Eur. J. Appl. Physiol. 2010, 109, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.M.; Gorelick, M. Validity of the Smarthealth Watch to Measure Heart Rate During Rest and Exercise. Meas. Phys. Educ. Exerc. Sci. 2011, 15, 18–25. [Google Scholar] [CrossRef]
- Beeler, N.; Roos, L.; Delves, S.K.; Veenstra, B.J.; Friedl, K.; Buller, M.J.; Wyss, T. The Wearing Comfort and Acceptability of Ambulatory Physical Activity Monitoring Devices in Soldiers. IISE Trans. Occup. Ergon. Hum. Factors 2018, 6, 1–10. [Google Scholar] [CrossRef]
- Navalta, J.W.; Ramirez, G.G.; Maxwell, C.; Radzak, K.N.; McGinnis, G.R. Validity and Reliability of Three Commercially Available Smart Sports Bras during Treadmill Walking and Running. Sci. Rep. 2020, 10, 7397. [Google Scholar] [CrossRef] [PubMed]
- Haddad, M.; Hermassi, S.; Aganovic, Z.; Dalansi, F.; Kharbach, M.; Mohamed, A.O.; Bibi, K.W. Ecological Validation and Reliability of Hexoskin Wearable Body Metrics Tool in Measuring Pre-Exercise and Peak Heart Rate During Shuttle Run Test in Professional Handball Players. Front. Physiol. 2020, 11, 957. [Google Scholar] [CrossRef] [PubMed]
- Föhr, T.; Tolvanen, A.; Myllymäki, T.; Järvelä-Reijonen, E.; Peuhkuri, K.; Rantala, S.; Kolehmainen, M.; Korpela, R.; Lappalainen, R.; Ermes, M.; et al. Physical Activity, Heart Rate Variability-Based Stress and Recovery, and Subjective Stress during a 9-Month Study Period. Scand. J. Med. Sci. Sports 2017, 27, 612–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parak, J.; Tarniceriu, A.; Renevey, P.; Bertschi, M.; Delgado-Gonzalo, R.; Korhonen, I. Evaluation of the Beat-to-Beat Detection Accuracy of PulseOn Wearable Optical Heart Rate Monitor. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 8099–8102. [Google Scholar]
- Delgado-Gonzalo, R.; Parak, J.; Tarniceriu, A.; Renevey, P.; Bertschi, M.; Korhonen, I. Evaluation of Accuracy and Reliability of PulseOn Optical Heart Rate Monitoring Device. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 430–433. [Google Scholar]
- Robertson, A.H.; King, K.; Ritchie, S.D.; Gauthier, A.P.; Laurence, M.; Dorman, S.C. Validating the Use of Heart Rate Variability for Estimating Energy Expenditure. Int. J. Hum. Mov. Sports Sci. 2015, 3, 11–26. [Google Scholar] [CrossRef] [Green Version]

| Parameter | µ ± σ | Range [Min–Max] |
|---|---|---|
| Age (years) | 33.88 ± 8.48 | [23–58] |
| Height (cm) | 176.36 ± 3.96 | [154–193] |
| Weight (kg)) | 78.24 ± 16.18 | [51–115] |
| Body mass index (kg/m2) | 24.99 ± 3.96 | [20–39] |
| Error Type | Strap | Vest |
|---|---|---|
| MAE (bpm) | 0.93 | 3.82 |
| MAPE (%) | 0.76 | 3.32 |
| Reliability (%) | 94.61 | 96.68 |
| Accuracy (%) | 99.24 | 84.70 |
| Title 1 | Strap | Vest |
|---|---|---|
| MAE (ms) | 6.54 | 25.14 |
| MAPE (%) | 1.31 | 5.02 |
| Correct beats (%) | 99.21 | 96.28 |
| Missing beats (%) | 0.31 | 0.96 |
| Extra beats (%) | 0.48 | 2.76 |
| Parameter | Error Type | Strap | Vest |
|---|---|---|---|
| Average HR (bpm) | Bias (ME) (bpm) | −0.05 | 1.77 |
| MAE (bpm) | 0.05 | 2.23 | |
| MAPE (%) | 0.04 | 2.18 | |
| RMSE (bpm) | 0.22 | 42.99 | |
| Correlation coefficient | r = 0.99, (p < 0.001) (2Pe) | r = 0.96, (p < 0.001) (2Pe) | |
| Energy Expenditure, Total (kcal) | Bias (ME) (kcal) | −2.32 | 3.73 |
| MAE (kcal) | 3.22 | 9.45 | |
| MAPE (%) | 1.70 | 6.63 | |
| RMSE (kcal) | 4.42 | 19.80 | |
| Correlation coefficient | r = 0.99, (p < 0.001) (2Pe) | ρ = 0.93, (p < 0.001) (1Sp) | |
| EPOC Peak (ml/kg) | Bias (ME) ((mL/kg) | −0.73 | 0.46 |
| MAE ((mL/kg) | 1.08 | 3.82 | |
| MAPE (%) | 3.90 | 54.15 | |
| RMSE (mL/kg) | 1.57 | 7.69 | |
| Correlation coefficient | ρ = 0.99, (p < 0.001) (1Sp) | ρ = 0.89, (p < 0.001) (1Sp) | |
| TRIMP (index) | Bias (ME) (index) | −0.05 | 1.23 |
| MAE (index) | 0.05 | 1.41 | |
| MAPE (%) | 0.38 | 8.99 | |
| RMSE | 0.01 | 3.84 | |
| Correlation coefficient | ρ = 0.99, (p < 0.001) (1Sp) | ρ = 0.94, (p < 0.001) (1Sp) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parak, J.; Salonen, M.; Myllymäki, T.; Korhonen, I. Comparison of Heart Rate Monitoring Accuracy between Chest Strap and Vest during Physical Training and Implications on Training Decisions. Sensors 2021, 21, 8411. https://doi.org/10.3390/s21248411
Parak J, Salonen M, Myllymäki T, Korhonen I. Comparison of Heart Rate Monitoring Accuracy between Chest Strap and Vest during Physical Training and Implications on Training Decisions. Sensors. 2021; 21(24):8411. https://doi.org/10.3390/s21248411
Chicago/Turabian StyleParak, Jakub, Mikko Salonen, Tero Myllymäki, and Ilkka Korhonen. 2021. "Comparison of Heart Rate Monitoring Accuracy between Chest Strap and Vest during Physical Training and Implications on Training Decisions" Sensors 21, no. 24: 8411. https://doi.org/10.3390/s21248411