Augmentative and Alternative Communication (AAC) Advances: A Review of Configurations for Individuals with a Speech Disability


Abstract
:1. Introduction
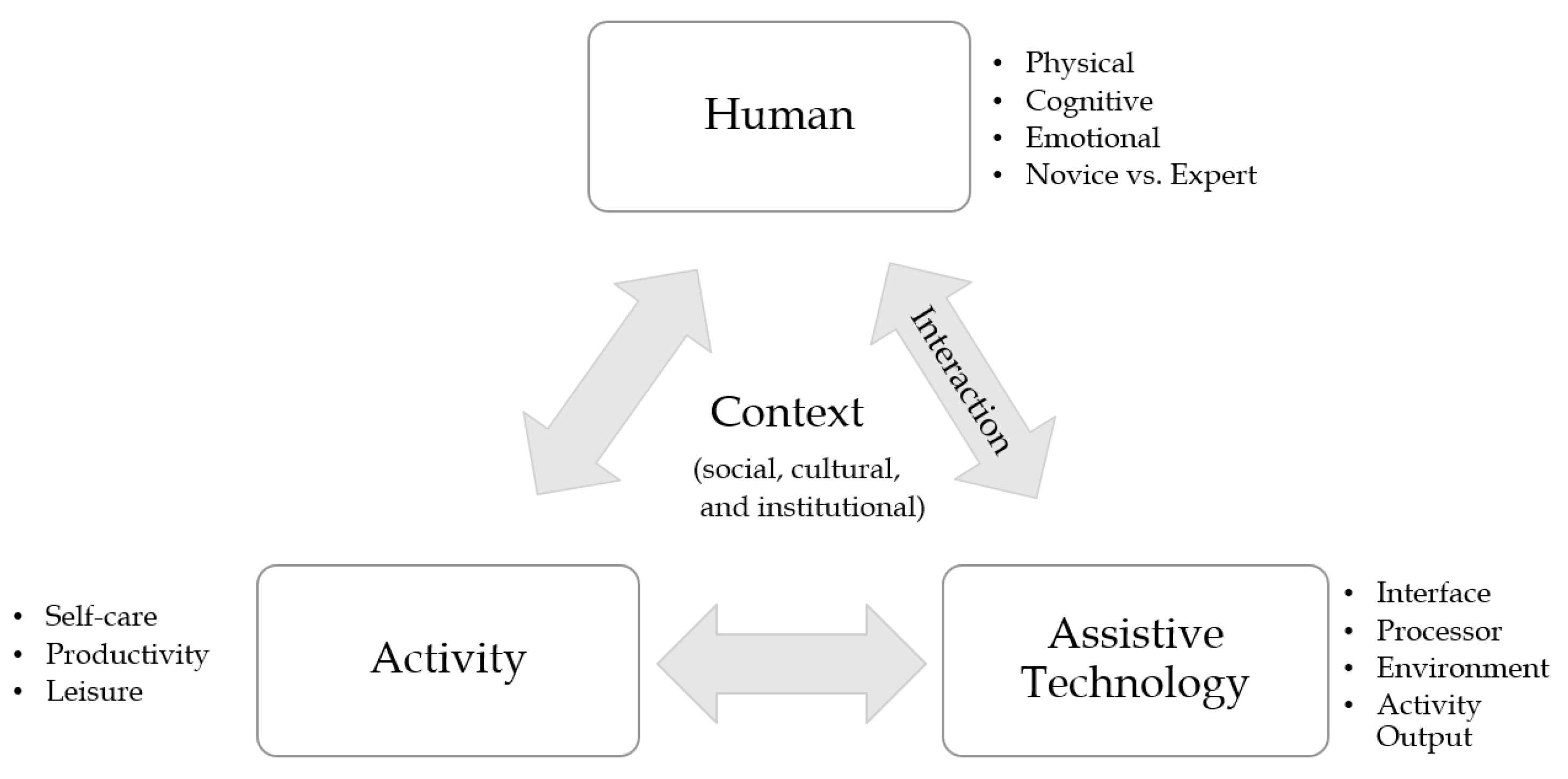
2. Human Interaction
3. Sensing Modalities and Their Functionalities
3.1. AAC Signal Sources and Associated Processing
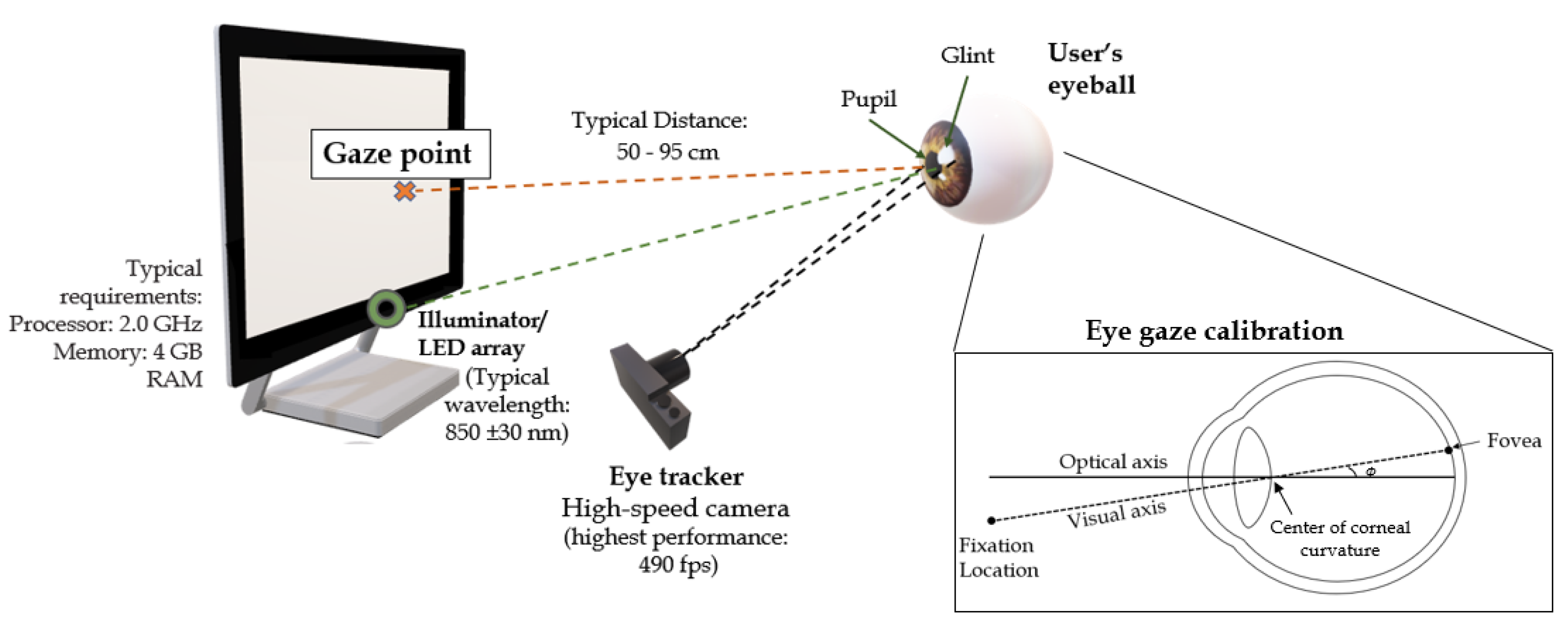
3.1.1. Imaging Methods
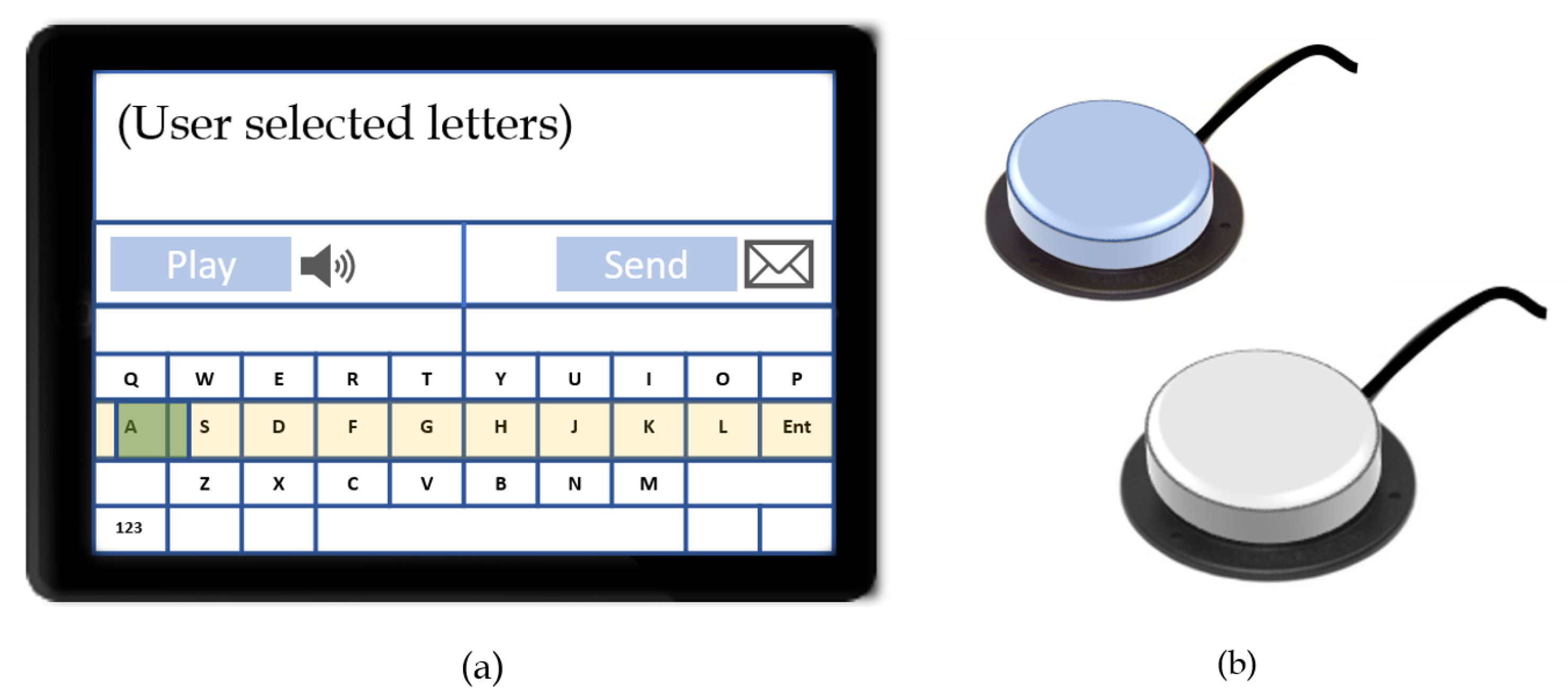
3.1.2. Mechanical and Electro-Mechanical Methods
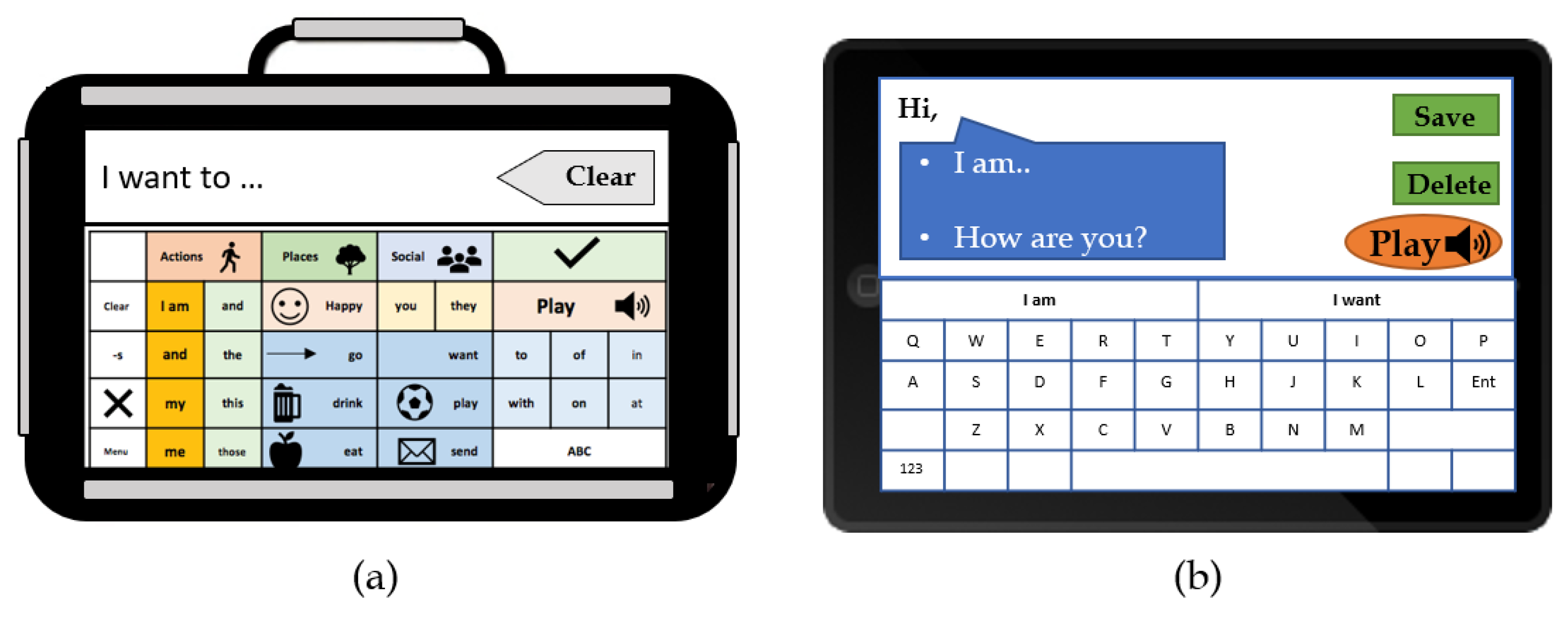
3.1.3. Touch-Activated Systems
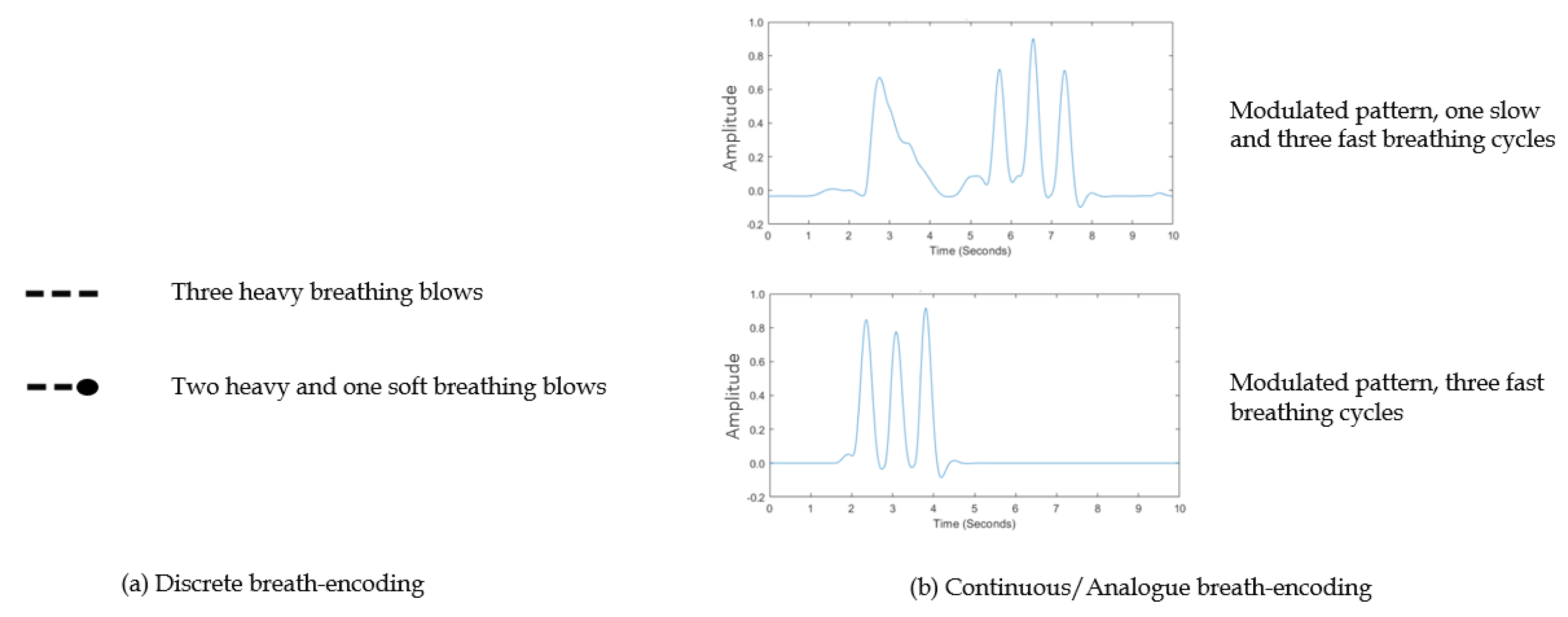
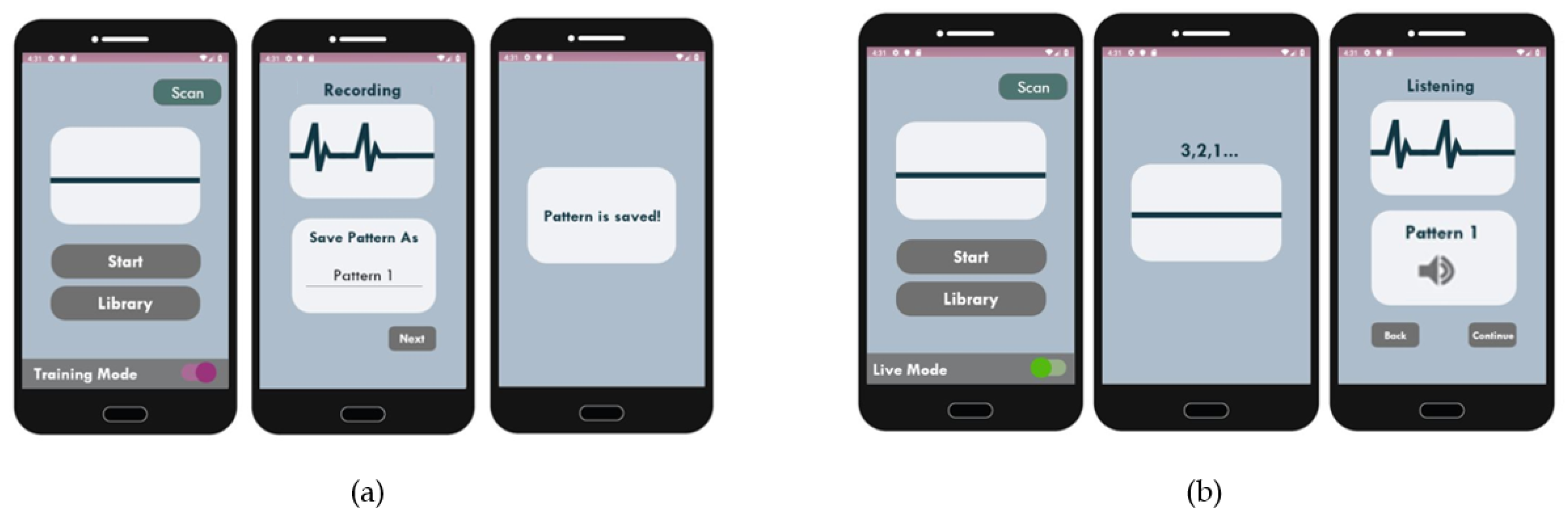
3.1.4. Breath-Activated Systems
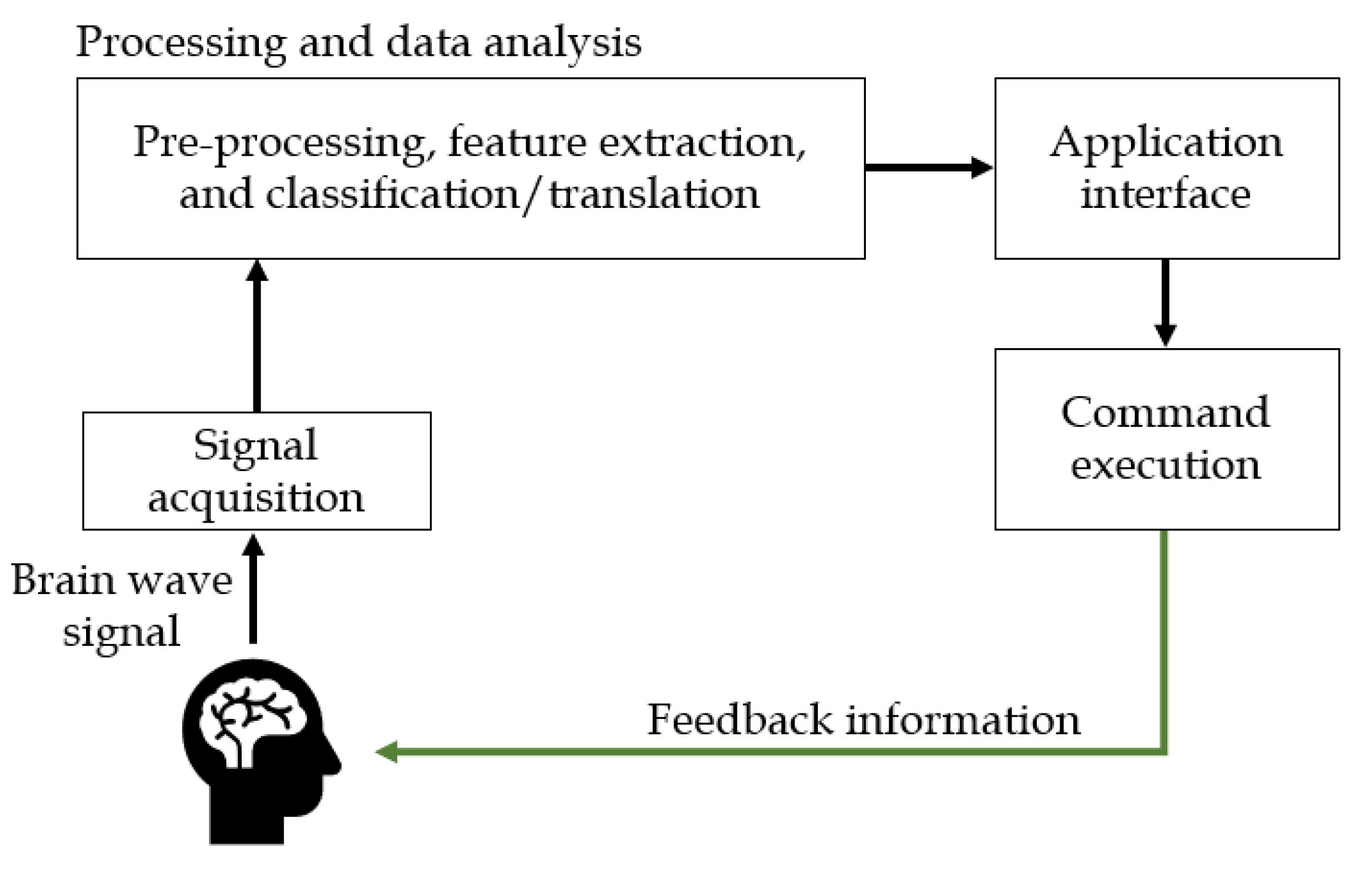
3.1.5. Brain–Computer Interface Methods
3.2. Machine and Deep Learning
3.3. Outputs and Speech Generating Devices
4. Comparison of Existing AAC Signal Sensing Methods
4.1. Ease of Access
4.2. Affordability
4.3. Ease of Programming and Maintaining
4.4. Portability
4.5. Conversational Rates
5. Conclusions
6. Future Research and Prospective Advances in AAC
6.1. Signal Sources and Usable Information Content
6.2. Intelligent AAC, DL functionalities, and NLP
6.3. Mobile APP Integration and Mobile Health Applications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AAC | augmentative and alternative communication |
| AI | artificial intelligence |
| ALS | Amyotrophic Lateral Sclerosis |
| APP | applications |
| AR | auto-regressive |
| ASD | Autistic Spectrum Disorders |
| AT | assistive technology |
| BCI | brain computer interface |
| DL | deep learning |
| EEG | electroencephalogram |
| fMRI | functional magnetic resonance imaging |
| HAAT | Human Activity Assistive Technology |
| IR | Infrared |
| IR-PCR | Infrared pupil corneal reflection |
| LIS | Locked-in-Syndrome |
| MEG | magnetoencephalography |
| MEMS | micro-electro-mechanical systems |
| ML | machine learning |
| MSE | mean square error |
| NIR | near-infrared |
| NIRS | near-infrared spectroscopy |
| NLP | natural language processing |
| PPG | photoplethysmogram |
| SGD | speech generating device |
| SLCN | speech, language or communication need |
| SMSW | synthesized machine spoken words |
| VOCA | voice output communication aid |
| WPM | words per minute |
References
- García-Méndez, S.; Fernández-Gavilanes, M.; Costa-Montenegro, E.; Juncal-Martínez, J.; Javier González-Castaño, F. Automatic natural language generation applied to alternative and augmentative communication for online video content services using simple NLG for Spanish. In Proceedings of the 15th Web for All Conference: Internet of Accessible Things, Lyon, France, 23–27 April 2018. [Google Scholar]
- Kerr, D.; Bouazza-Marouf, K.; Gaur, A.; Sutton, A.; Green, R. A breath controlled AAC system. In Proceedings of the CM2016 National AAC Conference, Orlando, FL, USA, 19–22 April 2016; pp. 11–13. [Google Scholar]
- Schultz Ascari, R.E.O.; Pereira, R.; Silva, L. Mobile Interaction for Augmentative and Alternative Communication: A Systematic Mapping. SBC J. Interact. Syst. 2018, 9, 105–118. [Google Scholar]
- Cook, A.M.; Polgar, J.M. Assistive Technologies Principles and Practices, 4th ed.; Elsevier: New York, NY, USA, 2015. [Google Scholar]
- Smith, A. Speech motor development: Integrating muscles, movements, and linguistic units. J. Commun. Disord. 2006, 39, 331–349. [Google Scholar] [CrossRef] [PubMed]
- van de Sandt-Koenderman, M.W.M.E. High-tech AAC and aphasia: Widening horizons? Aphasiology 2004, 18, 245–263. [Google Scholar] [CrossRef]
- Light, J.; McNaughton, D. The Changing Face of Augmentative and Alternative Communication: Past, Present, and Future Challenges. Augment. Altern. Commun. 2012, 28, 197–204. [Google Scholar] [CrossRef]
- Hodge, S. Why is the potential of augmentative and alternative communication not being realized? Exploring the experiences of people who use communication aids. Disabil. Soc. 2007, 22, 457–471. [Google Scholar] [CrossRef]
- Mirenda, P. Toward Functional Augmentative and Alternative Communication for Students With Autism. Lang. Speech Hear. Serv. Sch. 2003, 34, 203–216. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Augmentative and Alternative Communication and Voice Products and Technologies. In The Promise of Assistive Technology to Enhance Activity and Work Participation; The National Academies Press: Washington, DC, USA, 2017; pp. 209–310. [Google Scholar]
- Smith, E.; Delargy, M. Locked-in syndrome. Br. Med. J. 2005, 330, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Simion, E. Augmentative and Alternative Communication—Support for People with Severe Speech Disorders. Procedia-Soc. Behav. Sci. 2014, 128, 77–81. [Google Scholar] [CrossRef]
- Arthanat, S.; Bauer, S.M.; Lenker, J.A.; Nochajski, S.M.; Wu, Y.W.B. Conceptualization and measurement of assistive technology usability. Disabil. Rehabil. Assist. Technol. 2007, 2, 235–248. [Google Scholar] [CrossRef]
- Giesbrecht, E. Application of the human activity assistive technology model for occupational therapy research. Aust. Occup. Ther. J. 2013, 60, 230–240. [Google Scholar] [CrossRef]
- Iacono, T.; Lyon, K.; Johnson, H.; West, D. Experiences of adults with complex communication needs receiving and using low tech AAC: An Australian context. Disabil. Rehabil. Assist. Technol. 2013, 8, 392–401. [Google Scholar] [CrossRef]
- McNaughton, D.; Light, J. The iPad and mobile technology revolution: Benefits and challenges for individuals who require augmentative and alternative communication. AAC Augment. Altern. Commun. 2013, 29, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Shane, H.C.; Blackstone, S.; Vanderheiden, G.; Williams, M.; Deruyter, F. Using AAC technology to access the world. Assist. Technol. 2012, 24, 3–13. [Google Scholar] [CrossRef]
- Baxter, S.; Enderby, P.; Evans, P.; Judge, S. Barriers and facilitators to the use of high-technology augmentative and alternative communication devices: A systematic review and qualitative synthesis. Int. J. Lang. Commun. Disord. 2012, 47, 115–129. [Google Scholar] [CrossRef]
- Glennen, S.L. Augmentative and alternative communication systems. In The Handbook of Augmentative and Alternative Communication; Cengage Learning: Boston, MA, USA, 1997; pp. 59–69. ISBN 9780323096317. [Google Scholar]
- Tobii Dynavox PCEye Plus. Available online: https://www.tobiidynavox.com/devices/eye-gaze-devices/pceye-plus/ (accessed on 10 February 2019).
- Chennamma, H.R.; Yuan, X. A Survey on Eye-Gaze Tracking Techniques. Indian J. Comput. Sci. Eng. 2013, 4, 388–393. [Google Scholar]
- Kar, A.; Corcoran, P. A review and analysis of eye-gaze estimation systems, algorithms and performance evaluation methods in consumer platforms. IEEE Access 2017, 5, 16495–16519. [Google Scholar] [CrossRef]
- Hansen, D.W.; Ji, Q. In the Eye of the Beholder: A Survey of Models for Eyes and Gaze. IEEE Trans. Pattern Anal. Mach. Intell. 2010, 32, 478–500. [Google Scholar] [CrossRef] [PubMed]
- Townend, G.S.; Marschik, P.B.; Smeets, E.; van de Berg, R.; van den Berg, M.; Curfs, L.M.G. Eye Gaze Technology as a Form of Augmentative and Alternative Communication for Individuals with Rett Syndrome: Experiences of Families in The Netherlands. J. Dev. Phys. Disabil. 2016, 28, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-H.K.; O’Leary, M. Eye Gaze 101: What Speech-Language Pathologists Should Know About Selecting Eye Gaze Augmentative and Alternative Communication Systems. Perspect. ASHA Spec. Interes. Groups 2018, 3, 24–32. [Google Scholar] [CrossRef]
- Ball, L.; Nordness, A.; Fager, S.; Kersch, K.; Mohr, B.; Pattee, G.L.; Beukelman, D. Eye-Gaze Access to AAC Technology for People with Amyotrophic Lateral Sclerosis. J. Med. Speech. Lang. Pathol. 2010, 18, 11–23. [Google Scholar]
- Corno, F.; Farinetti, L.; Signorile, I.; Torino, P. A Cost-effective solution for eye-gaze assistive technology. In Proceedings of the IEEE International Conference on Multimedia and Expo, Lausanne, Switzerland, 26–29 August 2002; pp. 433–436. [Google Scholar]
- Majaranta, P.; Aoki, H.; Donegan, M.; Hansen, D.W.; Hansen, J.P. Gaze Interaction and Applications of Eye Tracking: Advances in Assistive Technologies; IGI Publishing: Hershey, PA, USA, 2011. [Google Scholar]
- Bates, R.; Donegan, M.; Istance, H.O.; Hansen, J.P.; Räihä, K.J. Introducing COGAIN: Communication by gaze interaction. Univ. Access Inf. Soc. 2007, 6, 159–166. [Google Scholar] [CrossRef]
- Bates, R.; Istance, H.; Oosthuizen, L.; Majaranta, P. Survey of De-Facto Standards in Eye Tracking; Communication by Gaze Interaction; Information Society Technologies: Tallinn, Estonia, 2005. [Google Scholar]
- Al-Rahayfeh, A.; Faezipour, M. Eye Tracking and Head Movement Detection: A State-of-Art Survey. IEEE J. Transl. Eng. Heal. Med. 2013, 1, 2100212. [Google Scholar] [CrossRef]
- Janthanasub, V. Ophapasai: Augmentative and Alternative Communication Based on Video-Oculography Control Interface. Appl. Mech. Mater. 2016, 848, 60–63. [Google Scholar] [CrossRef]
- Tai, K.; Blain, S.; Chau, T. A Review of Emerging Access Technologies for Individuals With Severe Motor Impairments. Assist. Technol. 2008, 20, 204–221. [Google Scholar] [CrossRef]
- Harezlak, K.; Kasprowski, P. Application of eye tracking in medicine: A survey, research issues and challenges. Comput. Med. Imaging Graph. 2018, 65, 176–190. [Google Scholar] [CrossRef]
- van der Geest, J.N.; Frens, M.A. Recording eye movements with video-oculography and scleral search coils: A direct comparison of two methods. J. Neurosci. Methods 2002, 114, 185–195. [Google Scholar] [CrossRef]
- Robinsont, D. A Method of Measuring Eye Movement Using a Scleral Search Coil in a Magnetic Field. IEEE Trans. Bio-Med. Electron. 1963, 10, 137–145. [Google Scholar]
- Tobii Technology Accuracy and Precision Test Method for Remote Eye Trackers—Test Specification Report. 2011. Available online: https://stemedhub.org/resources/3311/download/Tobii_Test_Specifications_Accuracy_and_PrecisionTestMethod_version_2_1_1_.pdf (accessed on 7 February 2011).
- Farivar, R.; Michaud-Landry, D. Construction and Operation of a High-Speed, High-Precision Eye Tracker for Tight Stimulus Synchronization and Real-Time Gaze Monitoring in Human and Animal Subjects. Front. Syst. Neurosci. 2016, 10, 1–10. [Google Scholar] [CrossRef]
- Schwiegerling, J.T. Eye Axes and Their Relevance to Alignment of Corneal Refractive Procedures. J. Refract. Surg. 2013, 29, 515–516. [Google Scholar] [CrossRef] [PubMed]
- Salvucci, D.D.; Goldberg, J.H. Identifying fixations and saccades in eye-tracking protocols. In Proceedings of the Symposium on Eye Tracking Research & Applications, Palm Beach Gardens, FL, USA, 6–8 November 2000; pp. 71–78. [Google Scholar]
- Poole, A.; Ball, L.J. Eye Tracking in Human-Computer Interaction and Usability Research: Current Status and Future Prospects. Available online: http://citeseer.ist.psu.edu/viewdoc/summary?doi=10.1.1.95.5691 (accessed on 1 January 2005).
- Kunka, B.; Kostek, B. Non-intrusive infrared-free eye tracking method. In Proceedings of the Signal Processing Algorithms, Architectures, Arrangements, and Applications Conference Proceedings (SPA), Poznan, Poland, 24–26 September 2009; pp. 105–109. [Google Scholar]
- Talk To Me Technologies. Eyespeak. Available online: https://www.talktometechnologies.com/pages/eyespeak (accessed on 9 April 2019).
- IntelliGaze by Alea Technologies. IntelliGaze. Available online: https://www.intelligaze.com/en/ (accessed on 9 April 2019).
- EagleEyes. Available online: https://ofoa.net/eagleeyes/ (accessed on 9 April 2019).
- MacKenzie, I.S.; Ashtiani, B. BlinkWrite: Efficient text entry using eye blinks. Univ. Access Inf. Soc. 2011, 10, 69–80. [Google Scholar] [CrossRef]
- Bhalla, M.R.; Bhalla, A.V. Comparative Study of Various Touchscreen Technologies. Int. J. Comput. Appl. 2010, 6, 12–18. [Google Scholar] [CrossRef]
- Lee, D. The State of the Touch-Screen Panel Market in 2011. Inf. Disp. 2011, 27, 12–16. [Google Scholar] [CrossRef]
- Qin, H.; Cai, Y.; Dong, J.; Lee, Y.-S. Direct Printing of Capacitive Touch Sensors on Flexible Substrates by Additive E-Jet Printing With Silver Nanoinks. J. Manuf. Sci. Eng. 2017, 139, 31011. [Google Scholar] [CrossRef]
- Intuary Inc. Verbally. Available online: http://verballyapp.com/index.html (accessed on 9 April 2019).
- AssistiveWare. Proloquo2Go. Available online: https://www.assistiveware.com/products/proloquo2go (accessed on 9 April 2019).
- Therapy Box. Predictable TM. Available online: https://therapy-box.co.uk/predictable (accessed on 9 April 2019).
- Massaroni, C.; Venanzi, C.; Silvatti, A.; Lo Presti, D.; Saccomandi, P.; Formica, D.; Giurazza, F.; Caponero, M.; Schena, E. Smart textile for respiratory monitoring and thoraco-abdominal motion pattern evaluation. J. Biophotonics 2018, 11, e201700263. [Google Scholar] [CrossRef]
- Itasaka, Y.; Miyazaki, S.; Tanaka, T.; Shibata, Y.; Ishikawa, K. Detection of Respiratory Events during Polysomnography—Nasal-Oral Pressure Sensor Versus Thermocouple Airflow Sensor. Pract. Oto-Rhino-Laryngol. 2010, 129, 60–63. [Google Scholar] [CrossRef]
- Zhang, X.; Ding, Q. Respiratory rate monitoring from the photoplethysmogram via sparse signal reconstruction. Physiol. Meas. 2016, 37, 1105–1119. [Google Scholar] [CrossRef]
- Yahya, O.; Faezipour, M. Automatic detection and classification of acoustic breathing cycles. In Proceedings of the 2014 Zone 1 Conference of the American Society for Engineering Education, Bridgeport, CT, USA, 3–5 April 2014. [Google Scholar]
- Elsahar, Y.; Bouazza-Marouf, K.; Kerr, D.; Gaur, A.; Kaushik, V.; Hu, S. Breathing pattern interpretation as an alternative and effective voice communication solution. Biosensors 2018, 8, 48. [Google Scholar] [CrossRef]
- Shorrock, T.; MacKay, D.; Ball, C. Efficient Communication by Breathing. In Deterministic and Statistical Methods in Machine Learning; Springer: Heidelberg/Berlin, Germany, 2005; pp. 88–97. [Google Scholar]
- Plotkin, A.; Sela, L.; Weissbrod, A.; Kahana, R.; Haviv, L.; Yeshurun, Y.; Soroker, N.; Sobel, N. Sniffing enables communication and environmental control for the severely disabled. Proc. Natl. Acad. Sci. USA 2010, 107, 14413–14418. [Google Scholar] [CrossRef]
- Fager, S.; Bardach, L.; Russell, S.; Higginbotham, J. Access to augmentative and alternative communication: New technologies and clinical decision-making. J. Pediatr. Rehabil. Med. 2012, 5, 53–61. [Google Scholar]
- Garcia, R.G.; Ibarra, J.B.G.; Paglinawan, C.C.; Paglinawan, A.C.; Valiente, L.; Sejera, M.M.; Bernal, M.V.; Cortinas, W.J.; Dave, J.M.; Villegas, M.C. Wearable augmentative and alternative communication device for paralysis victims using Brute Force Algorithm for pattern recognition. In Proceedings of the 2017 IEEE 9th International Conference on Humanoid, Nanotechnology, Information Technology, Communication and Control, Environment and Management (HNICEM), Manila, Philippines, 1–3 December 2017; pp. 1–6. [Google Scholar]
- Voiceitt. Available online: http://www.voiceitt.com/why-voiceitt.html (accessed on 9 April 2019).
- Chaudhary, U.; Birbaumer, N.; Curado, M.R. Brain-Machine Interface (BMI) in paralysis. Ann. Phys. Rehabil. Med. 2015, 58, 9–13. [Google Scholar] [CrossRef]
- Birbaumer, N.; Murguialday, A.R.; Cohen, L. Brain-computer interface in paralysis. Curr. Opin. Neurol. 2008, 21, 634–638. [Google Scholar] [CrossRef]
- Yeo, M.; Jiang, L.; Tham, E.; Xiong, W. Evaluation of a low-cost alternative communication device with brain control. In Proceedings of the 2015 10th IEEE Conference on Industrial Electronics and Applications, ICIEA 2015, Auckland, New Zealand, 15–17 June 2015; pp. 229–232. [Google Scholar]
- Kaiser, V.; Bauernfeind, G.; Kreilinger, A.; Kaufmann, T.; Kübler, A.; Neuper, C.; Müller-Putz, G.R. Cortical effects of user training in a motor imagery based brain-computer interface measured by fNIRS and EEG. Neuroimage 2014, 85, 432–444. [Google Scholar] [CrossRef]
- Hippe, Z.S.; Kulikowski, J.L.; Mroczek, T.; Wtorek, J. A Robust Asynchronous SSVEP Brain-Computer Interface Based On Cluster Analysis of Canonical Correlation Coefficients. Adv. Intell. Syst. Comput. 2014, 300, 3–14. [Google Scholar]
- Chen, X.; Wang, Y.; Nakanishi, M.; Gao, X.; Jung, T.-P.; Gao, S. High-speed spelling with a noninvasive brain–computer interface. Proc. Natl. Acad. Sci. USA 2015, 112, E6058–E6067. [Google Scholar] [CrossRef]
- Tan, P.; Tan, G.; Cai, Z. Dual-tree complex wavelet transform-based feature extraction for brain computer interface. In Proceedings of the 12th International Conference on Fuzzy Systems and Knowledge Discovery, FSKD 2015, Zhangjiajie, China, 15–17 August 2015; pp. 1136–1140. [Google Scholar]
- Thomas, J.; Maszczyk, T.; Sinha, N.; Kluge, T.; Dauwels, J. Deep learning-based classification for brain-computer interfaces. In Proceedings of the 2017 IEEE International Conference on Systems, Man, and Cybernetics, SMC 2017, San Diego, CA, USA, 5–8 October 2017; pp. 234–239. [Google Scholar]
- Gupta, A.; Parameswaran, S.; Lee, C.H. Classification of electroencephalography (EEG) signals for different mental activities using Kullback Leibler (KL) divergence. In Proceedings of the ICASSP, IEEE International Conference on Acoustics, Speech and Signal Processing, Taipei, Taiwan, 19–24 April 2009; pp. 1697–1700. [Google Scholar]
- Lotte, F.; Congedo, M.; Lécuyer, A.; Lamarche, F.; Arnaldi, B. A review of classification algorithms for EEG-based brain-computer interfaces. J. Neural Eng. 2007, 4, R1–R13. [Google Scholar] [CrossRef]
- Zhang, Y.; Ji, X.; Zhang, Y. Classification of EEG signals based on AR model and approximate entropy. In Proceedings of the 2015 International Joint Conference on Neural Networks (IJCNN), Killarney, Ireland, 12–17 July 2015. [Google Scholar]
- Guger, C.; Schlögl, A.; Neuper, C.; Walterspacher, D.; Strain, T.; Pfurtscheller, G. Rapid prototyping of an EEG-based brain-computer interface (BCI). IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 49–58. [Google Scholar] [CrossRef]
- Ortiz-Rosario, A.; Adeli, H. Brain-computer interface technologies: From signal to action. Rev. Neurosci. 2013, 24, 537–552. [Google Scholar] [CrossRef]
- Choi, B.; Jo, S. A Low-Cost EEG System-Based Hybrid Brain-Computer Interface for Humanoid Robot Navigation and Recognition. PLoS ONE 2013, 8, e74583. [Google Scholar] [CrossRef]
- Nijboer, F.; Plass-Oude Bos, D.; Blokland, Y.; van Wijk, R.; Farquhar, J. Design requirements and potential target users for brain-computer interfaces–recommendations from rehabilitation professionals. Brain-Comput. Interfaces 2014, 1, 50–61. [Google Scholar] [CrossRef]
- McFarland, D.J.; Wolpaw, J.R. Brain–computer interface use is a skill that user and system acquire together. PLoS Biol. 2018, 16, 10–13. [Google Scholar] [CrossRef]
- Perdikis, S.; Tonin, L.; Saeedi, S.; Schneider, C.; Millán, J. del R. The Cybathlon BCI race: Successful longitudinal mutual learning with two tetraplegic users. PLoS Biol. 2018, 16, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Nuyujukian, P.; Albites Sanabria, J.; Saab, J.; Pandarinath, C.; Jarosiewicz, B.; Blabe, C.H.; Franco, B.; Mernoff, S.T.; Eskandar, E.N.; Simeral, J.D.; et al. Cortical control of a tablet computer by people with paralysis. PLoS ONE 2018, 13, e0204566. [Google Scholar] [CrossRef]
- Yu, T.; Li, Y.; Long, J.; Gu, Z. Surfing the Internet with a BCI mouse. J. Neural Eng. 2012, 9, 036012. [Google Scholar] [CrossRef]
- Karim, A.A.; Hinterberger, T.; Richter, J.; Mellinger, J.; Neumann, N.; Flor, H.; Kübler, A.; Birbaumer, N. Neural Internet: Web surfing with brain potentials for the completely paralyzed. Neurorehabil. Neural Repair 2006, 20, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Pennington, C.; McCoy, K.F.; Trnka, K.; McCaw, J.; Yarrington, D. The effects of word prediction on communication rate for AAC. In Proceedings of the NAACL HLT 2007, Rochester, NY, USA, Rochester, NY, USA, 26 April 2007; pp. 173–176. [Google Scholar]
- Alomari, M.H.; Abubaker, A.; Turani, A.; Baniyounes, A.M.; Manasreh, A. EEG Mouse: A Machine Learning-Based Brain Computer Interface. Int. J. Adv. Comput. Sci. Appl. 2014, 5, 193–198. [Google Scholar]
- Higginbotham, D.J.; Lesher, G.W.; Moulton, B.J.; Roark, B. The application of natural language processing to augmentative and alternative communication. Assist. Technol. 2012, 24, 14–24. [Google Scholar] [CrossRef]
- Trnka, K.; Yarrington, D.; McCoy, K.; Pennington, C. Topic modeling in fringe word prediction for AAC. In Proceedings of the 11th International Conference on Intelligent User Interfaces, Sydney, Australia, 29 January–1 February 2006; pp. 276–282. [Google Scholar]
- Müller, K.R.; Krauledat, M.; Dornhege, G.; Curio, G.; Blankertz, B. Machine Learning and Applications for Brain-Computer Interfacing. In Human Interface and the Management of Information. Methods, Techniques and Tools in Information Design; Springer: Berlin/Heidelberg, Germany, 2007; Volume 4557, p. 132. [Google Scholar]
- Shenoy, P.; Krauledat, M.; Blankertz, B.; Rao, R.P.N.; Müller, K.R. Towards adaptive classification for BCI. J. Neural Eng. 2006, 3, R13–R23. [Google Scholar] [CrossRef]
- McFarland, D.J.; Wolpaw, J.R. Brain-Computer Interfaces for Communication and Control. ACM Commun. 2011, 54, 60–66. [Google Scholar] [CrossRef]
- Mainsah, B.O.; Collins, L.M.; Colwell, K.A.; Sellers, E.W.; Ryan, D.B.; Caves, K.; Throckmorton, C.S. Increasing BCI communication rates with dynamic stopping towards more practical use: An ALS study. J. Neural Eng. 2015, 12, 16013. [Google Scholar] [CrossRef]
- Hussein, A.; Adda, M.; Atieh, M.; Fahs, W. Smart home design for disabled people based on neural networks. Procedia Comput. Sci. 2014, 37, 117–126. [Google Scholar] [CrossRef]
- Alamsaputra, D.M.; Kohnert, K.J.; Munson, B.; Reichle, J. Synthesized speech intelligibility among native speakers and non-native speakers of English. Augment. Altern. Commun. 2006, 22, 258–268. [Google Scholar] [CrossRef]
- Beukelman, D.R.; Mirenda, P. Augmentative and Alternative Communication: Supporting Children and Adults with Complex Communication Needs, 4th ed.; Paul H. Brookes Pub.: Baltimore, MD, USA, 2013. [Google Scholar]
- Zhang, X.; Kulkarni, H.; Morris, M.R. Smartphone-Based Gaze Gesture Communication for People with Motor Disabilities. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; pp. 2878–2889. [Google Scholar]
- Villanueva, A.; Cabeza, R.; Porta, S. Eye tracking system model with easy calibration. In Proceedings of the 2004 symposium on Eye Tracking Research & Applications, San Antonio, TX, USA, 2004; Volume 1, p. 55. [Google Scholar]
- Sellers, E.W.; Vaughan, T.M.; Wolpaw, J.R. A brain-computer interface for long-term independent home use. Amyotroph. Lateral Scler. 2010, 11, 449–455. [Google Scholar] [CrossRef]
- Brumberg, J.S.; Pitt, K.M.; Mantie-Kozlowski, A.; Burnison, J.D. Brain–computer interfaces for augmentative and alternative communication: A tutorial. Am. J. Speech-Lang. Pathol. 2018, 27, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Abdulkader, S.N.; Atia, A.; Mostafa, M.-S.M. Brain computer interfacing: Applications and challenges. Egypt. Inform. J. 2015, 16, 213–230. [Google Scholar] [CrossRef]
- Kumar, M. Reducing the Cost of Eye Tracking Systems. Citeseer 2008, 4. Available online: https://hci.stanford.edu/research/GUIDe/publications/Stanford%20CSTR2006-08%20-%20Reducing%20the%20Cost%20of%20Eye-Gaze%20Tracking%20Systems.pdf (accessed on 1 January 2006).
- Light, J.; McNaughton, D.; Beukelman, D.; Fager, S.K.; Fried-Oken, M.; Jakobs, T.; Jakobs, E. Challenges and opportunities in augmentative and alternative communication: Research and technology development to enhance communication and participation for individuals with complex communication needs. AAC Augment. Altern. Commun. 2019, 35, 1–12. [Google Scholar] [CrossRef]
- Courtney, V.E.; Koverb, S.T. An Open Conversation on Using Eye-Gaze Methods in Studies of Neurodevelopmental Disorders. J. Speech Lang. Hear. Res. 2015, 58, 1719–1732. [Google Scholar]
- Kok, E.M.; Jarodzka, H. Before your very eyes: The value and limitations of eye tracking in medical education. Med. Educ. 2017, 51, 114–122. [Google Scholar] [CrossRef]
- Wang, Y.T.; Wang, Y.; Cheng, C.K.; Jung, T.P. Developing stimulus presentation on mobile devices for a truly portable SSVEP-based BCI. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Osaka, Japan, 3–7 July 2013; pp. 5271–5274. [Google Scholar]
- Waller, A. Telling tales: Unlocking the potential of AAC technologies. Int. J. Lang. Commun. Disord. 2019, 1–11. [Google Scholar] [CrossRef]
- Tauroza, S.; Allison, D. Speech rates in British English. Appl. Linguist. 1990, 11, 90–105. [Google Scholar] [CrossRef]
- Wilkinson, K.M.; Mitchell, T. Eye Tracking Research to Answer Questions about Augmentative and Alternative Communication Assessment and Intervention. Augment. Altern. Commun. 2015, 30, 106–119. [Google Scholar] [CrossRef]
- Costigan, F.A.; Newell, K.M. An analysis of constraints on access to augmentative communication in cerebral palsy. Can. J. Occup. Ther. 2009, 76, 153–161. [Google Scholar] [CrossRef]
- Kumar, S.; Aishwaraya, B.K.; Bhanutheja, K.N.; Chaitra, M. Breath to speech communication with fall detection for Elder/Patient with take care analytics. In Proceedings of the 2016 IEEE International Conference on Recent Trends in Electronics, Information & Communication Technology (RTEICT), Bangalore, India, 20–21 May 2016; pp. 527–531. [Google Scholar]
- Moore, M.M. Real-World Applications for Brain—Computer Interface Technology. IEEE Trans. Neural Syst. Rehabil. Eng. 2003, 11, 162–165. [Google Scholar] [CrossRef]
- Ruan, S.; Wobbrock, J.O.; Liou, K.; Ng, A.; Landay, J. Speech is 3x faster than typing for english and mandarin text entry on mobile devices. arXiv 2016, arXiv:1608.07323. [Google Scholar]
- Leo, M.; Furnari, A.; Medioni, G.G.; Trivedi, M.; Farinella, G.M. Deep Learning for Assistive Computer Vision. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; p. 11134. [Google Scholar]
- Baxter, S.; Enderby, P.; Evans, P.; Judge, S. Interventions using high-technology communication devices: A state of the art review. Folia Phoniatr. Logop. 2012, 64, 137–144. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signal Sensing Category | Activation Method |
|---|---|
| Imaging methods | Eye gaze systems, head-pointing devices |
| Mechanical and Electromechanical methods | Mechanical keyboards, switch access |
| Touch-activated methods | Touchscreens, touch membrane keyboards |
| Breath-activated methods | Microphones, low-pressure sensors |
| Brain–Computer Interface methods | Invasive and non-invasive |
| Signal Source | Mode | Typical Hardware Requirements | Areas of Strength | Limitations and Areas of Improvement |
|---|---|---|---|---|
| Imaging methods | Eye gazing |
| ||
| Head-pointing |
| Less expensive compared to typical eye-gaze systems |
| |
| Mechanical/Electro- mechanical methods | Automatic, step, or inverse activation | Single switch, array of switches | Requires minimal motor control [4] | Generally slow |
| Typing/icon selection | Mechanical keyboards | Instant feedback to user whenever a key is pressed [4,19] | Voluntary muscle control is a requirement for activation [4,19] | |
| Touch-activated methods | Force production through:
|
| Minimal activation pressure |
|
| Breath-activated methods | Fine breath tuning [58] |
| Integration with a predictive language model |
|
| Sniff control [59] | Control sensors for the acquisition of nasal pressure. | Confirmed usability with patients in LIS | Slowness: rate of three characters per minute. | |
| Discrete breath encoding [61,108] |
| Wearable configuration |
| |
| Analogue breath encoding [57] |
| Continuous/analogue breath encoding |
| |
| BCI methods | Invasive | Implantable electrodes | Communication and control of environment without the need for body movements [64] | |
| Non-invasive | External monitoring: EEG, MEG, fMRI, NIRS. [63] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elsahar, Y.; Hu, S.; Bouazza-Marouf, K.; Kerr, D.; Mansor, A. Augmentative and Alternative Communication (AAC) Advances: A Review of Configurations for Individuals with a Speech Disability. Sensors 2019, 19, 1911. https://doi.org/10.3390/s19081911
Elsahar Y, Hu S, Bouazza-Marouf K, Kerr D, Mansor A. Augmentative and Alternative Communication (AAC) Advances: A Review of Configurations for Individuals with a Speech Disability. Sensors. 2019; 19(8):1911. https://doi.org/10.3390/s19081911
Chicago/Turabian StyleElsahar, Yasmin, Sijung Hu, Kaddour Bouazza-Marouf, David Kerr, and Annysa Mansor. 2019. "Augmentative and Alternative Communication (AAC) Advances: A Review of Configurations for Individuals with a Speech Disability" Sensors 19, no. 8: 1911. https://doi.org/10.3390/s19081911