1. Introduction
The number of people over 60 years of age is rapidly increasing worldwide. The main reasons for this demographic change are the increase in life expectancy and the fall in the birth rate [
1]. This has become a public health problem, since aging is generally associated with a decrease in physical and psychological capacity, as well as an increase in the risk of disability, dependence and a number of comorbidities [
1,
2].
One of the consequences generated by aging is the increased risk of falls, which have been defined as accidental events in which the person falls after losing control of the center of gravity and no effort is made to restore the balance, or it is inefficient [
3].
Falls represent a major public health problem in the elderly population. Approximately one third of the population over 65 years old has experienced at least one fall per year. In addition, this frequency increases by 50% in individuals older than 85 years. Between 20% and 30% of falls result in an injury that requires medical attention, constituting the leading cause of death or non-fatal injury in older adults [
4,
5,
6]. Therefore, the early detection of the decreased function of the elderly is important to initiate precociously the preventive measures that allow for maintaining their functional independence [
7].
Normally, rehabilitation professionals perform evaluations through observation, as well as through the application of scales or assessment instruments, which provide a certain level of objectivity to the evaluations. There is a large number of tests and scales that allow for evaluating and assessing the static balance, dynamic balance and gait of healthy subjects or with motor problems [
8], the Timed Up & Go test (TU & Go) being the most used worldwide. This test measures the dynamic balance and functional mobility in older adults, as well as in the neurological population [
9,
10,
11].
The TU & Go is a simple test that can be performed anywhere, and consists of the subject getting up from a chair from the sitting to the bipedal position, walking three meters, turn, returning and sitting on the chair again, as illustrated in
Figure 1. The variable measured is the total time taken by the test and then the score assigned in seconds is observed, which is correlated with the risk of falls [
9,
12].
Some of the advantages of the TU & Go test is the simplicity in its application and its short duration. In addition, it requires little equipment and allows the possibility that people with a functional impairment can perform the test. However, one of the limitations is that the TU & Go, although it provides relevant information about the risk of falls, is not capable of determining subjects with greater difficulties objectively. Barry et al. [
13] mentioned that a limitation in the predictive value of the test could be explained by the fact that it is a unique test that evaluates the overall balance and mobility, which can be improved by combining it with technological tools for the movement analysis, such as optoelectronic laboratories with passive reflective markers, considered the gold standard instrument for analysis of human movement, or several alternatives, like wireless motion sensors such as inertial sensors or inertial measurement units (IMU).
Optoelectronic laboratories, despite providing accurate measurements, are expensive and their application takes a long time, since training and experience is required to interpret the results. In addition, in several countries, there are rural or remote locations with no resources for these advanced technological evaluations systems.
In recent years, a variety of evidence has been observed regarding the development of different devices that use inertial sensors, applications and/or smartphones as a low-cost alternative to optoelectronic systems, which have allowed for specifically visualizing the phases in which subjects could present greater problems with the consequent probability to fall during the application of the TU & Go test [
14,
15]. Different authors [
7,
8,
11] indicate that the phases of the TU & Go test correspond to: the transition from sitting position to standing, walking towards the turning mark, turning, walking back to the chair, turning and the sit back. This has been shown to increase the predictive value of the test in relation to the risk of falls and the phases in which subjects present greater difficulties.
Thus, it has been demonstrated that it is possible to implement an automatic segmentation of these phases or activities through feature-based algorithms [
11,
16], complex algorithms based on machine learning [
7,
17] or by principal components analysis (PCA) [
18]—as techniques based in Wavelet decomposition [
19]—using inertial sensors. Feature-based algorithms have the advantage of being simple to implement, but their performance is diminished due to the great variability that exists in the morphology of the signals they use to perform the segmentation—angular velocity and acceleration—those that depend on the environment and the execution time of the activities to be identified. Algorithms based on machine learning have a good response to the great variability of the characteristics present in the signals to be processed, but they are complex in their implementation—like those that use principal components analysis—and, to guarantee the above, they depend on a large amount of data where the mentioned variabilities are presented.
One way to reduce the disadvantages of feature-based methods is using the orientation data from Inertial Measurement Units (IMU) [
14,
20]. This orientation angles have been used in different parts of the body for the segmentation of activities during the execution of the test, since they have low variability in their inter-subject characteristics, allowing for extracting characteristics of each phase independently [
21,
22].
In relation to the above, this study presents an automatic segmentation methodology that uses a feature-based algorithm to identify the typical sub-tasks carried out during a three-meter TU & Go test in two groups of subjects (young and older adults) using the orientation angles of a single wireless IMU on the back (L3–L4, approximately) to analyze independently the data of the inertial sensors, in order to provide a complete report on the risk of falls and promote the use of low–cost technological objective elements and simple use in hospitals or rehabilitation centers of rural or remote locations.
2. Material and Methods
2.1. Design and Setting
A study with a descriptive design is presented, in which experimental tests were performed to analyze the segmentation of the TU & Go test stages, contrasted with the measurements obtained using a wireless IMU on the lower–back. A total of 25 healthy young subjects (18 men and 7 women) between 25 and 33 years old, and 12 elderly subjects (7 men and 5 women) between 59 and 93 years old were recruited in the city of Concepcion, Chile.
Exclusion criteria were the diagnosis of a neurological, vestibular, musculoskeletal or systemic disease that could alter the ability to walk; the diagnosis of any cardiovascular, respiratory or metabolic disease or other conditions that could interfere with the present study; having undergone surgery on the trunk and lower limbs at least two years prior to the present study, the use of assistive devices for walking and the presence of serious visual alterations that could alter the gait pattern.
The measurements were carried out at the Biomedical Engineering laboratory and in the facilities of the Kinesiology department of the Universidad de Concepción. Prior to the measurements, the test was explained to the participants and two trials without data collection were performed to check the understanding of each participant. The authorization was requested through informed consent, which was approved by the Biosecurity, Bioethical and Ethical Committee of the University of Concepción (Number 3180551).
2.2. IMU Sensor
A homemade IMU—developed at the laboratory of Biomedical Engineering of the Universidad de Concepción—was used.
The chip sensor utilized [
23] has a three-axis accelerometer, a three-axis gyroscope and a three-axis magnetometer (see
Table 1), as well as an embedded internal processor able to fuse the magnetic and the inertial data using an extended Kalman filter to accurately deliver the orientation in quaternions, to avoid singularities presents in the Euler and Navigation representations. Then, the orientation data is obtained in angle representation with an accuracy of ±1 deg. The data is sampled at 100 Hz with a low cost 32–bit microcontroller with an Advance RISC (reduce instruction set computer) Machine (ARM) Cortex-M0+ processor and sent to a software application via Bluetooth 3.0 up to a maximum distance of 20 m without risk of occlusion. The entire system is powered by a 500-mAh LiPo battery, which gives 10-h of autonomy.
Figure 2 shows the implemented sensor and its disposition on the subjects.
2.3. Test Procedure
The developed sensor is positioned on the back at the height of L3–L4 for young and elderly subjects. It has been shown that the use of a single IMU in that position allows for the detection of all gait events, biomechanical elements of the pelvis and other spatial and temporal kinematics factor [
24,
25,
26].
The TU & Go test was performed following the recommendations of [
22]. Three meters away from the chair, a cone was used to mark the location where the patients had to make the turn. Before carrying out the tests, the procedure was explained with a demonstration, to resolve and clarify doubts. Each participant was recorded at 60 fps using a GOPRO HERO 7 high resolution digital video camera (GoPro, Inc., San Mateo, CA, USA) using lineal FOV (Field of View) mode to reduce the image distortion.
Three TU & Go test repetitions were performed by the older adults group, using for the analysis the performance of the higher time of the test carried out. For the young group, only one test was carried out.
Figure 3 shows the set up used for the measurements.
2.4. Segmentation Algorithm
For the segmentation of standing, walking, turning and sitting activities, an algorithm was designed. This algorithm processed inclination () and rotation () signals of an inertial sensor placed on the back of a subject at L3–L4, approximately.
2.4.1. Standing/Sitting Events Identification
To determine the events of standing and sitting, the
signal was used. This corresponds to the inclination actions during the activities to be identified. When a subject is standing or sitting, he tends to make a slight forward inclination with respect to the resting position until it regains its initial inclination (see
Figure 4), which can even be observed in subjects with reduced mobility [
27].
In order to condition the
signal, this is smoothed by an average filter of order
N = 5 (see Equation (
1)) and normalized by the absolute maximum of the smooth signal, as seen in Equation (
2):
Then, the Pitch signal is processed using a local maximum detector, finding
and
, that corresponds to the maximum angle of inclination in the standing and sitting events, respectively (see
Figure 5).
Then, the difference between samples to the left of
is calculated, as indicated in Equation (
3), and to the right of
, as indicated in Equation (
4), to start the search for the standing action, were
i is a sample iterator. Thus, the start and end of standing action are obtained using Equations (
5) and (
6), respectively, with a factor of 0.05 to determine the threshold slope stop, which was found experimentally:
Similarly, through the same methodology, the sitting action is sought using the difference between samples to the left of
, as indicated in Equation (
7), and to the right of
, as indicated in Equation (
8). Then, the start and end of standing action are obtained using the Equations (
9) and (
10), respectively:
Figure 6 shows the final result of the search method and
Figure 7 shows the proposed standing/sitting activities identification method.
2.4.2. Turning Events Identification
To determine the turns around the 3-m mark and prior to sitting,
is used, which corresponds to changes in the orientation of the sensor during turns. When a subject performs the TU & Go test, it is subjected to a circuit that forces it to make turns of 180 degrees approximately, which can be unequivocally measured by the sensor in the back, since, during turns, the sensor also changes its orientation next to it (see
Figure 8).
To condition the orientation change signal, as for the inclination signal, this is smoothed by an average filter of order
N = 5 (see Equation (
11)) and normalized by the absolute maximum of the signal, as seen in Equation (
12):
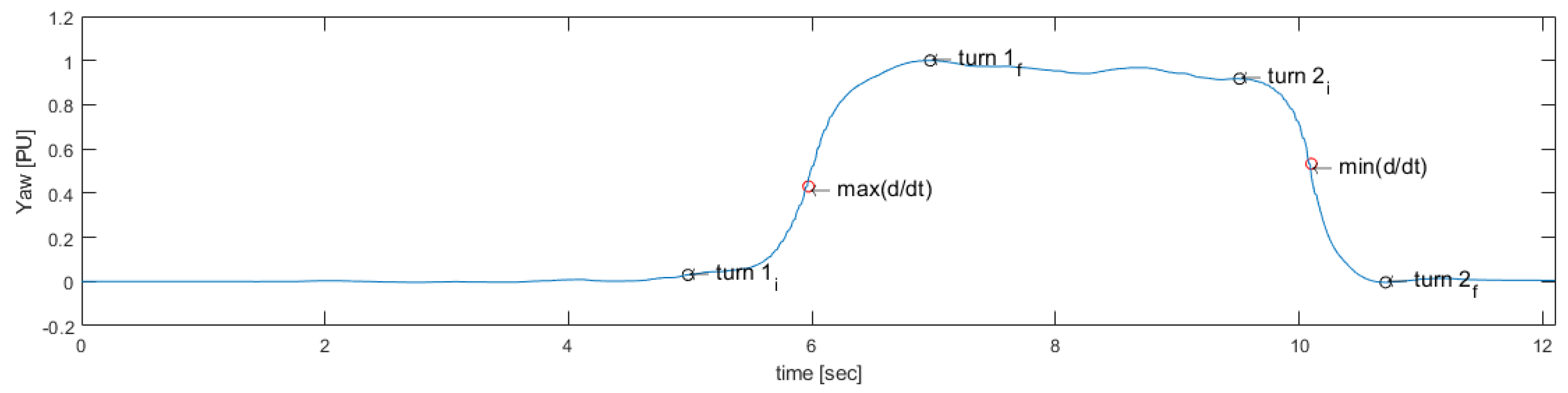
Then, the rotation signal is derived and processed to identify the maximum value
and the minimum value
, which are useful to identify the start and end points of the first turn and the second turn, respectively, as seen in
Figure 9.
Thus, through a sliding window of 0.1 s or 10 samples (Equations (
13) and (
14)), the start of the 3-m tuning is searched by calculating the mean of the samples in the window to the left of
and the end of the 3-m tuning calculating the mean of the samples in the window to the right of
using Equations (
15) and (
16), respectively:
Finally, the start and the end of the 3-m turning are obtained through Equations (
17) and (
18), respectively:
Then, using a sliding window of 0.1 s or 10 samples (Equations (
19) and (
20)), the start of the pre-sitting tuning is sought by calculating the mean of the samples in the window to the left of
and the end of the pre-sitting tuning calculating the mean of the samples in the window to the right of
using Equations (
21) and (
22), respectively:
Similarly, the start and the end of the pre-sitting turning are obtained through Equations (
23) and (
24), respectively:
Figure 10 shows the final result of the search method and
Figure 11 indicates the proposed turning activities’ identification method.
4. Discussion
In this study, a segmentation of the TU & Go test activities using a single wireless IMU was performed in two different age groups. For this, a comparison between the measurements obtained by the typical observational analysis and the proposed methodology, the segmentation of the TU & Go test activities and the characterization of the inertial signals acquired from the TU & Go test stages were carried out with interesting results.
Effective treatment, specifically for gait disturbances and for risk of falls assessment, requires reliable tools. Tridimensional motion capturing systems are the gold standard of gait assessment, but, due to the space and time requirements and the high cost of the equipment, its use in clinical practice is far from routine [
29]. In addition, a limited number of consecutive strides can be measured and they require camera and markers that may limit their use in the clinical practice.
In this context, IMUs may be used to assess gait performance and risk of falls. Moreover, these technologies present several advantages such as they are portable, low-cost and lightweight; they are good at measuring acceleration and turns, they are suitable for measuring brief, high speed events and they can be used indoors and outdoors regardless of lighting conditions; finally, they can continuously evaluate over long periods of time. However, they must answer to their usefulness as a clinical tool [
30]. Thus, these technological devices must be assessed in terms of clinical feasibility and psychometric properties [
31,
32].
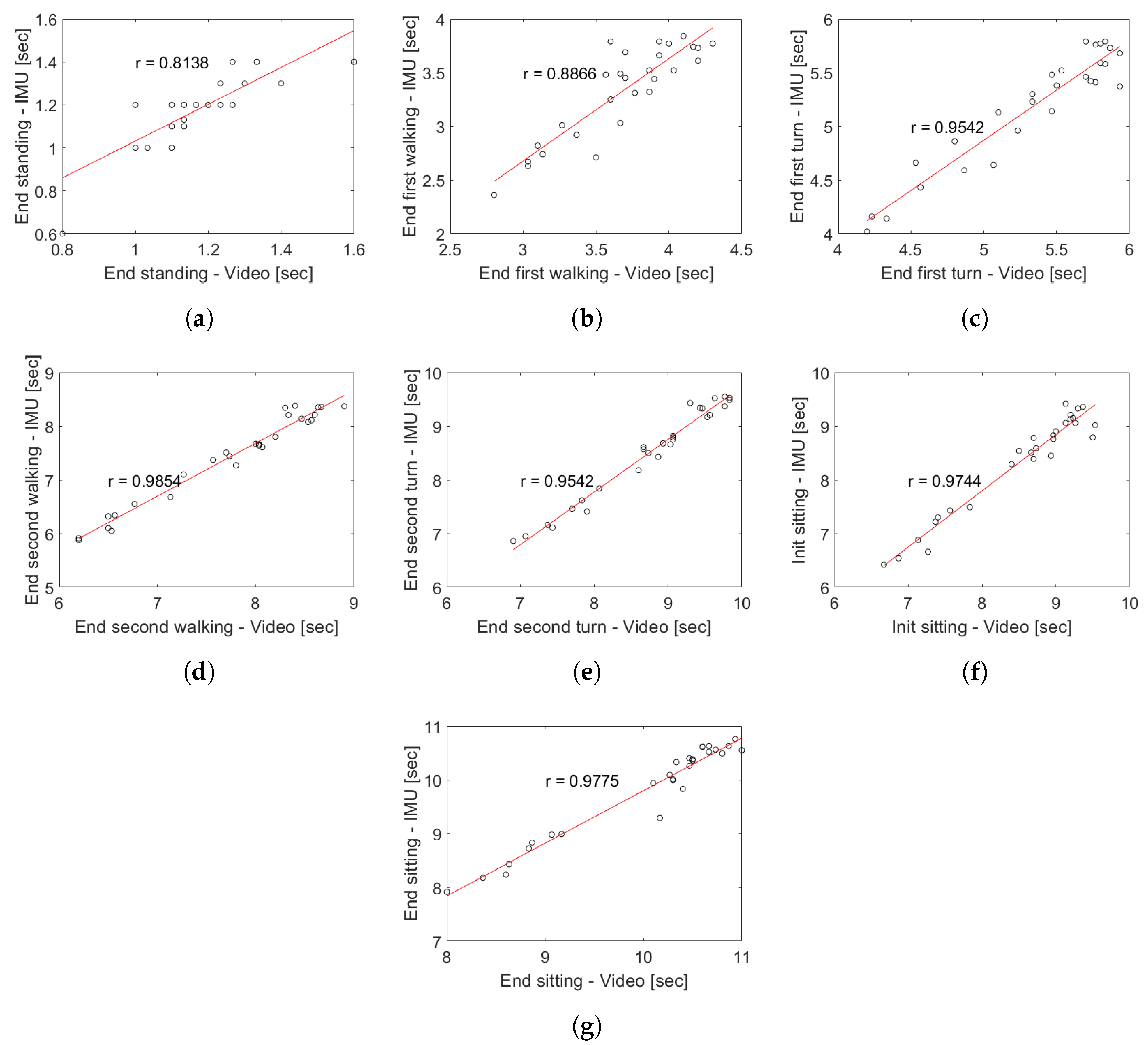
The proposal model obtained a high correlation respect to video recording (see
Figure 12), allowing for identifying all the events with only a single wireless IMU which present a low variability in characteristics inter-subjects. It allows for extracting characteristics of each phases independently, in comparison with other works that use a body fixed sensor array [
11,
16]. In general, during the proof of concept of the proposed methodology in young subjects, a high degree of concordance was obtained with respect to the segmentation performed by video, which is demonstrated in the correlation coefficients of
Figure 14. In the case of the group of older adults, the correlation analysis was omitted because the results could be unrepresentative due to the low number of subjects and the atypical data present in the subject with a high risk of falls (see subject 12 of
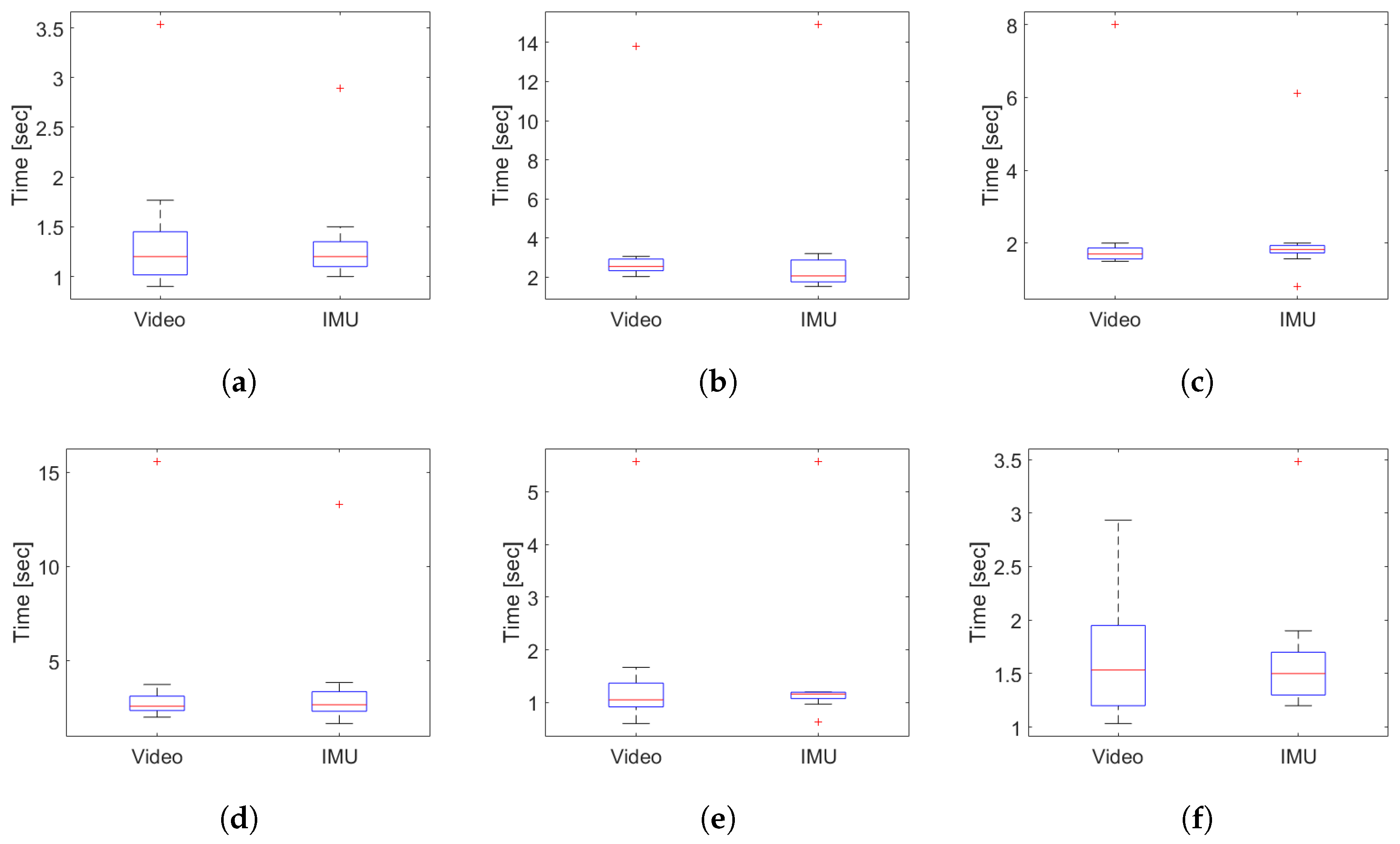
Table 3). The worst correlation obtained was found in the identification of the moment in which the person finishes the sit-to-stand transition, due to the difficulty to identify in a visual way the exact point of the end of the standing and the beginning of the first walk sub-task. However, the proposed analysis algorithm was capable of identifying the exact transition point with an average maximum error of 0.36 s (see
Figure 15b) for young subjects and a maximum average error of 0.63 s for older adults (see
Figure 16d).
The segmentation presented in the present study allows for improving objectivity to the clinical practice in the evaluation of the performance of the patients. By observing the standing/sitting phases using
, it is possible to determine the inclination of the trunk during sit to walk transfer in young subjects (see
Table 5) and older adults subjects (see
Table 7. This is relevant because, as mentioned by Pozaic et al., the transition from sit to walk is the event with the highest number of falls in the elderly population [
33].
On the other hand, the analysis of the turning phases through
will allow for observing the degrees and the time that the subject takes to carry out this activity (
Figure 18c,e). The ability to turn safely is relevant to functional independence and is considered another difficult task with a high risk of falling [
34,
35].
Although the conventional TU & Go test is a clinical tool that allows for measuring the risk of falling, it uses a single global parameter to estimate it. However, the stage that could be interfering in the execution of the task in less time is not specifically discriminate. The current methodology provides information about variables such as: standing acceleration (Acc. Su), sitting acceleration (Acc. Sd), rotation velocity of the 3-m turning (Vel.
), rotation velocity of the pre-sitting turning (Vel.
), number of steps during the first walk (Steps
), number of steps during the second walk (Steps
), number of steps during the 3-m turning (Steps
), number of steps during the pre-sitting turning (Steps
), inclination degrees of the trunk during standing (
Su) and sitting (
Sd) (see
Table 5).
Other authors [
36,
37,
38,
39] have explored the use of IMU technology for gait assessment during the TU & Go test. However, this approach allows for segmenting the transitions between each sub-task in an exact and automatic way, using a simple algorithm and a low–cost movement sensor, allowing for extracting characteristics of each one of them due to the positioning of the IMU in the young and older adults groups. The above can be extrapolated when performing tests of 6 and 10 m to extract more parameters of the gait during the first and second walk.
This study presents some limitations. Firstly, the segmentation of each event during the analysis of the videos was performed in an observational way. Second, it is not possible to determine how the algorithm would perform in other populations such as people with neurological disorders. However, the whole sample recruited was determined as the starting point to be capable of validating the algorithm and the sensors used in pathological population in future research. Clinical validation studies of these devices should be carried out in populations with specific characteristics related to gait and balance impairments.

 ,
, 




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}