Development and Validation of Ambulosono: A Wearable Sensor for Bio-Feedback Rehabilitation Training

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Data Collection
2.2. Data Analysis
2.3. Statistical Analysis
3. Results
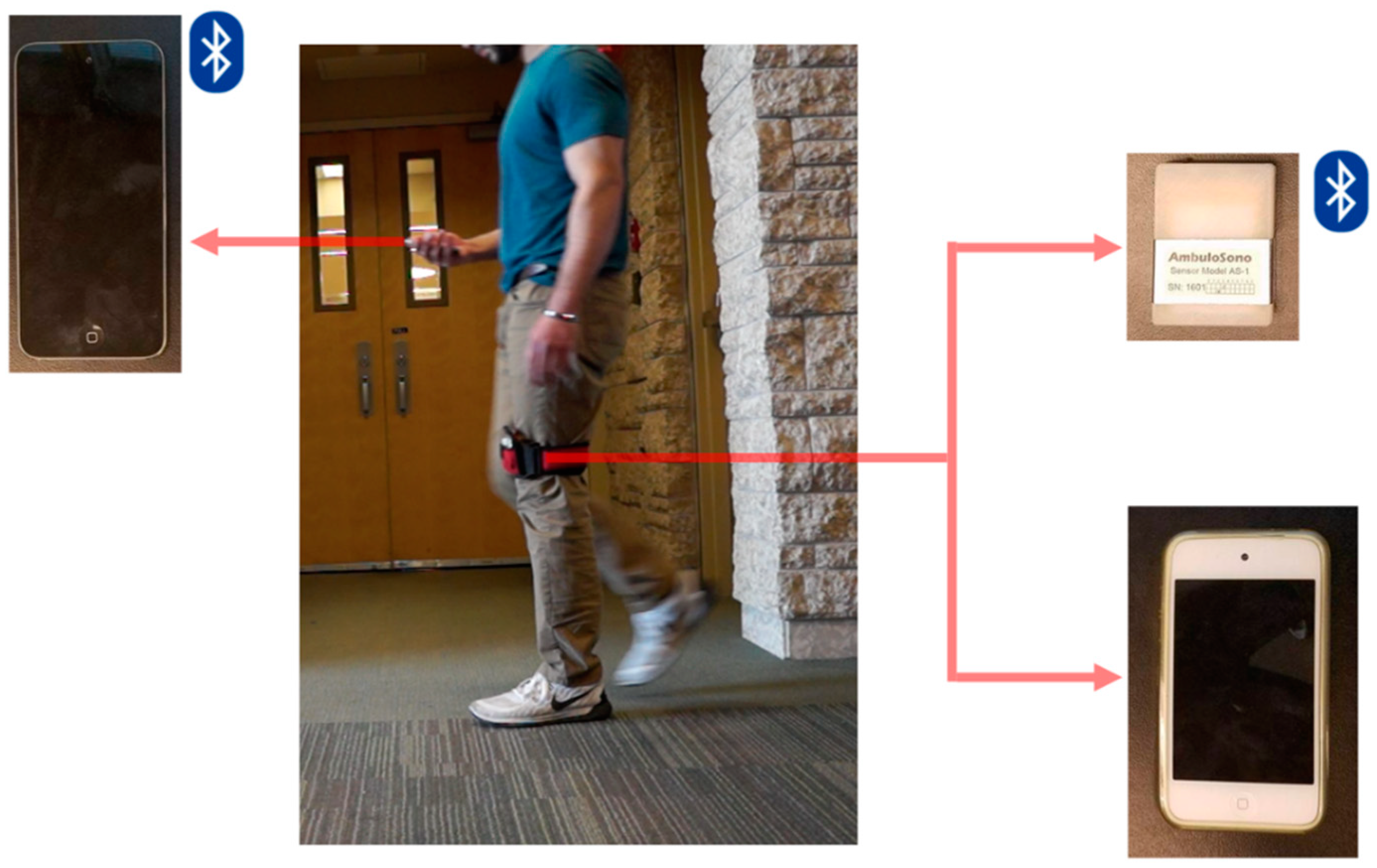
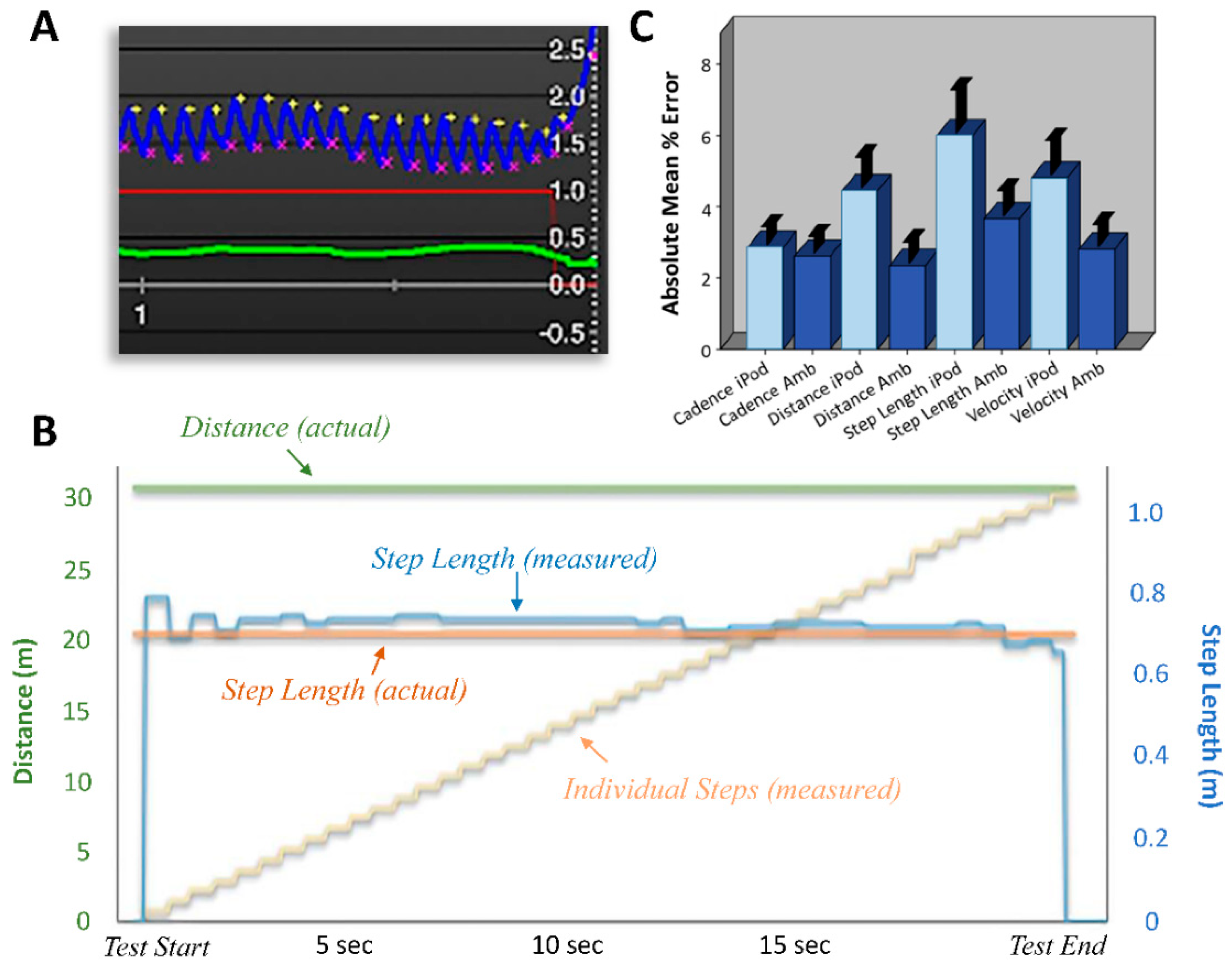
3.1. Sensors and Gait Measurements
3.2. Ambulosono Sensor Testing and Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kluge, F.; Gaßner, H.; Hannink, J.; Pasluosta, C.; Klucken, J.; Eskofier, B.M. Towards Mobile Gait Analysis: Concurrent Validity and Test-Retest Reliability of an Inertial Measurement System for the Assessment of Spatio-Temporal Gait Parameters. Sensors 2017, 17, 1522. [Google Scholar] [CrossRef] [PubMed]
- Merola, A.; Sturchio, A.; Hacker, S.; Serna, S.; Vizcarra, J.A.; Marsili, L.; Fasano, A.; Espay, A.J. Technology-based assessment of motor and nonmotor phenomena in Parkinson disease. Expert Rev. Neurother. 2018, 18, 825–845. [Google Scholar] [CrossRef] [PubMed]
- Porciuncula, F.; Roto, A.V.; Kumar, D.; Davis, I.; Roy, S.; Walsh, C.J.; Awad, L.N. Wearable Movement Sensors for Rehabilitation: A Focused Review of Technological and Clinical Advances. PM&R 2018, 10, S220–S232. [Google Scholar]
- Chomiak, T.; Watts, A.; Meyer, N.; Pereira, F.V.; Hu, B. A training approach to improve stepping automaticity while dual-tasking in Parkinson’s disease. Medicine 2017, 96, e5934–e5939. [Google Scholar] [CrossRef] [PubMed]
- Majumder, S.; Mondal, T.; Deen, M. Wearable Sensors for Remote Health Monitoring. Sensors 2017, 17, 130. [Google Scholar] [CrossRef] [PubMed]
- McGregor, S.; Churchward, P.; Soja, K.; O’Driscoll, D.; Braybrook, M.; Khodakarami, H.; Evans, A.; Farzanehfar, P.; Hamilton, G.; Horne, M. The use of accelerometry as a tool to measure disturbed nocturnal sleep in Parkinson’s disease. Nat. NPJ Park. Dis. 2018, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Chomiak, T.; Pereira, F.V.; Meyer, N.; de Bruin, N.; Derwent, L.; Luan, K.; Cihal, A.; Brown, L.A.; Hu, B. A new quantitative method for evaluating freezing of gait and dual-attention task deficits in Parkinson’s disease. J. Neural Transm. 2015, 122, 1523–1531. [Google Scholar] [CrossRef]
- Hansen, T.I.; Lehn, H.; Evensmoen, H.R.; Håberg, A.K. Initial assessment of reliability of a self-administered web-based neuropsychological test battery. Comput. Hum. Behav. 2016, 63, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Schaafsma, J.D.; Balash, Y.; Gurevich, T.; Bartels, A.L.; Hausdorff, J.M.; Giladi, N. Characterization of freezing of gait subtypes and the response of each to levodopa in Parkinson’s disease. Eur. J. Neurol. 2003, 10, 391–398. [Google Scholar] [CrossRef]
- Lewis, G.N.; Byblow, W.D.; Walt, S.E. Stride length regulation in Parkinson’s disease: The use of extrinsic, visual cues. Brain 2000, 123, 2077–2090. [Google Scholar] [CrossRef]
- Iansek, R.; Huxham, F.; McGinley, J. The sequence effect and gait festination in Parkinson disease: Contributors to freezing of gait? Mov. Disord. 2006, 21, 1419–1424. [Google Scholar] [CrossRef] [PubMed]
- Chien, S.L.; Lin, S.Z.; Liang, C.C.; Soong, Y.S.; Lin, S.H.; Hsin, Y.L.; Lee, C.W.; Chen, S.Y. The efficacy of quantitative gait analysis by the GAITRite system in evaluation of parkinsonian bradykinesia. Park. Relat. Disord. 2006, 12, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-K.; Kim, S.-G.; Shin, Y.-J.; Choi, E.-H.; Choe, Y.-W. The relationship between anterior pelvic tilt and gait, balance in patient with chronic stroke. J. Phys. Ther. Sci. 2017, 30, 27–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peixoto, J.G.; de Souza Moreira, B.; Diz, J.B.M.; Timoteo, E.F.; Kirkwood, R.N.; Teixeira-Salmela, L.F. Analysis of symmetry between lower limbs during gait of older women with bilateral knee osteoarthritis. Aging Clin. Exp. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Roche, B.; Simon, A.-L.; Guilmin-Crépon, S.; Boizeau, P.; Andriss, B.; Alberti, C.; Presedo, A.; Ilharreborde, B.; Husson, I. Test-retest reliability of an instrumented electronic walkway system (GAITRite) for the measurement of spatio-temporal gait parameters in young patients with Friedreich’s ataxia. Gait Posture 2018, 66, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Beerse, M.; Lelko, M.; Wu, J. Biomechanical analysis of the timed up-and-go (TUG) test in children with and without Down syndrome. Gait Posture 2019, 68, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Wrisley, D.M.; Marchetti, G.F.; Kuharsky, D.K.; Whitney, S.L. Reliability, internal consistency, and validity of data obtained with the functional gait assessment. Phys. Ther. 2004, 84, 906–918. [Google Scholar]
- Herman, T.; Weiss, A.; Brozgol, M.; Giladi, N.; Hausdorff, J.M. Gait and balance in Parkinson’s disease subtypes: Objective measures and classification considerations. J. Neurol. 2014, 261, 2401–2410. [Google Scholar] [CrossRef]
- Ivey, F.M.; Katzel, L.I.; Sorkin, J.D.; Macko, R.F.; Shulman, L.M. The Unified Parkinson’s Disease Rating Scale as a predictor of peak aerobic capacity and ambulatory function. J. Rehabil. Res. Dev. 2012, 49, 1269–1276. [Google Scholar] [CrossRef]
- Ossig, C.; Antonini, A.; Buhmann, C.; Classen, J.; Csoti, I.; Falkenburger, B.; Schwarz, M.; Winkler, J.; Storch, A. Wearable sensor-based objective assessment of motor symptoms in Parkinson’s disease. J. Neural Transm. 2016, 123, 57–64. [Google Scholar] [CrossRef]
- Chomiak, T.; Watts, A.; Burt, J.; Camicioli, R.; Tan, S.N.; McKeown, M.J.; Hu, B. Differentiating Cognitive or Motor Dimensions Associated with the Perception of Fall-Related Self-Efficacy in Parkinson’s Disease. Nat. NPJ Park. Dis. 2018, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Odin, P.; Chaudhuri, K.R.; Volkmann, J.; Antonini, A.; Storch, A.; Dietrichs, E.; Pirtošek, Z.; Henriksen, T.; Horne, M.; Devos, D.; et al. Viewpoint and practical recommendations from a movement disorder specialist panel on objective measurement in the clinical management of Parkinson’s disease. Nat. NPJ Park. Dis. 2018, 4, 14. [Google Scholar] [CrossRef] [PubMed]
- Chomiak, T.; Pereira, F.V.; Luan, K.; Cihal, A.; Meyer, N.; Hu, B. Gait differences between initial symptom onset of tremor-dominant and non-tremor dominant sub-types in Parkinson’s disease (P1.051). Neurology 2016, 86. [Google Scholar]
- Hu, B. Sustained Relief of Multiple Types of Gait Freezing in Parkinson’s Disease: A Novel, Music-Based Meta-Conditioning Treatment Protocol (Ambulosono) (P4.328). Neurology 2016, 86. [Google Scholar]



{kind=link}
{kind=link}
| Step Length (m) | Trial 1 | Trial 2 |
|---|---|---|
| Known Standard | 0.71 | 0.71 |
| New Sensor | 0.72 | 0.72 |
| iPod | 0.67 | 0.67 |
| Distance (m) | ||
| Known Standard | 30.48 | 30.48 |
| New Sensor | 30.13 | 30.06 |
| iPod | 29.28 | 29.18 |
| Cadence (steps/min) | ||
| Known Standard | 106.76 | 106.09 |
| New Sensor | 107.16 | 108.26 |
| iPod | 106.05 | 108.33 |
| Velocity (m/s) | ||
| Known Standard | 1.24 | 1.26 |
| New Sensor | 1.27 | 1.28 |
| iPod | 1.2 | 1.21 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chomiak, T.; Sidhu, A.S.; Watts, A.; Su, L.; Graham, B.; Wu, J.; Classen, S.; Falter, B.; Hu, B. Development and Validation of Ambulosono: A Wearable Sensor for Bio-Feedback Rehabilitation Training. Sensors 2019, 19, 686. https://doi.org/10.3390/s19030686
Chomiak T, Sidhu AS, Watts A, Su L, Graham B, Wu J, Classen S, Falter B, Hu B. Development and Validation of Ambulosono: A Wearable Sensor for Bio-Feedback Rehabilitation Training. Sensors. 2019; 19(3):686. https://doi.org/10.3390/s19030686
Chicago/Turabian StyleChomiak, Taylor, Abhijot Singh Sidhu, Alexander Watts, Luke Su, Brian Graham, Joshua Wu, Suzanne Classen, Brian Falter, and Bin Hu. 2019. "Development and Validation of Ambulosono: A Wearable Sensor for Bio-Feedback Rehabilitation Training" Sensors 19, no. 3: 686. https://doi.org/10.3390/s19030686