A Computational Framework for Data Fusion in MEMS-Based Cardiac and Respiratory Gating

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
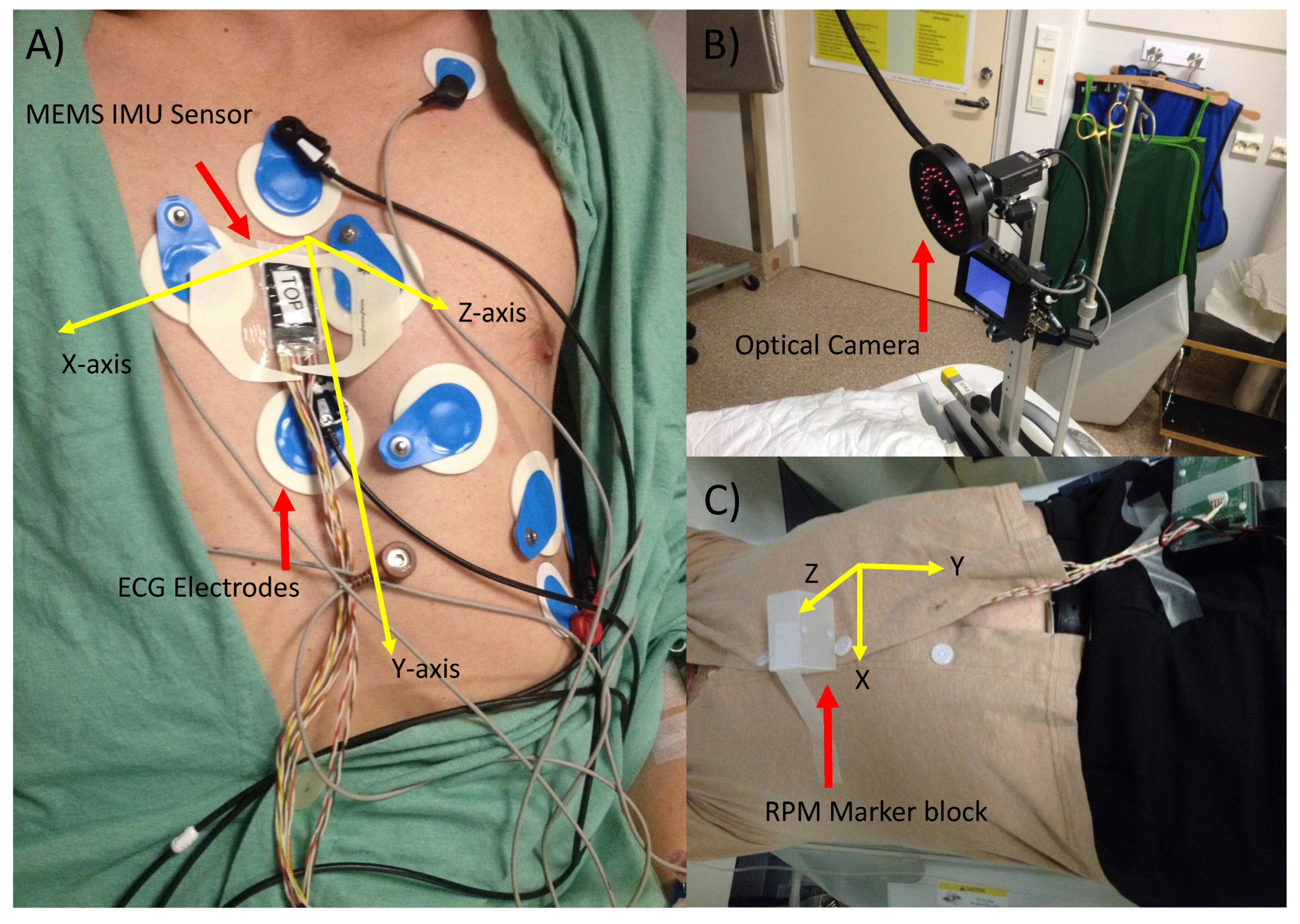
2.1. Data Acquisition and Experimental Protocol
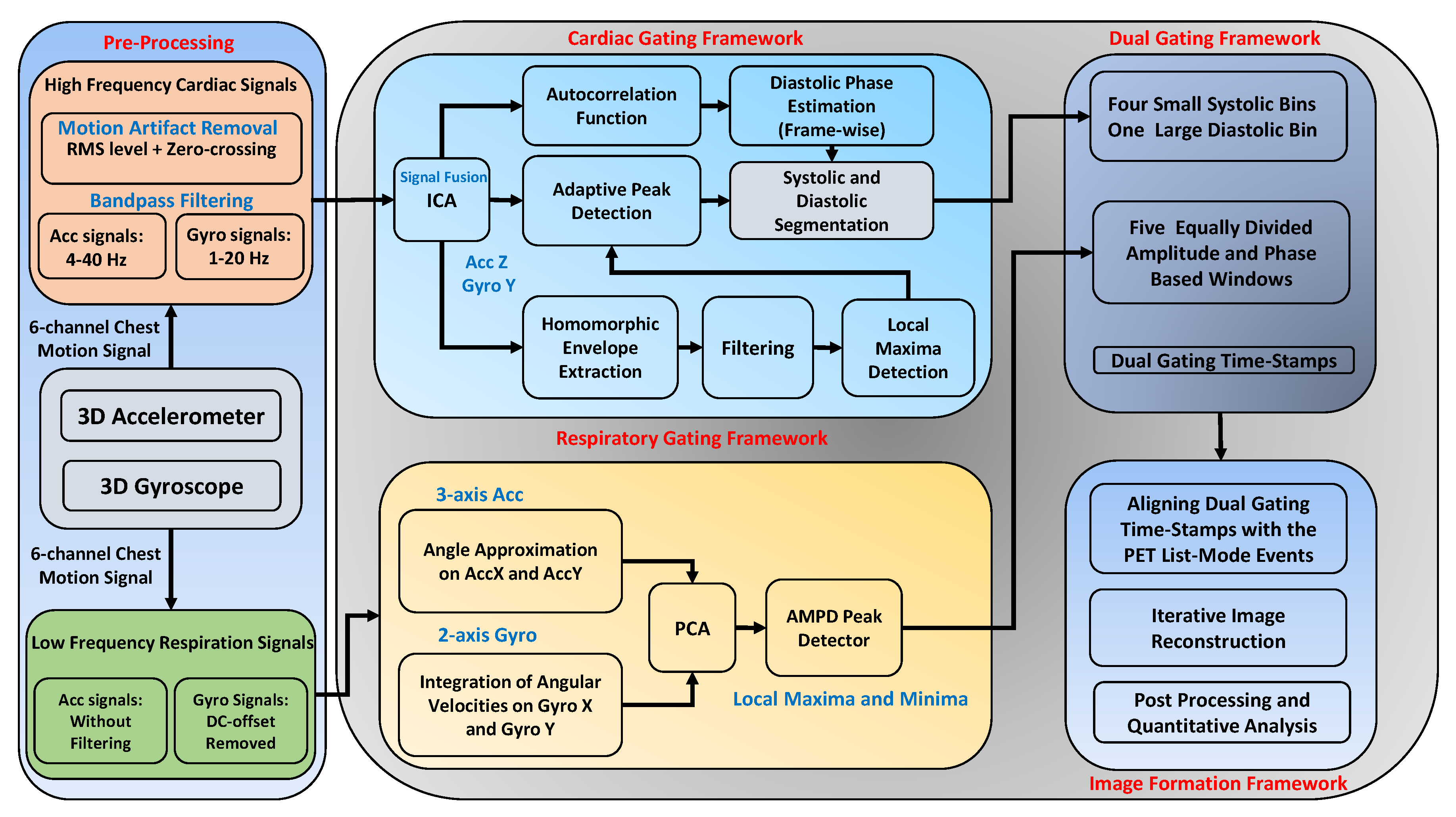
2.2. MEMS-Based Chest Motion Processing
2.2.1. Rotational and Translational Cardiac Motion Fusion
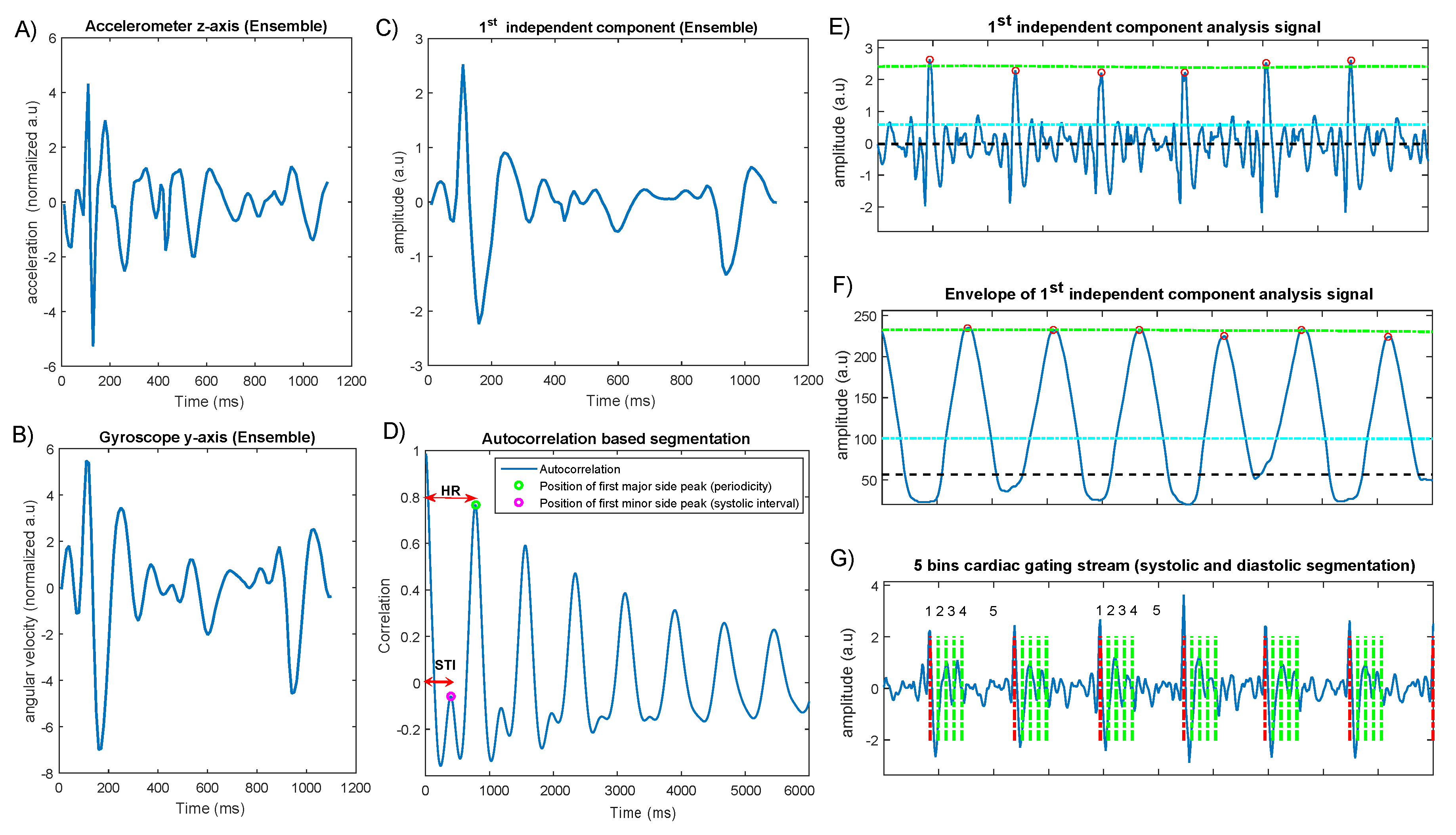
2.2.2. Standalone Cardiac Cycle Segmentation
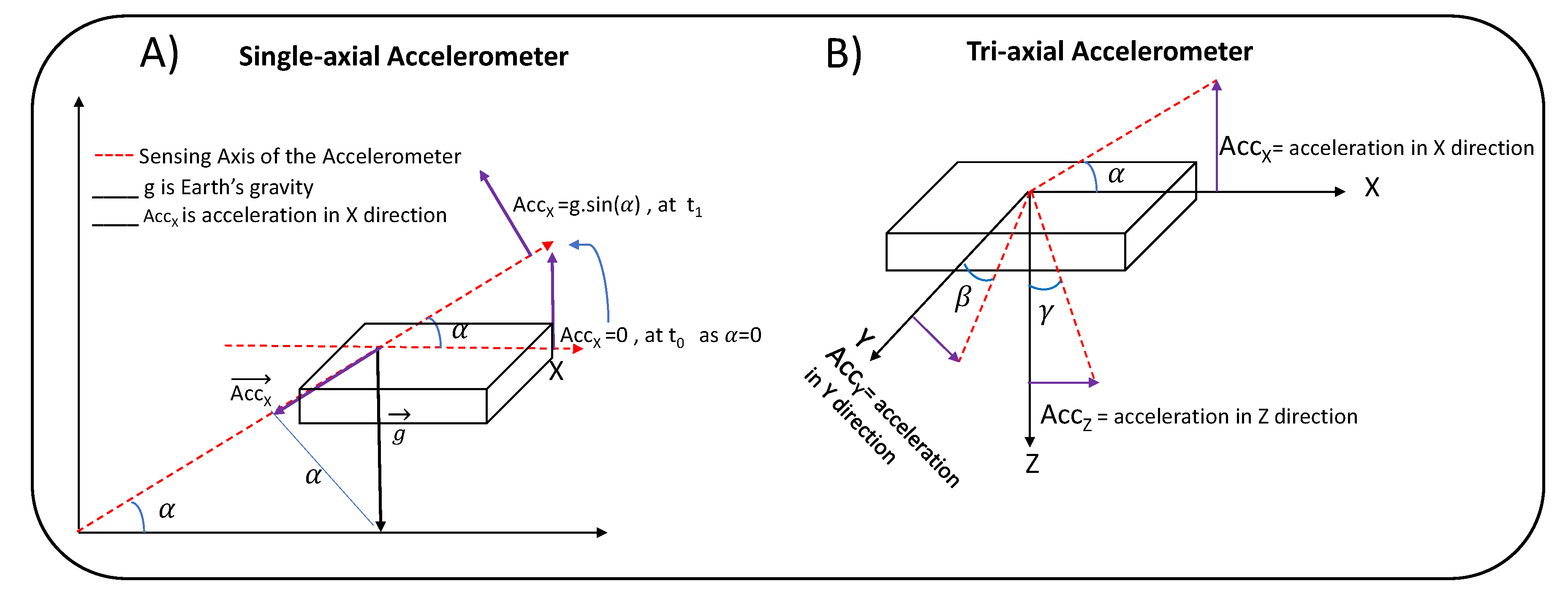
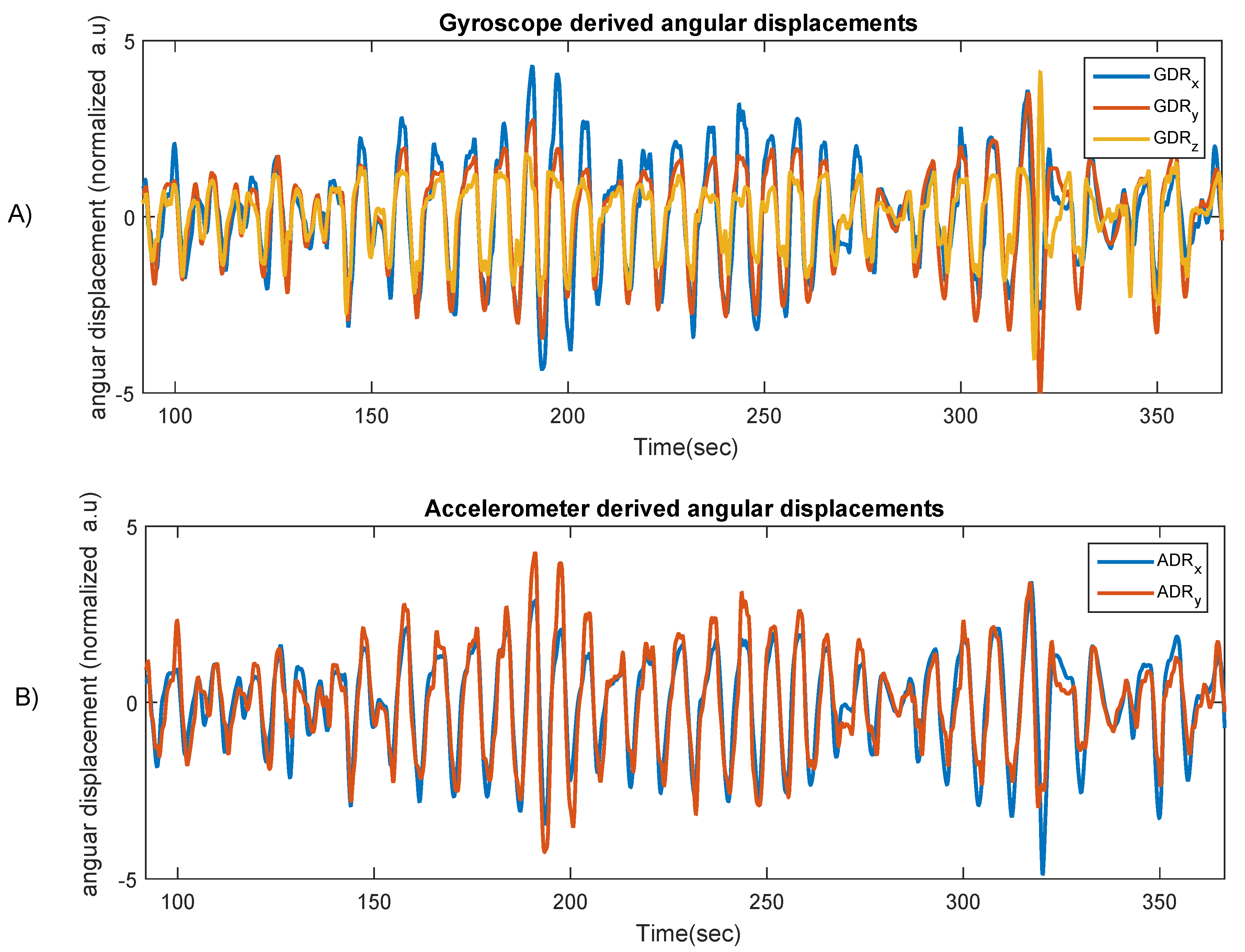
2.2.3. Decomposition of Chest Angular Movements
2.2.4. Chest-Derived Respiratory Motion Fusion
3. Results
3.1. Validation of Respiratory and Cardiac Data
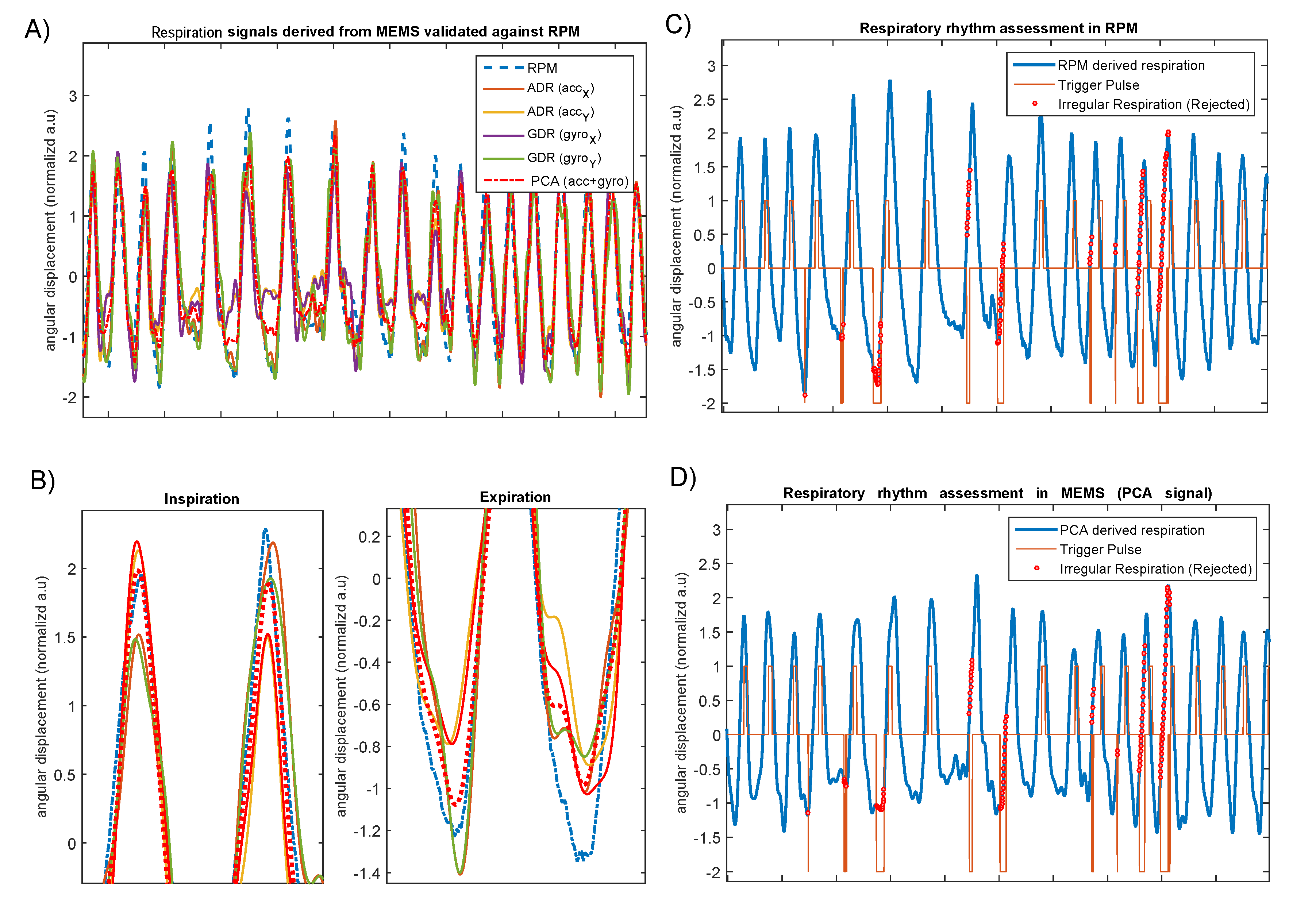
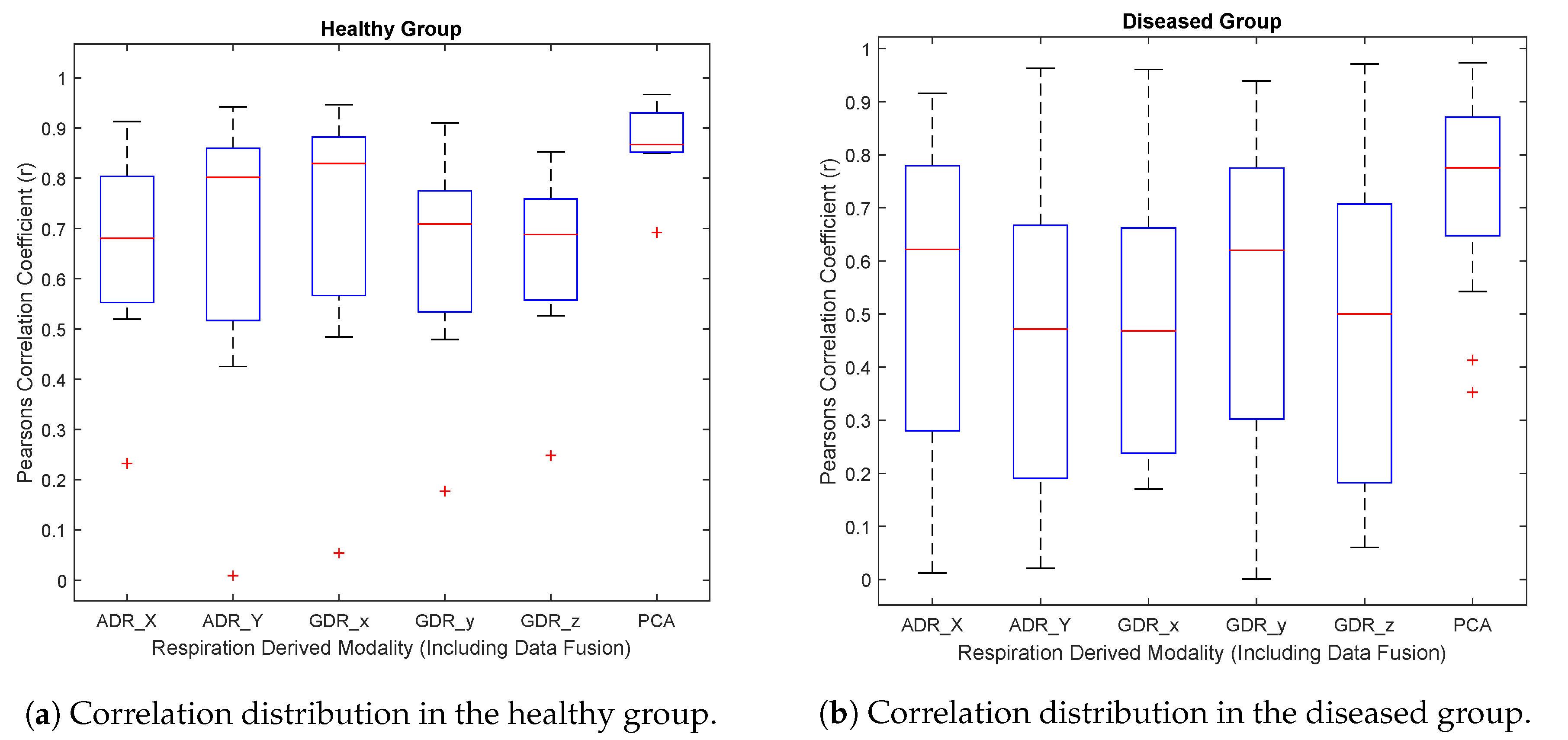
3.1.1. ADR and GDR against Optical Camera (RPM)
3.1.2. Beat-to-Beat Estimation of the Cardiac Cycles and Related Cardiac Events
3.1.3. Estimation of the Breathing Cycles (Peak Inhalation and Exhalation)
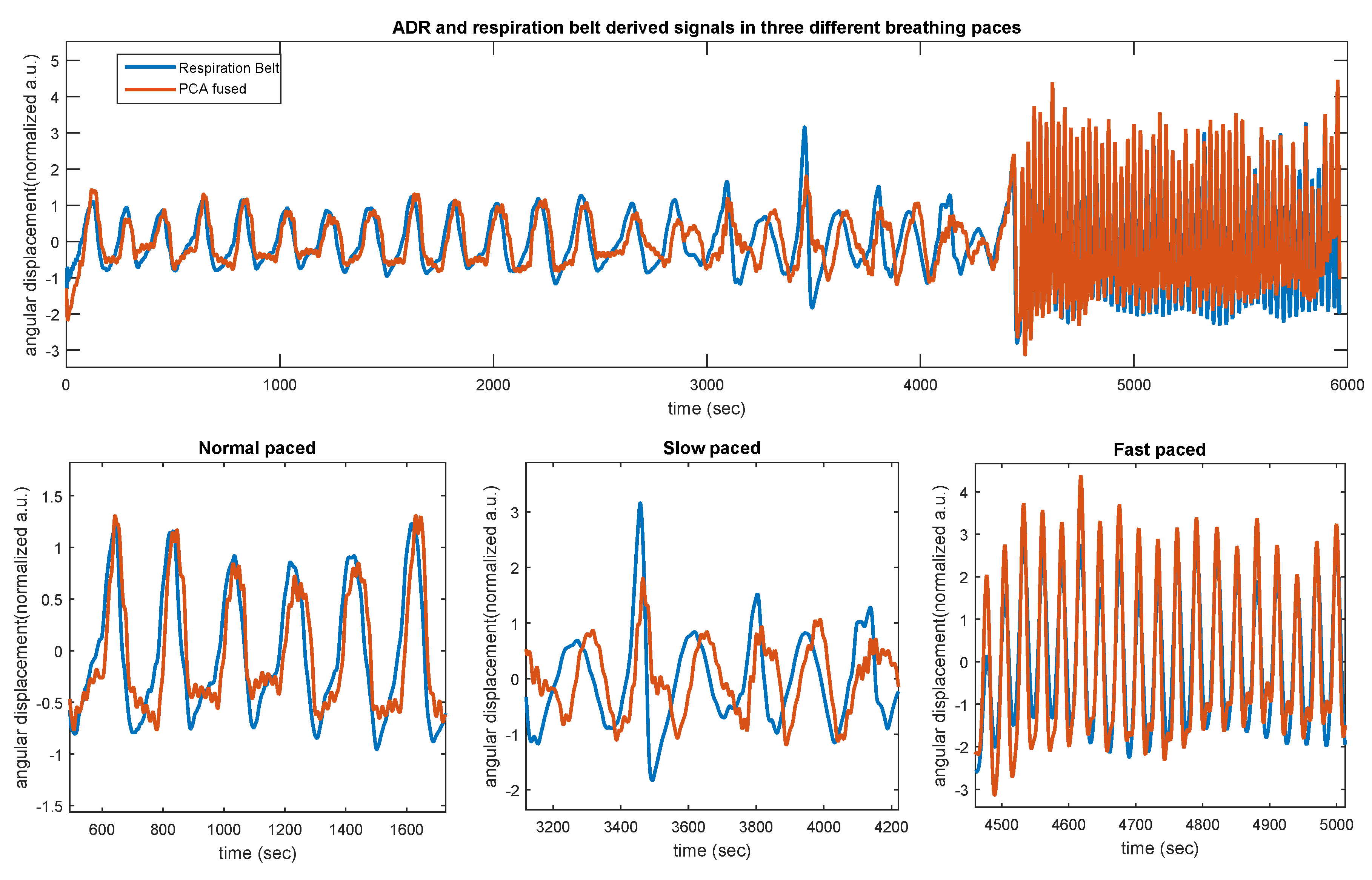
3.2. Respiration Belt
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schindler, T.H.; Schelbert, H.R.; Quercioli, A.; Dilsizian, V. Cardiac PET Imaging for the Detection and Monitoring of Coronary Artery Disease and Microvascular Health. JACC Cardiovasc. Imaging 2010, 3, 623–640. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Pierce, L.A., II; Alessio, M.A.; Kinahan, P.E. The impact of respiratory motion on tumor quantification and delineation in static PET/CT imaging. Phys. Med. Biol. 2009, 54, 7345. [Google Scholar] [CrossRef] [PubMed]
- Nehmeh, S.; Erdi, Y.; Ling, C.; Rosenzweig, K.; Squire, O.; Braban, L.; Ford, E.; Sidhu, K.; Mageras, G.; Larson, S.; et al. Effect of respiratory gating on reducing lung motion artifacts in PET imaging of lung cancer. Med. Phys. 2002, 29, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Teo, B.K.; Saboury, B.; Munbodh, R.; Scheuermann, J.; Torigian, D.A.; Zaidi, H.; Alavi, A. The effect of breathing irregularities on quantitative accuracy of respiratory gated PET/CT. Med. Phys. 2012, 39, 7390–7397. [Google Scholar] [CrossRef] [PubMed]
- Keall, P.J.; Mageras, G.S.; Balter, J.M.; Emery, R.S.; Forster, K.M.; Jiang, S.B.; Kapatoes, J.M.; Low, D.A.; Murphy, M.J.; Murray, B.R.; et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76 a. Med. Phys. 2006, 33, 3874–3900. [Google Scholar] [CrossRef] [PubMed]
- Nehmeh, S.A.; Erdi, Y.E.; Pan, T.; Yorke, E.; Mageras, G.S.; Rosenzweig, K.E.; Schoder, H.; Mostafavi, H.; Squire, O.; Pevsner, A.; et al. Quantitation of respiratory motion during 4D PET/CT acquisition. Med. Phys. 2004, 31, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Dawood, M.; Büther, F.; Lang, N.; Schober, O.; Schäfers, K.P. Respiratory gating in positron emission tomography: A quantitative comparison of different gating schemes. Med. Phys. 2007, 34, 3067–3076. [Google Scholar] [CrossRef]
- Büther, F.; Dawood, M.; Stegger, L.; Wübbeling, F.; Schäfers, M.; Schober, O.; Schäfers, K.P. List Mode–Driven Cardiac and Respiratory Gating in PET. J. Nucl. Med. 2009, 50, 674–681. [Google Scholar] [CrossRef]
- Slomka, P.J.; Pan, T.; Germano, G. Imaging moving heart structures with PET. J. Nucl. Cardiol. 2016, 23, 486–490. [Google Scholar] [CrossRef]
- Tadi, M.J.; Teuho, J.; Lehtonen, E.; Saraste, A.; Pänkäälä, M.; Koivisto, T.; Teräs, M. A novel dual gating approach using joint inertial sensors: Implications for cardiac PET imaging. Phys. Med. Biol. 2017, 62, 8080. [Google Scholar] [CrossRef]
- Wick, C.A.; Inan, O.T.; McClellan, J.H.; Tridandapani, S. Seismocardiography-Based Detection of Cardiac Quiescence. IEEE Trans. Biomed. Eng. 2015, 62, 2025–2032. [Google Scholar] [CrossRef]
- Wick, C.A.; Auffermann, W.F.; Shah, A.J.; Inan, O.T.; Bhatti, P.T.; Tridandapani, S. Echocardiography as an indication of continuous-time cardiac quiescence. Phys. Med. Biol. 2016, 61, 5297. [Google Scholar] [CrossRef]
- Yao, J.; Tridandapani, S.; Wick, C.A.; Bhatti, P.T. Seismocardiography-Based Cardiac Computed Tomography Gating Using Patient-Specific Template Identification and Detection. IEEE J. Transl. Eng. Health Med. 2017, 5, 1–14. [Google Scholar] [CrossRef]
- Yao, J.; Tridandapani, S.; Auffermann, W.; Wick, C.; Bhatti, P. An Adaptive Seismocardiography (SCG)-ECG Multimodal Framework for Cardiac Gating Using Artificial Neural Networks. IEEE J. Transl. Eng. Health Med. 2018, 6, 1–11. [Google Scholar] [CrossRef]
- Wartzek, T.; Brüser, C.; Walter, M.; Leonhardt, S. Robust sensor fusion of unobtrusively measured heart rate. IEEE J. Biomed. Health Inform. 2014, 18, 654–660. [Google Scholar] [CrossRef]
- Tadi, M.J.; Koivisto, T.; Pänkäälä, M.; Paasio, A. Accelerometer-based method for extracting respiratory and cardiac gating information for dual gating during nuclear medicine imaging. J. Biomed. Imaging 2014, 2014, 6. [Google Scholar]
- Yang, C.; Tavassolian, N. An independent component analysis approach to motion noise cancelation of cardio-mechanical signals. IEEE Trans. Biomed. Eng. 2018, 66, 784–793. [Google Scholar] [CrossRef]
- Hyvärinen, A. Fast and robust fixed-point algorithms for independent component analysis. IEEE Trans. Neural Netw. 1999, 10, 626–634. [Google Scholar] [CrossRef] [Green Version]
- Wick, C.; Su, J.J.; McClellan, J.; Brand, O.; Bhatti, P.; Buice, A.; Stillman, A.; Tang, X.; Tridandapani, S. A System for Seismocardiography-Based Identification of Quiescent Heart Phases: Implications for Cardiac Imaging. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 869–877. [Google Scholar] [CrossRef]
- Hyvärinen, A.; Oja, E. Independent component analysis: Algorithms and applications. Neural Netw. 2000, 13, 411–430. [Google Scholar] [CrossRef]
- Inan, O.; Migeotte, P.F.; Park, K.S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef]
- Jafari Tadi, M.; Lehtonen, E.; Saraste, A.; Tuominen, J.; Koskinen, J.; Teräs, M.; Airaksinen, J.; Pänkäälä, M.; Koivisto, T. Gyrocardiography: A New Non-invasive Monitoring Method for the Assessment of Cardiac Mechanics and the Estimation of Hemodynamic Variables. Sci. Rep. 2017, 7, 6823. [Google Scholar] [CrossRef]
- Hurnanen, T.; Kaisti, M.; Tadi, M.J.; Vähä-Heikkilä, M.; Nieminen, S.; Iftikhar, Z.; Paukkunen, M.; Pänkäälä, M.; Koivisto, T. Heartbeat detection using multidimensional cardiac motion signals and dynamic balancing. In EMBEC & NBC 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 896–899. [Google Scholar]
- Jafari Tadi, M.; Lehtonen, E.; Hurnanen, T.; Koskinen, J.; Eriksson, J.; Pänkäälä, M.; Teräs, M.; Koivisto, T. A real-time approach for heart rate monitoring using a Hilbert transform in seismocardiograms. Physiol. Meas. 2016, 37, 1885. [Google Scholar] [CrossRef]
- Scholkmann, F.; Boss, J.; Wolf, M. An efficient algorithm for automatic peak detection in noisy periodic and quasi-periodic signals. Algorithms 2012, 5, 588–603. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, BME-32, 230–236. [Google Scholar] [CrossRef]
- Rubeaux, M.; Joshi, N.; Dweck, M.R.; Fletcher, A.; Motwani, M.; Thomson, L.E.; Germano, G.; Dey, D.; Berman, D.S.; Newby, D.E.; et al. Demons versus level-set motion registration for coronary 18F-sodium fluoride PET. Proc. SPIE Int. Soc. Opt. Eng. 2016, 9784, 97843Y. [Google Scholar] [Green Version]
- Joshi, N.V.; Vesey, A.T.; Williams, M.C.; Shah, A.S.; Calvert, P.A.; Craighead, F.H.; Yeoh, S.E.; Wallace, W.; Salter, D.; Fletcher, A.M.; et al. 18F-fluoride positron emission tomography for identification of ruptured and high-risk coronary atherosclerotic plaques: A prospective clinical trial. Lancet 2014, 383, 705–713. [Google Scholar] [CrossRef]
- Jolliffe, I. Principal Component Analysis; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Jaewon, Y.; Mehdi, K.; Hope, T.; Karen, O.; Youngho, S. Technical Note: Fast respiratory motion estimation using sorted singles without unlist processing: A feasibility study. Med. Phys. 2017, 44, 1632–1637. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Year) | Height (cm) | Weight (kg) | BMI (kg/m) | |||||
|---|---|---|---|---|---|---|---|---|
| Dataset | Min–Max | Mean±SD | Min–Max | Mean±SD | Min–Max | Mean±SD | Min–Max | Mean±SD |
| DS I | 27–39 | 32 ± 4.0 | 172–190 | 178 ± 6.0 | 60–120 | 88 ± 19.0 | 20–34.0 | 27.0 ± 5.0 |
| DS II | 44–84 | 61 ± 10.0 | 153–200 | 176 ± 11.0 | 47–116 | 88 ± 17.0 | 22.4–32.5 | 28.8 ± 3.4 |
| DS III | 23–38 | 28 ± 4.8 | 173–190 | 179 ± 5.0 | 65–85 | 75 ± 7.7 | 20.7–25.7 | 23.2 ± 1.5 |
| Healthy Group Correlation) | Mean Trigger Offset (s) | ||||||
|---|---|---|---|---|---|---|---|
| Subject | ADRy | ADRx | GDRy | GDRx | GDRz | PCA | |RPM-PCA| |
| 1 | 0.65 | 0.42 | 0.48 | 0.70 | 0.65 | 0.69 | 0.29 ± 0.17 |
| 2 | 0.52 | 0.79 | 0.87 | 0.47 | 0.52 | 0.86 | 0.20 ± 0.17 |
| 3 | 0.83 | 0.94 | 0.94 | 0.79 | 0.85 | 0.96 | 0.18 ± 0.13 |
| 4 | 0.91 | 0.82 | 0.82 | 0.91 | 0.73 | 0.93 | 0.12 ± 0.08 |
| 5 | 0.72 | 0.05 | 0.05 | 0.69 | 0.24 | 0.85 | 0.37 ± 0.19 |
| 6 | 0.68 | 0.80 | 0.81 | 0.72 | 0.76 | 0.85 | 0.20 ± 0.15 |
| 7 | 0.23 | 0.87 | 0.88 | 0.17 | 0.69 | 0.91 | 0.22 ± 0.16 |
| average | 0.65 | 0.66 | 0.69 | 0.64 | 0.63 | 0.87 | 0.23 |
| std | 0.20 | 0.31 | 0.30 | 0.22 | 0.18 | 0.08 | 0.15 |
| Diseased Group (Correlation) | Mean Trigger Offset (s) | ||||||
|---|---|---|---|---|---|---|---|
| Subject | ADRy | ADRx | GDRy | GDRx | GDRz | PCA | |RPM-PCA| |
| 1 | 0.80 | 0.17 | 0.17 | 0.80 | 0.51 | 0.67 | 0.34 ± 0.20 |
| 2 | 0.92 | 0.76 | 0.79 | 0.94 | 0.81 | 0.91 | 0.28 ± 0.18 |
| 3 | 0.85 | 0.92 | 0.92 | 0.84 | 0.25 | 0.93 | 0.16 ± 0.19 |
| 4 | 0.65 | 0.55 | 0.48 | 0.44 | 0.84 | 0.81 | 0.33 ± 0.10 |
| 5 | 0.87 | 0.55 | 0.53 | 0.90 | 0.88 | 0.85 | 0.24 ± 0.20 |
| 6 | 0.08 | 0.22 | 0.23 | 0.07 | 0.06 | 0.41 | 0.27 ± 0.18 |
| 7 | 0.91 | 0.96 | 0.96 | 0.92 | 0.97 | 0.97 | 0.19 ± 0.13 |
| 8 | 0.08 | 0.16 | 0.17 | 0.09 | 0.06 | 0.69 | 0.23 ± 0.17 |
| 9 | 0.38 | 0.37 | 0.37 | 0.36 | 0.32 | 0.89 | 0.29 ± 0.16 |
| 10 | 0.56 | 0.02 | 0.26 | 0.69 | 0.58 | 0.88 | 0.33 ± 0.18 |
| 11 | 0.69 | 0.53 | 0.61 | 0.62 | 0.68 | 0.81 | 0.39 ± 0.19 |
| 12 | 0.28 | 0.74 | 0.74 | 0.56 | 0.72 | 0.78 | 0.30 ± 0.18 |
| 13 | 0.62 | 0.14 | 0.17 | 0.64 | 0.60 | 0.64 | 0.27 ± 0.18 |
| 14 | 0.33 | 0.18 | 0.19 | 0.34 | 0.13 | 0.35 | 0.47 ± 0.17 |
| 15 | 0.29 | 0.68 | 0.68 | 0.29 | 0.49 | 0.67 | 0.22 ± 0.14 |
| 16 | 0.72 | 0.63 | 0.61 | 0.71 | 0.33 | 0.79 | 0.18 ± 0.14 |
| 17 | 0.69 | 0.35 | 0.37 | 0.68 | 0.50 | 0.74 | 0.28 ± 0.19 |
| 18 | 0.11 | 0.47 | 0.47 | 0.07 | 0.16 | 0.58 | 0.33 ± 0.20 |
| 19 | 0.01 | 0.37 | 0.35 | 0.00 | 0.14 | 0.54 | 0.47 ± 0.18 |
| average | 0.52 | 0.46 | 0.48 | 0.52 | 0.48 | 0.73 | 0.30 |
| std | 0.31 | 0.28 | 0.26 | 0.31 | 0.29 | 0.17 | 0.17 |
| ICA (Fusion) | Hilbert (Accelerometer) | Hilbert (Gyroscope) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subject ID | TPR | PPV | F1 | RMSE | TPR | PPV | F1 | RMSE | TPR | PPV | F1 | RMSE |
| 1 | 0.98 | 0.98 | 0.98 | 42.5 | 0.86 | 0.83 | 0.84 | 114.3 | 0.85 | 0.84 | 0.84 | 118.0 |
| 2 | 0.93 | 0.93 | 0.93 | 49.6 | 0.98 | 0.99 | 0.99 | 51.6 | 0.99 | 0.99 | 0.99 | 43.5 |
| 3 | 0.90 | 0.90 | 0.90 | 63.0 | 0.87 | 0.86 | 0.87 | 44.0 | 0.81 | 0.80 | 0.81 | 154.8 |
| 4 | 0.94 | 0.95 | 0.94 | 107.5 | 0.87 | 0.88 | 0.88 | 60.9 | 0.84 | 0.84 | 0.84 | 142.6 |
| 5 | 0.97 | 0.97 | 0.97 | 33.5 | 0.94 | 0.94 | 0.94 | 51.1 | 0.98 | 0.97 | 0.98 | 36.9 |
| 6 | 0.81 | 0.79 | 0.80 | 42.2 | 0.45 | 0.41 | 0.43 | 160.9 | 0.71 | 0.62 | 0.66 | 114.0 |
| 7 | 0.95 | 0.94 | 0.95 | 39.4 | 0.16 | 0.16 | 0.16 | 94.8 | 0.37 | 0.37 | 0.37 | 71.9 |
| 8 | 0.92 | 0.92 | 0.92 | 35.5 | 0.83 | 0.67 | 0.75 | 104.1 | 0.85 | 0.67 | 0.75 | 68.1 |
| 9 | 0.99 | 0.97 | 0.98 | 44.0 | 0.91 | 0.76 | 0.83 | 251.5 | 0.88 | 0.74 | 0.80 | 255.2 |
| 10 | 0.99 | 0.99 | 0.99 | 16.9 | 0.98 | 0.98 | 0.98 | 25.5 | 0.99 | 0.99 | 0.99 | 5.6 |
| 11 | 0.95 | 0.97 | 0.96 | 38.0 | 0.93 | 0.95 | 0.94 | 75.6 | 0.92 | 0.94 | 0.93 | 76.6 |
| 12 | 0.98 | 0.70 | 0.81 | 91.2 | 0.99 | 0.77 | 0.87 | 81.1 | 0.99 | 0.77 | 0.87 | 47.3 |
| 13 | 0.91 | 0.97 | 0.94 | 57.9 | 0.88 | 0.92 | 0.90 | 30.0 | 0.92 | 0.96 | 0.94 | 33.7 |
| 14 | 0.99 | 0.99 | 0.99 | 53.7 | 0.93 | 0.93 | 0.93 | 74.3 | 0.92 | 0.93 | 0.92 | 162.7 |
| 15 | 0.98 | 0.99 | 0.98 | 16.6 | 0.98 | 0.98 | 0.98 | 31.0 | 0.99 | 0.99 | 0.99 | 20.1 |
| 16 | 0.76 | 0.82 | 0.79 | 98.2 | 0.55 | 0.50 | 0.52 | 138.1 | 0.69 | 0.61 | 0.65 | 110.0 |
| 17 | 0.99 | 0.99 | 0.99 | 24.0 | 0.97 | 0.98 | 0.98 | 66.3 | 0.99 | 0.99 | 0.99 | 11.5 |
| 18 | 0.98 | 0.98 | 0.98 | 87.7 | 0.99 | 0.99 | 0.99 | 20.4 | 0.99 | 0.99 | 0.99 | 52.3 |
| 19 | 0.92 | 0.94 | 0.93 | 168.3 | 0.89 | 0.88 | 0.88 | 125.7 | 0.90 | 0.89 | 0.89 | 87.3 |
| average | 0.94 | 0.93 | 0.93 | 58.4 | 0.84 | 0.81 | 0.82 | 84.3 | 0.87 | 0.84 | 0.85 | 84.9 |
| std | 0.06 | 0.08 | 0.06 | 37.6 | 0.21 | 0.22 | 0.22 | 56.76 | 0.15 | 0.17 | 0.15 | 62.9 |
| Healthy Subjects (ADR and Respiration Belt) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Normal Paced Breathing | Slow Paced Breathing | Fast Paced Breathing | |||||||
| Subject | ADRx | ADRy | PCA | ADRx | ADRy | PCA | ADRx | ADRy | PCA |
| 1 | 0.48 | 0.22 | 0.18 | 0.46 | 0.49 | 0.46 | 0.87 | 0.60 | 0.90 |
| 2 | 0.75 | 0.70 | 0.74 | 0.13 | 0.69 | 0.69 | 0.92 | 0.91 | 0.94 |
| 3 | 0.50 | 0.70 | 0.66 | 0.58 | 0.36 | 0.61 | 0.69 | 0.64 | 0.75 |
| 4 | 0.38 | 0.55 | 0.14 | 0.49 | 0.012 | 0.49 | 0.38 | 0.68 | 0.54 |
| 5 | 0.26 | 0.57 | 0.37 | 0.51 | 0.46 | 0.51 | 0.65 | 0.34 | 0.66 |
| 6 | 0.13 | 0.52 | 0.53 | 0.50 | 0.44 | 0.52 | 0.27 | 0.74 | 0.74 |
| 7 | 0.82 | 0.61 | 0.82 | 0.59 | 0.33 | 0.49 | 0.63 | 0.54 | 0.68 |
| 8 | 0.32 | 0.12 | 0.32 | 0.34 | 0.48 | 0.35 | 0.71 | 0.62 | 0.72 |
| 9 | 0.67 | 0.42 | 0.68 | 0.47 | 0.58 | 0.45 | 0.60 | 0.63 | 0.66 |
| 10 | 0.62 | 0.17 | 0.63 | 0.72 | 0.37 | 0.74 | 0.87 | 0.83 | 0.87 |
| 11 | 0.63 | 0.15 | 0.42 | 0.67 | 0.56 | 0.64 | 0.64 | 0.60 | 0.79 |
| 12 | 0.37 | 0.63 | 0.69 | 0.65 | 0.40 | 0.66 | 0.67 | 0.57 | 0.67 |
| average | 0.49 | 0.45 | 0.51 | 0.51 | 0.43 | 0.55 | 0.66 | 0.64 | 0.74 |
| std | 0.21 | 0.22 | 0.22 | 0.16 | 0.17 | 0.11 | 0.19 | 0.14 | 0.12 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jafari Tadi, M.; Lehtonen, E.; Teuho, J.; Koskinen, J.; Schultz, J.; Siekkinen, R.; Koivisto, T.; Pänkäälä, M.; Teräs, M.; Klén, R. A Computational Framework for Data Fusion in MEMS-Based Cardiac and Respiratory Gating. Sensors 2019, 19, 4137. https://doi.org/10.3390/s19194137
Jafari Tadi M, Lehtonen E, Teuho J, Koskinen J, Schultz J, Siekkinen R, Koivisto T, Pänkäälä M, Teräs M, Klén R. A Computational Framework for Data Fusion in MEMS-Based Cardiac and Respiratory Gating. Sensors. 2019; 19(19):4137. https://doi.org/10.3390/s19194137
Chicago/Turabian StyleJafari Tadi, Mojtaba, Eero Lehtonen, Jarmo Teuho, Juho Koskinen, Jussi Schultz, Reetta Siekkinen, Tero Koivisto, Mikko Pänkäälä, Mika Teräs, and Riku Klén. 2019. "A Computational Framework for Data Fusion in MEMS-Based Cardiac and Respiratory Gating" Sensors 19, no. 19: 4137. https://doi.org/10.3390/s19194137