A High-Level Control Algorithm Based on sEMG Signalling for an Elbow Joint SMA Exoskeleton


Abstract
:1. Introduction
1.1. Electromyogram Signals
1.2. Related Work
2. Materials and Methods
2.1. Elbow SMA Exoskeleton
2.1.1. Actuator Design
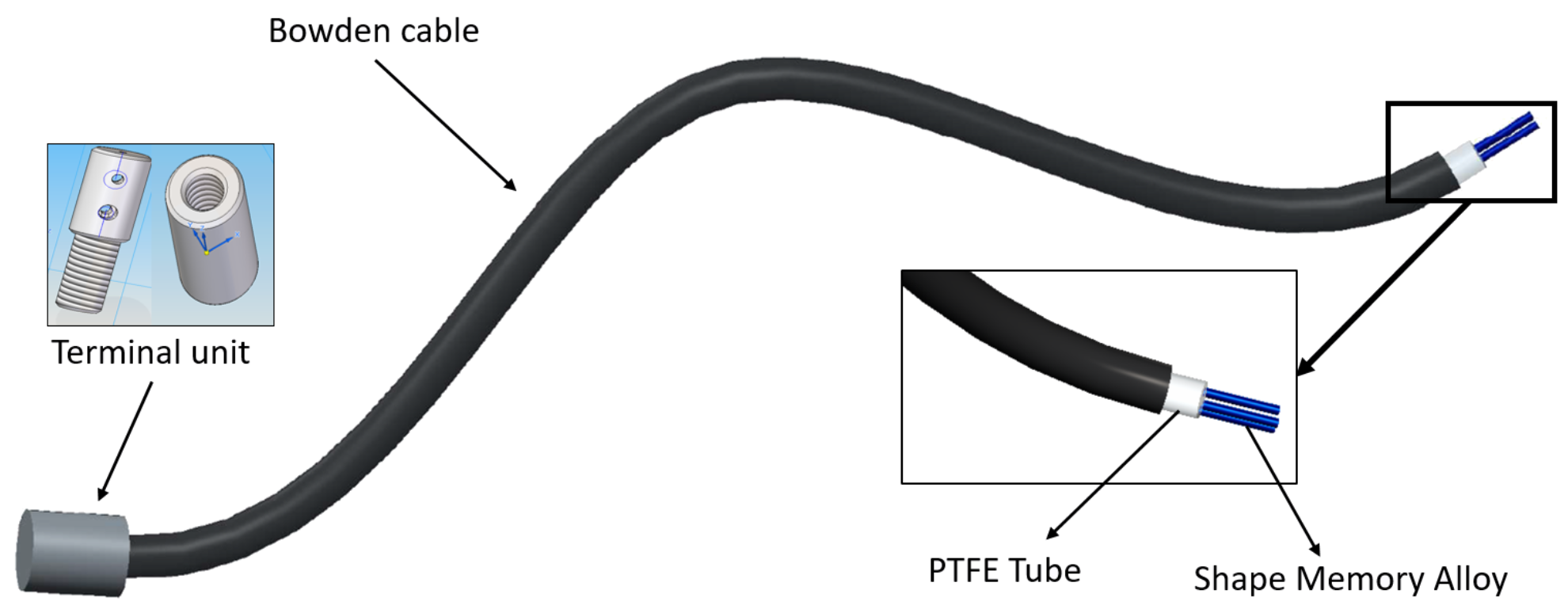
- The Bowden cable is a mechanical flexible cable which consists of a flexible inner cable that forms a metal spiral and a flexible outer nylon sheath. This type of wire can guide the SMA actuators and transmit the force. In addition, the metal has the property of dissipating the heat, which is an advantage during the recuperation of the initial position phase.
- The PTFE tube can support high temperatures, more than 250 °C; it is an electrical insulator and does not cause friction.
- The terminal units are used at one end to connect the actuator to the actuated system and at the other to fix the SMA wires to the Bowden cable. They also serve as connectors for the power supply (using the control signal). These units are formed of two pieces that can be screwed to each other to set the tension of the SMA wires. The total SMA wire tension range adjustment is 0.01 m.
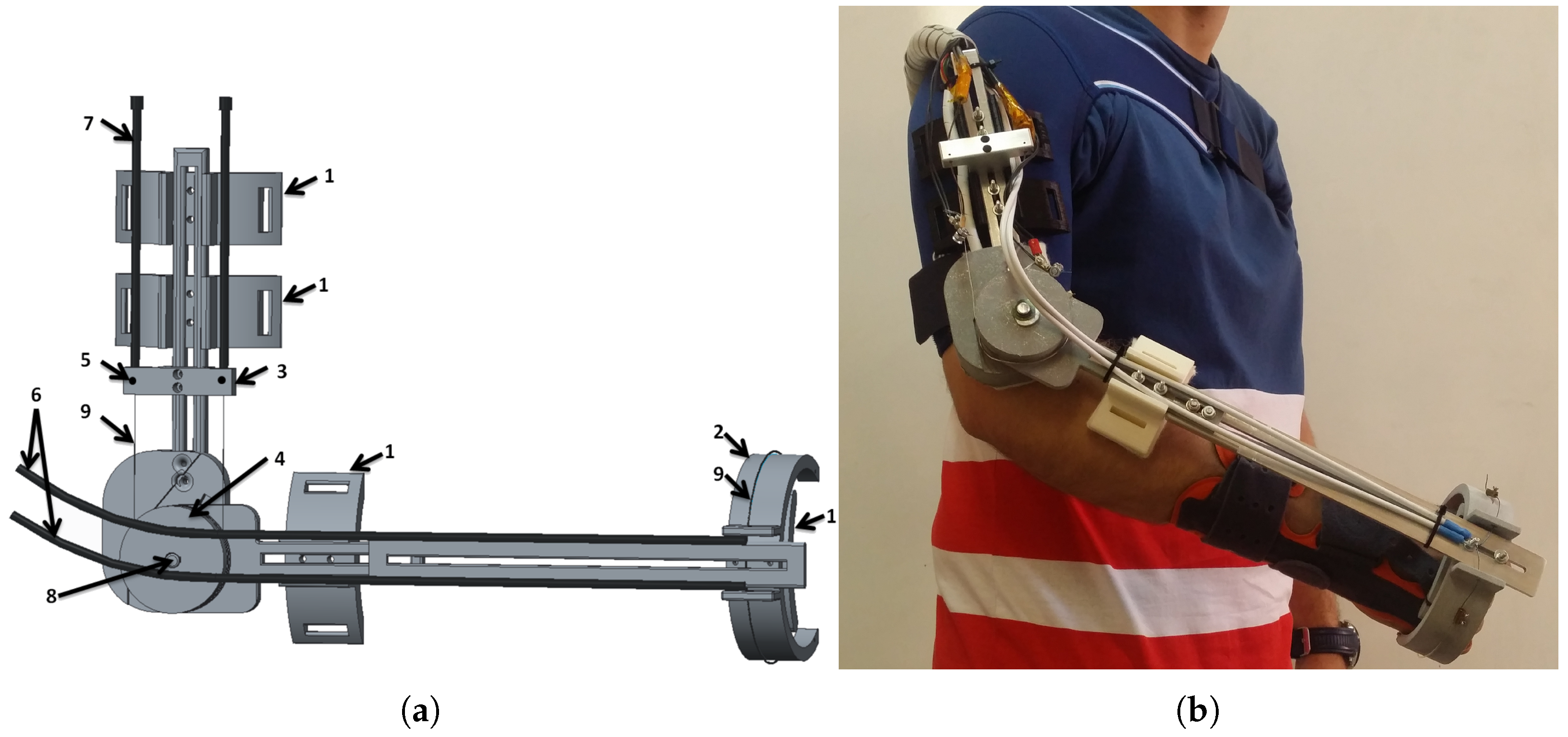
2.1.2. Exoskeleton Design
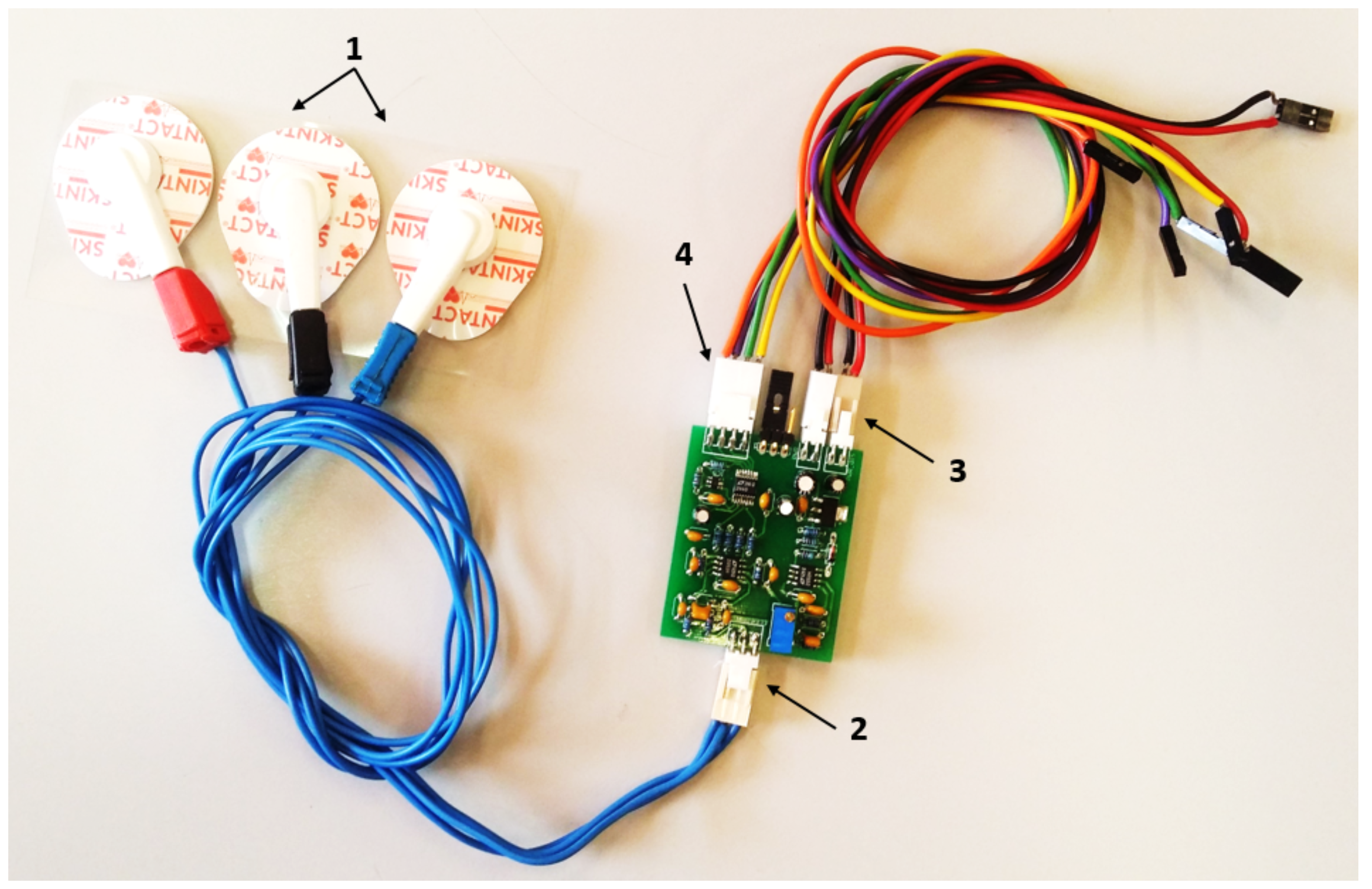
2.1.3. Electronic Hardware
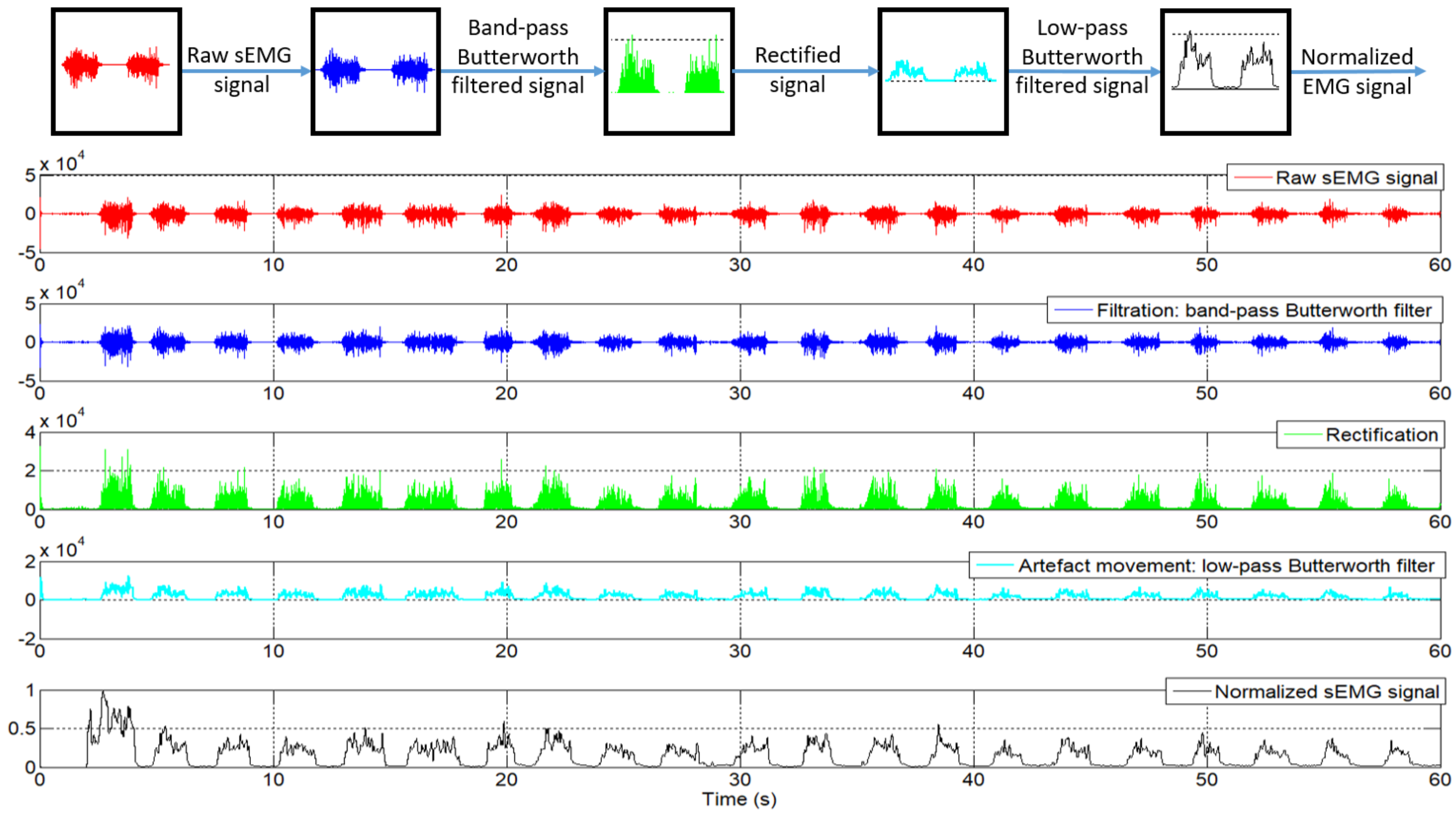
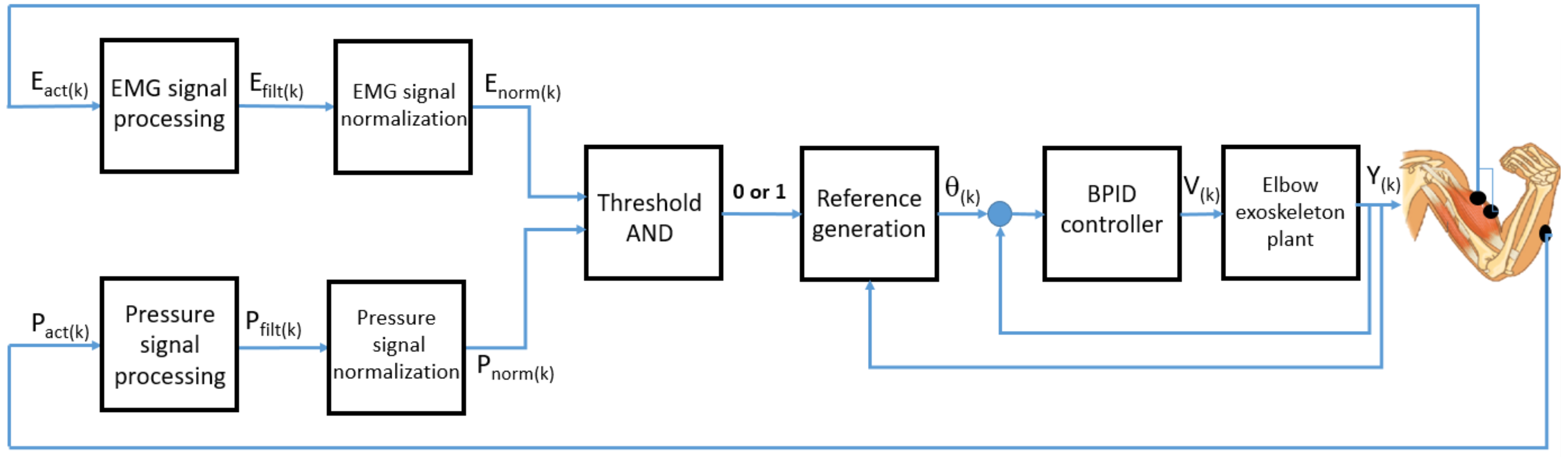
2.2. The High-Level Control Algorithm
3. Results
3.1. Results of Simulation
3.2. Results with the Real SMA Exoskeleton
4. Conclusions
- Data acquisition mode: to evaluate and diagnose the patient. Also, in this mode of operation, the angular limits of elbow movement are saved to set the angular reference limits for the control algorithm.
- Passive rehabilitation mode: The exoskeleton follows a defined angular reference, the most common being a sinusoidal type. In this case, the patient executes repetitive movements, not taking into account the movement intention of the patient. The exoskeleton can support all the movement in flexion, extension, or flexion–extension.
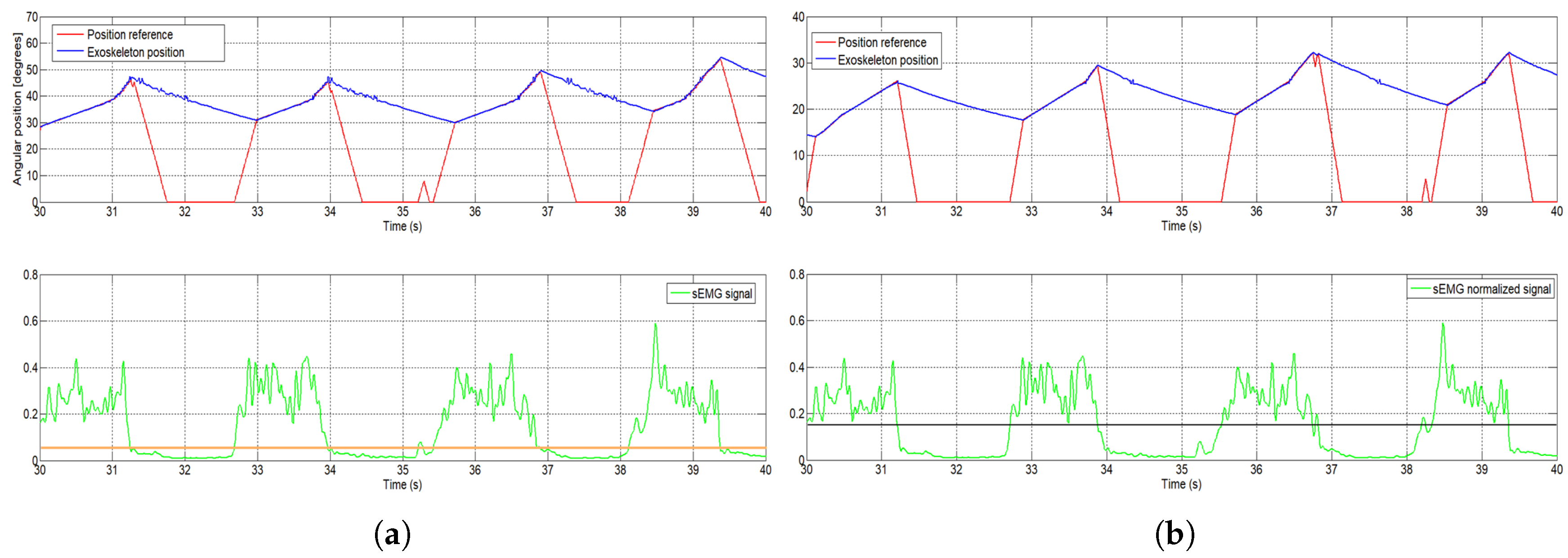
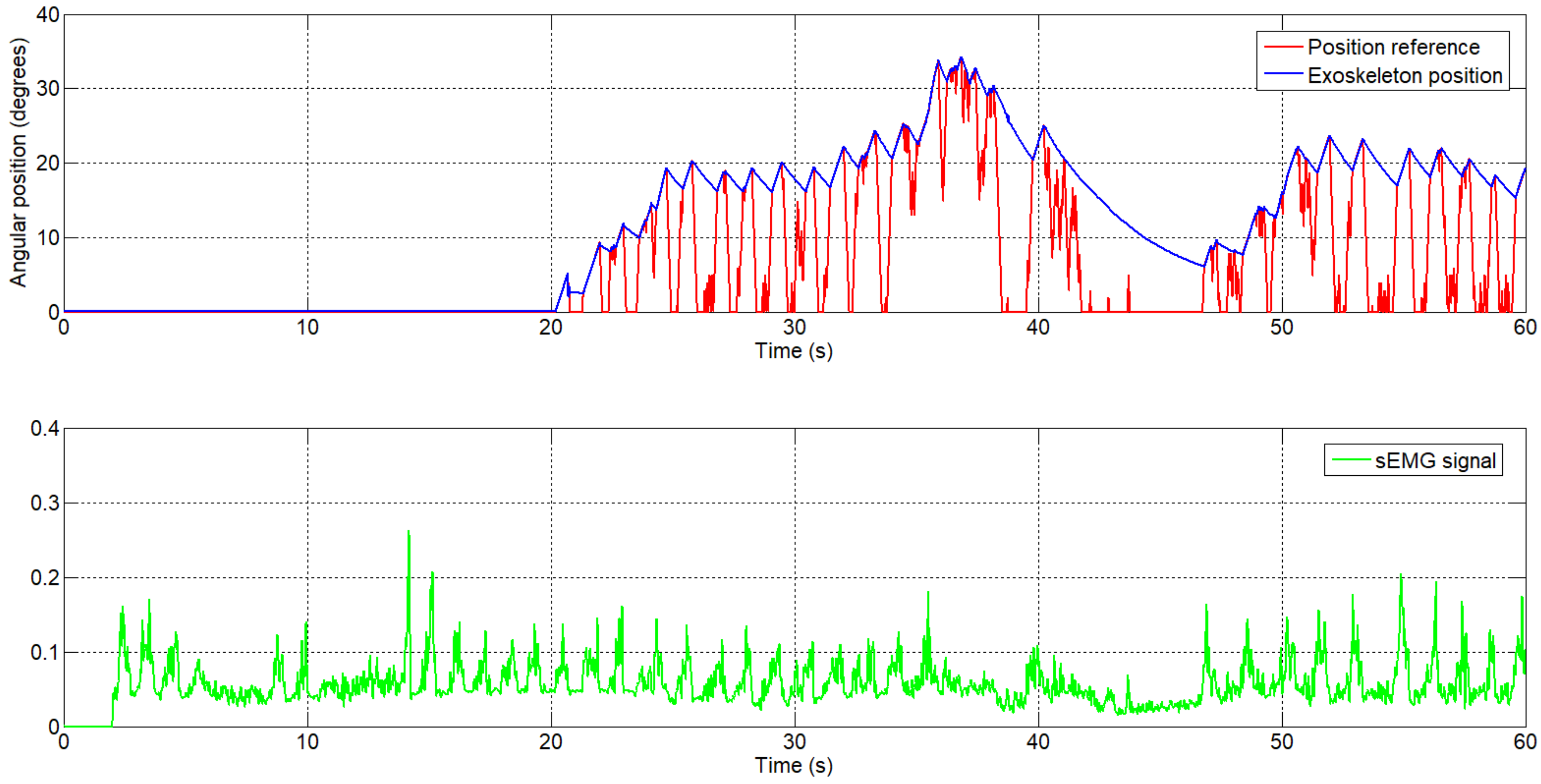
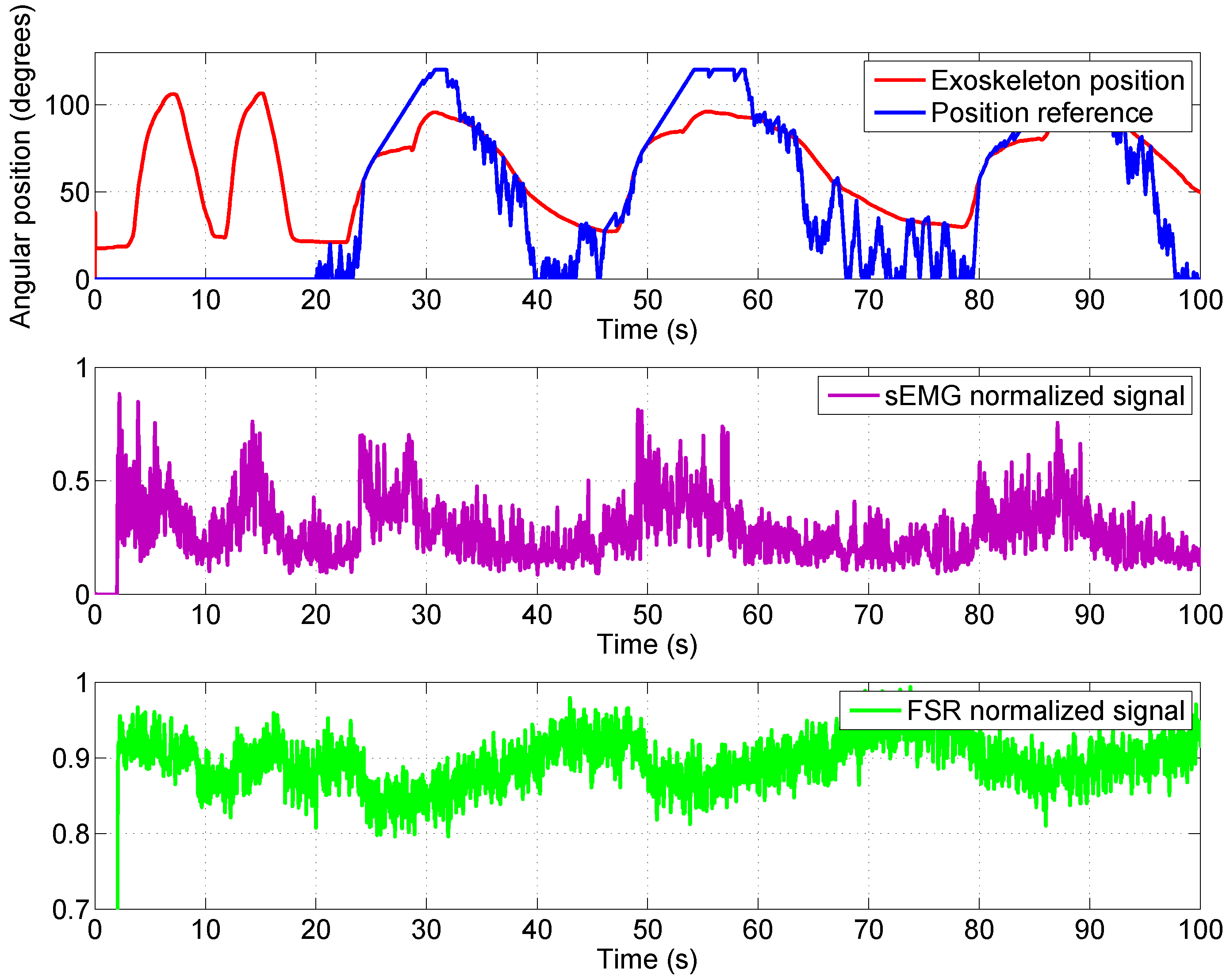
- Active rehabilitation mode: The angular reference for the elbow exoskeleton is generated as a function of the patient’s intention for movement, detected by the sEMG signals and force/pressure signals. In this case, the patient is actively involved in the rehabilitation therapy, and if movement intention is not detected, the angular reference goes to 0 degrees. This type of rehabilitation can only be used with patients who present a minimum activity level in their motor function; otherwise, a passive rehabilitation can be used.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| SMA | Shape Memory Alloy |
| UC3M | Carlos III University of Madrid |
| FSR | Force Sensing Resistor |
| PWM | Pulse-Width Modulation |
| sEMG | Surface electromyography |
| PTFE | Polytetrafluoroethylene |
| DOF | Degrees of freedom |
| SPI | Serial Peripheral Interface |
| PLA | Polylactic Acid |
| MES | Myoelectric signals |
References
- Harwin, W.S.; Murgia, A.; Stokes, E.K. Assessing the effectiveness of robot facilitates neurorehabilitation for relearning motor skills. Med. Biol. Eng. Comput. 2011, 49, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Pons, J.L. Wearable Robots; John Wiley & Sons: Chichester, UK, 2008. [Google Scholar]
- Copaci, D.; Flores, A.; Rueda, F.; Alguacil, I.; Blanco, D.; Moreno, L. Wearable Elbow Exoskeleton Actuated with Shape Memory Alloy. In Converging Clinical and Engineering Research on Neurorehabilitation II, Proceedings of the 3rd International Conference on NeuroRehabilitation (ICNR2016) Segovia, Spain, 18–21 October 2016; Springer: Basel, Switzerland, 2016; pp. 477–481. [Google Scholar]
- Copaci, D. Non-Linear Actuators and Simulation Tools for Rehabilitation Devices. Ph.D. Thesis, Carlos III University, Getafe, Spain, 2017. [Google Scholar]
- Copaci, D.; Blanco, D.; Moreno, L. Wearable elbow exoskeleton actuated with Shape Memory Alloy in antagonist movement. In Proceedings of the Joint Workshop on Wearable Robotics and Assistive Devices, International Conference on Intelligent Robots and Systems (IROS 2016), Daejeon, Korea, 9–14 October 2016. [Google Scholar]
- Norman, R.W.; Komi, P.V. Electromechanical delay in skeletal muscle under normal movement conditions. Acta Physiol. Scand. 1979, 106, 241–248. [Google Scholar] [CrossRef] [PubMed]
- DiCicco, M.; Lucas, L.; Matsuoka, Y. Comparison of Two Control Strategies for a Muscle Controlled Orthotic Exoskeleton for the Hand. In Proceedings of the IEEE International Conference on Robotics and Automation, New Orleans, LA, USA, 26 April–1 May 2004; pp. 1622–1627. [Google Scholar]
- Martini, F.H.; Timmons, M.J.; Tallitsch, R.B. Human Anatomy; Pearson Education Inc.: Old Tappan, NJ, USA, 1997; ISBN 0-13-049178-0. [Google Scholar]
- Battye, C.K.; Nightingale, A.; Whillis, J. The use of myo-electric currents in the operation of prostheses. Bone Jt. J. 1955, 37, 506–510. [Google Scholar] [CrossRef]
- Bottomley, A.H. Myo-electric control of powered prostheses. Bone Jt. J. 1965, 47, 411–415. [Google Scholar] [CrossRef]
- Farry, K.A.; Walker, L.D.; Baraniuk, R.B. Myoelectric Teleoperation of a Complex Robotic Hand. IEEE Trans. Rob. Autom. 1996, 12, 775–788. [Google Scholar] [CrossRef]
- Fukuda, O.; Tsuji, T.; Ohtsuka, A.; Kaneko, M. EMG-based Human-Robot Interface for Rehabilitation Aid. In Proceedings of the IEEE International Conference on Robotics and Automation, Leuven, Belgium, 16–20 May 1998; pp. 3942–3947. [Google Scholar]
- Kuribayashi, K.; Shimizu, S.; Okimura, K.; Taniguchi, T. A discrimination system using neural netwok for EMG-control prostheses-Integral type of emg signal processing. In Proceedings of the 1993 IEEERSJ International Conference on Intelligent Robots and Systems, Yokohama, Japan, 26–30 July 1993; pp. 1750–1755. [Google Scholar]
- Benjnya, N.; Kenney, S.B. Myoelectric Hand Orthosis. J. Prosthet. Orthot. 1990, 2, 149–154. [Google Scholar]
- Singh, R.M.; Chatterji, S. Trends and Callenges in EMG Based Control Scheme of Exoskeleton Robots—A Review. Int. J. Sci. Eng. Res. 2012, 3, 506–510. [Google Scholar]
- Vasan, G.; Pilarski, P. Learning from Demonstration: Teaching a Myoelectric Prosthesis with an Intact Limb via Reinforcement Learning. In Proceedings of the 15th International Conference on Rehabilitation Robotics (ICORR2017), London, UK, 17–20 July 2017. [Google Scholar]
- Hudgins, B.; Parker, P.; Scott, R. A new strategy for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 1993, 40, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Au, A.T.C.; Kirsch, R.F. EMG-based prediction of shoulder and elbow kinematics in able-bodied and spinal cord injured individuals. IEEE Trans. Rehabil. Eng. 2000, 8, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, K.; Tanaka, T.; Fukuda, T. Neuro-Fuzzy Control of a Robotic Exoskeleton with EMG Signals. IEEE Trans. Fuzzy Syst. 2004, 12, 481–490. [Google Scholar] [CrossRef]
- Gopura, R.; Kiguchi, K. An Exoskeleton Robot for Human Forearm and Wrist Motion Assist-Hardware Design and EMG-Based Controller. Int. J. Adv. Mech. Des. Syst. Manuf. 2008, 2, 1067–1083. [Google Scholar]
- Gopura, R.; Kiguchi, K. Application of Surface Electromyographic Signals to Control Exoskeleton Robots. In Applications of EMG in Clinical and Sports Medicine Catriona Steele; IntechOpen: Rijeka, Croatia, 2012. [Google Scholar] [Green Version]
- Kiguchi, K.; Hayashi, Y. An EMG-Based Control for an Upper-Limb Power-Assist Exoskeleton Robot. IEEE Trans. Syst. Man Cybern. Part B Cybern. 2012, 42, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Lenzi, T.; de Rossi, S.M.M.; Vitiello, N.; Carroza, M.C. Intention-Based EMG Control of Powered Exoskeletons. IEEE Trans. Biomed. Eng. 2012, 58, 2180–2190. [Google Scholar] [CrossRef] [PubMed]
- Lucas, L.; DiCicco, M.; Matsuoka, Y. An EMG-Controlled Hand Exoskeleton for Natural Pinching. J. Robot. Mechatron. 2004, 16, 482–488. [Google Scholar] [CrossRef]
- Villoslada, A.; Flores, A.; Copaci, D.; Blanco, D.; Moreno, L. High displacement flexible shape memory alloy actuator for soft wearable robots. Robot. Auton. Syst. 2015, 73, 91–101. [Google Scholar] [CrossRef]
- Technical Characteristics of Flexinol, Dynalloy, Inc. Makers of Dynamic Alloys. Available online: http://www.dynalloy.com/ (accessed on 18 June 2018).
- Saes Group. Available online: https://www.saesgetters.com/ (accessed on 18 June 2018).
- Flores, A.; Copaci, D.; Villoslada, A.; Blanco, D.; Moreno, L. Sistema Avanzado de Protipado Rápido para Control en la Educación en Ingeniería para grupos Multidisciplinares. Rev. Iberoam. Autom. Inf. Ind. 2016, 13, 350–362. [Google Scholar]
- De Luca, C.J.; Gilmore, L.D.; Kuznetsov, M.; Roy, S.H. Filtering the surface EMG signal: Movement artifact and baseline noise contamination. J. Biomech. 2010, 43, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Song, R.; Tong, K.Y.; Hu, X.; Li, L. Assistive Control System Using Continuous Myoelectric Signal in Robot-Aided Arm Training for Patients after Stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copaci, D.; Flores, A.; Villoslada, A.; Blanco, D. Modelado y Simulación de Actuadores SMA con Carga Variable. In Proceedings of the XXXVI Jornadas de Automática, Bilbao, Spain, 2–4 September 2015. [Google Scholar]
- Hioki, M.; Ebisawa, S.; Sakaeda, H.; Mouri, T.; Nakagawa, S.; Uchida, Y.; Kawasaki, H. Design and control of electromyogram prosthetic hand with high grasping force. In Proceedings of the 2011 IEEE International Conference on Robotics and Biomimetics, Karon Beach, Phuket, Thailand, 7–11 December 2011; pp. 1128–1133. [Google Scholar]
- Hioki, M.; Kawasaki, H.; Sakaeda, H.; Nishimoto, Y.; Mouri, T. Finger Rehabilitation Support System Using a Multifingered Haptic Interface Controlled by a Surface Electromyogram. J. Robot. 2011, 167516. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diameter Size [mm] | Force [N] | Cooling Time 70 °C [s] | Cooling Time 90 °C [s] |
|---|---|---|---|
| 0.025 | 0.0089 | 0.18 | 0.15 |
| 0.038 | 0.02 | 0.24 | 0.2 |
| 0.050 | 0.36 | 0.4 | 0.3 |
| 0.076 | 0.80 | 0.8 | 0.7 |
| 0.100 | 1.43 | 1.1 | 0.9 |
| 0.130 | 2.23 | 1.6 | 1.4 |
| 0.150 | 3.21 | 2.0 | 1.7 |
| 0.200 | 5.70 | 3.2 | 2.7 |
| 0.250 | 8.91 | 5.4 | 4.5 |
| 0.310 | 12.80 | 8.1 | 6.8 |
| 0.380 | 22.50 | 10.5 | 8.8 |
| 0.510 | 35.60 | 16.8 | 14.0 |
| Movement | SMA Wires | Maximum Actuator Force [N] | Length [m] | Weight [kg] |
|---|---|---|---|---|
| Flexion | 3 | 354 | 1.5 | 0.16 |
| Extension | 2 | 236 | 1.5 | 0.15 |
| Pronation | 1 | 118 | 2 | 0.1 |
| Supination | 1 | 118 | 2 | 0.1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Copaci, D.; Serrano, D.; Moreno, L.; Blanco, D. A High-Level Control Algorithm Based on sEMG Signalling for an Elbow Joint SMA Exoskeleton. Sensors 2018, 18, 2522. https://doi.org/10.3390/s18082522
Copaci D, Serrano D, Moreno L, Blanco D. A High-Level Control Algorithm Based on sEMG Signalling for an Elbow Joint SMA Exoskeleton. Sensors. 2018; 18(8):2522. https://doi.org/10.3390/s18082522
Chicago/Turabian StyleCopaci, Dorin, David Serrano, Luis Moreno, and Dolores Blanco. 2018. "A High-Level Control Algorithm Based on sEMG Signalling for an Elbow Joint SMA Exoskeleton" Sensors 18, no. 8: 2522. https://doi.org/10.3390/s18082522
APA StyleCopaci, D., Serrano, D., Moreno, L., & Blanco, D. (2018). A High-Level Control Algorithm Based on sEMG Signalling for an Elbow Joint SMA Exoskeleton. Sensors, 18(8), 2522. https://doi.org/10.3390/s18082522