1. Introduction
Due to the recent advances in sensor systems, the Internet-of-Things, and medical devices, it is possible to provide personalized and continuous health care at home [
1]. People with chronic diseases or elderly people are the ones that most benefit from these home care systems [
2]. Thanks to these developments, patients can be more independent and reduce their visits to the doctor. This contributes greatly to the quality of their life [
3]. The evolution of monitoring systems entails sensors collecting greater amounts of data; this means that we have to be prepared to process more medical data [
4].
It is therefore essential to find solutions that will allow for the management of large amounts of data in a fast, efficient, and accurate way [
5]. To achieve efficient management, it is essential to apply a context layer to the collected data. Context-aware systems play a notable role in the processing and analyzing of data [
6]. The correct contextualization of the collected information is essential for understanding it and generating knowledge that can be used in decision making. To contextualize data, it is necessary to have additional information on the context that will make the collected data coherent and reliable [
7]. In many cases, additional context information comes from heterogeneous data sources, and it is necessary that they are reliable and accurate context providers. Poorly contextualized datasets can lead intelligent applications and systems to make the wrong decisions. This is a very serious issue for medical systems, in which a wrong decision caused by a contextualization error can put the health of the patient at risk [
8]. Hence, when designing homecare systems, it is important to pay close attention to the performance of the systems that add and manage contexts in context-aware systems.
Another important issue in today’s homecare systems is environmental factors such as air quality. It has been demonstrated that acting over these factors is a determinant in the prevention of different diseases [
9]. The problem is that much of current sensor systems employ only biomedical measurement devices that users must carry with them or with which they must interact in some way (such as a pulse sensor, body temperature meter, or glucometer). Just a few projects implement systems that monitor environmental factors in the home.
The lack of research in this area creates a necessity for new proposals in the field of air quality monitoring systems in homecare. These systems must measure air quality in domestic environments with the aim of improving user’s health. Current systems are compatible with traditional health care systems, based on biomedical sensors. The combination of both systems ensures the accuracy of information; this allows the prevention or treatment of certain diseases more effectively [
10]. In some cases, the use of biomedical sensors may be highly intrusive for the patient, and experts only recommend the use of air quality monitoring systems. One of these cases is the SIDS (Sudden Infant Dead Syndrome) [
11], studied in this work. We propose a system for the monitoring of air quality factors that trigger SIDS. This health problem (also known as “crib death” or “cot death”) is the death of a child under the age of one, which occurs abruptly and unexpectedly and remains unexplained after a post-mortem study. However, placing medical sensors on the body of the newborn increases the chances of it suffering this syndrome. Death usually occurs during sleep [
12]. Associated with SIDS is the ALTE (An Apparently Life-Threatening Event) that occurs when the infant has a prolonged sleep apnea crisis; it exhibits altered muscle tone and skin color. The infant does not respond to small stimuli until cardiopulmonary resuscitation is performed [
13].
In developed countries, SIDS is one of the most frequent causes of mortality in infants aged between 28 days and one-year-old. It is the third leading cause of death in infants in the US (8%) and the most frequent in the post-neonatal period (40–50%). In 90% of cases it occurs during the first 6 months of life. Maximum incidence occurs between the 2nd and 4th month; it is infrequent in the first month of life, sporadic after six months, and exceptional after one year. The incidence of SIDS has decreased thanks to preventive actions; in most European countries it occurs 1.5 and 2 per 1000 births. In countries like Spain, mortality rates are 0.34 per 1000 births [
12]. The incidence is higher in males and in cold and wet months. This is due to excessive bedding along with excessive temperature and humidity in the room. The risk is greater if the infant weighs less than 1500 g [
13].
On the other hand, the incidence of ALTE in the United States is estimated to occur in 0.5–6% of newborns. Some studies suggest that between 5–10% of SIDS victims had previously had an ALTE episode [
14]. At present, SIDS has not been found to present any pathognomonic aspect (a symptom that characterizes and defines a certain disease). It is a multifactorial process that does not obey a specific and unique cause [
12]. However, the most accepted hypothesis associates this syndrome with a cardiorespiratory control disorder in the brainstem, causing alterations in arterial tension and in the sleep wake cycle. Alterations in respiratory regulation during sleep lead to a ventilation deficit. Babies that are at a higher risk of suffering SIDS have a lower capacity for ventilator response to hypercapnia or hypoxia, which trigger progressive respiratory depression. All this, together with external factors (e.g., viral infections, exposure to tobacco smoke, and ambient stressors) can lead to death [
15].
In recent years, other risk factors like air quality, temperature, or humidity have been identified; they are related to the environment in which the child lives. It is possible to act positively with regard to these factors and, therefore, decrease the frequency of SIDS, as demonstrated in [
16]. The monitoring of these factors is essential for preventing this pathogen from causing the baby’s death during sleep [
17,
18].
This paper presents a system that integrates different air quality sensors, together with real-time image processing techniques, for the monitoring of the main air quality factors that cause SIDS (temperature, humidity, and gases concentration). By analyzing the air quality in the room where the infant sleeps, it is possible to detect early risks that may affect them [
19]. The system includes a module that monitors the baby’s heart rate through the analysis of the images obtained by a webcam. Thanks to real-time heart rate monitoring, it is possible to monitor the health of the newborn and prevent possible episodes of SIDS. A relevant aspect of the work is that it proposes a non-intrusive system, since no sensor is in direct contact with the baby’s body. All the data generated by the sensor system is managed and contextualized by a context-aware framework. This framework is capable of generating knowledge that allows the detection of anomalies in the data. This article aims to establish a safer sleeping environment for newborns, reducing the risk factors involved in SIDS.
The article is organized as follows:
Section 2 overviews the state of the art in this area.
Section 3 describes the designed context-aware system by the authors in this paper.
Section 4 describes the proposed non-intrusive monitoring system and outlines the case study carried out in this work in a real environment. Finally,
Section 5 presents the conclusions drawn from the conducted research and experiments.
2. Previous Works
As described in the previous section, the objective of this work is the design of an air quality monitoring system that is capable of detecting risks that lead to sudden death in infants. Before designing the system, it was necessary to review the current state of the art on the topic of the work. Context-aware systems are key tools for managing and generating knowledge from the data collected by sensor systems. In this section, we look at the main developments in monitoring and sensor systems for telemedicine and homecare systems. We also review the main context-aware systems proposed in the bio-sanitary and environmental monitoring fields. Finally, studies that address Sudden Infant Death Syndrome detection are considered.
2.1. Health Care Monitoring Systems
Health systems and telemedicine are important areas for the application of the Internet-of-Things (IoT) [
20]. The capabilities provided by IoT have been used in medical applications such as remote health control, fitness programs, chronic disease treatment, or elderly care [
21]. In recent years, researchers have worked with different IoT technologies, focusing on the field of health and the resolution of a variety of practical challenges. A very popular line of research among different research groups focused on Environmental Intelligence is Ambient Assisted Living (AAL). AAL systems are destined to make elderly people independent in their own home and in a comfortable and safe way. In the study [
22], authors propose a modular architecture for automation, security, control, and communication in an AAL system. This framework provides different services to the elderly through the implementation of a radiofrequency-based communication system together with algorithms for the detection of medical problems managed by a human expert. The authors of [
23] propose an open, flexible, and secure IoT cloud platform. This platform manages numerous limitations associated with interoperability, security, quality of service (QoS), and storage of medical data. The authors of [
24] see this definition in AAL-based systems as fundamental. Other studies such as [
25] stressed that a standard technological framework should be developed for AAL systems.
Mobile health services (m-health) use mobile devices, medical sensors, and communication technologies to provide mobile healthcare services as described in [
26]. The use of m-IoT-based services has been examined for non-invasive sensor environments for the measurement of glucose levels as described in the paper [
27]. The authors of [
28] propose a system that combines the use of physical sensing devices (body temperature, blood pressure, and glucose) with non-invasive sensing devices (movement in the home, electricity consumption, and bed or sofa occupancy).
Different medical problems have been studied by researchers in recent years. The monitoring of the level of urine excreted by a patient admitted to a medical center is one example. The authors of [
29] propose the use of a low cost wireless sensing device capable of measuring the level of excreted urine in real time, which makes it possible to identify possible medical problems quickly. Another example of a studied medical problem is systems that measure the patients’ electrocardiogram. Various studies [
30,
31,
32,
33] analyzed different ECG (electrocardiography) monitoring techniques in IoT environments. There are also numerous studies that monitor patients’ body temperature remotely [
34,
35].
The non-intrusive system proposed in this work will be able to integrate easily with health care systems to provide information on air quality. In the current literature, there are no systems of this type within health care systems and that is why this work seeks to provide new work in this area.
2.2. Context-Aware and E-Health
The joint use of context-aware systems and e-health systems [
1] for the contextualization of medical data from sensors is a field that is widely studied by researchers [
36,
37]. In [
6], the authors defined the term Smart Health as a combination between e-Health and context-aware systems in smart cities. The authors made an overview of the main elements involved in Smart Health and described the different challenges and opportunities offered by this technology. The authors of [
38] proposed a remote health monitoring system, based on context-aware and wireless devices based on Bluetooth. Along the same lines, the authors of [
39] designed an e-Health system for the home environment. The proposal featured a combination of medical sensors and social sensors (temperature, opening of a door, and presence). With the use of a context-aware framework, medical and social sensors’ data are fused in order to generate knowledge that is capable of detecting anomalous symptoms in user behavior. In [
40], authors develop a context-aware system for the monitoring of a specific medical problem, in this case the continuous monitoring of an edema. There are works that try to identify and group the different context-aware architectures and the challenges they face in order to formulate a common frame of reference [
41].
In this topic, it is also not possible to find important references in the current literature that combine the use of non-intrusive systems for monitoring the risks of SIDS with a context-aware framework that provides context and precision with regard to the captured data.
2.3. Systems for the Prevention of SIDS Risks
After analyzing the current state of the art, we identified different works that propose different approaches for the prevention of SIDS. We first researched invasive monitoring systems, which use wearable devices that are placed on the newborns body. In these studies, [
42,
43,
44,
45], the authors obtain data through different medical sensors. In [
42], the authors present a band that the newborn wears on its chest; it is equipped with a temperature sensor, a pulse and breath sensor, and a motion sensor that is capable of determining the position in which he is sleeping. These sensors provide all the data needed to determine the child’s state of health. The authors of [
43] made use of commercial wearable medical sensors to collect the biomedical data of the newborn, which is sent to a remote server.
A widely studied field in the prevention of SIDS is the detection and monitoring of infant breathing while they are asleep, with the aim of detecting apneas that lead to premature death. The studies that focus on this problem adapt two particular techniques. On the one hand, there are works that propose non-invasive monitoring [
46,
47,
48,
49,
50] and use different methodologies for this purpose. The authors of [
46] analyzed the images taken by a camera installed on the baby’s crib in order to detect breathing movements. The authors of [
47] proposed the analysis of acoustic signals produced by the neonate; they were registered by a microphone installed in its cradle. In [
47], the authors presented the NanoPulse Baby SleepGuard system. This device is able to monitor breathing and heart rate during sleep. The device is equipped with UWB (ultra-wide-band) radar technology that records variations in the movement of the baby’s body. Other studies, however, propose invasive systems in which the sensors are in contact with the body. The authors of [
51] analyzed the effectiveness of an inductive sensor versus a capacitive sensor in monitoring sleep apnea.
Another field of work in the prevention and control of SIDS is the monitoring of the environment in which the newborn rests. In this line, the authors of [
52] propose the use of a device that is capable of measuring the level of CO
2 (Carbon Dioxide) exhaled by the newborn in its cradle. Thanks to the data provided by this sensor, the authors can detect possible breathing anomalies that can lead to an apnea episode. The authors of [
53] combined the use of an infrared temperature sensor together with a breathing detection system through the analysis of the acoustic signal collected by a microphone.
In the current literature, it is possible to find works that focus on the design of intelligent systems; they aim to provide accuracy in detecting possible alerts or incidents inferred from the data collected by sensor systems such as those described in this section. In [
54], the authors presented a two-level approach based on neural networks that is capable of differentiating false alarms from real incidents.
Once the current literature on SIDS detection and monitoring systems has been analyzed, it is possible to identify a lack in works related to prevention based on monitoring through environmental sensors. The studied articles focus on the use of medical sensors for monitoring the state of health of newborns, but not for prevention based on environmental factors. Therefore, the aim is to provide a novel solution through the design of an environmental monitoring system and a Context-Awareness framework. It is a non-invasive system, unlike the vast majority of works found in the literature.
4. Proposed Non-Intrusive Monitoring System
This section describes the proposed non-intrusive system for the detection of possible air quality risks that trigger sudden infant death syndrome. In the first place, the identified risk factors are described. It was necessary to consider these factors when designing the system. Second, the different sensors used in the case study are described. Moreover, we look at gas levels that are considered harmful by human experts. The heart rate calculation system is also described below; it obtains the infants heart rate by analyzing the images captured by the webcam. Finally, we overview the entire system and the results obtained in the case study.
4.1. Analysis of Risk Factors in SIDS
This section analyses the different risk factors involved in SIDS. First, all the elements related to the neonate are analyzed. All those factors that do not have to do with the atmospheric conditions have been discarded, since that is not the objective in this study.
Table 2 shows the direct risk factors [
73].
Out of these factors, those that do not require environmental monitoring such as: age, sex, race, etc., should be discarded. These data will be relevant when contextualizing the data measured by the sensor network. The monitoring of the position of the newborn while asleep has been ruled out in this work. The use of any sensor that registers the position requires the placement of a device in the baby’s body that would add a new external risk factor. The only non-intrusive method of monitoring this factor is through the analysis of the camera images, which will be studied in a future line of work.
The air quality factors that can be monitored in real time are exposure to tobacco smoke, the increase in the amount of CO2 in the environment as a result of sharing bed with parents or siblings, and the thermal stress produced by the heating systems together with an increase in humidity. In addition, a monitoring of the concentration of accumulated gases in the room where the newborn rests is carried out.
4.2. Sensorization System
To monitor the identified risk factors, it is necessary to implement specialized hardware that will support the different sensors. This device will act as the central monitoring node in the proposed sensor network. In the current market there are different types of devices that have this capacity. The Arduino platform is the most extended, free code, and reduced cost. Therefore, a board based on Arduino has been the device used in the design of the system.
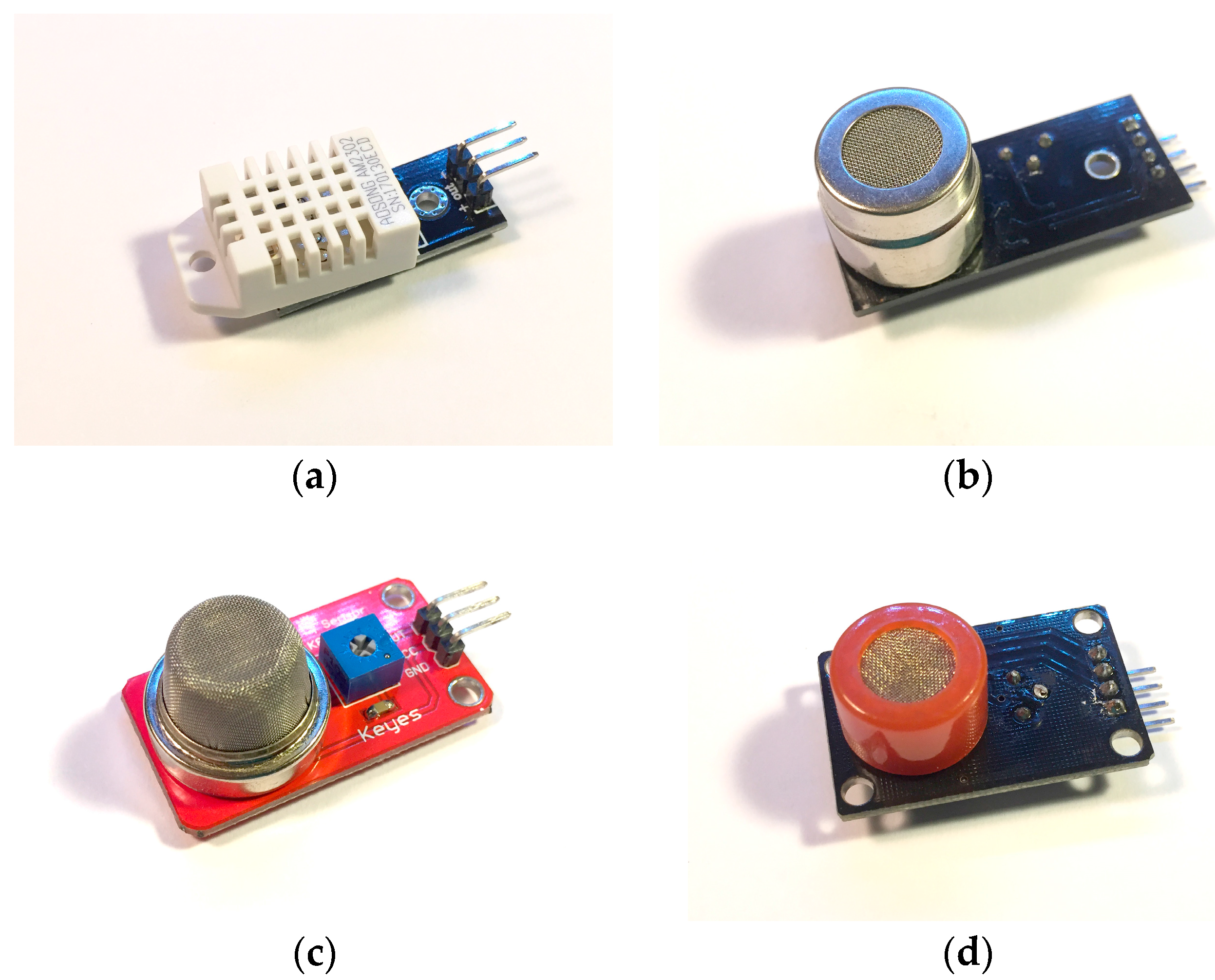
Next,
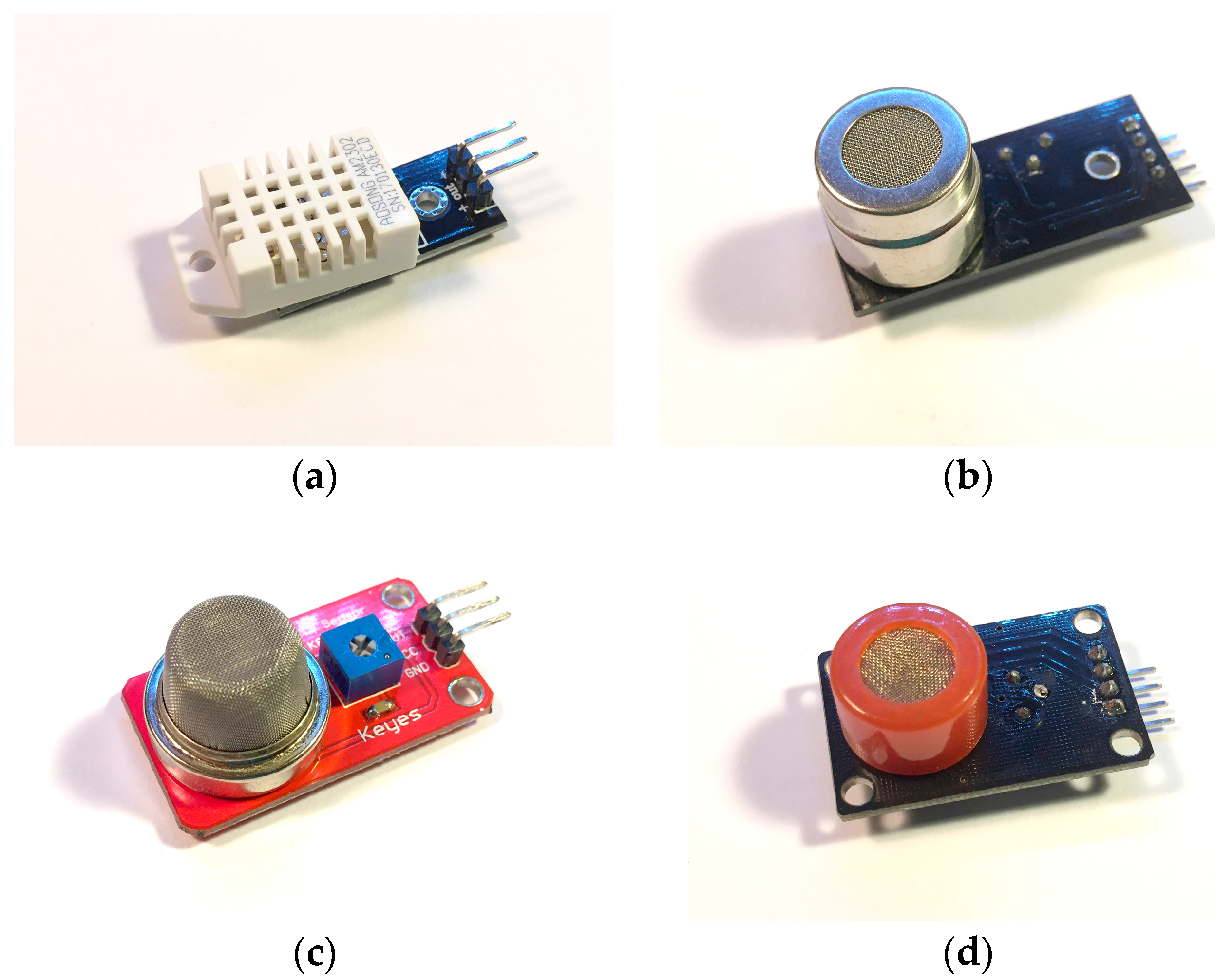
Figure 3 describes the air quality sensors that will be part of the architecture. These sensors are low cost and have a high accuracy when measuring both temperature and humidity and the concentration of harmful gases. The sensors have been previously calibrated by the manufacturer and have an accuracy of ±1%.
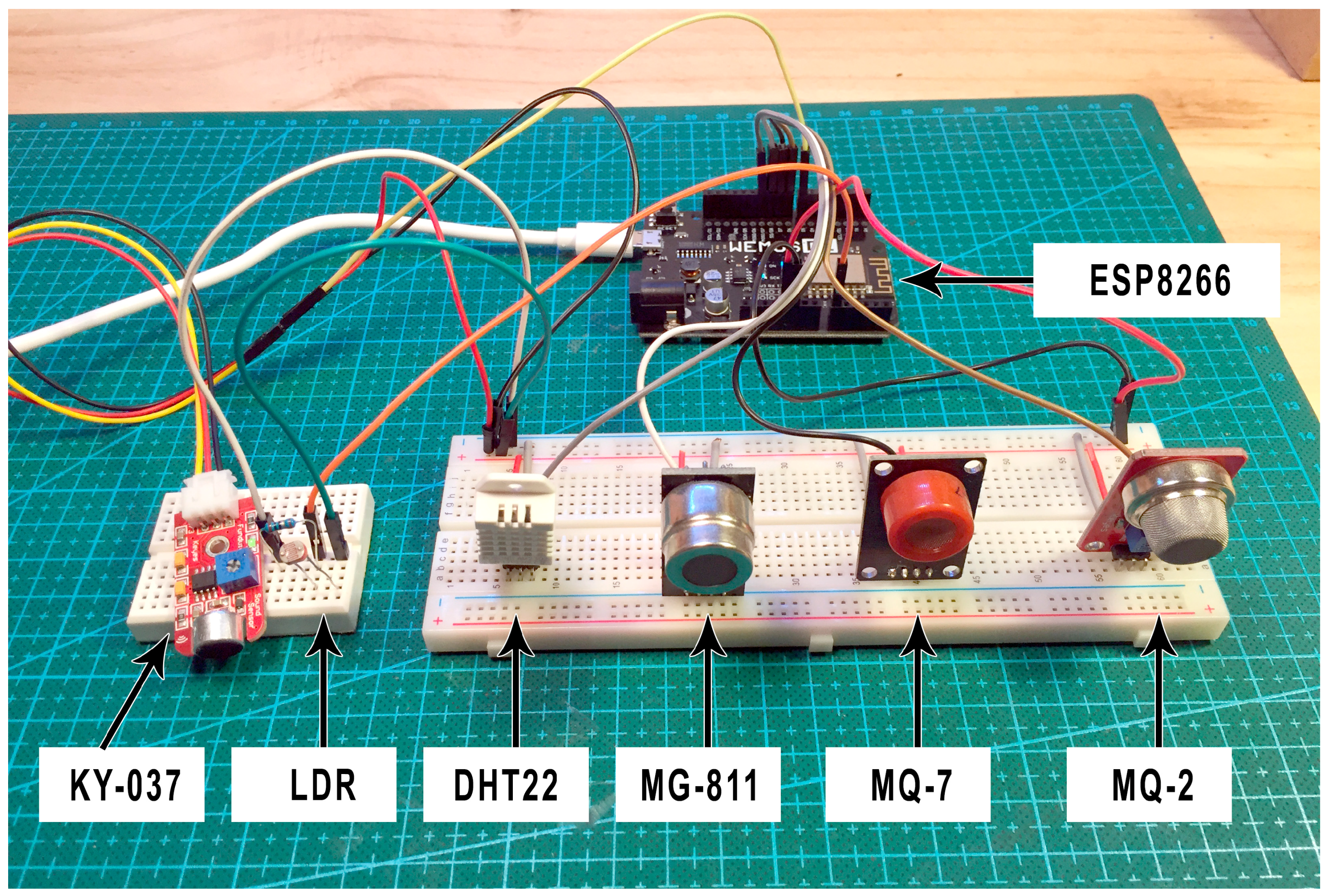
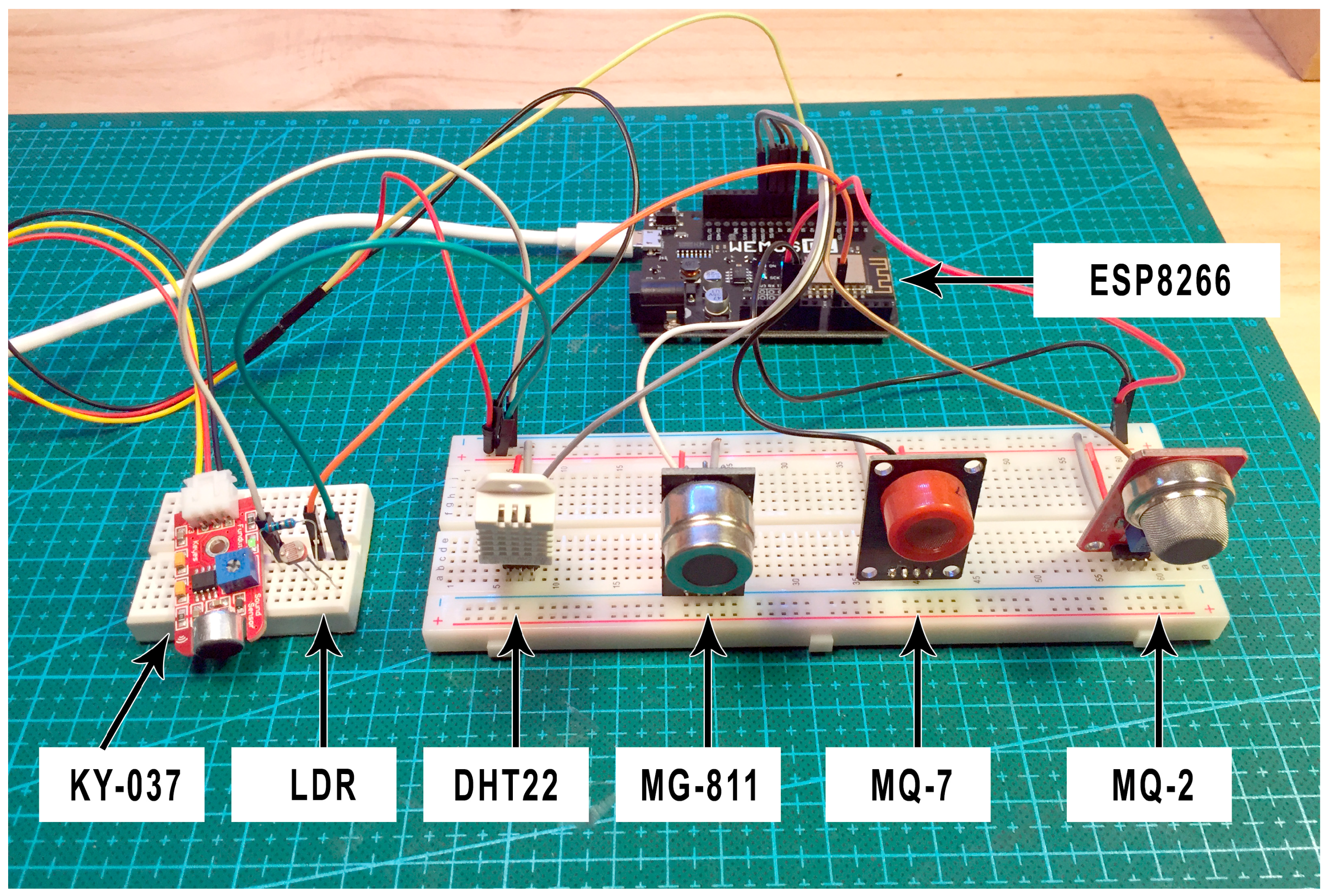
Figure 4 shows the sensor network (MG811, MQ-7, MQ-2, and DHT22) connected to the Arduino microcontroller. Additionally, the system incorporates a sound sensor (KY-037) and an LDR sensor in order to provide context data such as the presence of people in the room or the state of light. The final set of sensors will be responsible for collecting all data in the infant’s room.
Additionally, the system will have wireless WiFi connectivity, allowing the data to be sent to the remote server. This is possible thanks to the connection of an ESP8266 module that allows for the connection of the Arduino microcontroller board with the home’s wireless network.
4.3. Harmful Concentration Levels
At present, there are different international agencies and societies in charge of designing and elaborating different air quality standards. These standards warn of gas concentration levels that may be harmful to health, according to the conducted medical studies. Some of the main standards are:
NAAQS (National Ambient Air Quality Standards) [
74]; this is a standard for the regulation of air quality in open spaces in the United States.
OSHA (Occupational Safety and Health Administration) [
75] is also a US standard for air regulation in industrial environments.
MAK (Maximum Concentrations at the Workplace) [
76] for the regulation of quality levels in industrial environments provided by the German government.
Canadian [
77] air quality levels for domestic and housing environments created by the Canadian government.
WHO (World Health Organization)/Europe [
78] general air quality standard (both indoor and outdoor).
One of the main societies in charge of writing and reviewing these standards is ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers) [
79]. This company has developed a standard called Ventilation for Acceptable Indoor Air Quality [
80], which lists harmful concentration levels for common gases. It is a widely accepted standard in the scientific community and will be the basis for determining dangerous concentration levels in the proposed system.
Table 3 shows the maximum exposure levels to these gases (CO, CO
2, and tobacco smoke) during a day that will be used as reference values in the Service Provider module of our proposed BDCaM framework. The maximum humidity and temperature levels in a room where the newborn sleeps are also detailed. These data correspond to the central region of Spain and to the temperate seasons (such as spring or autumn) during which the case study described in this work was carried out.
4.4. Heart Rate Calculation through Open CV
Once the air quality factors in the newborn’s bedroom have been monitored, the task of obtaining the pulse through a non-invasive system is dealt with. For this purpose, we employed a technique called photoplethysmography [
81]. Photoplethysmography or PPG is a technique of non-invasive detection of the cardiovascular pulse wave (also called pulse of blood volume) in the reflected light variations. This technique provides the information needed to calculate the heart rate. A small wireless webcam on the periphery of the newborn’s cradle to obtain images from which data are extracted.
One problem with the measurement of PPG is that it is susceptible to signal corruption induced by motion and motion artifacts, as detailed in [
82], which are caused by the movement of whole or part of the displayed object. An optimal technique for eliminating noise in the PPG signal is the blind separation of BSS sources (Blind Source Separation) [
82].
Blind source separation is a signal processing technique that consists of estimating sources in linearly mixed signals. For the treatment of the PPG signal, the BSS is implanted using the ICA technique (Independet Component Analysis) [
83].
ICA is a technique of signal discovery from independent sources of a set of observations that are composed of linear mixtures of the underlying sources.
The data is represented by a random vector
(1) and the components by a random vector
(2). The objective of ICA is to transform the observed data
using a linear static transformation
as indicated in (3) in S maximally independent components, measured by some function
(4) of independence. This technique is used because it contains a large capacity to reduce artifacts by movement in PPG signals.
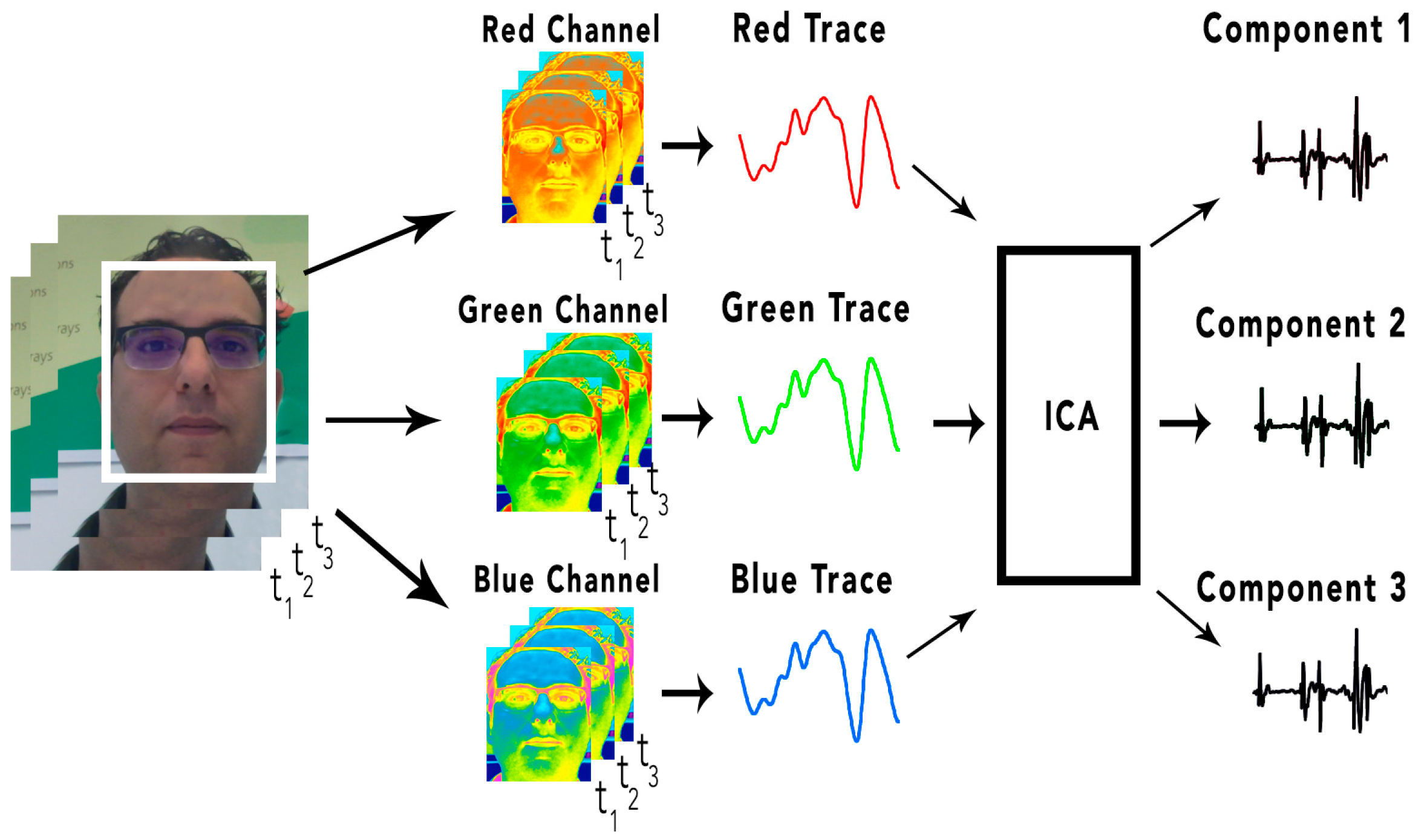
The underlying signal of interest that ICA uses is the wave of the cardiovascular pulse that spreads throughout the body. During a cardiac cycle (cardiovascular pulse), the facial blood vessels change volumetrically by modifying the length of the trajectory of the incident light; these changes in the amount of reflected light indicate the time of the cardiovascular events. Using the RGB sensors that make up a camera, a mixture of the plethysmographic signal reflected by the light can be collected. The objective of ICA is to find a separation of the PPG signal in order to collect the independent sources contained in it. An overview of how the pulse is recovered by volumetric changes in the blood vessels (plethysmographic signal) is shown in
Figure 5.
First, a tracking and face detection system has been developed within the video frames to locate the region of interest. For this, OpenCV (Open Computer Vision) is used. The face detection algorithm is based on the work of the authors of [
35] through a pre-trained Haardcascade capable of detecting the region of interest in an image.
Once the region of interest is located, it is separated into three RGB channels, generating a spatial average over all the pixels of the region, thus producing the three signals: Red, Green, and Blue. The signals generated are decomposed into three other signals from independent sources using ICA. Finally, the FFT (Fast Fourier Transform) is applied to the second resulting signal to obtain the power spectrum. The pulse frequency is designated as the frequency that corresponds to the highest power of the spectrum within an operating frequency band. Therefore, an operating range of [0.75, 4] Hz is used, which corresponds to [45, 240] bpm (beats per minute). In this way, a wide range of heart rate measurements is provided.
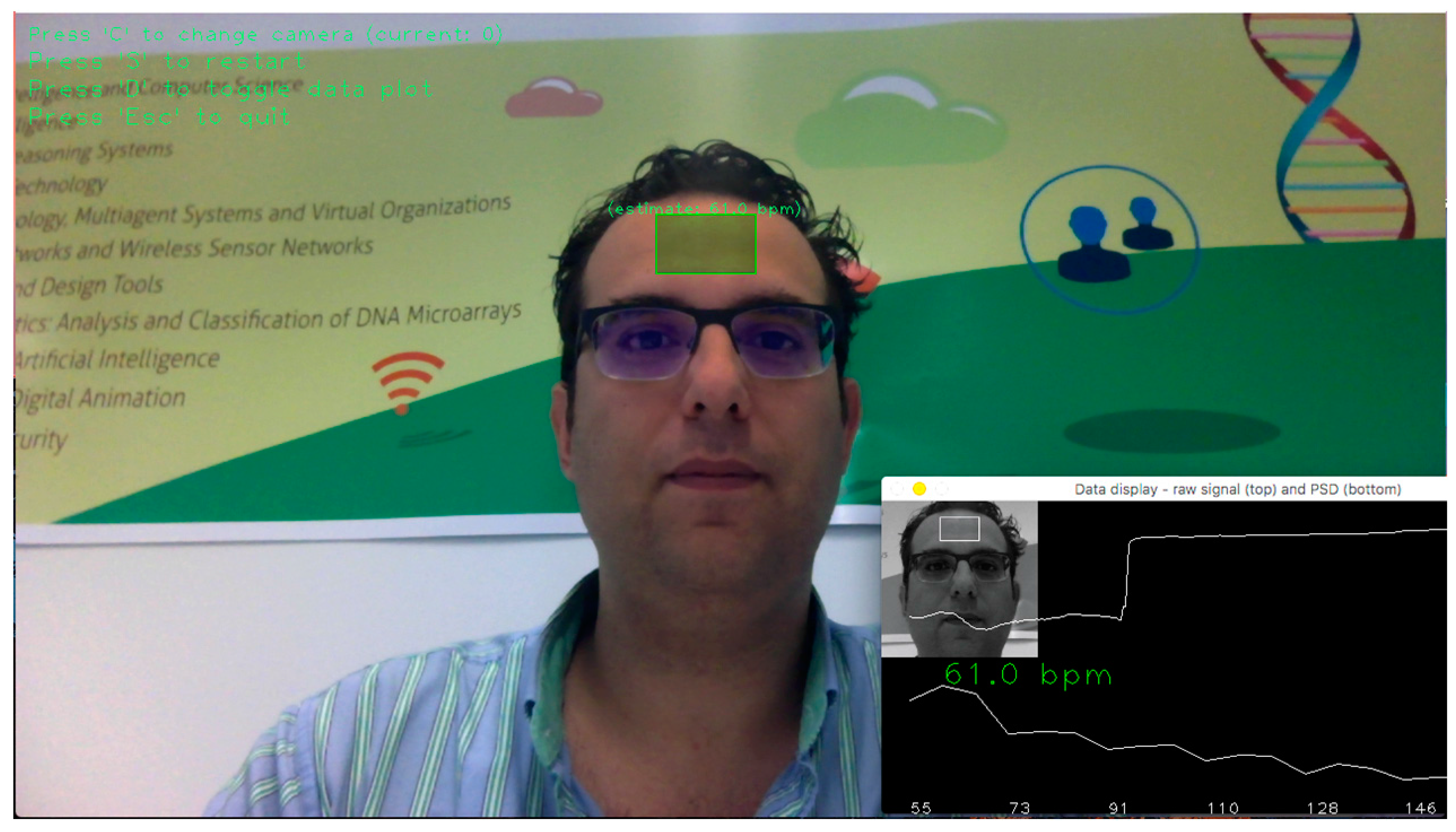
Figure 6 shows the system operating through a wireless webcam. The software recognizes the region of interest that is the forehead (in green) and determines the user’s pulse through the analysis of the images.
4.5. Final System
Having described the elements of the designed system, the connection between the different nodes of the network is detailed.
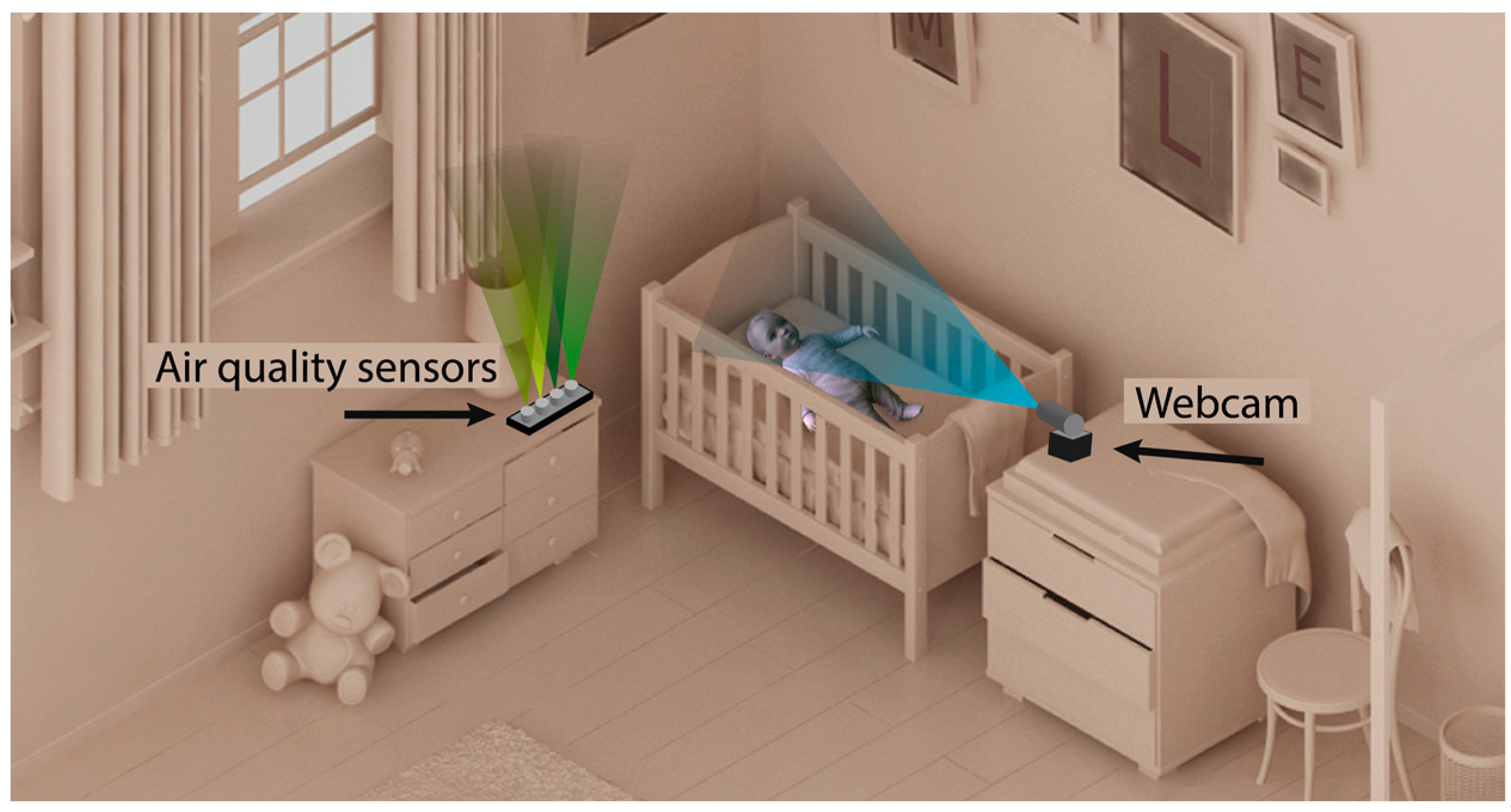
Figure 7 shows that the proposed system is based on the installation of the two nodes described in the previous sections. One of the nodes is the air quality sensor system shown in
Figure 4, which is located next to the newborn’s cradle. It is a wireless device that can be connected to the conventional electrical network. The other node is the webcam that takes images for the calculation of the pulse; it must be located in front of the cradle. In this way, the face of the newborn is captured regardless of the position in which it is sleeping.
The data captured by the different air quality sensors are sent wirelessly every 120 s through the domestic Wi-Fi network to the central node of the system. The images of the webcam are also sent to this node.
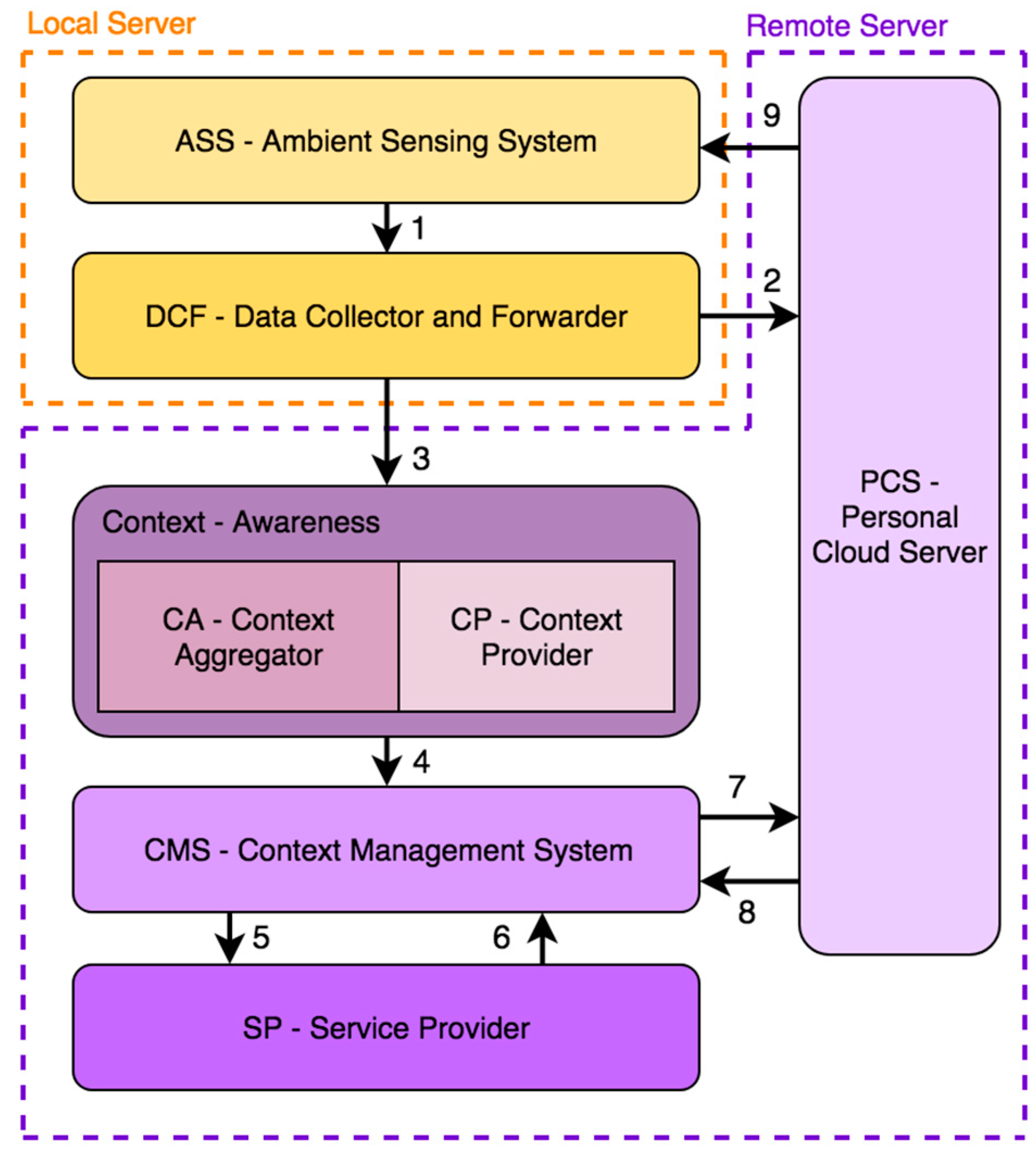
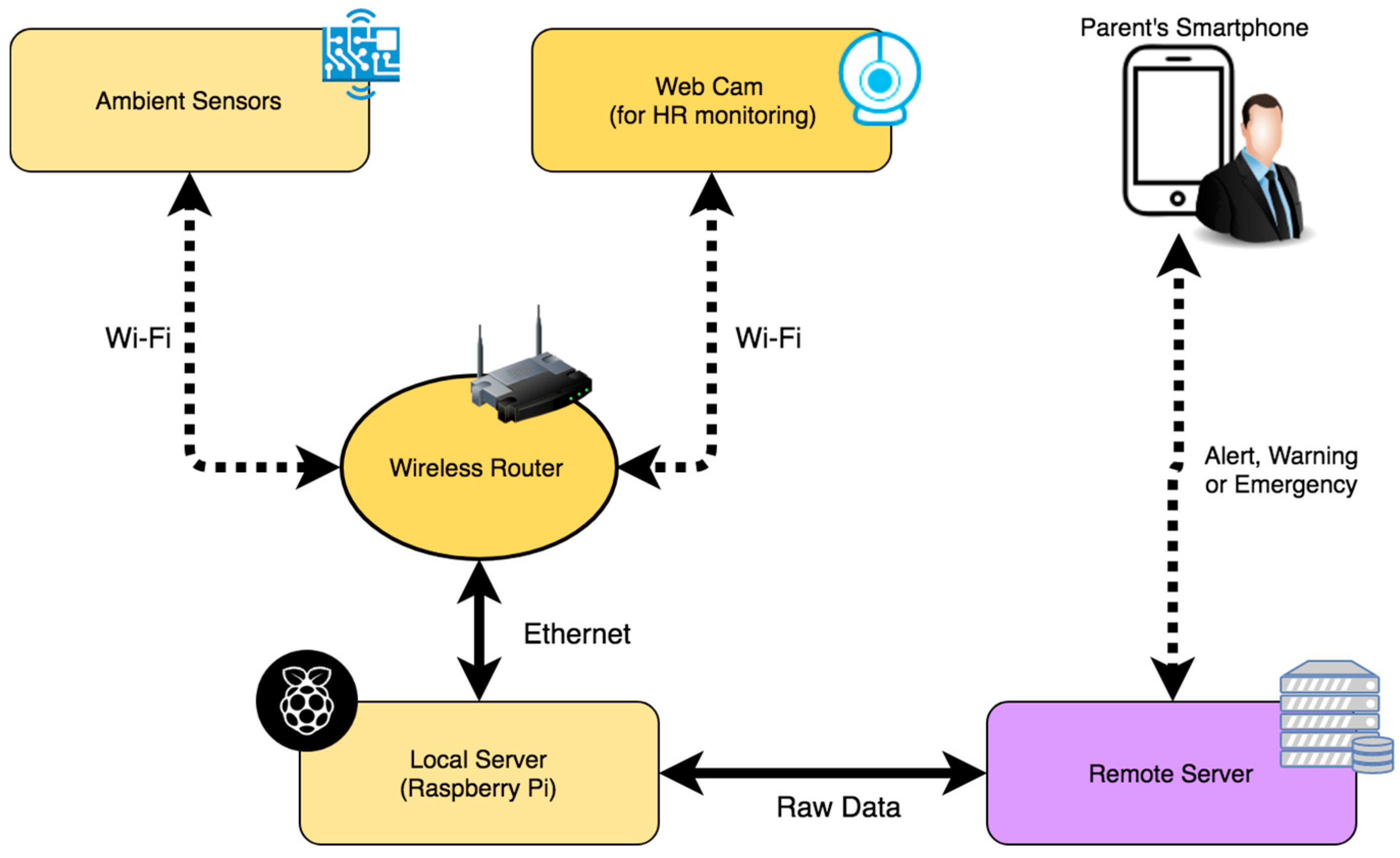
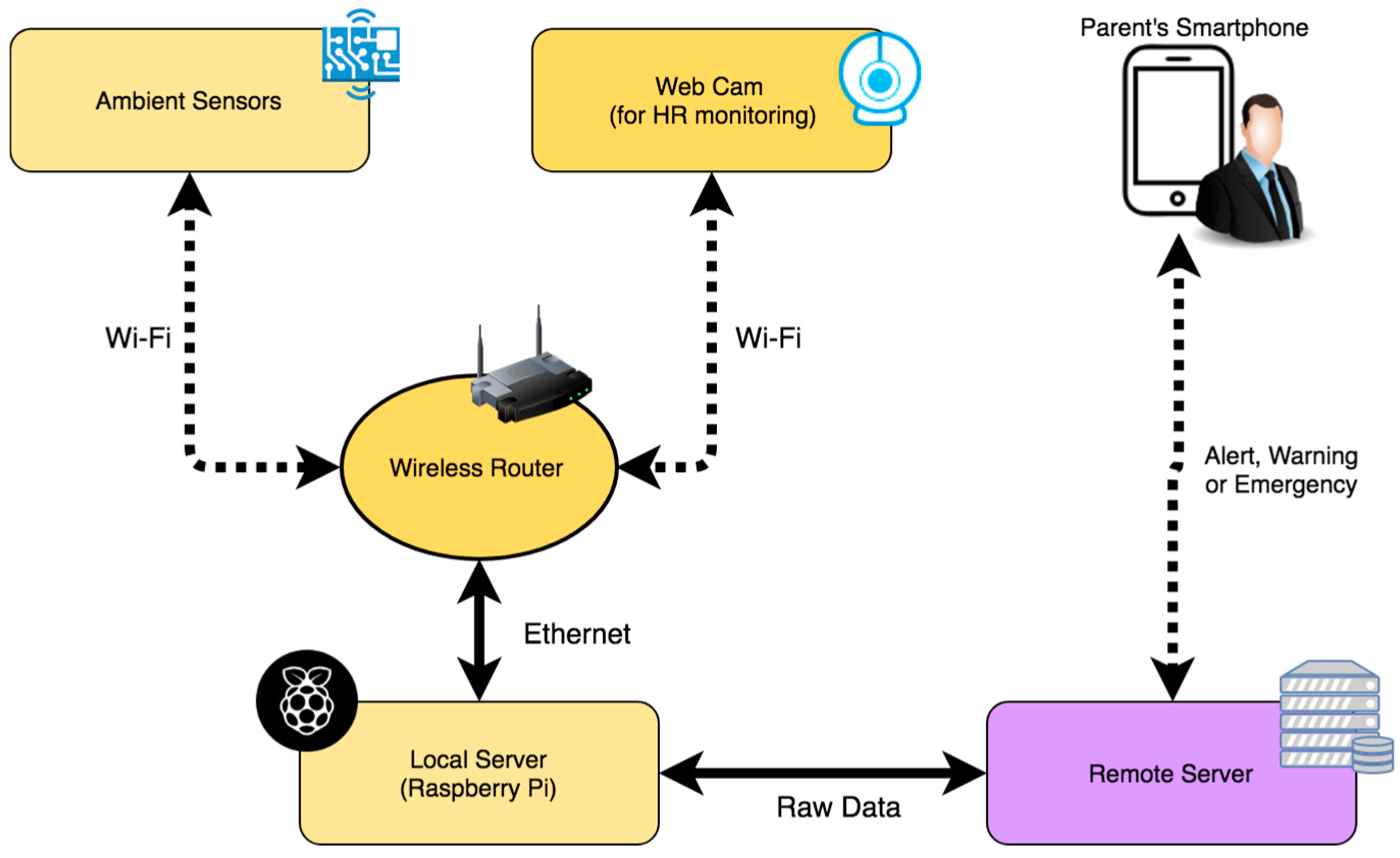
Figure 8 shows the different elements of the system and their different connections in the network. As a local server that acts as the central node responsible for obtaining the information that arrives from the other two nodes, the Raspberry Pi microcomputer is used. It is a low cost device that has the necessary computing capacity both to obtain air quality data and to process the images of the webcam and get the pulse of the newborn. Once these data are analyzed, they are sent in raw to the remote server defined in the BDCaM model, which will be responsible for processing and analyzing the information. In the case of detecting an anomaly in the values obtained (such as measured values above the maximum allowed or the loss of the newborn’s pulse), the emergency process is triggered, and an alert notification is sent to the mobile device of the parent or caregiver.
4.6. Experimental Results
At the time of performing the experimentation of the system designed in this work in a real environment, 5 households were selected in which the system was deployed for 3 months. In the households, described in
Table 4 and
Table 5, neonates live between the ages of 3 and 14 months.
In order to generate specific rules for each baby within the system, the contextual data related to each one has been transformed into numerical data as shown in
Table 5. Thanks to this transformation, the processing of the data and its subsequent analysis is carried out in a faster and simpler way. These data are fundamental when contextualizing the information measured by the sensorization system.
In a traditional alert system based on thresholds, there are only two possible states for an alert: active or not active. The designed system is able to identify different alert levels and trigger actions according to their degree.
Table 6 shows the different classes and basic classification rules defined by the human experts for the case study. These rules are based on the current context calculated in the context-aware framework designed.
To evaluate the accuracy and performance of the system, a comparison was made between the classifications made by the proposed system and a set of general medical rules based on thresholds. In
Table 7, it is possible to visualize the obtained results. Each of the measured data represents each of the measurements made by the system. As previously described, the system sends a data (set of values measured by the different sensors) every 120 s; this leaves a total of 720 data per day. Thus, during the 3-month case study 64,800 data were obtained in total from the 5 houses. After contextualizing the data, the new aggregated values are analyzed together with the original data. After preprocessing these data and eliminating erroneous data produced by system failures or connection errors, less than 64,800 data were left. In
Table 7, we can observe that when a measured value is above or below the threshold, the traditional threshold-based system deduces this abnormal situation producing numerous false positives. On the other hand, the proposed system is able to learn the corrected threshold quickly for each patient and in each context.
Additionally, a web application has been developed to control and visualize all the parameters.
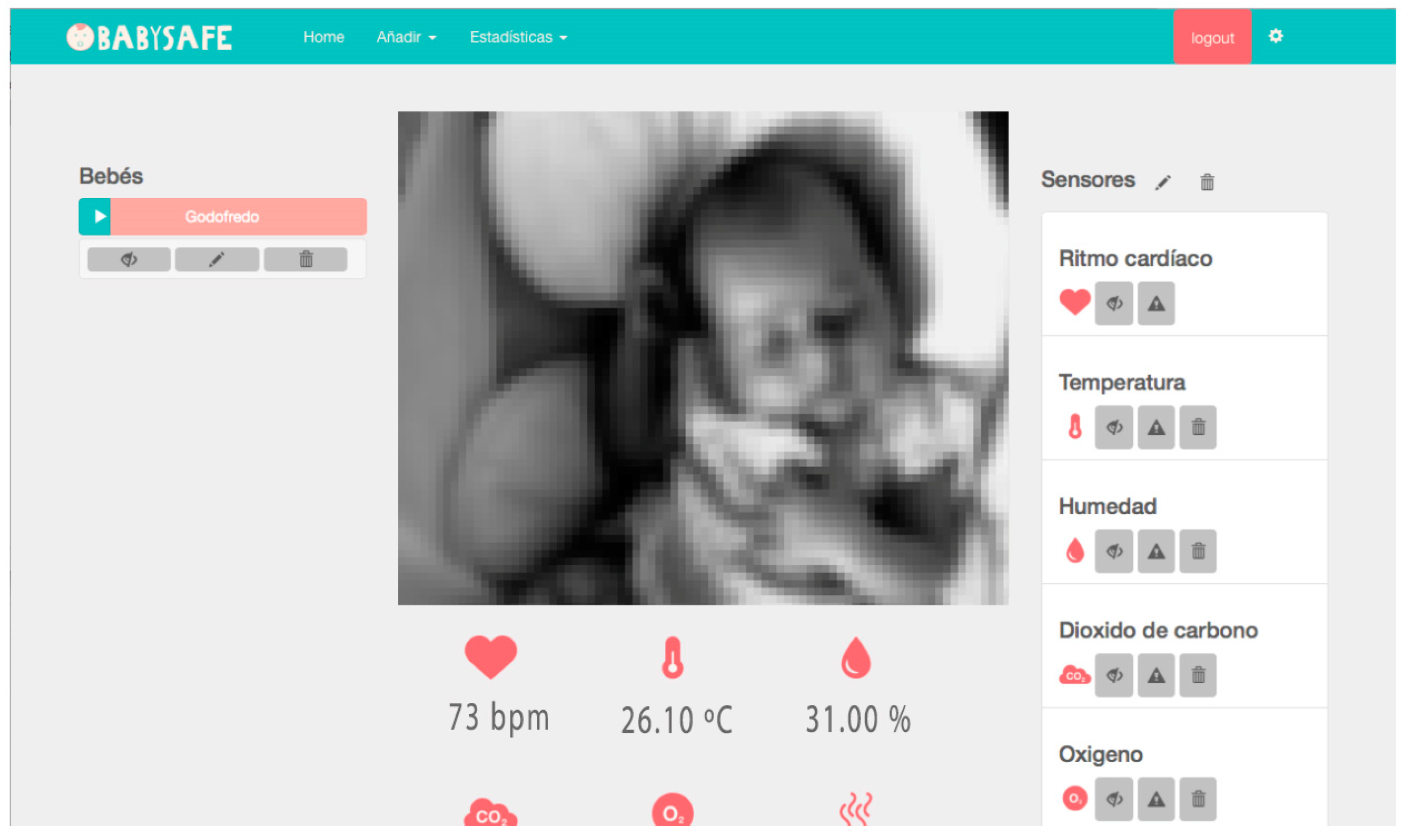
Figure 9 shows a screenshot of the developed web interface. In the central part, the image of the baby is shown in real time. For security reasons, this functionality is only available if the user accesses the application from the same home network where the camera is located. The images taken by the camera are not sent through the network. The values measured in real time are displayed in the lower part of the image. On the right-hand side, we can find a list of the different sensors. In the lower part of the image, the icons are used to define the threshold values from which the different warnings and alerts are triggered. It is also possible to turn off or activate the sensors individually or display a history of data recorded by them.
A mobile application has been developed in order to notify the parents and caregivers of any incidents. This application consists of a simple interface which can be accessed by logging in. Once the user is logged in, the remote server will notify the user when an emergency occurs. This application, therefore, allows parents or caregivers to intervene quickly when an emergency occurs.
5. Conclusions
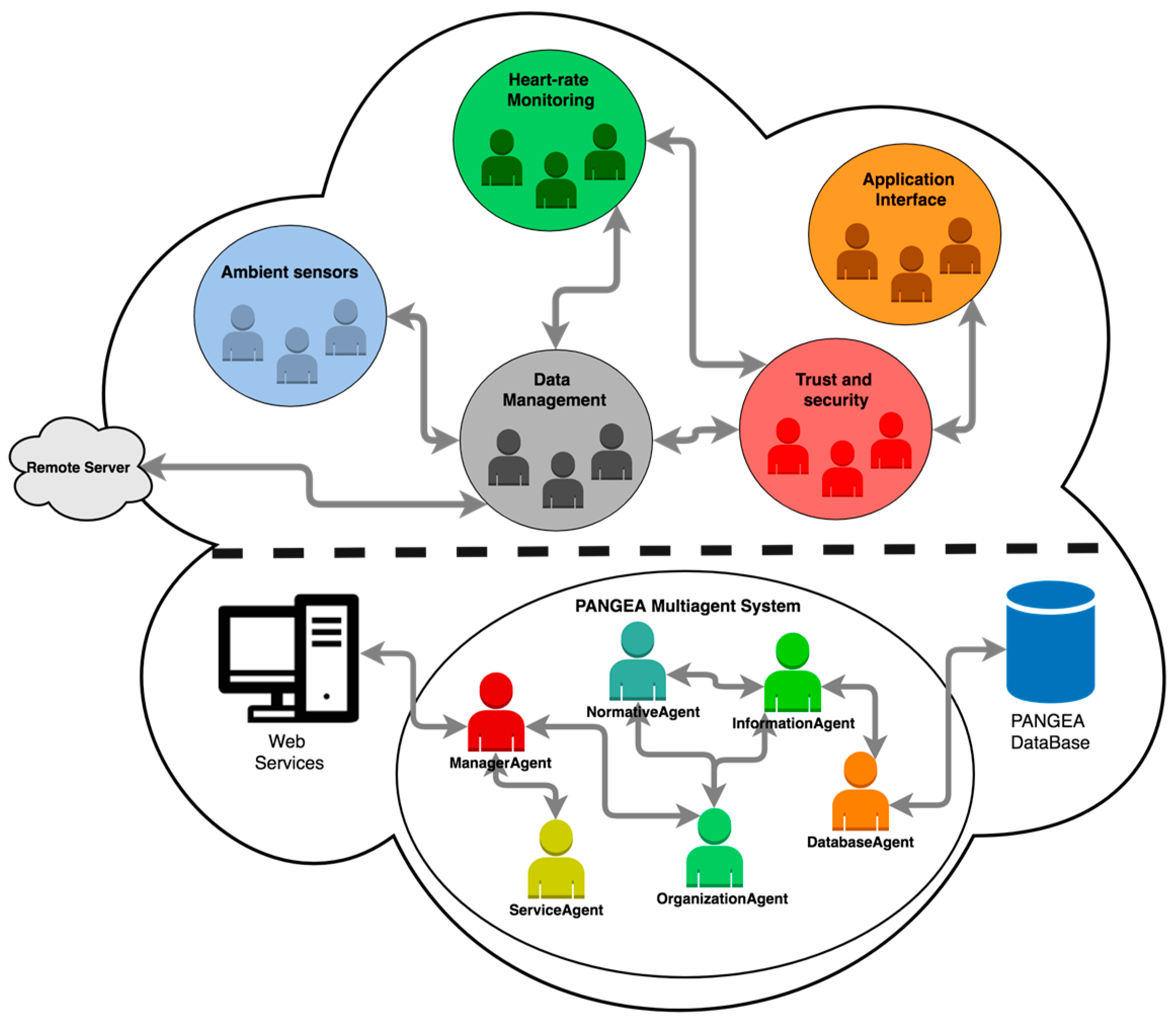
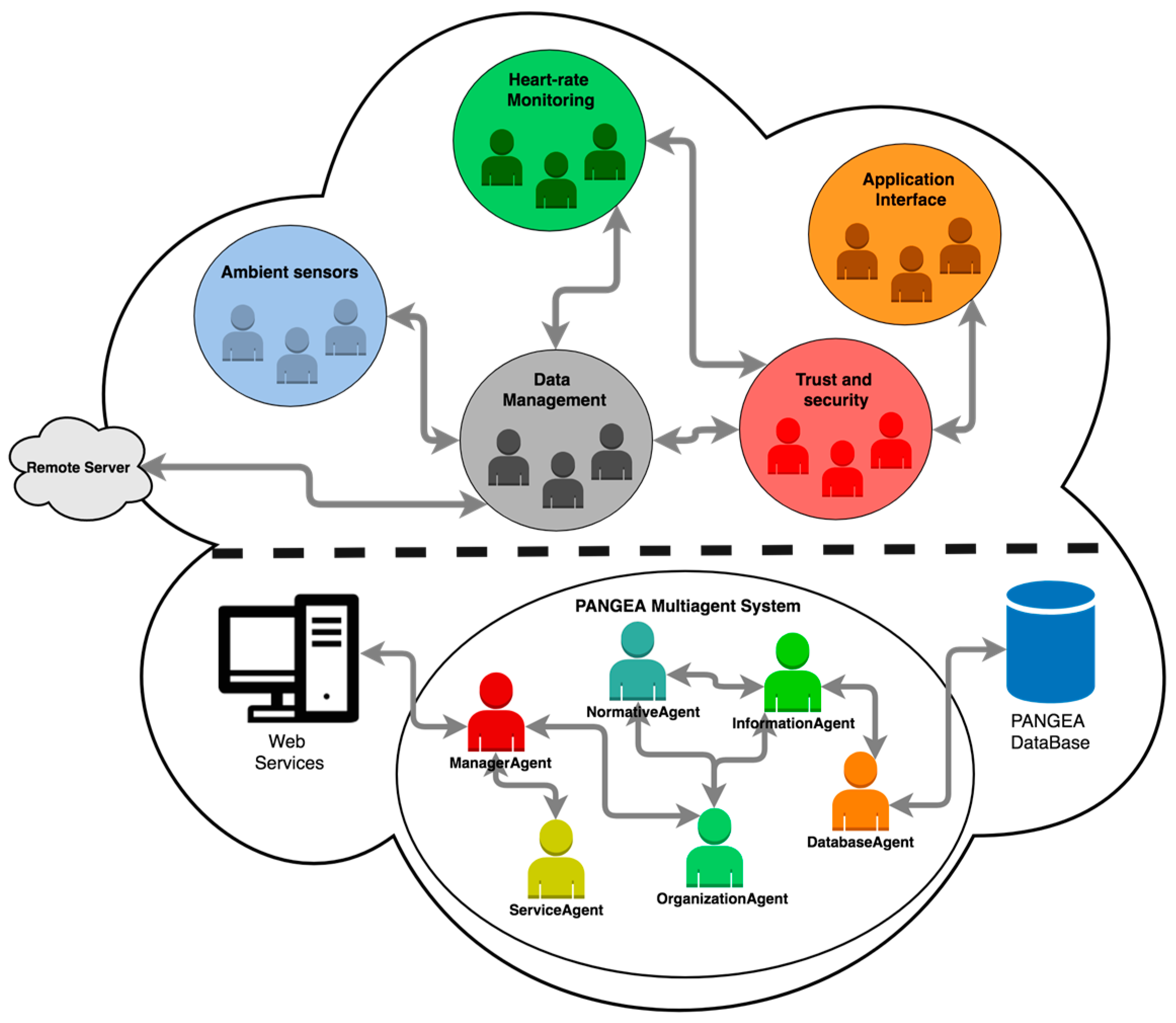
This article presents an air quality sensor system capable of monitoring the main risk factors that can trigger the Sudden Infant Death Syndrome. Thanks to the use of a context-aware framework, it is possible to generate personalized knowledge for each user, allowing for the deduction of precise rules based on the context. The aggregation of context data such as weather or air quality conditions to deployed sensorization systems allows for greater precision in the analysis. The different sensors in the system are coordinated by an Agent-based Virtual Organization, which can be deployed in each of the sensorization devices. Thanks to this coordination, the system is able to integrate a variety of sensors with different communication protocols, both wired and wireless (Bluetooth, Wi-Fi, RFID).
The proposed sensorization system is a completely non-intrusive system. Sensors are not in direct contact with the newborn, and they have no influence over its sleep. This is an important development in the monitoring of newborns, since most of the systems studied in
Section 2 use intrusive sensors that impede the infant from resting properly. In this work, not only the air quality of the environment is monitored, but also the HR of the newborn is monitored with the images captured by a web camera located in front of the cradle.
The total cost of the monitoring system is below US $150, making it a low cost system that is easy to configure. Likewise, a web data visualization system has been developed that provides parents and guardians with access to all the information that is being measured in real time, the historical data, and the assessments made by the system. Moreover, an application for mobile devices has been designed. It provides information and is a fundamental tool for warning the parents when the infant is in a dangerous situation. Thanks to this, corrective actions can be carried out quickly and directly, without producing false alarms. In other SIDS monitoring systems, however, false alarms are common.
To evaluate the proposed system, a case study was carried out in the homes of 5 different infants. As demonstrated by the data obtained in the case study, the use of a framework based on context significantly reduces the number of false positives of traditional threshold-based models. These notable results aid in establishing safer environments for newborns, reducing the current incidence of SIDS. The use of context-aware frameworks provides solidity and flexibility. This is due to the integration of different technologies and protocols in combination with data contextualization techniques in which external heterogeneous data sources are used.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}