Bowel Sounds Identification and Migrating Motor Complex Detection with Low-Cost Piezoelectric Acoustic Sensing Device

 , , , and
, , , and
Abstract
1. Introduction
2. Material and Method
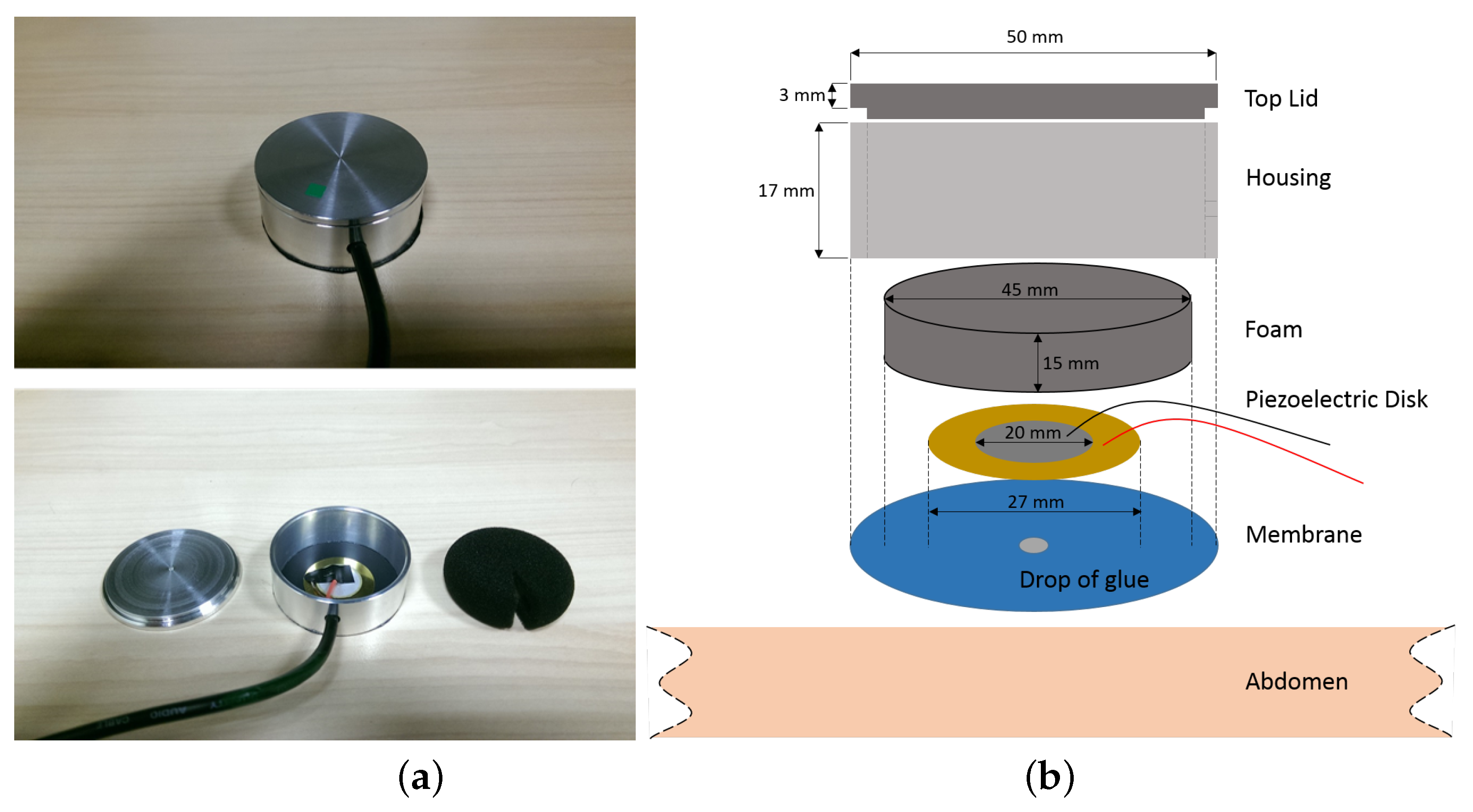
2.1. Sensor Design
2.2. Preliminary Verification
2.3. Experiment Setup
3. Result and Discussion
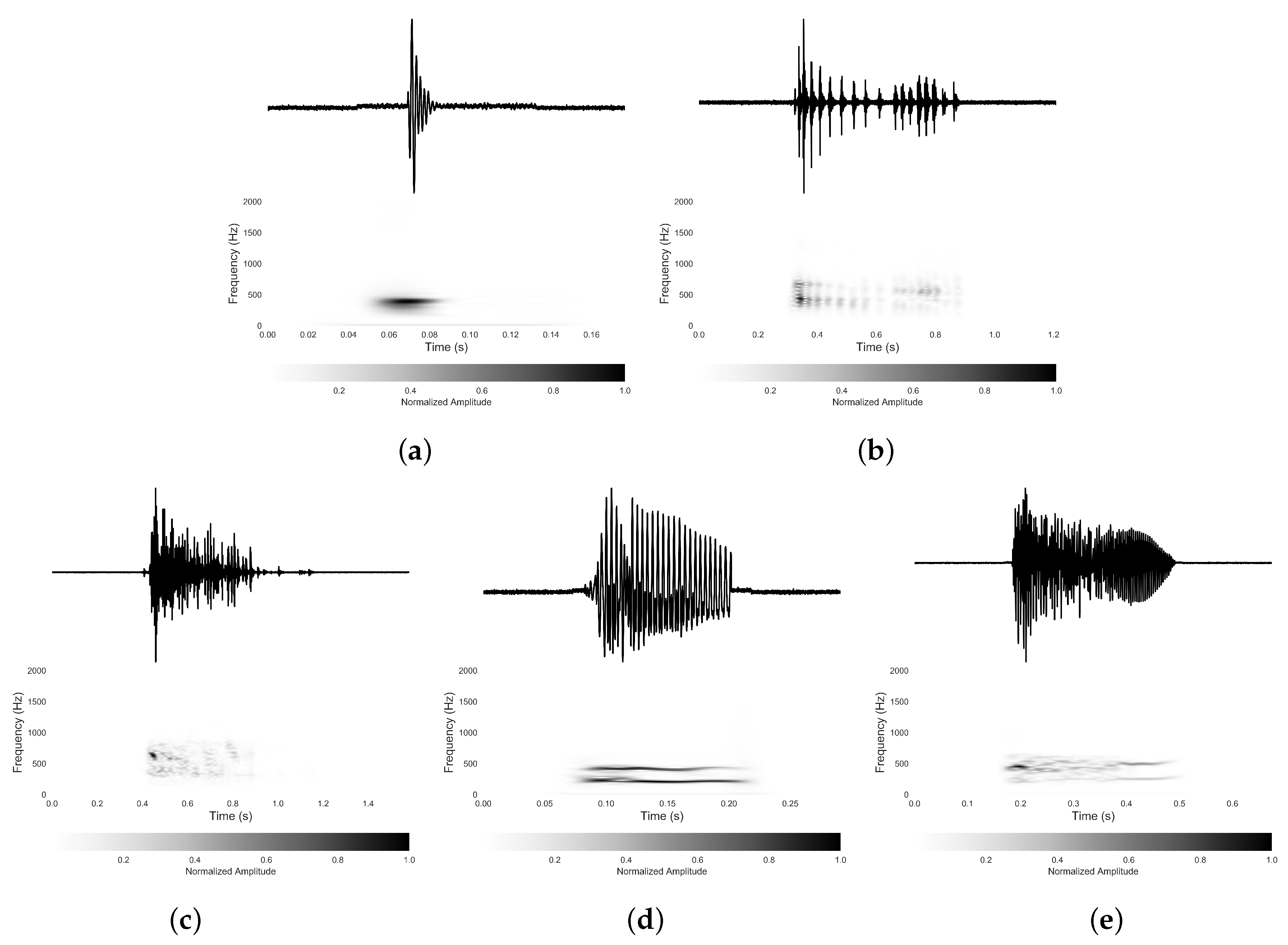
3.1. Bowel Sound Categories
3.2. Quantity and Characteristics of Different Types of Bowel Sound
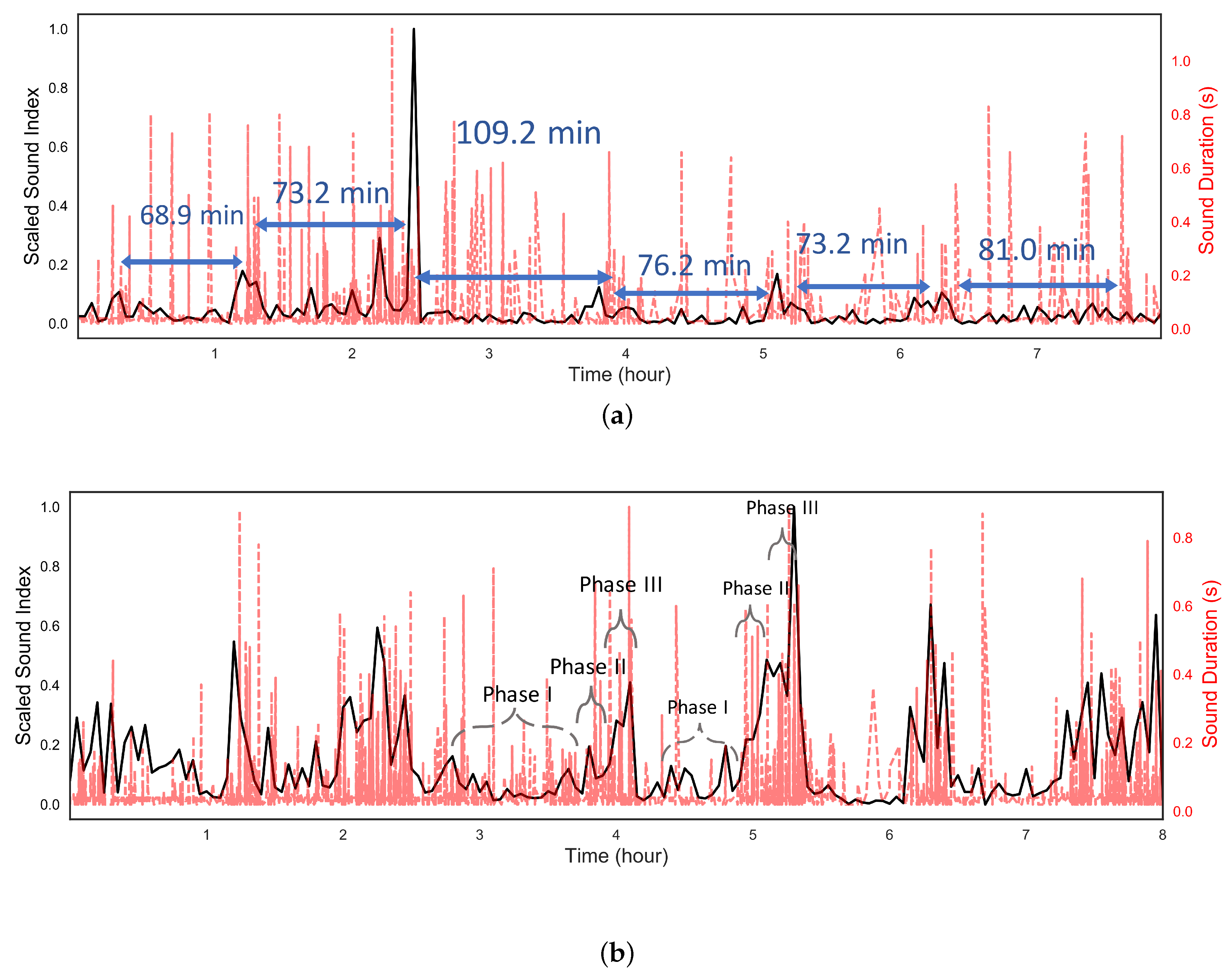
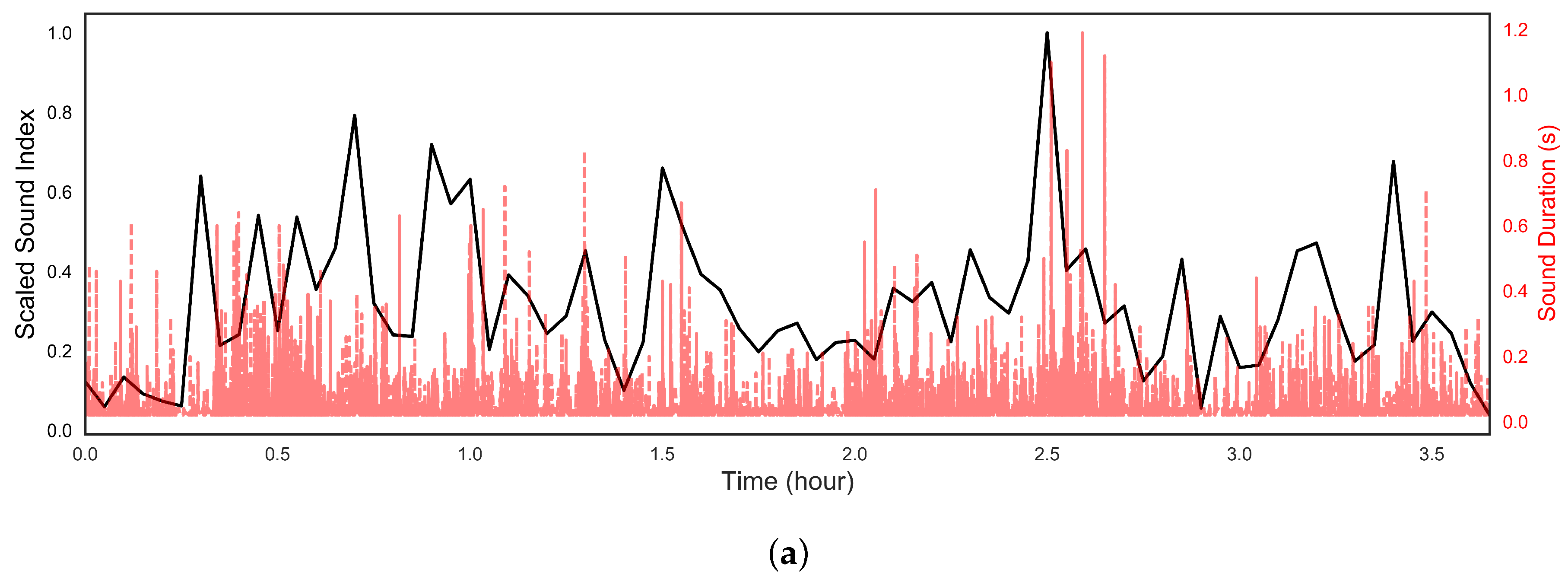
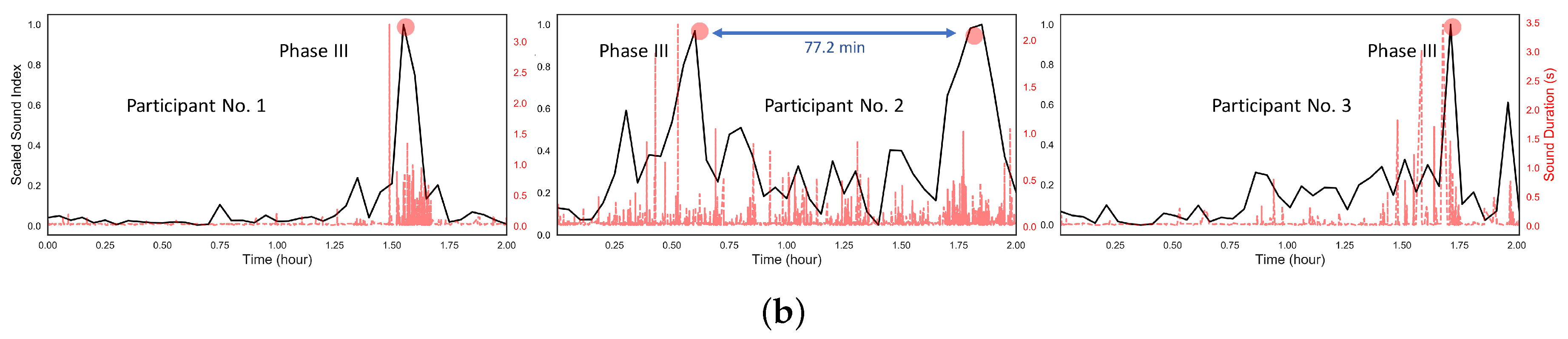
3.3. Migrating Motor Complex Detection
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BS | Bowel Sound |
| SB | Single Burst |
| MB | multiple bursts |
| CRS | Continue Random Sound |
| HS | Harmonic Sound |
| MMC | Migrating Motor Complex |
| SD | Standard Deviation |
| CV | Coefficient of Variation |
References
- Hanna, I.R.; Silverman, M.E. A history of cardiac auscultation and some of its contributors. Am. J. Cardiol. 2002, 90, 259–267. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, J.; Kim, T.; Lee, K.; Kim, S.; Bae, M. Extraction of acoustic biomarkers from PSG to detect osa. Sleep Med. 2017, 40, e160. [Google Scholar] [CrossRef]
- Kim, T.; Kim, J.W.; Lee, K. Detection of sleep disordered breathing severity using acoustic biomarker and machine learning techniques. Biomed. Eng. Online 2018, 17, 16. [Google Scholar] [CrossRef] [PubMed]
- Talley, N.J.; O’Connor, S. Clinical Examination: A Systematic Guide to Physical Diagnosis; Elsevier Health Sciences: Amsterdam, The Netherland, 2013. [Google Scholar]
- Shark, L.K.; Chen, H.; Goodacre, J. Knee acoustic emission: A potential biomarker for quantitative assessment of joint ageing and degeneration. Med. Eng. Phys. 2011, 33, 534–545. [Google Scholar] [CrossRef] [PubMed]
- Riknagel, D.; Al Humaidan, P.H.; Farlie, R.; Zimmermann, H.; Ramsing, M.; Struijk, J. Acoustic biomarker of placental pathophysiology and adverse fetal outcome. Placenta 2015, 36, A6. [Google Scholar] [CrossRef]
- Cannon, W.B. Auscultation of the rhythmic sounds produced by the stomach and intestines. Am. J. Physiol.-Leg. Content 1905, 14, 339–353. [Google Scholar] [CrossRef]
- Inderjeeth, A.J.; Webberley, K.M.; Muir, J.; Marshall, B.J. The potential of computerised analysis of bowel sounds for diagnosis of gastrointestinal conditions: A systematic review. Syst. Rev. 2018, 7, 124. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Allwood, G.; Webberley, K.M.; Inderjeeth, A.J.; Osseiran, A.; Marshall, B.J. Tu2017-Non-Invasive Diagnosis of Irritable Bowel Syndrome via Novel Bowel Sound Features: Proof of Principle. Gastroenterology 2018, 154, S1370. [Google Scholar] [CrossRef]
- Tomomasa, T.; Morikawa, A.; Sandler, R.H.; Mansy, H.A.; Koneko, H.; Masahiko, T.; Hyman, P.E.; Itoh, Z. Gastrointestinal sounds and migrating motor complex in fasted humans. Am. J. Gastroenterol. 1999, 94, 374. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T. Interdigestive migrating motor complex—Its mechanism and clinical importance. J. Smooth Muscle Res. 2013, 49, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Linden, D.R. Measurement of gastrointestinal and colonic motor functions in humans and animals. Cell. Mol. Gastroenterol. Hepatol. 2016, 2, 412–428. [Google Scholar] [CrossRef] [PubMed]
- Medhus, A.; Sandstad, O.; Bredesen, J.; Husebye, E. The migrating motor complex modulates intestinal motility response and rate of gastric emptying of caloric meals. Neurogastroenterol. Motil. 1995, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ulusar, U.D.; Canpolat, M.; Yaprak, M.; Kazanir, S.; Ogunc, G. Real-time monitoring for recovery of gastrointestinal tract motility detection after abdominal surgery. In Proceedings of the 2013 7th International Conference on Application of Information and Communication Technologies (AICT), Azerbaijan, Baku, 23–25 October 2013; pp. 1–4. [Google Scholar]
- Sakata, O.; Suzuki, Y.; Matsuda, K.; Satake, T. Temporal changes in occurrence frequency of bowel sounds both in fasting state and after eating. J. Artif. Organs 2013, 16, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Seo, J.H.; Ryu, S.H.; Kim, M.H.; Song, C.G. Estimation algorithm of the bowel motility based on regression analysis of the jitter and shimmer of bowel sounds. Comput. Methods Programs Biomed. 2011, 104, 426–434. [Google Scholar] [CrossRef]
- Spiegel, B.M.; Kaneshiro, M.; Russell, M.M.; Lin, A.; Patel, A.; Tashjian, V.C.; Zegarski, V.; Singh, D.; Cohen, S.E.; Reid, M.W.; et al. Validation of an acoustic gastrointestinal surveillance biosensor for postoperative ileus. J. Gastrointest. Surg. 2014, 18, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Kaneshiro, M.; Kaiser, W.; Pourmorady, J.; Fleshner, P.; Russell, M.; Zaghiyan, K.; Lin, A.; Martinez, B.; Patel, A.; Nguyen, A.; et al. Postoperative gastrointestinal telemetry with an acoustic biosensor predicts ileus vs. uneventful GI recovery. J. Gastrointest. Surg. 2016, 20, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Sato, R.; Emoto, T.; Gojima, Y.; Akutagawa, M. Automatic Bowel Motility Evaluation Technique for Noncontact Sound Recordings. Appl. Sci. 2018, 8, 999. [Google Scholar] [CrossRef]
- Emoto, T.; Abeyratne, U.R.; Gojima, Y.; Nanba, K.; Sogabe, M.; Okahisa, T.; Akutagawa, M.; Konaka, S.; Kinouchi, Y. Evaluation of human bowel motility using non-contact microphones. Biomed. Phys. Eng. Express 2016, 2, 045012. [Google Scholar] [CrossRef]
- Kim, K.S.; Seo, J.H.; Song, C.G. Non-invasive algorithm for bowel motility estimation using a back-propagation neural network model of bowel sounds. Biomed. Eng. Online 2011, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Ruiz, J.; Bao, C.; Roy, S. Tabla: A Proof-of-Concept Auscultatory Percussion Device for Low-Cost Pneumonia Detection. Sensors 2018, 18, 2689. [Google Scholar] [CrossRef] [PubMed]
- Farooq, M.; Sazonov, E. Automatic measurement of chew count and chewing rate during food intake. Electronics 2016, 5, 62. [Google Scholar] [CrossRef] [PubMed]
- Dimoulas, C.; Kalliris, G.; Papanikolaou, G.; Kalampakas, A. Novel wavelet domain Wiener filtering de-noising techniques: Application to bowel sounds captured by means of abdominal surface vibrations. Biomed. Signal Process. Control 2006, 1, 177–218. [Google Scholar] [CrossRef]
- Dimoulas, C.A.; Papanikolaou, G.; Petridis, V. Pattern classification and audiovisual content management techniques using hybrid expert systems: A video-assisted bioacoustics application in abdominal sounds pattern analysis. Expert Syst. Appl. 2011, 38, 13082–13093. [Google Scholar] [CrossRef]
- Watson, W.; Knox, E. Phonoenterography: The recording and analysis of bowel sounds. Gut 1967, 8, 88. [Google Scholar] [CrossRef] [PubMed]
- Dalle, D.; Devroede, G.; Thibault, R.; Perrault, J. Computer analysis of bowel sounds. Comput. Biol. Med. 1975, 4, 247–256. [Google Scholar] [CrossRef]
- Du, X.; Allwood, G.; Webberley, K.M.; Osseiran, A.; Wan, W.; Antonina, V.; Marshall, B.J. A mathematical model of bowel sound generation. J. Acoust. Soc. Am. 2018, 144, EL485–EL491. [Google Scholar]
- Ulusar, U.D. Recovery of gastrointestinal tract motility detection using Naive Bayesian and minimum statistics. Comput. Biol. Med. 2014, 51, 223–228. [Google Scholar] [CrossRef]
- Ranta, R.; Louis-Dorr, V.; Heinrich, C.; Wolf, D.; Guillemin, F. Digestive activity evaluation by multichannel abdominal sounds analysis. IEEE Trans. Biomed. Eng. 2010, 57, 1507–1519. [Google Scholar] [CrossRef]
- Allwood, G.; Du, X.; Webberley, M.; Osseiran, A.; Marshall, B. Advances in Acoustic Signal Processing Techniques for Enhanced Bowel Sound Analysis. IEEE Rev. Biomed. Eng. 2018. [Google Scholar] [CrossRef]
- Dimoulas, C.; Kalliris, G.; Papanikolaou, G.; Petridis, V.; Kalampakas, A. Bowel-sound pattern analysis using wavelets and neural networks with application to long-term, unsupervised, gastrointestinal motility monitoring. Expert Syst. Appl. 2008, 34, 26–41. [Google Scholar] [CrossRef]
- Ching, S.S.; Tan, Y.K. Spectral analysis of bowel sounds in intestinal obstruction using an electronic stethoscope. World J. Gastroenterol. 2012, 18, 4585. [Google Scholar] [CrossRef] [PubMed]
- Craine, B.L.; Silpa, M.; O’toole, C.J. Computerized auscultation applied to irritable bowel syndrome. Dig. Dis. Sci. 1999, 44, 1887–1892. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, T.; Saji, E.; Yajima, R.; Onodera, O.; Nishizawa, M. Reduced bowel sounds in Parkinson’s disease and multiple system atrophy patients. Clin. Auton. Res. 2011, 21, 181–184. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant No. | Gender | BMI | SB | MB | CRS | HS |
|---|---|---|---|---|---|---|
| 1 | female | 36.7 | ~800 (86.4%) | 82 (8.9%) | 27(2.9%) | 13 (1.3%) |
| 2 | male | 38.1 | ~900 (89.9%) | 65 (6.5%) | 28 (2.8%) | 6 (0.6%) |
| 3 | female | 29.4 | ~3900 (96.8%) | 74 (1.8%) | 44 (1.1%) | 4 (0.01%) |
| 4 | female | 21.9 | ~2200 (84.1%) | 354 (9.4%) | 141 (5.4%) | 11 (0.4%) |
| 5 | male | 19.1 | ~1400 (76.7%) | 245 (13.4%) | 142 (7.8%) | 23 (1.3%) |
| 6 | female | 37.6 | ~2000 (88.0%) | 151 (6.6%) | 98 (4.3%) | 13 (0.6%) |
| 7 | male | 26.0 | ~3900 (89.5%) | 208 (4.8%) | 153 (3.5%) | 77 (1.7%) |
| 8 | female | 27.6 | ~250 (93.6%) | 11 (4.1%) | 4 (1.5%) | 2 (0.7%) |
| 9 | female | 22.8 | ~3900 (82.6%) | 590 (12.5%) | 149 (3.2%) | 47 (1.0%) |
| 10 | female | 28.4 | ~4500 (89.3%) | 457 (9.1%) | 50 (1.0%) | 18 (0.4%) |
| Mean | 28.8 | 2375.0 (87.8%) | 223.7 (7.8%) | 83.6 (3.5%) | 21.4 (0.9%) | |
| SD 1 | 6.4 | 1476.0 (5.4%) | 180.1 (3.5%) | 56.0(2.0%) | 22.2 (0.5%) | |
| CV 2 | 0.22 | 0.62 (0.06) | 0.80 (0.45) | 0.67 (0.57) | 1.04 (0.56) |
| Type | Duration (ms) 25–75% | Spectral Bandwidth (Hz) 25–75% | Spectral Flatness 25–75% | Mean-Crossing Ratio 25–75% |
|---|---|---|---|---|
| SB | 26–42 | 283.7–710.9 | 0.1207–0.2585 | 0.3221–0.4059 |
| MB | 56–445.8 | 358.5–995.8 | 0.1647–0.3477 | 0.3681–0.4411 |
| CRS | 215–674 | 151.5–419.7 | 0.06818–0.2007 | 0.2096–0.3867 |
| HS | 124–385 | 145.6–438.1 | 0.07096–0.2272 | 0.1211–0.3493 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, X.; Allwood, G.; Webberley, K.M.; Osseiran, A.; Marshall, B.J. Bowel Sounds Identification and Migrating Motor Complex Detection with Low-Cost Piezoelectric Acoustic Sensing Device. Sensors 2018, 18, 4240. https://doi.org/10.3390/s18124240
Du X, Allwood G, Webberley KM, Osseiran A, Marshall BJ. Bowel Sounds Identification and Migrating Motor Complex Detection with Low-Cost Piezoelectric Acoustic Sensing Device. Sensors. 2018; 18(12):4240. https://doi.org/10.3390/s18124240
Chicago/Turabian StyleDu, Xuhao, Gary Allwood, Katherine Mary Webberley, Adam Osseiran, and Barry J. Marshall. 2018. "Bowel Sounds Identification and Migrating Motor Complex Detection with Low-Cost Piezoelectric Acoustic Sensing Device" Sensors 18, no. 12: 4240. https://doi.org/10.3390/s18124240
APA StyleDu, X., Allwood, G., Webberley, K. M., Osseiran, A., & Marshall, B. J. (2018). Bowel Sounds Identification and Migrating Motor Complex Detection with Low-Cost Piezoelectric Acoustic Sensing Device. Sensors, 18(12), 4240. https://doi.org/10.3390/s18124240