
Unobtrusive Estimation of Cardiac Contractility and Stroke Volume Changes Using Ballistocardiogram Measurements on a High Bandwidth Force Plate

Abstract
:1. Introduction
2. Methods and Materials
2.1. Protocol
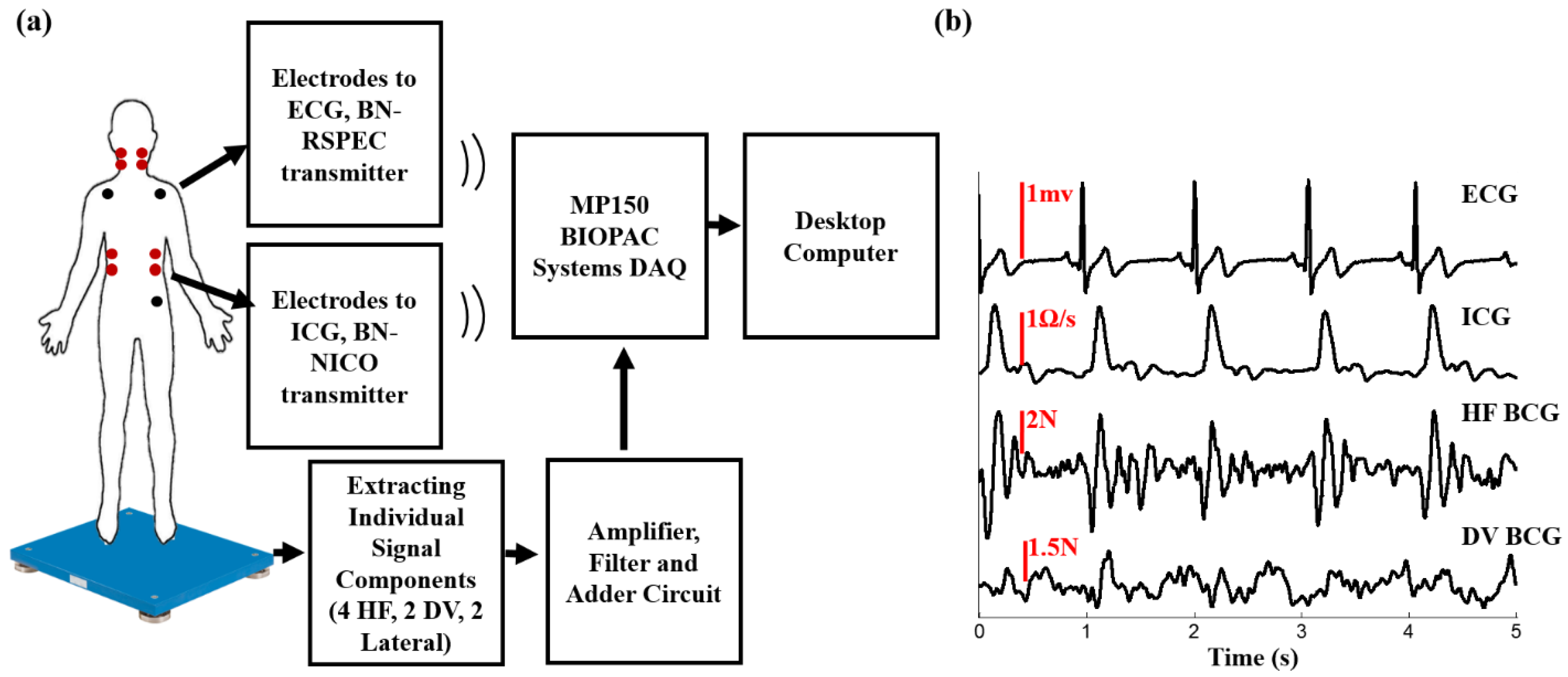
2.2. Hardware Design
2.3. Data Processing
2.4. Feature Extraction and Statistical Analysis
2.4.1. Correlation at Rest
2.4.2. Correlation during Exercise Recovery
2.5. Estimating Relative Changes in Stroke Volume
2.6. Signal-to-Noise Ratio Calculations
3. Results and Discussion
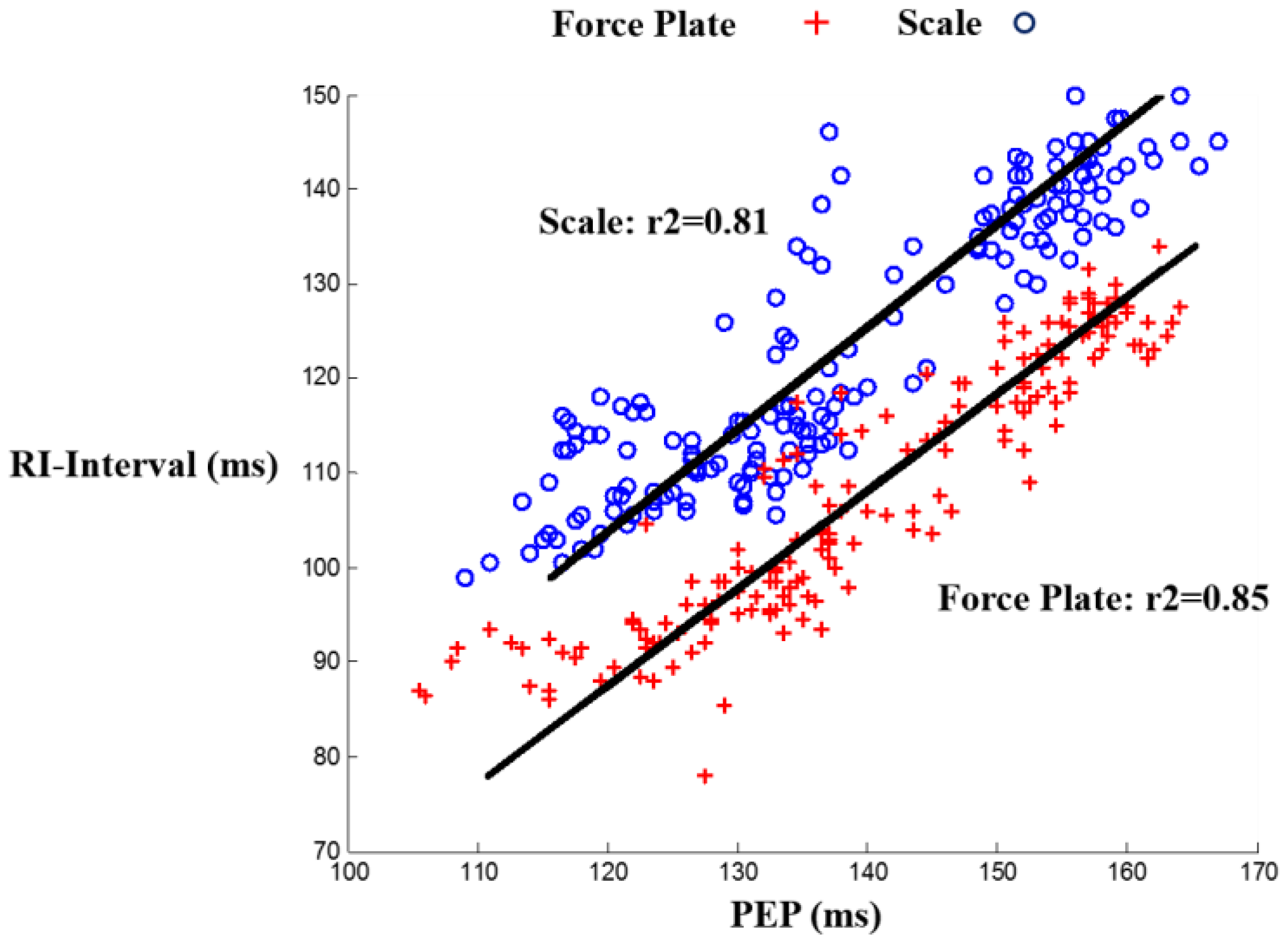
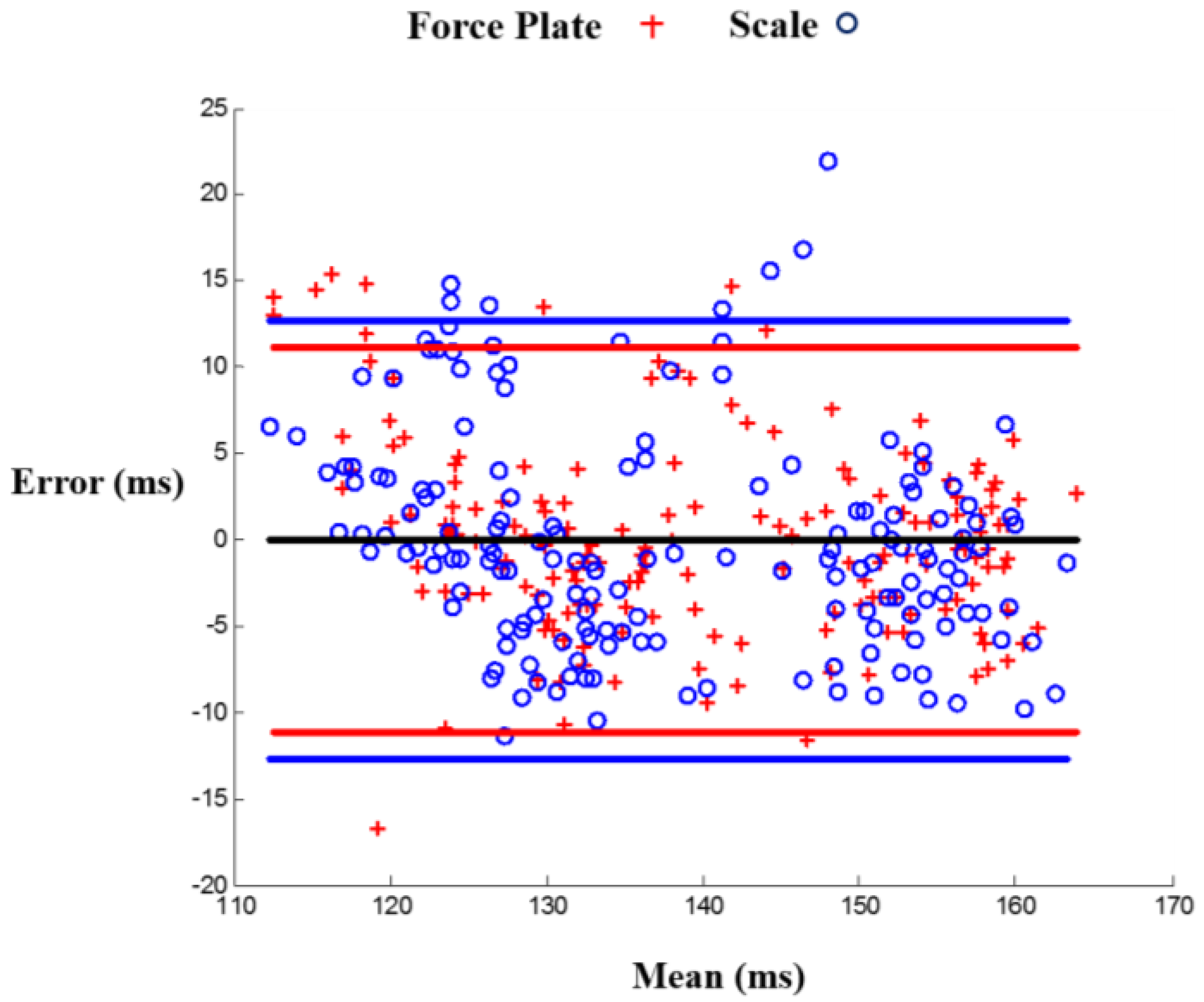
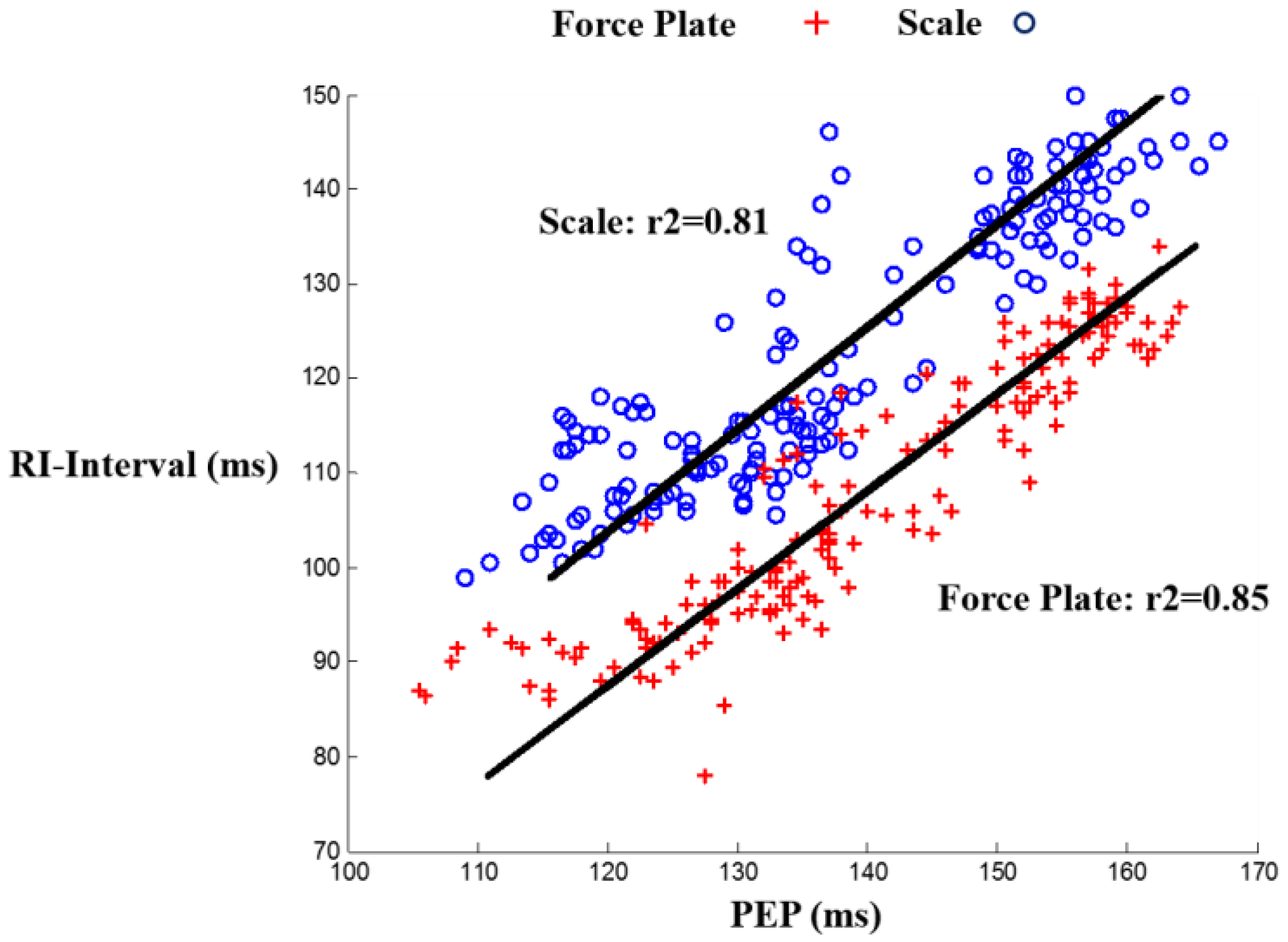
3.1. RI and PEP Correlation for Scale and Force Plate BCG during Rest
3.2. RI and PEP Correlation for Head-to-Foot Force Plate BCG during Recovery
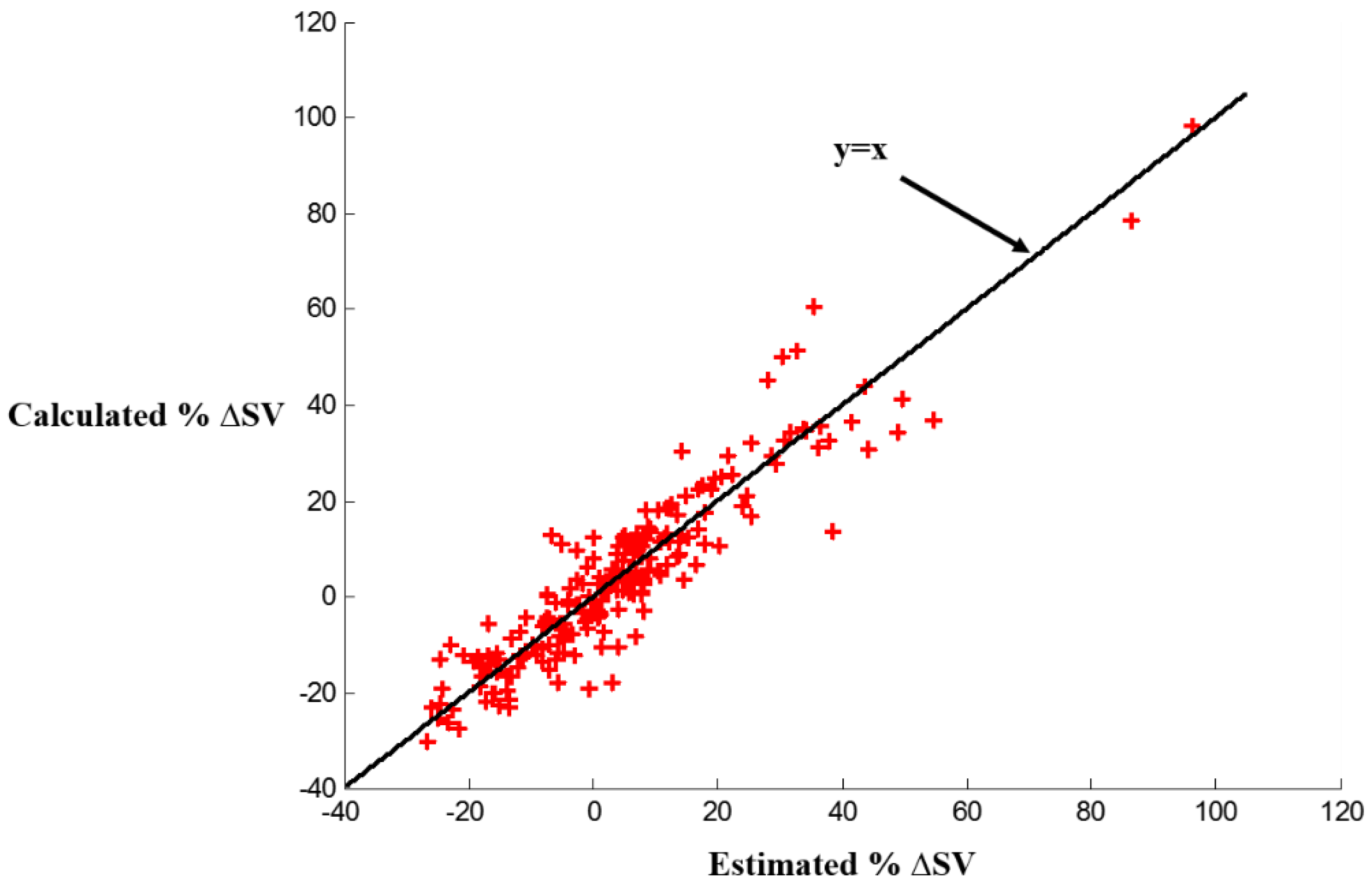
3.3. Stroke Volume Estimation from Head-to-Foot Force Plate BCG during Recovery
3.4. Signal-to-Noise Ratio Comparison for Scale BCG and Force Plate Head-to-Foot BCG
3.5. Limitations
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.M. Physiology of the Heart, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Heidenreich, P.A.; Trogdon, J.G.; Khavjou, O.A.; Butler, J.; Dracup, K.; Ezekowitz, M.D.; Finkelstein, E.A.; Hong, Y.; Johnston, S.C.; Khera, A.; et al. Forecasting the future of cardiovascular disease in the United States: A policy statement from the American Heart Association. Circulation 2011, 123, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.B.; Magalski, A.; Braunschweig, F.; Böhm, M.; Reynolds, D.; Steinhaus, D.; Luby, A.; Linde, C.; Ryden, L.; Cremers, B.; et al. Ongoing right ventricular hemodynamics in heart failureclinical value of measurements derived from an implantable monitoring system. J. Am. Coll. Cardiol. 2003, 41, 565–571. [Google Scholar] [CrossRef]
- Paré, G.; Jaana, M.; Sicotte, C. Systematic Review of Home Telemonitoring for Chronic Diseases: The Evidence Base. J. Am. Med. Inform. Assoc. 2007, 14, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Bui, A.L.; Fonarow, G.C. Home Monitoring for Heart Failure Management. J. Am. Coll. Cardiol. 2012, 59, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Nutting, P.A.; Crabtree, B.F.; Miller, W.L.; Stange, K.C.; Stewart, E.; Jaén, C. Transforming Physician Practices to Patient-Centered Medical Homes: Lessons from the National Demonstration Project. Health Aff. 2011, 30, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Martínez, A.; Everss, E.; Rojo-Alvarez, J.L.; Figal, D.P.; García-Alberola, A. A systematic review of the literature on home monitoring for patients with heart failure. J. Telemed. Telecare 2006, 12, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Javaid, A.Q.; Wiens, A.D.; Fesmire, N.F.; Weitnauer, M.A.; Inan, O.T. Quantifying and Reducing Posture-Dependent Distortion in Ballistocardiogram Measurements. IEEE J. Biomed. Health Inform. 2015, 19, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Talley, R.C.; Meyer, J.F.; McNay, J.L. Evaluation of the pre-ejection period as an estimate of myocardial contractility in dogs. Am. J. Cardiol. 1971, 27, 384–391. [Google Scholar] [CrossRef]
- Klabunde, R.E. Cardiovascular Physiology, 2nd ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2012. [Google Scholar]
- Ermishkin, V.V.; Lukoshkova, E.V.; Saidova, M.A.; Shitov, V.N.; Vinogradova, O.L.; Khayutin, V.M. Beat-by-Beat Changes in Pre-Ejection Period during Functional Tests Evaluated by Impedance Aortography: A Step to a Left Ventricular Contractility Monitoring; Springer Berlin Heidelberg: Graz, Austria, 2007; pp. 655–658. [Google Scholar]
- Etemadi, M.; Inan, O.T.; Giovangrandi, L.; Kovacs, G.T. Rapid assessment of cardiac contractility on a home bathroom scale. IEEE Trans. Inform. Technol. Biomed. 2011, 15, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Inan, O.T.; Migeotte, P.F.; Kwang-Suk, P.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef] [PubMed]
- Starr, I.; Rawson, A.; Schroeder, H.; Joseph, N. Studies on the estimation of cardiac ouptut in man, and of abnormalities in cardiac function, from the heart’s recoil and the blood’s impacts; The ballistocardiogram. Am. J. Physiol. Legacy Content 1939, 127, 1–28. [Google Scholar]
- Inan, O.T.; Etemadi, M.; Wiard, R.; Giovangrandi, L.; Kovacs, G.T.A. Robust ballistocardiogram acquisition for home monitoring. Physiol. Meas. 2009, 30, 169. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.P.; Rittogers, S.E.; Froester, W.F.; Boudoulas, H. A critical review of the systolic time intervals. Circulation 1977, 56, 146–158. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, A.; Allen, M.T.; Fahrenberg, J.; Kelsey, R.M.; Lovallo, W.R.; van Doornen, L.J.P. Methodological Guidelines for Impedance Cardiography. Psychophysiology 1990, 27, 1–23. [Google Scholar] [PubMed]
- Cybulski, G. Ambulatory Impedance Cardiography: The Systems and Their Applications (Lecture Notes in Electrical Engineering); Springer: Berlin, Germany, 2011. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Arai, T.; Lee, K.; Cohen, R.J. Cardiac output and stroke volume estimation using a hybrid of three windkessel models. In Proceedings of the IEEE 32nd Annual International Conference of Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 1–4 September 2010; pp. 4971–4974.
- Rabbi, A.F.; Gagarin, R.; Huang, G.C.; Iskander, M.F. Stroke volume estimation from the new noninvasive cardiopulmonary stethoscope. In Proceedings of the 2014 IEEE Antennas and Propagation Society International Symposium (APSURSI), Memphis, TN, USA, 6–12 July 2014; pp. 967–968.
- Schmidt, C. Comparison of electrical velocimetry and transoesophageal Doppler echocardiography for measuring stroke volume and cardiac output. Br. J. Anaesth. 2005, 95, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Chatti, R.; de Rudniki, S.; Marque, S.; Dumenil, A.; Descorps-Declere, A.; Cariou, A.; Duranteau, J.; Aout, M.; Vicaut, E.; Cholley, B. Comparison of two versions of the Vigileo-FloTracTM system (1.03 and 1.07) for stroke volume estimation: A multicentre, blinded comparison with oesophageal Doppler measurements. Br. J. Anaesth. 2009, 102, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Critchley, L.A.; Critchley, J.A. A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J. Clin. Monit. Comput. 1999, 15, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Stroffregen, T.A.; Yoshida, K.; Villard, S.; Scibora, L.; Bardy, B. Stance width influences postural stability and motion sickness. J. Ecol. Physiol. 2010, 22, 169–191. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | µ Error (mL) | σ Error (mL) | % µ Error | % σ Error |
|---|---|---|---|---|
| 1 | 2.0 | 1.7 | 3.6 | 3.1 |
| 2 | 1.4 | 0.9 | 3.4 | 2.3 |
| 3 | 3.7 | 2.6 | 6.5 | 4.6 |
| 4 | 4.0 | 4.9 | 5.4 | 6.7 |
| 5 | 2.5 | 1.8 | 6.4 | 4.7 |
| 6 | 2.8 | 2.0 | 8.9 | 6.4 |
| 7 | 3.4 | 3.1 | 6.6 | 6.0 |
| 8 | 2.8 | 2.6 | 4.6 | 4.3 |
| 9 | 5.6 | 4.9 | 11.0 | 9.5 |
| 10 | 3.4 | 2.5 | 4.5 | 3.4 |
| 11 | 3.1 | 3.0 | 5.3 | 5.1 |
| 12 | 3.3 | 1.4 | 5.2 | 2.1 |
| 13 | 1.6 | 1.3 | 3.3 | 2.8 |
| 14 | 1.9 | 1.4 | 4.6 | 3.3 |
| 15 | 1.0 | 0.8 | 2.2 | 1.8 |
| 16 | 3.4 | 1.8 | 4.7 | 2.5 |
| 17 | 3.5 | 2.5 | 4.6 | 3.2 |
| Average | 2.9 | 2.3 | 5.3 | 4.2 |
| Subject | Gender | Height (cm) | Weight (kg) | FP SNR (dB) | Scale SNR (dB) |
|---|---|---|---|---|---|
| 1 | Female | 160 | 59 | 6.0 | 5.6 |
| 2 | Male | 175 | 75 | 8.6 | 7.6 |
| 3 | Female | 168 | 68 | 8.1 | 5.3 |
| 4 | Female | 160 | 52 | 1.7 | 1.3 |
| 5 | Male | 183 | 86 | 8.3 | 4.3 |
| 6 | Male | 175 | 74 | 1.5 | -1.8 |
| 7 | Female | 152 | 49 | 5.5 | 4.6 |
| 8 | Male | 178 | 65 | 3.4 | 1.7 |
| 9 | Male | 178 | 88 | 1.6 | 1.5 |
| 10 | Male | 178 | 68 | 2.6 | 1.2 |
| 11 | Male | 190 | 88 | 7.1 | 5.1 |
| 12 | Female | 175 | 68 | 9.0 | 8.1 |
| 13 | Male | 175 | 70 | 3.8 | 3.8 |
| 14 | Male | 185 | 76 | 8.3 | 8.3 |
| 15 | Male | 175 | 79 | 3.1 | 2.7 |
| 16 | Female | 163 | 75 | 6.7 | 6.6 |
| 17 | Female | 168 | 61 | 8.0 | 7.8 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashouri, H.; Orlandic, L.; Inan, O.T. Unobtrusive Estimation of Cardiac Contractility and Stroke Volume Changes Using Ballistocardiogram Measurements on a High Bandwidth Force Plate. Sensors 2016, 16, 787. https://doi.org/10.3390/s16060787
Ashouri H, Orlandic L, Inan OT. Unobtrusive Estimation of Cardiac Contractility and Stroke Volume Changes Using Ballistocardiogram Measurements on a High Bandwidth Force Plate. Sensors. 2016; 16(6):787. https://doi.org/10.3390/s16060787
Chicago/Turabian StyleAshouri, Hazar, Lara Orlandic, and Omer T. Inan. 2016. "Unobtrusive Estimation of Cardiac Contractility and Stroke Volume Changes Using Ballistocardiogram Measurements on a High Bandwidth Force Plate" Sensors 16, no. 6: 787. https://doi.org/10.3390/s16060787