
Neurologic Biomarkers, Neuroimaging, and Cognitive Function in Persistent Atrial Fibrillation: A Cross-Sectional Study
 , , ,
, , ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
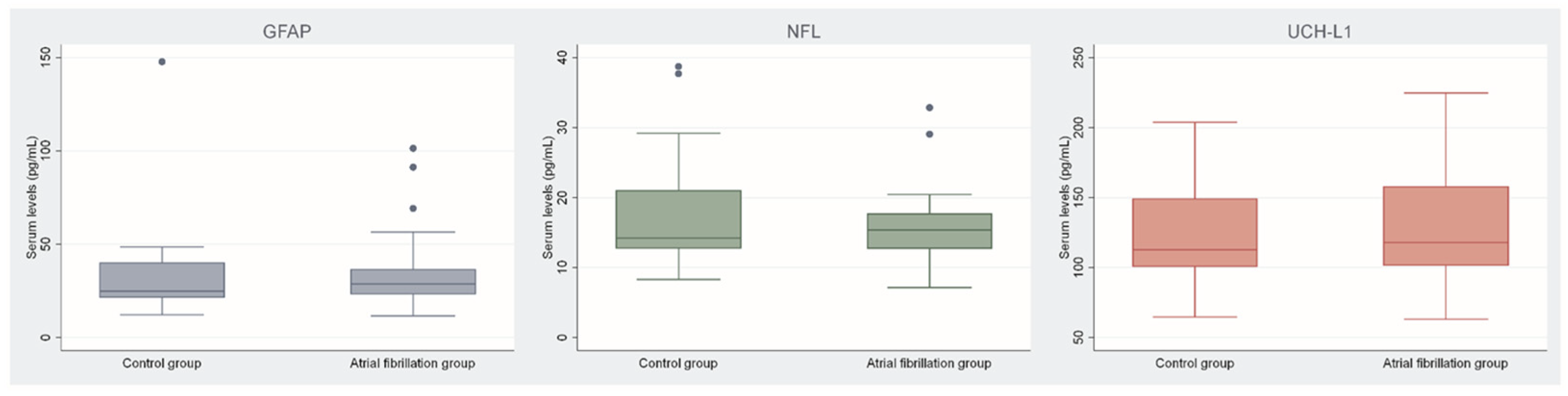
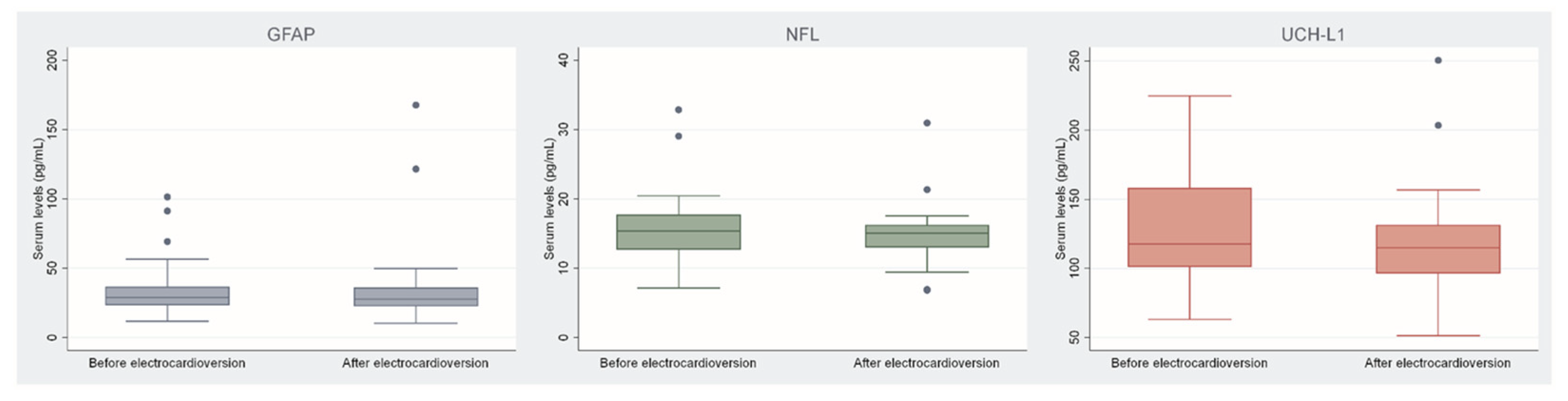
2.1. Specific Neurologic Biomarkers
2.2. Neuroimaging with Magnetic Resonance
2.3. Cognitive Function Assessment
2.4. Correlation Analysis
3. Discussion
4. Materials and Methods
4.1. Ethical Considerations and Informed Consent
4.2. Study Design and Patients
4.3. Outcomes
4.4. Laboratory Analysis and Specific Neurologic Biomarkers
4.5. Neuroimaging by Magnetic Resonance
4.6. Cognitive Assessment
4.7. Clinical Assessment
4.8. Statistical Methods
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.-H.; McAnulty, J.H.; Zheng, Z.-J.; et al. Worldwide Epidemiology of Atrial Fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Rivard, L.; Khairy, P. Mechanisms, Clinical Significance, and Prevention of Cognitive Impairment in Patients with Atrial Fibrillation. Can. J. Cardiol. 2017, 33, 1556–1564. [Google Scholar] [CrossRef]
- Aryal, R.; Patabendige, A. Blood–Brain Barrier Disruption in Atrial Fibrillation: A Potential Contributor to the Increased Risk of Dementia and Worsening of Stroke Outcomes? Open Biol. 2021, 11, 200396. [Google Scholar] [CrossRef]
- Manolis, T.A.; Manolis, A.A.; Apostolopoulos, E.J.; Melita, H.; Manolis, A.S. Atrial Fibrillation and Cognitive Impairment: An Associated Burden or Burden by Association? Angiology 2020, 71, 498–519. [Google Scholar] [CrossRef]
- Rydén, L.; Sacuiu, S.; Wetterberg, H.; Najar, J.; Guo, X.; Kern, S.; Zettergren, A.; Shams, S.; Pereira, J.B.; Wahlund, L.-O.; et al. Atrial Fibrillation, Stroke, and Silent Cerebrovascular Disease: A Population-Based MRI Study. Neurology 2021, 97, e1608–e1619. [Google Scholar] [CrossRef]
- Conen, D.; Rodondi, N.; Müller, A.; Beer, J.H.; Ammann, P.; Moschovitis, G.; Auricchio, A.; Hayoz, D.; Kobza, R.; Shah, D.; et al. Relationships of Overt and Silent Brain Lesions with Cognitive Function in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 73, 989–999. [Google Scholar] [CrossRef]
- Galenko, O.; Jacobs, V.; Knight, S.; Bride, D.; Cutler, M.J.; Muhlestein, J.B.; Carlquist, J.L.; Anderson, J.L.; Knowlton, K.U.; Jared Bunch, T. Circulating Levels of Biomarkers of Cerebral Injury in Patients with Atrial Fibrillation. Am. J. Cardiol. 2019, 124, 1697–1700. [Google Scholar] [CrossRef]
- Polymeris, A.A.; Coslovksy, M.; Aeschbacher, S.; Sinnecker, T.; Benkert, P.; Kobza, R.; Beer, J.; Rodondi, N.; Fischer, U.; Moschovitis, G.; et al. Serum Neurofilament Light in Atrial Fibrillation: Clinical, Neuroimaging and Cognitive Correlates. Brain Commun. 2020, 2, fcaa166. [Google Scholar] [CrossRef]
- Sjölin, K.; Aulin, J.; Wallentin, L.; Eriksson, N.; Held, C.; Kultima, K.; Oldgren, J.; Burman, J. Serum Neurofilament Light Chain in Patients with Atrial Fibrillation. J. Am. Heart Assoc. 2022, 11, e025910. [Google Scholar] [CrossRef]
- Matuszczak, E.; Tylicka, M.; Komarowska, M.D.; Debek, W.; Hermanowicz, A. Ubiquitin Carboxy-terminal Hydrolase L1–Physiology and Pathology. Cell Biochem. Funct. 2020, 38, 533–540. [Google Scholar] [CrossRef]
- Polymeris, A.A.; Helfenstein, F.; Benkert, P.; Aeschbacher, S.; Leppert, D.; Coslovsky, M.; Willemse, E.; Schaedelin, S.; Blum, M.R.; Rodondi, N.; et al. Renal Function and Body Mass Index Contribute to Serum Neurofilament Light Chain Levels in Elderly Patients with Atrial Fibrillation. Front. Neurosci. 2022, 16, 819010. [Google Scholar] [CrossRef]
- Berman, J.P.; Norby, F.L.; Mosley, T.; Soliman, E.Z.; Gottesman, R.F.; Lutsey, P.L.; Alonso, A.; Chen, L.Y. Atrial Fibrillation and Brain Magnetic Resonance Imaging Abnormalities: The ARIC Study. Stroke 2019, 50, 783–788. [Google Scholar] [CrossRef]
- Shao, I.Y.; Power, M.C.; Mosley, T.; Jack, C.; Gottesman, R.F.; Chen, L.Y.; Norby, F.L.; Soliman, E.Z.; Alonso, A. Association of Atrial Fibrillation with White Matter Disease: The ARIC Study. Stroke 2019, 50, 989–991. [Google Scholar] [CrossRef]
- Kobayashi, A.; Iguchi, M.; Shimizu, S.; Uchiyama, S. Silent Cerebral Infarcts and Cerebral White Matter Lesions in Patients with Nonvalvular Atrial Fibrillation. J. Stroke Cerebrovasc. Dis. 2012, 21, 310–317. [Google Scholar] [CrossRef]
- Papanastasiou, C.A.; Theochari, C.A.; Zareifopoulos, N.; Arfaras-Melainis, A.; Giannakoulas, G.; Karamitsos, T.D.; Palaiodimos, L.; Ntaios, G.; Avgerinos, K.I.; Kapogiannis, D.; et al. Atrial Fibrillation Is Associated with Cognitive Impairment, All-Cause Dementia, Vascular Dementia, and Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J. Gen. Intern. Med. 2021, 36, 3122–3135. [Google Scholar] [CrossRef]
- Sepehri Shamloo, A.; Dagres, N.; Müssigbrodt, A.; Stauber, A.; Kircher, S.; Richter, S.; Dinov, B.; Bertagnolli, L.; Husser-Bollmann, D.; Bollmann, A.; et al. Atrial Fibrillation and Cognitive Impairment: New Insights and Future Directions. Heart Lung Circ. 2020, 29, 69–85. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, K.K.W. Glial Fibrillary Acidic Protein: From Intermediate Filament Assembly and Gliosis to Neurobiomarker. Trends Neurosci. 2015, 38, 364–374. [Google Scholar] [CrossRef]
- Rozanski, M.; Waldschmidt, C.; Kunz, A.; Grittner, U.; Ebinger, M.; Wendt, M.; Winter, B.; Bollweg, K.; Villringer, K.; Fiebach, J.B.; et al. Glial Fibrillary Acidic Protein for Prehospital Diagnosis of Intracerebral Hemorrhage. Cerebrovasc. Dis. 2017, 43, 76–81. [Google Scholar] [CrossRef]
- Shemilt, M.; Boutin, A.; Lauzier, F.; Zarychanski, R.; Moore, L.; McIntyre, L.A.; Nadeau, L.; Fergusson, D.A.; Mercier, E.; Archambault, P.; et al. Prognostic Value of Glial Fibrillary Acidic Protein in Patients with Moderate and Severe Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Crit. Care Med. 2019, 47, e522–e529. [Google Scholar] [CrossRef] [PubMed]
- Thelin, E.P.; Zeiler, F.A.; Ercole, A.; Mondello, S.; Büki, A.; Bellander, B.-M.; Helmy, A.; Menon, D.K.; Nelson, D.W. Serial Sampling of Serum Protein Biomarkers for Monitoring Human Traumatic Brain Injury Dynamics: A Systematic Review. Front. Neurol. 2017, 8, 300. [Google Scholar] [CrossRef]
- Singh, G.P.; Nigam, R.; Tomar, G.S.; Monisha, M.; Bhoi, S.K.; Arulselvi, S.; Sengar, K.; Akula, D.; Panta, P.; Anindya, R. Early and Rapid Detection of UCHL1 in the Serum of Brain-Trauma Patients: A Novel Gold Nanoparticle-Based Method for Diagnosing the Severity of Brain Injury. Analyst 2018, 143, 3366–3373. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, S.; Sechi, E.; Ferrari, S. Serum Neurofilament Light Chain Studies in Neurological Disorders, Hints for Interpretation. J. Neurol. Sci. 2020, 416, 116986. [Google Scholar] [CrossRef]
- Bittner, S.; Oh, J.; Havrdová, E.K.; Tintoré, M.; Zipp, F. The Potential of Serum Neurofilament as Biomarker for Multiple Sclerosis. Brain 2021, 144, 2954–2963. [Google Scholar] [CrossRef]
- Fazekas, F.; Chawluk, J.; Alavi, A.; Hurtig, H.; Zimmerman, R. MR Signal Abnormalities at 1.5 T in Alzheimer’s Dementia and Normal Aging. Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef]
- Iverson, G.L.; Marsh, J.M.; Connors, E.J.; Terry, D.P. Normative Reference Values, Reliability, and Item-Level Symptom Endorsement for the PROMIS® v2.0 Cognitive Function-Short Forms 4a, 6a and 8a. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2021, 36, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.G.M.; Lip, G.Y.H. A Novel User-Friendly Score (HAS-BLED) To Assess 1-Year Risk of Major Bleeding in Patients with Atrial Fibrillation. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Control Group (n = 16; 39.0%) | Atrial Fibrillation Group (n = 25; 61.0%) | p-Value |
|---|---|---|---|
| Age (years) | 67 (63, 69) | 68 (63, 72) | 0.768 * |
| Female sex | 6 (37.5%) | 9 (36.0%) | 0.923 * |
| Body mass index (kg/m2) | 28 (26, 31) | 29 (26, 31) | 0.490 † |
| Systolic blood pressure (mmHg) | 132 (122, 152) | 137 (129, 144) | 0.769 † |
| Diastolic blood pressure (mmHg) | 78 (74, 88) | 80 (73, 82) | 0.928 † |
| Mean blood pressure (mmHg) | 95 (93, 109) | 100 (91, 102) | 0.916 † |
| Heart rate (/min) | 68 (58, 73) | 90 (78, 96) | <0.001 † |
| CHA2DS2VASc risk score | 2 (1, 3) | 2 (2, 3) | 0.506 † |
| HAS-BLED risk score | 1 (0, 1) | 1 (0, 1) | 0.965 † |
| Laboratory parameters | |||
| Total cholesterol (mmol/L) | 5.5 (4.7, 6.2) | 5.5 (4.1, 5.8) | 0.228 † |
| LDL cholesterol (mmol/L) | 3.4 (2.5, 3.7) | 3.3 (2.3, 3.8) | 0.591 † |
| Creatinine (µmol/L) | 79.0 (75.0, 87.0) | 83.5 (74.8, 101.8) | 0.271 † |
| eGFR (ml/min/1.73 m2) | 80.0 (67.0, 87.0) | 67.5 (52.0, 90.3) | 0.500 † |
| Hematocrite (%) | 0.42 (0.41, 0.43) | 0.43 (0.39, 0.46) | 0.702 † |
| Hemoglobin (g/L) | 142.0 (141.0, 155.0) | 142.5 (131.3, 154.8) | 0.344 † |
| NT-proBNP (pg/mL) | 85.0 (53.0, 157.0) | 895.0 (678.0, 1430.8) | <0.001 † |
| hsTnT (ng/mL) | 11.6 (9.3, 14.4) | 10.2 (6.8, 12.3) | 0.109 † |
| Glucose (mmol/L) | 5.5 (5.3, 7.6) | 5.9 (5.2, 6.8) | 0.295 † |
| Albumine (g/L) | 43.3 (41.3, 46.8) | 44.2 (42.1, 47.0) | 0.682 † |
| vWF | 1.3 (1.1, 1.7) | 1.7 (1.4, 1.7) | 0.038 † |
| Comorbidities | |||
| Arterial hypertension | 12 (75.0%) | 18 (72.0%) | 0.833 * |
| Diabetes mellitus | 3 (18.8%) | 4 (16.0%) | 0.819 * |
| Chronic kidney disease | 0 (0.0%) | (0.0%) | / |
| Smoking: | 0.127 * | ||
| Active smoking | 4 (25.0%) | 7 (28.0%) | |
| Prior smoking | 7 (43.8%) | 4 (16.0%) | |
| Medications | |||
| Beta blockers | 3 (18.8%) | 22 (88.0%) | <0.001 * |
| Statins | 4 (25.0%) | 7 (28.0%) | 0.833 * |
| ASA | 4 (25.0%) | / | / |
| Use of anticoagulation: | <0.001 * | ||
| Warfarin | 0 (0.0%) | 3 (12.0%) | |
| DOAC | 1 (6.3%) | 22 (88.0%) | |
| Biomarkers | |||
| GFAP (pg/mL) | 24.7 (21.3, 42.3) | 28.7 (22.9, 38.6) | 0.347 † |
| UCH-L1 (pg/mL) | 112.8 (99.6, 152.0) | 117.7 (100.9, 159.8) | 0.885 † |
| NFL (pg/mL) | 14.2 (12.7, 21.5) | 15.4 (12.3, 17.7) | 0.886 † |
| Variables | Control Group (n = 16; 39.0%) | Atrial Fibrillation Group (n = 25; 61.0%) | p-Value |
|---|---|---|---|
| Magnetic resonance imaging | |||
| Large cortical and non-cortical lesions | 0 (0.0%) | 2 (8.0%) | 0.246 * |
| Large cortical and non-cortical lesions (number) | / | 0.1 ± 0.3 | / |
| Small non-cortical lesions | 5 (31.3%) | 5 (20.0%) | 0.413 * |
| Small non-cortical lesions (number) | 1.2 ± 3.0 | 0.6 ± 1.4 | 0.373 † |
| Microbleeding | 3 (18.8%) | 0 (0.0%) | 0.025 * |
| Microbleeding (number) | 1.4 ± 5.0 | / | 0.172 † |
| White matter hyperintensity | 14 (87.5%) | 23 (92.0%) | 0.636 * |
| Acute or subacute thromboembolic lesions | 1 (6.3%) | 0 (0.0%) | 0.206 * |
| Fazekas scale | 1.1 ± 0.8 | 1.2 ± 0.8 | 0.775 † |
| Variables | Control Group (n = 16; 39.0%) | Atrial Fibrillation Group (n = 25; 61.0%) | p-Value * |
|---|---|---|---|
| PROMIS index | 51.2 ± 6.2 | 52.2 ± 9.6 | 0.706 |
| PROMIS dimension 1: Slower thinking | 3.8 ± 0.8 | 4.2 ± 1.0 | 0.205 |
| PROMIS dimension 2: Impression of brain thinking impairment | 4.3 ± 0.8 | 4.2 ± 0.9 | 0.595 |
| PROMIS dimension 3: Need for a stronger focus on everyday activities | 4.6 ± 0.6 | 4.3 ± 0.9 | 0.295 |
| PROMIS dimension 4: Impairment in multi-tasking | 4.4 ± 0.8 | 4.3 ± 1.1 | 0.762 |
| PROMIS dimension 5: Concentration impairment | 4.1 ± 0.9 | 4.0 ± 1.1 | 0.796 |
| PROMIS dimension 6: Need for stronger focus to avoid mistakes | 4.2 ± 0.9 | 4.2 ± 1.0 | 0.967 |
| PROMIS dimension 7: Impairment in idea shaping | 4.5 ± 0.5 | 4.1 ± 1.1 | 0.215 |
| PROMIS dimension 8: Impairment in number calculation | 4.6 ± 0.6 | 4.5 ± 0.9 | 0.872 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kedžo, J.; Domjanović Škopinić, T.; Domjanović, J.; Marinović Guić, M.; Lovrić Kojundžić, S.; Tandara, L.; Matetić, A.; Jurišić, Z. Neurologic Biomarkers, Neuroimaging, and Cognitive Function in Persistent Atrial Fibrillation: A Cross-Sectional Study. Int. J. Mol. Sci. 2023, 24, 2902. https://doi.org/10.3390/ijms24032902
Kedžo J, Domjanović Škopinić T, Domjanović J, Marinović Guić M, Lovrić Kojundžić S, Tandara L, Matetić A, Jurišić Z. Neurologic Biomarkers, Neuroimaging, and Cognitive Function in Persistent Atrial Fibrillation: A Cross-Sectional Study. International Journal of Molecular Sciences. 2023; 24(3):2902. https://doi.org/10.3390/ijms24032902
Chicago/Turabian StyleKedžo, Josip, Tea Domjanović Škopinić, Josipa Domjanović, Maja Marinović Guić, Sanja Lovrić Kojundžić, Leida Tandara, Andrija Matetić, and Zrinka Jurišić. 2023. "Neurologic Biomarkers, Neuroimaging, and Cognitive Function in Persistent Atrial Fibrillation: A Cross-Sectional Study" International Journal of Molecular Sciences 24, no. 3: 2902. https://doi.org/10.3390/ijms24032902