1. Introduction
Globally, colorectal carcinoma (CRC) is the third cancer in terms of incidence and second in terms of mortality [
1]. In Poland CRC is the second most common cancer in men and woman, with the third leading causes of cancer deaths in Greater Poland Region [
2]. CRC is characterized by high inter-patient and intra-tumor heterogeneity, as well as temporal molecular heterogeneity during treatment, which is known to influence the response to therapy and prognosis [
3]. While genetic and epigenetic mechanisms are important and quite well described in colorectal carcinogenesis, the basis of the most cases of cancer is unknown. A small subset of CRC cases (up to 3%) arises as a consequence of inflammatory bowel diseases [
4].
Both in histologically normal and morphologically changed colon, quantitative and qualitative changes in mucin polysaccharides were described for a few decades [
5,
6,
7,
8]. Some studies suggest that the aberrant and deregulated expression of mucins represent a link between cancer and inflammation [
9].
Mucins are large
O-glycoproteins with high carbohydrate content (over 70%). These mucin glycoconjugates provide the mucus with its biophysiochemical properties, due to their nature and extent of glycosylation [
10]. Carbohydrates are critical for numerous biological processes (i.e., cell–cell adhesion, protein folding, protein trafficking, and cell signaling), with aberrant glycosylation implicated in a variety of diseases, including cancer [
11].
During neoplastic progression, changes in the proportions of mucin glycoconjugates were described: e.g., neutral mucin increase, a reduction in the proportion of side chains of sialic acid, hypersecretion of weakly acid sialomucin and reduction of excessively acid sulfomucin [
5,
6,
7,
9]. Qualitative changes in sialic acid glycans include loss of O-acetyl substituents at C4, C7, C8, C9 or in the polyhydroxy side chain of sialomucin, causing some colonic tumors to contain much less mucin than the adjacent normal tissue [
5,
12,
13].
Colon cancer mucins have differences in both core carbohydrates and peripheral carbohydrate structures that are being investigated as diagnostic and prognostic markers [
14,
15,
16]. It is considered that CRCs producing large amounts of mucus indicate poorer prognosis [
17], and mucinous subtype (~10–15% of cases) is a predictor of poor outcome [
18,
19,
20].
Changes in tissue mucin carbohydrate content are most often analyzed with two basic histochemical (HC) techniques, namely periodic-acid Schiff (PAS) reaction, and alcian blue (AB) staining [
13,
16,
21]. However, these methods are often modified: e.g., combined PAS/AB [
8,
9,
16], mild PAS [
6,
22], PBT/KOH/PAS [
7], PAT/KOH/PAS [
12], KOH-AB pH 1-PAPS [
23], HID-AB [
7,
8,
24], and/or GOS sequence [
25]. The large panel of techniques creates the need for evaluation of their ability to detect particular polysaccharide groups. Their ability to diagnose the largest possible amount of CRC patients (high degree of sensitivity), as well as identify people unaffected by the disease (high degree of specificity) is also very important [
6,
25,
26]. It needs to be added that the progress of glycobiology is delayed by the difficulties in obtaining optimal, commercially available human glycan-specific antibodies used for immunohistochemical (IHC) reactions. To detect and monitor several cancers (including CRC), antibodies that target Sialyl Lewis A (Ca19.9) (antibodies to O-Glycans) are often used as serum biomarkers [
11]. To evaluate the tissue polysaccharide expression, so called MUC1 specific glycan-Tn/STn-MUC1 was synthesized and used [
27].
Traditional HC evaluation of mucin expression conducted by most of pathologists includes visual microscopic observation, use of general descriptions of HC reactions (color of staining reaction, positive/negative, weak, or no staining, etc.) [
13,
22], as well as the use of semi-quantitative scales for estimation of staining intensity and the proportion of positive cells [
6,
9,
28,
29]. The proportion of cells/tumors positive for a particular type of mucins is often indicated: neutral or acidic (sulfomucin, sialomucin) and mixed sialomucin and sulfomucin [
6,
29]. Due to staining heterogeneity of the CRC cells, the pathologists’ visual scoring and interpretation is highly subjective.
The use of computer software to evaluate HC reaction in CRC can only be found in a limited number of studies. A prototype of such analyses could be the quantitative analysis of the area percentage of epithelium expressing galactose-oxidase-Schiff (GOS)-reactive saccharides in CRC, performed with the use of computer-assisted IBAS image cytometry system (AutoCyte, Inc. Elon College, Elon, NC, USA) [
25]. Other authors evaluated deeply scanned mucinous CRC samples at x4 objective magnification with the use of NIS elements image analysis software (Nikon) [
18]. Another study employed the Image J software and Adobe Photoshop, to complement the semi-quantitative analysis [
29].
The number of technical modifications of HC reactions, evaluation of different regions of tumor (epithelium/complete mucosa), lack of unified tissue staining grading systems and difficulties in conduction of meta-analysis of changes in mucin glycoconjugates during colon carcinogenesis, motivated us to compare the results of analyses conducted with the use of two credible, fast and consistent computer-assisted techniques for HC evaluation of mucin expression in CRC. Protocol standardization and minimization of human input subjectivity is important in creating reproducible IHC and HC results.
The first aim of the study was to analyze the HC distribution of PAS- and AB-positive mucins in CRC and normal colorectal tissue samples (control), as well as to evaluate the diagnostic-prognostic role of the carbohydrates’ expression in colorectal carcinogenesis. The second aim was to show a clinical usefulness of two algorithms for quantitative evaluation of HC reaction in color microscopy images by using Image-Pro Premier and Filter HSV programs.
3. Discussion
In our study, there were no differences in PAS+ glycan detection frequency between CRC (100%) and control samples (100%). Other authors with the use of combined PAS-AB detection kit obtained ~70% positive tumors. However, they do not reference these results to control samples [
16].
Quantitative data, obtained from two algorithms of digital image analysis, showed a decreased expression of both PAS+ and AB+ polysaccharides in CRC compared to “normal” colon samples. These results correspond with the results of other authors [
29]. However, the information stating that with the increase of tumor grade, a considerable decrease in the acid mucin production and an increase in the neutral mucin expression is observed, cannot be confirmed [
29]. Allen et al., using modified PAS reaction (PB-KOH-PAS), showed a significant diminution in the amount of O-acylated sialomucins in CRC, compared with its adjacent mucosa [
7]. Similarly, Corfield et al. noted that total mucin sialic acid content significantly decreased with reduction of the O-acetyl transferase activity in CRC vs. control samples [
30].
The results of studies that described an increase in the amount of neutral mucins, a reduction in the proportion of side chains of sialic acid [
5] and/or hyper and moderate secretion of weakly acidic sialomucins in 88% of cases [
9] cannot be confirmed, as particular functional groups of mucin glycoconjugates have not been analyzed. However, it seems that lower mean expression of both PAS+ and AB+ mucins detected in CRC samples, compared to control presented in our study, evidences proportional decrease of both these mucus polysaccharide types in colorectal tumors.
We have not confirmed the reports of more intense staining of neutral (PAS+) polysaccharides in the right colon of normal colorectal region revealed by other authors [
5,
6], suggesting sialic acid heterogeneity within the general population [
6]. However, we have observed increased AB staining in distal (left) vs. proximal (right) part of control colon. The difference in the presence of mucins between the left and right (more reactive for sialomucins) colons were shown in adenomas, since adenomas of the right colon are more protected by sialomucins and therefore less malignantly altered [
31]. In our study higher PAS+ mucins expression was detected in flat tumors (<3 mm) than in protruded (height of tumor ≥3 mm) CRC. Other authors showed more reactive sulfomucins (HID-AB+) in adenomas of < 10 mm diameter [
31].
The use of AB staining (pH 2.5) in this study allowed us to detect acidic mucins: sialomucins (dark blue), as well as sulfomucins (light blue), in 94% of CRC patients and in all of the control tissue samples. Other authors showed positive reaction for acidic polysaccharides in 60% CRC and only in 12% control samples [
8]. Relating to the results in which a significant reduction in excessively acidic sulfomucins was observed [
9], this study also noted a lower expression of AB+ polysaccharides in CRC vs. control. These results could confirm the suggested concept stating that a decline in the production of the sulfated mucins (sulfomucins) predisposes the colonic mucosa to malignancy [
29].
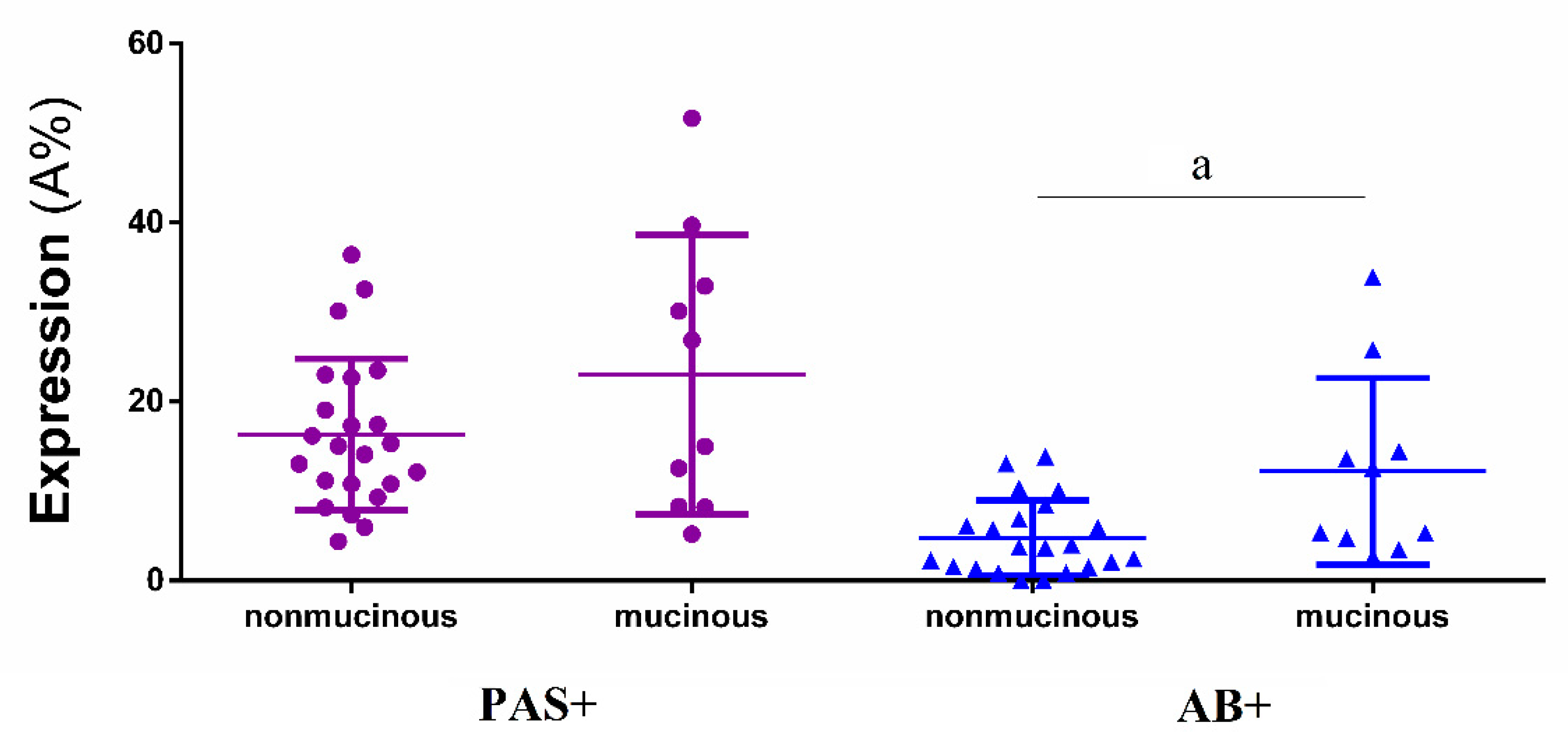
Higher expression of AB+ glycans in mucinous CRC, compared to nonmucinous subtypes, finds confirmation in the literature [
18]. In this study, no significant differences were noted in expression of PAS+ (neutral) and AB+ (acidic) polysaccharides depending on the different grade of CRC and clinical stages of cancer in TNM classification system. Other authors showed predominant cases with acidic mucins, especially in pure mucinous adenocarcinomas (>90%), while those with mixtures of acidic and neutral mucins were present in 62% of the cases. Clinical pure mucinous forms were detected mainly in advanced TNM stages [
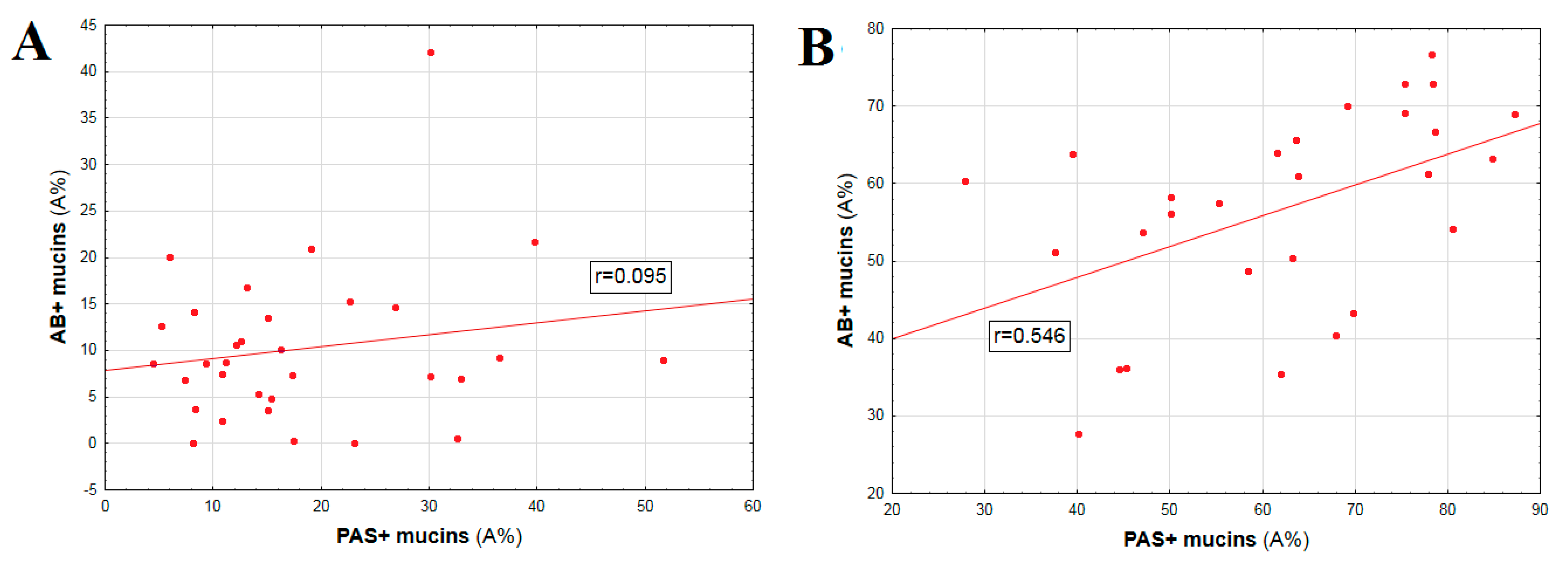
18]. Whereas, the present study showed a high positive correlation between mutual PAS+ and AB+ expression (
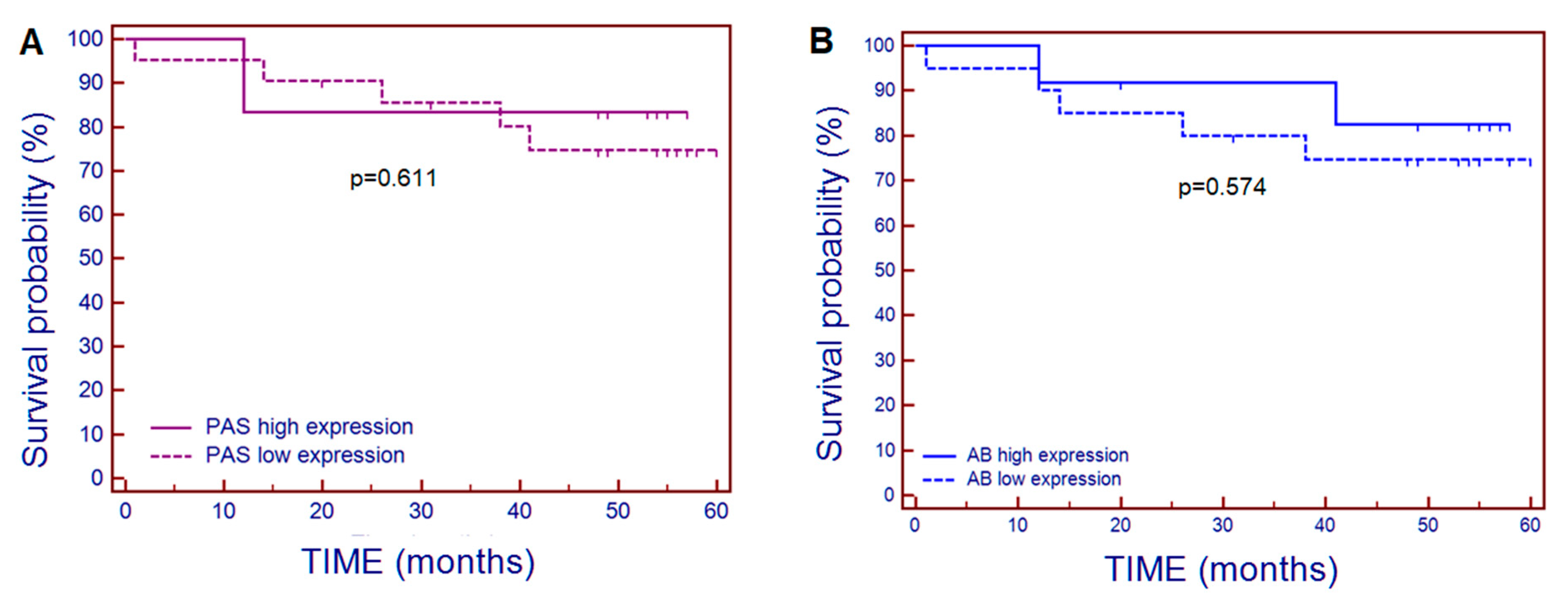
p < 0.008), as well as correlations with glucose concentration (PAS+ mucins), and hemoglobin level (AB+ mucins), but exclusively in unchanged colorectal samples (control). The small number of dead patients (
n = 7) analyzed in the current study, did not allow to draw binding conclusions on the predictive role of PAS+ and AB+ polysaccharides’ tissue expression for the survival time of patients with CRC of the Greater Poland Region.
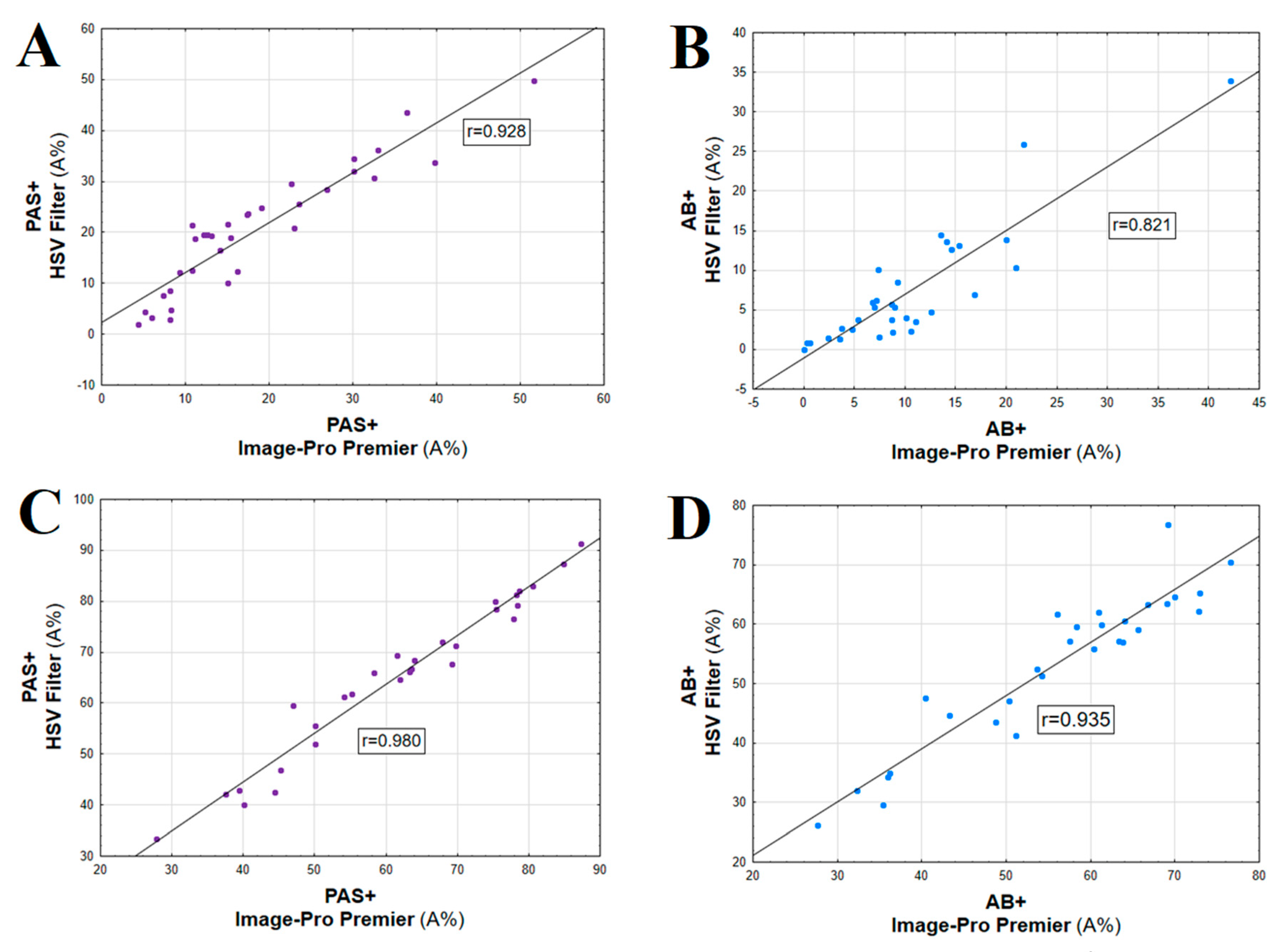
The two novel quantitative digital software types, used in this study, allowed for more objective determination of two types of mucin glycans’ expression, as well as correlation between the results of the analyses and clinicopathological data. Both Image-Pro Premier and Filter HSV can be used for evaluation of classic histochemistry results, as algorithms of initial microscopic picture analysis allow for appropriate counting of positively reacting structures. Image-Pro Premier is more accurate in counting faintly colored objects and objects located on uneven backgrounds, while Filter HSV is faster and more comfortable to use as a tool of HC reaction area in everyday pathological practice. IRS scale as evaluation system used in our study, is not suitable for assessing unchanged large intestinal mucosa tissues in which most cells produce mucus. These observations confirm the necessity of using more precise methods to quantify the expression of the mucins in healthy and cancerous tissues.
High correlation of quantitative expression results of two mucin glycans (PAS+ and AB+) was obtained with the use of smart segmentation algorithm and Filter HSV (Cronbach alpha value of 0.94–0.99). Both algorithms are highly reproducible. Both methods provide procedures of objective evaluation of HC reactions in pathological (CRC) and normal colon tissues (control). The polysaccharides expression using IRS scale correlated with expression obtained by using both algorithms of digital image analysis in CRC group. Comparing three methods (IRS, smart segmentation algorithm, and Filter HSV) for HC reaction evaluation, Cronbach’s alpha values were observed between 0.75 and 0.90.
Computerized analysis of tissue expression was better and more objective for precise evaluation of histochemical reactivity in case of PAS and AB than only semi-quantitative assessment using IRS score, especially in control colon tissue samples and/or in the cases of a very strong HC reaction.
The use of smart segmentation algorithm is accurate, particularly in the case of HC reactions that are difficult for credible visual evaluation, when the biomarker of interest is not uniformly distributed throughout the cell cytoplasm, or when it can only be found in the extracellular matrix. This algorithm also detects all (even faint) shades of magenta and blue.
Overall, it could be concluded, that the smart segmentation seems to be more accurate in identification of faintly-colored objects and objects located on uneven backgrounds, while Filter HSV software is faster, easier to handle in computer-researcher interaction and more comfortable to use as a tool of HC are evaluation in daily practice of pathologists.
4. Materials and Methods
4.1. Patients and Tissue Samples
Thirty-three patients (6 women and 27 men) were diagnosed and surgically treated between 2010–2015 (not treated previously with other forms of therapy), with the surgeries performed in the Chair and Department of General Surgery, Endocrinological and Gastroenterological Oncology, Poznan University of Medical Sciences. We have continued the study on selected patients with CRC only from the Greater Poland Region, from whom consent was obtained, and the perioperative tissue material met the requirements for scientific research [
32]. Patients affected by diabetes, active chronic organ diseases, including autoimmune diseases and other cancers, have been excluded from the study. Inclusion criteria reduced the number of patients, but resulted in greater homogeneity of the group and reduced the potential impact of other factors on the investigated polysaccharides expression.
The patient ages ranged from 32 to 89 years (median of 67 years). Seven patients died during the analysis period. Duration of patient survival reflected the time between the date of CRC surgery and the initial diagnosis, i.e., 1 October 2010, and 1 October 2015. The available clinical data for CRC than was taken into account, included: descriptive histopathological diagnosis, histologic grade and stage (TNM classification), age, patient sex, and basic laboratory studies. The American Joint Committee on Cancer (AJCC) TNM clinical stages (seventh edition) [
33] were assigned to each patient (0, I, II, III, and IV).
Locations of the colorectal tumors were divided into proximal (right) colon and distal (left) colon (including rectum). Macroscopic types were divided into protruded type (height of tumor ≥3 mm) and flat type (height of tumor <3 mm).
Thirty-three paired samples of colorectal tumor and control tissues were obtained simultaneously during surgical treatment. For the CRC, colon mucosa and, depending on the depth of tumor invasion, submucosal layers ~10–15 cm from the tumor site served as control tissues. In no case was tissue additional to that which would be removed normally during the usual surgical procedure taken from the patient. All tissue samples were fixed in 10% neutral buffered formalin for 24 h and routinely transferred into low-melting-point paraffin. To qualify the material for histochemistry, routine staining of the sections with hematoxylin and eosin (H+E) was performed.
4.2. Histochemical Studies
4.2.1. PAS (Periodic Acid Schiff) Reaction
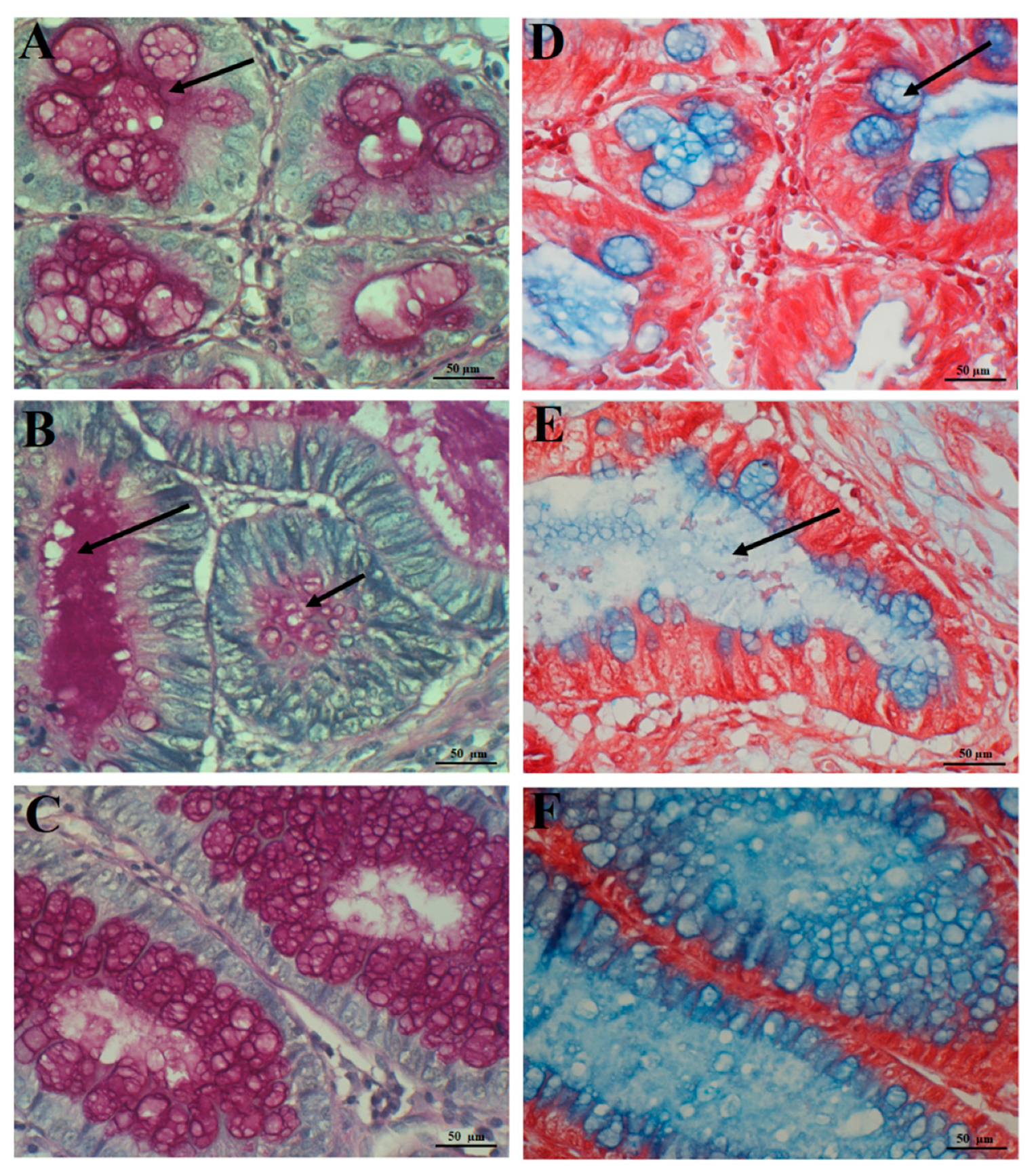
Classic PAS reaction employing the Schiff reagent (decolorized/discolored fuchsin-sulphurous acid) was applied to qualitatively detect neutral mucin polysaccharides in epithelial mucins/mucosubstances, as it is negative for non-sulfated and sulfated acid mucins (sialomucin and sulfomucin, respectively) [
6,
21]. Paraffin sections on microscopic slides were dewaxed and immersed in growing concentrations of ethanol, 50%, 60%, 70%, 80% and 100%, for 5 min in each solution. Then, the samples were immersed in 1% periodic acid (HJO
4)—5 min, washed twice for 2 min with distilled water, immersed in Schiff reagent for 30 min, washed thrice for 2 mins in sulfuric-acid water, washed under running water for 10 min and washed with distilled water. Finally, the paraffin sections were immersed for 2 min in hematoxylin, for counterstaining of cell nuclei, dehydrated in a series of alcohol solutions of increasing concentration and xylene, followed by placement under coverslips with the use of Canada balsam [
5]. The Schiff reagent bound aldehyde groups, yielding purple/red (magenta) color [
21]. The protocol of sulfuric-acid water (10 mL of 1 N HCl, 10 ml of 10% sodium metabisulfite water solution and 180 mL of water) and Schiff reagent preparation was in accordance with existing databases [
34].
4.2.2. Alcian Blue (AB) Staining
For selective detection of epithelial non-sulphated (sialomucins) and sulphated acid mucins (sulfomucins) (dark/light blue color, respectively) [
21] alcian blue (AB) staining in pH 2.5 was applied (Sigma-Aldrich, Poznan, Poland). The subsequent stages included (1) deparaffination of slices; (2) incubation in 1% solution of alcian blue (pH 2.5) for 23 min; (3) washing under running water for 3 min; (4) incubation in 1% safranin O solution (Sigma-Aldrich, Poland) for 10 s; (5) washing under running water for 7 min; (6) fast dehydration in a serial alcohol dilution (<1 min) and slide mounting. It needs to be added that goblet cells of normal colon mucosa serve as a control for both HC reactions (PAS, AB) [
6].
4.3. Semiquantitative Evaluation of the PAS+ and AB+ Mucins
The PAS+ and AB+ polysaccharide expression in CRC and control tissue specimens were evaluated by the semi-quantitative 12-points score (immunoreactive score, IRS), originally designed to assess immunohistochemical reactions [
35]. Number of cells with positive reaction (PP—percentage of positive cells) and intensity of the reaction (SI—staining intensity) were evaluated in 10 fields of Olympus B-2 microscope, at ×400 magnification. The final score reflected the product of the two variables (PPxSI) and ranged from 0 to 12 points (low reaction: 1 to 2 points, moderate reaction: 3 to 4 points, strong reaction: 6 to 12 points) and reflected the average number of PAS/AB-positive cells from all fields evaluated under microscope.
4.4. Quantitative Evaluation of Tissue Polysaccharide Expression
Histological slides with HC reaction were examined under the optical Olympus BH-2 microscope coupled to a digital camera. Color microscope images were recorded using a 40× magnification objective (at least 10 fields in every microscope slide with a PAS and AB-positive reaction) and LUCIA Image 5.0 computer software (2560 × 1920 pixels in size). A total of ~1300 color microscope images of CRC and control samples, stained with each of the used methods (PAS and AB), were separately counted using two algorithms.
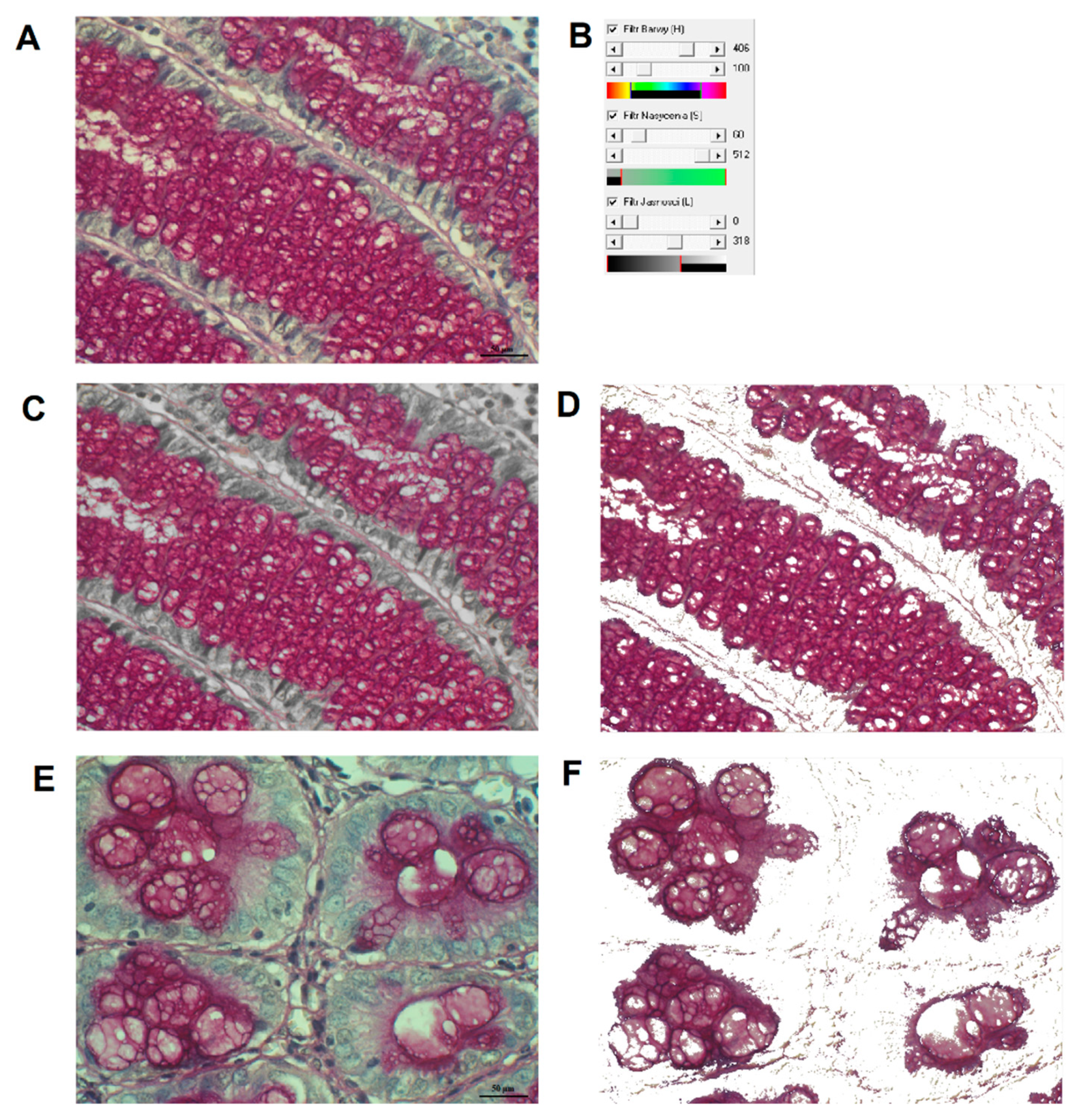
4.4.1. Image Analysis by using Filter HSV Program
The original Filter HSV program was worked out in the Department of Bioinformatics and Computational Biology, Poznan University of Medical Sciences [
36,
37]. In summary, for three coordinates of HSV color space: H (Hue), S (Saturation) and V (Value–brightness) ranges of colors (thresholds) specific for PAS and AB reactions were first assigned. Then, a segmentation of HC reaction was performed by thresholding (
Figure 6). The program automatically counts pixels specific for the reaction and determines a percentage of HC reaction area, in relation to the tissue area, i.e., area fraction (A%):
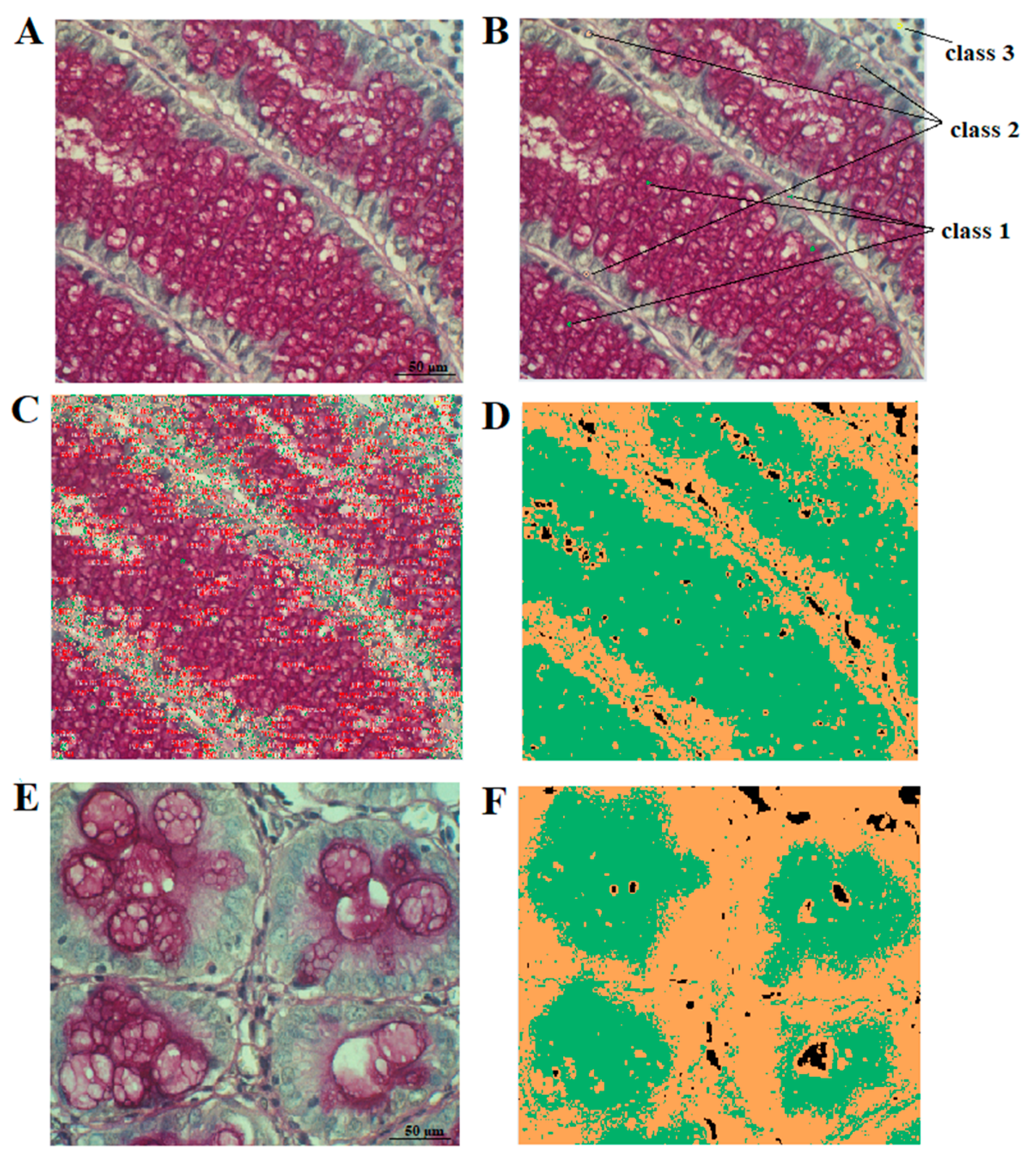
4.4.2. Image Analysis with Smart Segmentation Algorithm by using Image-Pro Premier Software (Media Cybernetics v 9.3.2)
Alternatively, a smart segmentation method was used, to extract and quantify the HC reaction. The method utilizes a pixel classification algorithm to identify objects and regions in three-steps. Thus, three classes of colors are defined (
Figure 7):
- -
class 1: colors specific for the HC reaction,
- -
class 2: colors of tissue without the reaction,
- -
class 3: background (i.e., everything which does not belong to class 1 and 2).
After detection and interactive classification of colors specific for the reaction in given morphological structures, the number of pixels representing the reaction was counted and the percentage A% was computed according to the following formula:
A% = (number of pixels belonging to class 1)/(number of pixels belonging to class 1 or class 2) × 100%. Ten microscopic fields were chosen randomly from samples of CRC tissue and the normal colorectal mucosa (control). In both methods, A% was determined in each of 10 fields per slide.
4.5. Statistical Analysis
Comparative analysis of results obtained using IRS scale and two computer-based methods were assessed by Cronbach’s alpha value. Two computer-based methods (smart segmentation algorithm and Filter HSV) were also assessed by Cronbach’s alpha coefficient. The consistency between the two computer-assisted techniques was confirmed by non-parametric Spearman’s correlation coefficient. All results were first verified by a normality test. Since the test confirmed a lack of normality, non-parametric methods were used for statistical analysis. Differences between PAS and AB expression in tumor tissue and in control were tested by the Wilcoxon test. Differences between unpaired results were verified by the Mann-Whitney test.
Correlations between A% vs. age and clinical data were analyzed by the Spearman’s correlation coefficient.
Two subgroups of tumor samples were also determined: below the mean expression and above the mean expression of PAS and AB reactions. The survival time of patients in both determined groups was analyzed by Kaplan-Meier and log-rank test. The statistical analysis was performed with Statistica v. 12. (Statsoft Inc., Tulsa, OK, USA). Results were accepted as significant at p < 0.05.
4.6. Ethics Statement
Informed consent was obtained from every subject, with approval for the research obtained from the institutional bioethical committee on Bioethics, Poznan University of Medical Sciences, 61-701 Poznan, Poland (no. 924/14). The research protocol fulfils the standards recommended by the Helsinki Convention.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}