Clinicopathologic Significance of VHL Gene Alteration in Clear-Cell Renal Cell Carcinoma: An Updated Meta-Analysis and Review


Abstract
:1. Introduction
2. Results
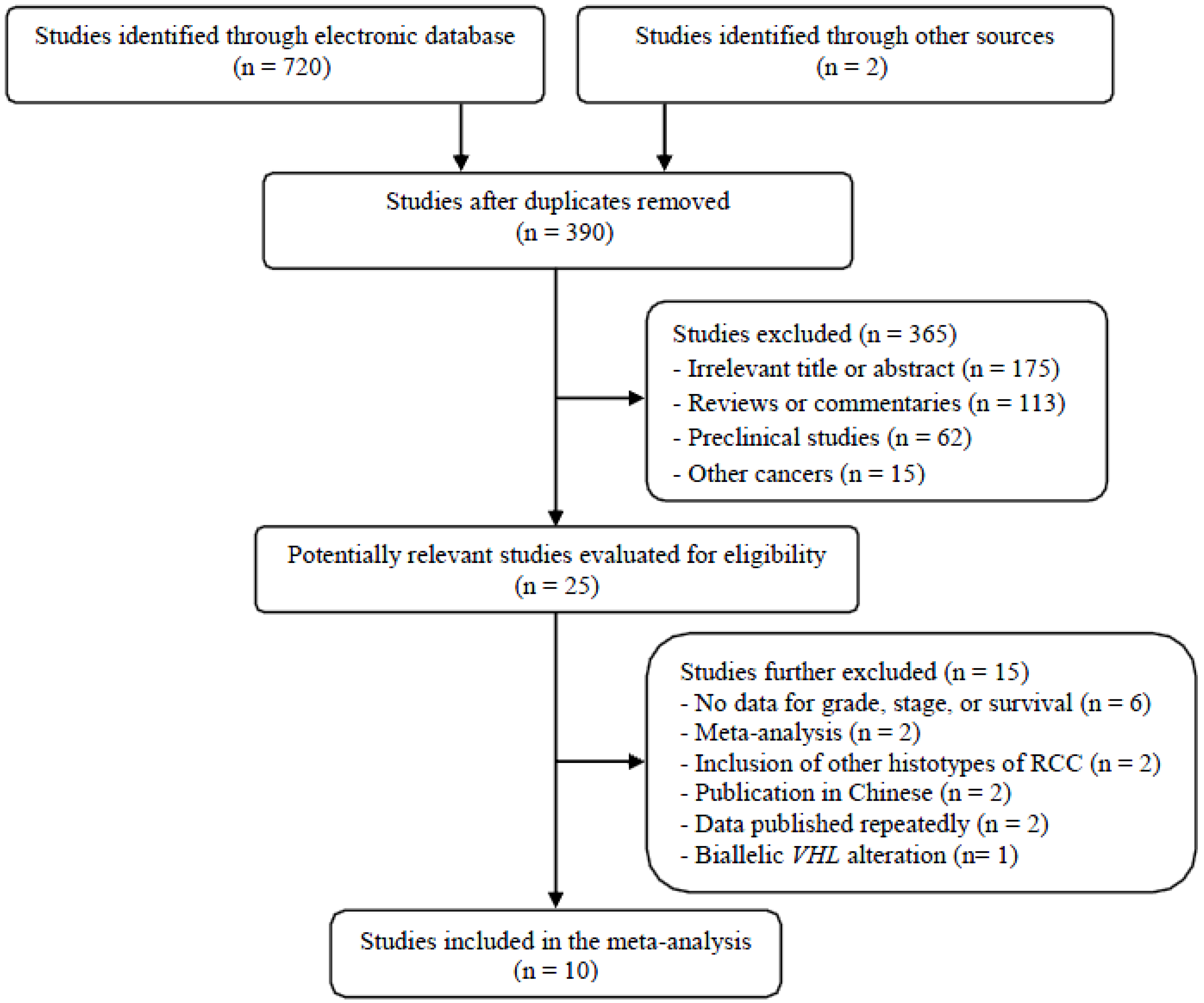
2.1. Results of Search
2.2. Characteristics of the Included Studies
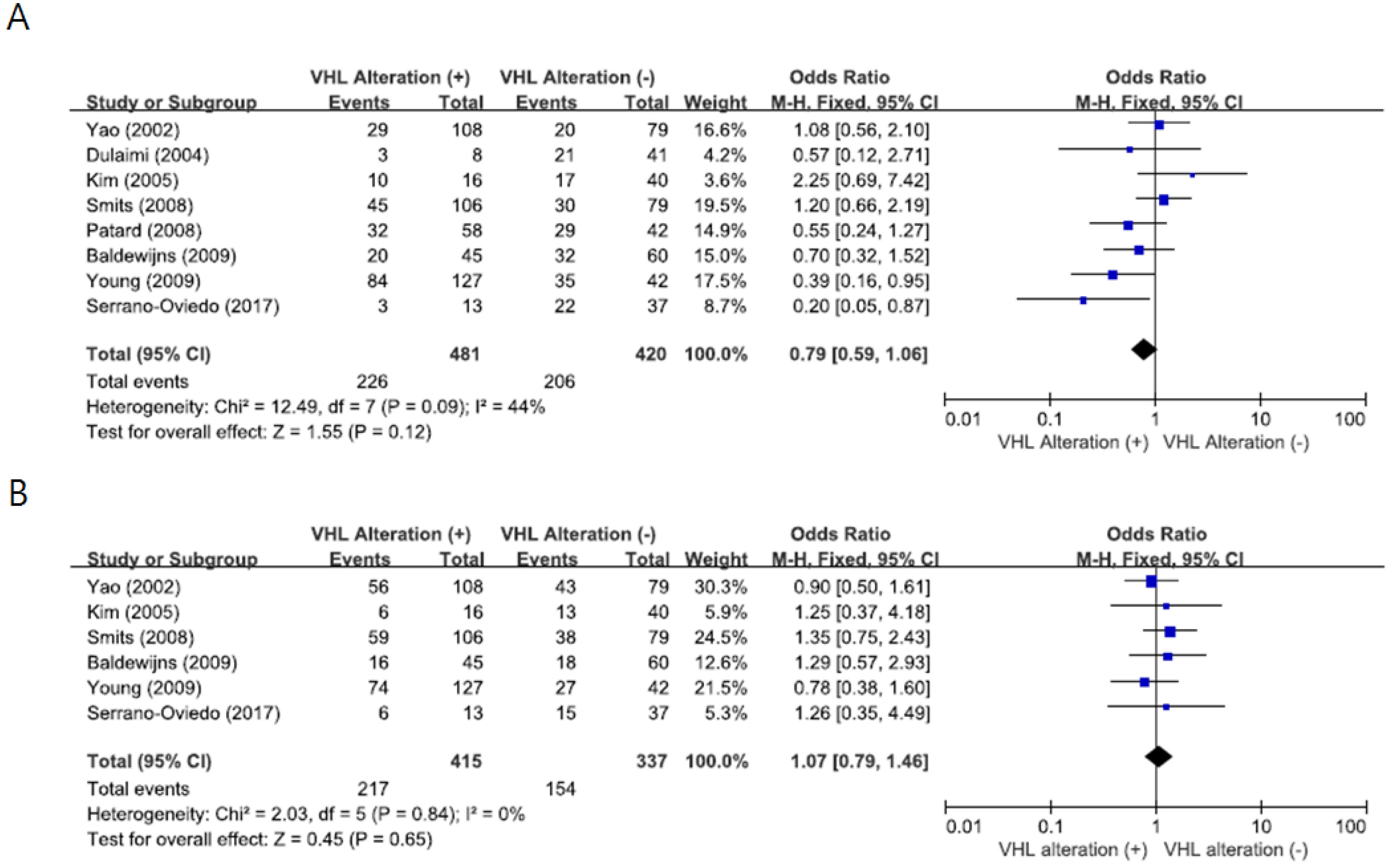
2.3. Impact of VHL Gene Alteration on Pathological Features
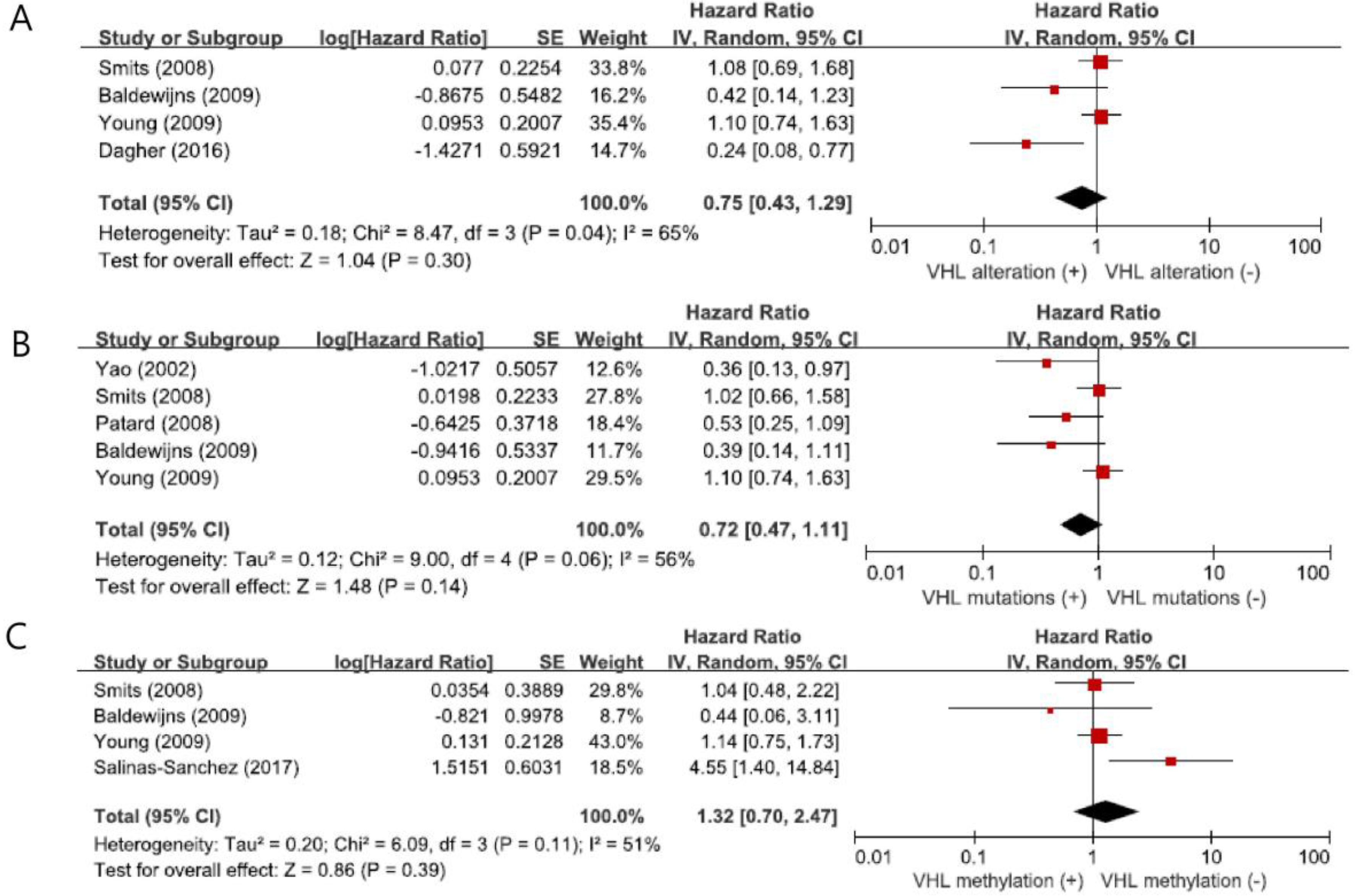
2.4. Impact of VHL Variations on Overall Survival
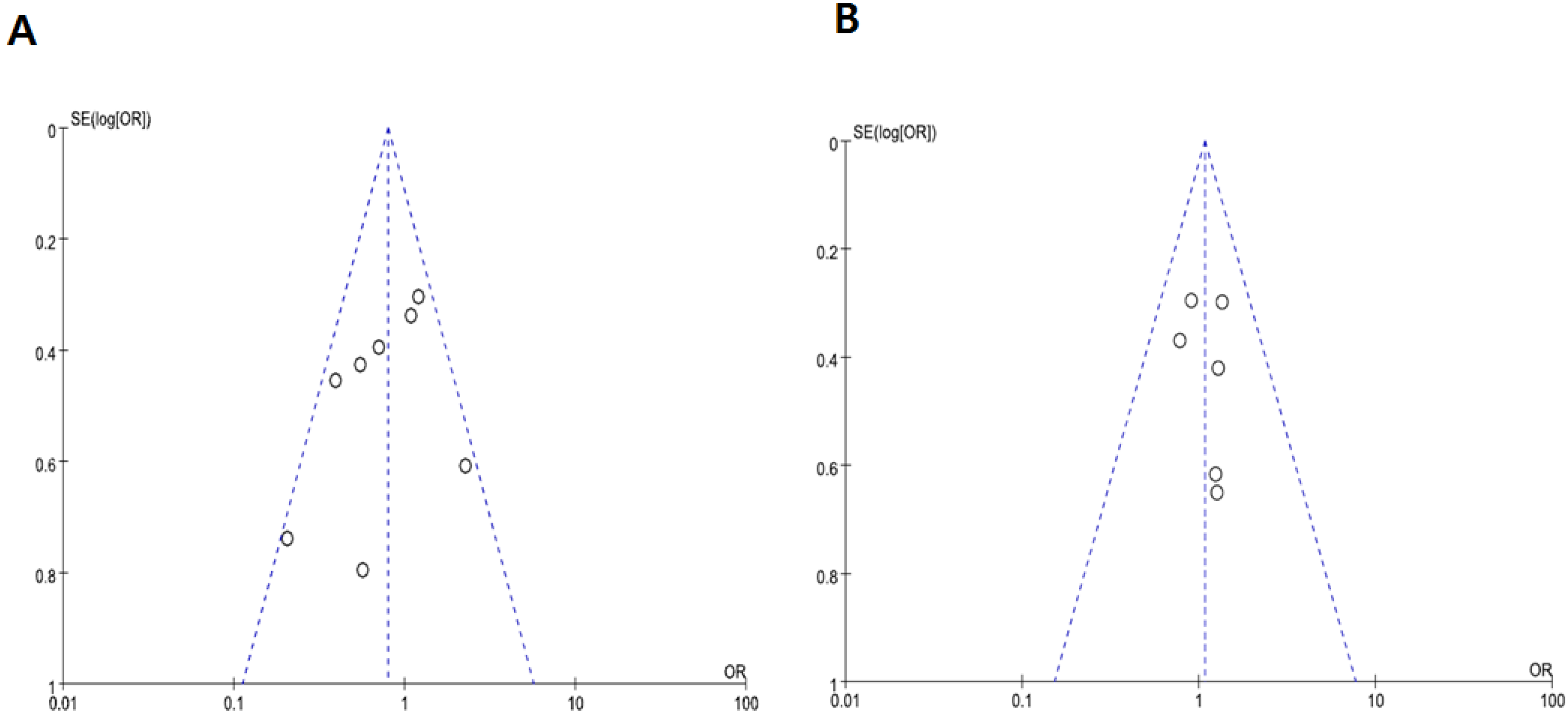
2.5. Publication Bias
3. Discussion
4. Materials and Methods
4.1. Searching Strategy
4.2. Inclusion Criteria
4.3. Data Extraction
4.4. Statistical Analyses
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ccRCC | clear-cell renal cell carcinoma |
| CI | confidence interval |
| DSS | disease-specific survival |
| HR | hazard ratio |
| LOF | loss of function |
| LOH | loss of heterozygosity |
| NG | nuclear grade |
| OR | odd ratio |
| OS | overall survival |
| PCR | polymerase chain reaction |
| VHL | von Hippel-Lindau |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S. Community of population-based regional cancer registries. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2015. Cancer Res. Treat. 2018, 50, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K. Renal Cell Tumors: Understanding Their Molecular Pathological Epidemiology and the 2016 WHO Classification. Int. J. Mol. Sci. 2017, 18, 2195. [Google Scholar] [CrossRef] [PubMed]
- Wolff, I.; May, M.; Hoschke, B.; Zigeuner, R.; Cindolo, L.; Hutterer, G.; Schips, L.; De Cobelli, O.; Rocco, B.; De Nunzio, C.; et al. Do we need new high-risk criteria for surgically treated renal cancer patients to improve the outcome of future clinical trials in the adjuvant setting? Results of a comprehensive analysis based on the multicenter CORONA database. Eur. J. Surg. Oncol. 2016, 42, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Smaletz, O. Current management and future directions in the treatment of advanced renal cell carcinoma-a latin american perspective: 10 Years in review. Int. Braz. J. Urol. 2015, 41, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Barata, P.C.; Rini, B.I. Treatment of renal cell carcinoma: Current status and future directions. CA Cancer J. Clin. 2017, 67, 507–524. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Jin, J.; Oya, M.; Uemura, H.; Takahashi, S.; Tatsugami, K.; Rha, S.Y.; Lee, J.L.; Chung, J.; Lim, H.Y.; et al. Safety of pazopanib and sunitinib in treatment-naive patients with metastatic renal cell ca rcinoma: Asian versus non-Asian subgroup analysis of the COMPARZ trial. J. Hematol. Oncol. 2018, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Latif, F.; Tory, K.; Gnarra, J.; Yao, M.; Duh, F.M.; Orcutt, M.L.; Stackhouse, T.; Kuzmin, I.; Modi, W.; Geil, L.; et al. Identification of the von Hippel-Lindau disease tumor suppressor gene. Science 1993, 260, 1317–1320. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of clear cell renal cell carcinoma. Nature 2013, 499, 43–49. [Google Scholar] [Green Version]
- Schödel, J.; Grampp, S.; Maher, E.R.; Moch, H.; Ratcliffe, P.J.; Russo, P.; Mole, D.R. Hypoxia, Hypoxia-inducible Transcription Factors, and Renal Cancer. Eur. Urol. 2016, 69, 646–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiesener, M.S.; Münchenhagen, P.M.; Berger, I.; Morgan, N.V.; Roigas, J.; Schwiertz, A.; Jürgensen, J.S.; Gruber, G.; Maxwell, P.H.; Löning, S.A.; et al. Constitutive activation of hypoxia-inducible genes related to overexpression of hypoxia-inducible factor-1alpha in clear cell renal carcinomas. Cancer Res. 2001, 61, 215–222. [Google Scholar]
- Gnarra, J.R.; Tory, K.; Weng, Y.; Schmidt, L.; Wei, M.H.; Li, H.; Latif, F.; Liu, S.; Chen, F.; Duh, F.M.; et al. Mutations of the VHL tumour suppressor gene in renal carcinoma. Nat. Genet. 1994, 7, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Shuin, T.; Kondo, K.; Torigoe, S.; Kishida, T.; Kubota, Y.; Hosaka, M.; Nagashima, Y.; Kitamura, H.; Latif, F.; Zbar, B.; et al. Frequent somatic mutations and loss of heterozygosity of the von Hippel-Lindau tumor suppressor gene in primary human renal cell carcinomas. Cancer Res. 1994, 54, 2852–2855. [Google Scholar] [PubMed]
- Zbar, B.; Brauch, H.; Talmadge, C.; Linehan, M. Loss of alleles of loci on the short arm of chromosome 3 in renal cell carcinoma. Nature 1987, 327, 721–724. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.G.; Latif, F.; Weng, Y.; Lerman, M.I.; Zbar, B.; Liu, S.; Samid, D.; Duan, D.S.; Gnarra, J.R.; Linehan, W.M.; et al. Silencing of the VHL tumor-suppressor gene by DNA methylation in renal carcinoma. Proc. Natl. Acad. Sci. USA 1994, 91, 9700–9704. [Google Scholar] [CrossRef] [PubMed]
- Cowey, C.L.; Rathmell, W.K. VHL gene mutations in renal cell carcinoma: Role as a biomarker of disease outcome and drug efficacy. Curr. Oncol. Rep. 2009, 11, 94–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, H.P.; Bender, B.U.; Berger, D.P.; Laubenberger, J.; Schultze-Seemann, W.; Wetterauer, U.; Ferstl, F.J.; Herbst, E.W.; Schwarzkopf, G.; Hes, F.J.; et al. Prevalence, morphology and biology of renal cell carcinoma in von Hippel-Lindau disease compared to sporadic renal cell carcinoma. J. Urol. 1998, 160, 1248–1254. [Google Scholar] [CrossRef]
- Brauch, H.; Weirich, G.; Brieger, J.; Glavac, D.; Rödl, H.; Eichinger, M.; Feurer, M.; Weidt, E.; Puranakanitstha, C.; Neuhaus, C.; et al. VHL alterations in human clear cell renal cell carcinoma: Association with advanced tumor stage and a novel hot spot mutation. Cancer Res. 2000, 60, 1942–1948. [Google Scholar] [PubMed]
- Khaliq, S.; Ajaz, S.; Firasat, S.; Shahid, S.; Hasan, A.S.; Sultan, G.; Mohsin, R.; Hashmi, A.; Mubarak, M.; Naqvi, S.A.; et al. Unique molecular alteration patterns in von Hippel-Lindau (VHL) gene in a cohort of sporadic renal cell carcinoma patients from Pakistan. Mutat. Res. 2014, 763–764, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Kondo, K.; Yao, M.; Yoshida, M.; Kishida, T.; Shuin, T.; Miura, T.; Moriyama, M.; Kobayashi, K.; Sakai, N.; Kaneko, S.; et al. Comprehensive mutational analysis of the VHL gene in sporadic renal cell carcinoma: Relationship to clinicopathological parameters. Gene Chromosom. Cancer 2002, 34, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Yoshida, M.; Kishida, T.; Nakaigawa, N.; Baba, M.; Kobayashi, K.; Miura, T.; Moriyama, M.; Nagashima, Y.; Nakatani, Y.; et al. VHL tumor suppressor gene alterations associated with good prognosis in sporadic clear-cell renal carcinoma. J. Natl. Cancer Inst. 2002, 94, 1569–1575. [Google Scholar] [CrossRef] [PubMed]
- Dulaimi, E.; Ibanez de Caceres, I.; Uzzo, R.G.; Al-Saleem, T.; Greenberg, R.E.; Polascik, T.J.; Babb, J.S.; Grizzle, W.E.; Cairns, P. Promoter hypermethylation profile of kidney cancer. Clin. Cancer Res. 2004, 10, 3972–3979. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Jung, C.W.; Cho, Y.H.; Lee, J.; Lee, S.H.; Kim, H.Y.; Park, J.; Park, J.O.; Kim, K.; Kim, W.S.; et al. Somatic VHL alteration and its impact on prognosis in patients with clear cell renal cell carcinoma. Oncol. Rep. 2005, 13, 859–864. [Google Scholar] [PubMed]
- Smits, K.M.; Schouten, L.J.; van Dijk, B.A.; Hulsbergen-van de Kaa, C.A.; Wouters, K.A.; Oosterwijk, E.; van Engeland, M.; van den Brandt, P.A. Genetic and epigenetic alterations in the von hippel-lindau gene: The influence on renal cancer prognosis. Clin. Cancer Res. 2008, 14, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Patard, J.J.; Fergelot, P.; Karakiewicz, P.I.; Klatte, T.; Trinh, Q.D.; Rioux-Leclercq, N.; Said, J.W.; Belldegrun, A.S.; Pantuck, A.J. Low CAIX expression and absence of VHL gene mutation are associated with tumor aggressiveness and poor survival of clear cell renal cell carcinoma. Int. J. Cancer 2008, 123, 395–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldewijns, M.M.; van Vlodrop, I.J.; Smits, K.M.; Vermeulen, P.B.; Van den Eynden, G.G.; Schot, F.; Roskams, T.; van Poppel, H.; van Engeland, M.; de Bruïne, A.P. Different angiogenic potential in low and high grade sporadic clear cell renal cell carcinoma is not related to alterations in the von Hippel-Lindau gene. Cell Oncol. 2009, 31, 371–382. [Google Scholar] [PubMed]
- Young, A.C.; Craven, R.A.; Cohen, D.; Taylor, C.; Booth, C.; Harnden, P.; Cairns, D.A.; Astuti, D.; Gregory, W.; Maher, E.R.; et al. Analysis of VHL Gene Alterations and their Relationship to Clinical Parameters in Sporadic Conventional Renal Cell Carcinoma. Clin. Cancer Res. 2009, 15, 7582–7592. [Google Scholar] [CrossRef] [PubMed]
- Dagher, J.; Kammerer-Jacquet, S.F.; Brunot, A.; Pladys, A.; Patard, J.J.; Bensalah, K.; Perrin, C.; Verhoest, G.; Mosser, J.; Lespagnol, A.; et al. Wild-type VHL Clear Cell Renal Cell Carcinomas Are a Distinct Clinical and Histologic Entity: A. 10-Year Follow-up. Eur. Urol. Focus 2016, 1, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrano-Oviedo, L.; Giménez-Bachs, J.M.; Nam-Cha, S.Y.; Cimas, F.J.; García-Cano, J.; Sánchez-Prieto, R.; Salinas-Sánchez, A.S. Implication of VHL, ERK5, and HIF-1alpha in clear cell renal cell carcinoma: Molecular basis. Urol. Oncol. 2017, 35, 15–22. [Google Scholar]
- Salinas-Sánchez, A.S.; Serrano-Oviedo, L.; Nam-Cha, S.Y.; Roche-Losada, O.; Sánchez-Prieto, R.; Giménez-Bachs, J.M. Prognostic Value of the VHL, HIF-1α, and VEGF Signaling Pathway and Associated MAPK (ERK1/2 and ERK5) Pathways in Clear-Cell Renal Cell Carcinoma. A. Long-Term Study. Clin. Genitourin. Cancer 2017, 15, 923–933. [Google Scholar]
- Escudier, B.; Pluzanska, A.; Koralewski, P.; Ravaud, A.; Bracarda, S.; Szczylik, C.; Chevreau, C.; Filipek, M.; Melichar, B.; Bajetta, E.; et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: A. randomised, double-blind phase III trial. Lancet 2007, 370, 2103–2111. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Fay, A.P.; Gagnon, R.; Lin, Y.; Bahamon, B.; Brown, V.; Rosenberg, J.E.; Hutson, T.E.; Baker-Neblett, K.L.; Carpenter, C.; et al. The role of aberrant VHL/HIF pathway elements in predicting clinical outcome to pazopanib therapy in patients with metastatic clear-cell renal cell carcinoma. Clin. Cancer Res. 2013, 19, 5218–5226. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Vaziri, S.A.J.; Jaeger, E.; Elson, P.; Wood, L.; Bhalla, I.P.; Small, E.J.; Weinberg, V.; Sein, N.; Simko, J.; et al. von Hippel-Lindau gene status and response to vascular endothelial growth factor targeted therapy for metastatic clear cell renal cell carcinoma. J. Urol. 2008, 180, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Kim, J.H.; Kim, H.S.; Zang, D.Y. Prognostic and predictive value of VHL gene alteration in renal cell carcinoma: A meta-analysis and review. Oncotarget 2017, 8, 13979–13985. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhao, Z.; Zhao, S.; Chen, C.; Cong, X.; Li, Z.; Ren, M. The Clinicopathological significance of epigenetic silencing of VHL promoter and renal cell carcinoma: A meta-analysis. Cell Physiol. Biochem. 2016, 40, 1465–1472. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Bachs, J.M.; Salinas-Sánchez, A.S.; Sánchez-Sánchez, F.; Lorenzo-Romero, J.G.; Donate-Moreno, M.J.; Pastor-Navarro, H.; García-Olmo, D.C.; Escribano-Martínez, J.; Virseda-Rodríguez, J.A. Determination of vhl gene mutations in sporadic renal cell carcinoma. Eur. Urol. 2006, 49, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Lessi, F.; Mazzanti, C.M.; Tomei, S.; Di Cristofano, C.; Minervini, A.; Menicagli, M.; Apollo, A.; Masieri, L.; Collecchi, P.; Minervini, R.; et al. VHL and HIF-1α: Gene variations and prognosis in early-stage clear cell renal cell carcinoma. Med. Oncol. 2014, 31, 840. [Google Scholar] [CrossRef] [PubMed]
- Schraml, P.; Struckmann, K.; Hatz, F.; Sonnet, S.; Kully, C.; Gasser, T.; Sauter, G.; Mihatsch, M.J.; Moch, H. VHL mutations and their correlation with tumour cell proliferation, microvessel density, and patient prognosis in clear cell renal cell carcinoma. J. Pathol. 2002, 196, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Jaeger, E.; Weinberg, V.; Sein, N.; Chew, K.; Fong, K.; Simko, J.; Small, E.J.; Waldman, F.M. Clinical response to therapy targeted at vascular endothelial growth factor in metastatic renal cell carcinoma: Impact of patient characteristics and Von Hippel-Lindau gene status. BJU Int. 2006, 98, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Panic, N.; Leoncini, E.; de Belvis, G.; Ricciardi, W.; Boccia, S. Evaluation of the endorsement of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement on the quality of published systematic review and meta-analyses. PLoS ONE 2013, 8, 83138. [Google Scholar] [CrossRef] [PubMed]
- Wald, N.J.; Bestwick, J.P. Presentation of meta-analysis plots. J. Med. Screen. 2015, 22, 49–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, 4002. [Google Scholar] [CrossRef] [PubMed]
- Eagger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) [Ref] | Country | Detection Methods | No. of Patients | VHL Alteration (Yes, No) (%) | Grade III–IV (Yes vs. No) p-Value OR for Grade III–IV (95% CI) | Stage III–IV (Yes vs. No) p-Value OR for Stage III–IV (95% CI) | HR for OS (95% CI) p-Value |
|---|---|---|---|---|---|---|---|
| Yao (2002) [22] | Japan | DNA-SSCP + direct sequencing | 187 | Mutations (yes: 98, no: 89) (52.4%) Methylation (yes: 10, no 177) (5.3%) | 29/108 (26.9%) vs. 20/79 (25.3%) p = 0.463 1.08 (0.56–2.10) | 56/108(51.8%) vs. 43/79 (54.4%) p = 0.463 0.9 (0.50–1.61) | Mutations: 0.36 (0.13–0.97) p = 0.023 |
| Dulaimi (2004) [23] | USA | MS-PCR | 50 | Methylation (yes: 8, no: 42) (16%) | 3/8(37.5%) vs. 21/41 (51.2%) NS 0.57 (0.12–2.71) | NA | NA |
| Kim (2005) [24] | Korea | DNA-SSCP + direct sequencing MS-PCR | 56 | Mutations or methylation (yes: 16, no: 40) (28.6%) | 10/16 (62.5%) vs. 17/40 (42.5%) p = 0.487 2.25 (0.69–7.42) | 6/16 (37.5%) vs. 13/40 (32.5%) p = 0.809 1.25 (0.37–4.18) | NA |
| Smits (2008) [25] | Netherlands | DNA-SSCP + direct sequencing MS-PCR | 185 | LOF mutations or methylation (yes: 106, no: 79) (57.3%) Methylation (yes: 16, no: 131) (10.9%) | 45/106 (42.5%) vs. 30/79 (38%) p = 0.537 1.20 (0.66–2.19) | 59/106 (55.7%) vs. 38/79 (48.1%) p = 0.681 1.35 (0.75–2.43) | 1.08 (0.69–1.68) p = 0.461 Mutations: 1.02 (0.66–1.58) Methylation: 1.04 (0.48–2.22) p = 0.439 |
| Patard (2008) [26] | France, USA | PCR + direct sequencing | 100 | Mutations (yes: 58, no: 42) (58%) | 32/58 (55.2%) vs. 29/42 (69%) p = 0.16 0.55 (0.24–1.27) | NA | 0.53 (0.25–1.09) p = 0.084 |
| Baldewijns (2009) [27] | Belgium | PCR + direct sequencing MS-PCR | 134 | LOF mutations or methylation (yes: 96, no: 38) (71.6%) | 20/45 (44.4%) vs. 32/60 (53.5%) p = 0.762 0.70 (0.32–1.52) | 16/45 (35.6%) vs. 18/60 (30%) p = 0.212 1.29 (0.57–2.93) | 0.42 (0.14–1.23) p = 0.423 Mutations: 0.39 (0.14–1.11) p = 0.078 Methylation: 0.44 (0.06–3.11) p = 0.411 |
| Young (2009) [28] | UK | PCR + DNA sequencing MS-PCR | 177 | Mutations (yes: 127, no: 42) (75.1%) Methylation (yes: 51, no: 112) (31.3%) | 84/127 (66.1%) vs. 35/42 (83.3%) 0.39 (0.16–0.95) 42/51 (82.4%) vs. 71/112 (63.4%) | 74/127 (58.3%) vs. 27/42 (64.3%) 0.78 (0.38–1.60) 33/51 (64.7%) vs. 66/112 (58.9%) | 1.10 (0.74–1.63) p = 0.63 Mutations: 0.87 (0.30–2.56) p = 0.80 Methylation: 1.14 (0.75–1.73) p = 0.54 |
| Dagher (2016) [29] | France | PCR + sequencing reaction MS-MLPA | 98 | Mutations, LOH, or methylation (yes: 87, no: 11) (88.8%) | NA | NA | 0.24 (0.075–0.766) p = 0.016 |
| Serrano-Oviedo (2017) [30] | Spain | PCR + direct sequencing | 50 | Mutations (yes: 13, no: 37) (26%) | 3/13 (23.1%) vs. 22/37 (59.5%) p = 0.036 0.20 (0.05–0.87) | 6/13 (46.2%) vs. 15/37 (40.5%) NS 1.26 (0.35–4.49) | NA |
| Salinas-Sanchez (2017) [31] | Spain | PCR + automatic DNA sequencing MS-PCR | 46 | Methylation (yes: 10, no: 36) (21.7%) | NA | NA | Methylation: 4.45 (1.40–14.84) p = 0.012 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Kim, J.H.; Jang, H.J.; Han, B.; Zang, D.Y. Clinicopathologic Significance of VHL Gene Alteration in Clear-Cell Renal Cell Carcinoma: An Updated Meta-Analysis and Review. Int. J. Mol. Sci. 2018, 19, 2529. https://doi.org/10.3390/ijms19092529
Kim HS, Kim JH, Jang HJ, Han B, Zang DY. Clinicopathologic Significance of VHL Gene Alteration in Clear-Cell Renal Cell Carcinoma: An Updated Meta-Analysis and Review. International Journal of Molecular Sciences. 2018; 19(9):2529. https://doi.org/10.3390/ijms19092529
Chicago/Turabian StyleKim, Hyeong Su, Jung Han Kim, Hyun Joo Jang, Boram Han, and Dae Young Zang. 2018. "Clinicopathologic Significance of VHL Gene Alteration in Clear-Cell Renal Cell Carcinoma: An Updated Meta-Analysis and Review" International Journal of Molecular Sciences 19, no. 9: 2529. https://doi.org/10.3390/ijms19092529
APA StyleKim, H. S., Kim, J. H., Jang, H. J., Han, B., & Zang, D. Y. (2018). Clinicopathologic Significance of VHL Gene Alteration in Clear-Cell Renal Cell Carcinoma: An Updated Meta-Analysis and Review. International Journal of Molecular Sciences, 19(9), 2529. https://doi.org/10.3390/ijms19092529